
Abstract
Background
Iron-refractory iron deficiency anaemia (IRIDA) is an autosomal recessive iron deficiency anaemia caused by mutations in the TMPRSS6 gene. Iron deficiency anaemia is common, whereas IRIDA is rare. The prevalence of IRIDA is unclear. This study aimed to estimate the carrier frequency and genetic prevalence of IRIDA using Genome Aggregation Database (gnomAD) data.
Methods
The pathogenicity of TMPRSS6 variants was interpreted according to the American College of Medical Genetics and Genomics (ACMG) and the Association for Molecular Pathology (AMP) standards and guidelines. The minor allele frequency (MAF) of TMPRSS6 gene disease-causing variants in 141,456 unique individuals was examined to estimate the global prevalence of IRIDA in seven ethnicities: African/African American (afr), American Admixed/Latino (amr), Ashkenazi Jewish (asj), East Asian (eas), Finnish (fin), Non-Finnish European (nfe) and South Asian (sas). The global and population-specific carrier frequencies and genetic prevalence of IRIDA were calculated using the Hardy–Weinberg equation.
Results
In total, 86 pathogenic/likely pathogenic variants (PV/LPV) were identified according to ACMG/AMP guideline. The global carrier frequency and genetic prevalence of IRIDA were 2.02 per thousand and 1.02 per million, respectively.
Conclusions
The prevalence of IRIDA is greater than previous estimates.
Similar content being viewed by others


Background
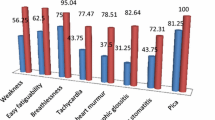
Iron-refractory iron deficiency anaemia (IRIDA) (OMIM: 206200, ORPHA: 209981) is a refractory iron deficiency anaemia that is unresponsive to oral iron treatment [1,2,3,4], leading to microcytic hypochromic anaemia, low transferrin saturation and serum iron [5]. Symptoms of IRIDA are usually mild, including tiredness (fatigue), weakness, pale skin, dizziness, and exercise-induced dyspnoea. These symptoms are most pronounced during childhood. Most IRIDA patients have normal growth and development [5]. IRIDA is usually suspected in childhood based on the results of routine blood tests. Diagnosis is according to laboratory tests showing hypochromic microcytic anaemia with low serum iron and transferrin saturation levels, and then the diagnosis is confirmed by genetic testing [6]. Treatment usually involves intravenous (IV) iron therapy [7].
IRIDA is a rare autosomal recessive disorder caused by mutations in the TMPRSS6 (transmembrane serine protease 6) gene [8]. The gene encodes a serine protease that plays an essential role in downregulating hepcidin, the key regulator of iron homeostasis [9,10,11], through the cleavage of the cell surface haemojuvelin BMP coreceptor (HJV), an activator of hepcidin expression [12,13,14,15]. The TMPRSS6 gene, located on chromosome 22, spans 18 exons and comprises 51,125 base pairs, encoding a protein of 802 amino acids. Since 2008, more than 100 TMPRSS6 variants have been identified in patients with IRIDA [16,17,18]. (The full paper list and full variant list are available in the Science Data Bank (ScienceDB) repository).
As high-throughput sequencing technology has evolved, re-evaluation guidelines for interpreting and classifying the pathogenicity of identified variants have been implemented. In addition, large-scale population databases have become widely available and can be used for assessment of genetic variants in rare diseases. In fact, for several diseases, there is evidence that these databases have improved the interpretation and classification of variants in patients with monogenic disease and allowed better prediction of which variants are likely to cause disease. The most widely used large-scale reference dataset is from Genome Aggregation Database (gnomAD), which consists of exome sequencing and genome sequencing data from unrelated individuals of diverse ancestries [19].
The World Health Organization (WHO) defines anaemia as a condition in which the number of red cells is insufficient to meet the body’s physiological needs. Iron deficiency anaemia (IDA) is the most common cause of anaemia worldwide. Although iron deficiency anaemia is relatively common [3], IRIDA is rare. Although its prevalence is unknown, the Orphanet database (https://www.orpha.net/consor/cgi-bin/index.php) estimates is to be less than 1 per 1 million. We attempted to obtain a more reliable estimate of the prevalence and carrier frequency of IRIDA from the Genome Aggregation Database (gnomAD) dataset using a previous protocol [20]. Additionally, we aimed to generate a curated artificial intelligence training dataset of TMPRSS6 variants for pathogenicity classification and interpretation.
Methods
Identification of previously reported TMPRSS6 disease-causing variants
To evaluate the genetic spectrum of IRIDA, a comprehensive search was performed to identify all previously reported disease-causing TMPRSS6 gene variants. Searches were conducted in the PubMed or Scopus database using the following combinations of search terms: iron deficiency anaemia, iron deficiency, iron-refractory iron deficiency anaemia, iron-refractory iron deficiency anaemia, Matriptase-2 (MT2), tmprss6, transmembrane serine protease 6, IRIDA, mutations, variants, variations, and mutants.
Two independent authors screened publications according to inclusion and exclusion criteria: original case reports reporting disease-causing variants of the TMPRSS6 gene were included, and variants in abstract, full-text, tables, figures, or supplementary figures and tables were extracted. Non-English-language articles, reviews, comments, editorials, letters, etc., and in vitro and animal model studies were excluded. Common TMPRSS6 polymorphisms associated with iron deficiency/iron deficiency anaemia in genome-wide association studies were also excluded.
All publications were saved in Medline format and stored in the MySQL and MongoDB databases using NCBI Entrez Programming Utilities [17] (E-utilities) with the Python package biopython [18] and MySQL/MongoDB database implementation.
Reported TMPRSS6 variants were also identified from Leiden Open Variation Database (LOVD) (https://www.lovd.nl/), NCBI [21] ClinVar (https://www.ncbi.nlm.nih.gov/clinvar/), dbSNP (https://www.ncbi.nlm.nih.gov/snp/), VarSome [22] (https://varsome.com/), Ensembl [23] (https://www.ensembl.org/) UniProtKB [24] (https://www.uniprot.org/), Genomenon Mastermind [25] (https://mastermind.genomenon.com/), LitVar [26] (https://www.ncbi.nlm.nih.gov/research/litvar2/), Online Mendelian Inheritance in Man (OMIM) (https://www.omim.org/) and HGMD (http://www.hgmd.cf.ac.uk/ac/index.php).
Prediction and functional annotation for all TMPRSS6 potential nonsynonymous single-nucleotide variants (nsSNVs) were compiled using dbNSFP 4 [27].
Identification and prediction of novel TMPRSS6 disease-causing variants
The gnomAD database (https://gnomad.broadinstitute.org/) was searched for novel disease-causing TMPRSS6 variants that had not yet been reported, and protein-truncating variants (PTVs) were examined (frameshifts, stop codons, initiator codons, splice donors and splice acceptors).
Interpretation of the pathogenicity of TMPRSS6 variants
The pathogenicity of variants was interpreted following the protocol by Zhang et al.[28] The pathogenicity of all missense, synonymous, and protein-truncating TMPRSS6 variants was classified according to Standards and Guidelines of the American College of Medical Genetics and Genomics (ACMG) and the Association for Molecular Pathology (AMP) [29] with the ClinGen Variant Curation Interface [30].
For missense and synonymous variants, we performed additional literature retrieval to curate in vitro or in vivo functional studies supportive of a damaging effect on TMPRSS6 missense/synonymous variants.
Variants classified as pathogenic and likely pathogenic were included. Variants classified as benign, likely benign, or uncertain significance were excluded. Pathogenic/likely pathogenic variants were included in the carrier frequency and genetic prevalence calculation.
Annotation of variants with minor allele frequencies (MAFs)
Each identified variant was normalized with HGVS nomenclature, SPDI [31], VCF, ClinVar, ClinGen Allele Registry [32], and dbSNP Reference SNP (rs or RefSNP) using Mutalyzer [33] (https://mutalyzer.nl/), NCBI Entrez Programming Utilities (E-utilities), VariantValidator [34] (https://variantvalidator.org/) and Ensembl REST API (https://rest.ensembl.org/).
The canonical TMPRSS6 transcript (NM_001374504.1, 3,265 bp) and protein (NP_001361433.1, 802 aa) selected by Matched Annotation from NCBI and EMBL-EBI (MANE) [35] differ from the 811 aa isoform in the literature. The difference between the two isoforms is that translation is initiated at an alternate start codon MLLLFHSKRM [36].
gnomAD v2.1.1 VCF files in Parquet format were downloaded from Microsoft Azure Open Datasets with the Microsoft AzCopy tool. The minor allele frequency of the gnomAD population for the following ethnic groups were retrieved with Apache Drill, Apache Spark, and Apache Zeppelin: African/African American (AFR), American Admixed/Latino (AMR), East Asian (EAS), Non-Finish European (NFE) and South Asian (SAS).
Carrier frequency and genetic prevalence calculation
The carrier frequency and genetic prevalence of IRIDA were calculated based on the Hardy–Weinberg equation [37]. For a monogenic autosomal recessive disorder, the genetic prevalence is \([1-{\prod }_{i}(1-{q}_{i}){]}^{2}\) based on the theory of probability, where qi stands for each pathogenic/likely pathogenic variant minor allele frequency. The genetic prevalence was approximately equal to \((\sum {q}_{i}{)}^{2}\), and the carrier frequency was \(2(1-\sum {q}_{i})\sum {q}_{i}\approx 2\sum {q}_{i}\). The disease prevalence was estimated by using the observed allele frequency of a pathogenic/likely pathogenic variant in the gnomAD database as the direct estimator for qi. The disease prevalence can be estimated by \({[1-{\prod }_{i}(1-\frac{{AC}_{i}}{{AN}_{i}})]}^{2}\approx \sum {AF}_{i}^{2}\), where AC is the allele count, AN is the corresponding allele number and AF is the corresponding allele frequency.
The Python statistics package statsmodels and scientific computing package NumPy and pandas were employed for calculating the 95% confidence interval (95% CI) for the binomial proportion of carrier frequency and the genetic prevalence with the Wilson Score interval. Graphics were plotted using the R graphic package ggplot2.
Results
Identification of TMPRSS6 missense, synonymous and protein-truncating variants
Comprehensive retrieval of IRIDA disease-causing variants resulted in the identification of 813 articles, of which 39 were considered eligible according to the exclusion and inclusion criteria. All disease-causing variant ETL pipelines and tools are shown in Fig. 1. From these articles, 86 disease-causing variants in the TMPRSS6 gene, including 40 missense variants and 46 protein-truncating variants (PTVs), are classified as pathogenic/likely pathogenic according to the Standards and guidelines of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology (missense variants are shown in Table 1; all variants are listed in the Science Data Bank (ScienceDB) online data repository). The most common mutation consequence is missense, accounting for 46.5% (40/86) of all pathogenic/likely pathogenic variants and more than half of the total allele frequency.

ETL pipeline of curation and classification of TMPRSS6 pathogenic/likely pathogenic variants. Extract: variants from literature retrieval and database search. Transformation: raw variant normalized HGVS nomenclature and curated. Load: based on the Hardy-Weinberg equation and binomial distribution model calculation
One synonymous variant (c.1086G > A/c.1086G > T, p.Thr362 =) is classified as likely pathogenic [38] (PP3, PP4, PM2, and PS3 criteria). However, this variant was excluded from the gnomAD dataset because of low confidence pLoF.
Forty-six protein-truncating variants were divided into three categories: frameshift (n = 20), nonsense (n = 17), and splice acceptor/donor (n = 9). PTVs accounted for more than half of the number of pathogenic/likely pathogenic variants after filtering (low confidence pLoF, LCR, Not LoF) but less than half of the total allele frequency.
Estimation of population prevalence and the carrier frequency of IRIDA
Pooling of the allele frequencies for all pathogenic/likely pathogenic variants provided a global minor allele frequency of 0.001, which is equivalent to a genetic prevalence of 1.0228 per 1 million (95% CI: [0.82, 1.28]) and a carrier frequency of 2.02 per 1 thousand (95% CI: [1.8, 2.28]). The African population had the highest prevalence, at 3.55 per million (95% CI: [1.76, 7.18]), with carrier frequency at 3.77 per thousand. Both non-Finish European and East Asian populations had a prevalence of greater than 1 per million, whereas the prevalence of American/Admixed Latino and South Asian populations was smaller than 1 per million. Ashkenazi Jewish and Finnish populations were not analysed because the sample size was too small to be calculated (Table 2 and Fig. 2).

Genetic prevalence and carrier frequency of IRIDA. A IRIDA genetic prevalence estimated from gnomAD allele frequencies. B IRIDA carrier frequency among diverse population. African/African American (afr), American Admixed/Latino (amr), Ashkenazi Jewish (asj), East Asian (eas), Finnish(fin), Non Finnish European (nfe) and South Asian (sas), other (oth)
Discussion
IRIDA is a rare autosomal recessive disorder caused by homozygous or compound heterozygous mutations in the transmembrane serine protease 6 (TMPRSS6) gene. IRIDA patients have microcytic hypochromic anaemia, low serum iron, and transferrin saturation. The prevalence is unknown. In this study, we sought to estimate the prevalence of IRIDA using 100 k-scale population genome data and to deepen our understanding of TMPRSS6 genetic variation. Using gnomAD data, we found that IRIDA affects 1.0228 per 1 million in the global population, which is higher than previous Orphanet database estimates of less than 1 per 1 million.
The main strength of this study was the use of 86 TMPRSS6 variants from a population of more than 100 k for prevalence estimates. In addition, we produced a curated variant dataset for TMPRSS6 that will be useful for further artificial intelligence-based classification of germline variant pathogenicity.
IRIDA can be difficult to distinguish from acquired iron deficiency unresponsive to oral iron therapy [39]. Overall, IRIDA is a genotypically and phenotypically heterogeneous disease. Allelic TMPRSS6 mutations are found in most patients with IRIDA. An algorithm has been developed based on blood and plasma values to distinguish patients with IRIDA resulting from biallelic TMPRSS6 mutations [40,41,42].
Combined heterozygous mutations in TMPRSS6 and activin A receptor type 1 (ACVR1) have been reported to cause IRIDA [43]. High hepcidin expression in the proband was reported with ACVR1 R258S and TMPRSS6 I212T. This digenic model suggests that combined heterozygous mutations in TMPRSS6 and other BMP/SMAD signalling pathway genes are likely to cause IRIDA. This may explain index cases in which there is only one pathogenic mutation and one or more single-nucleotide polymorphism combination.
TMPRSS6 polymorphisms are more frequent than germline TMPRSS6 mutations, and common TMPRSS6 variants are associated with erythrocyte traits, including haemoglobin concentration (Hb), haematocrit (Hct), mean corpuscular volume (MCV), mean corpuscular haemoglobin (MCH), mean corpuscular haemoglobin concentration (MCHC) and red blood cell (RBC) count [44, 45]. Additionally, TMPRSS6 polymorphisms in iron deficiency anaemia are partially responsive to oral iron treatment [46, 47]. A 3-tier classification system for variants of the TMPRSS6 gene has been proposed to better understand and define the IRIDA spectrum [48].
Synonymous mutations are also called neutral or silent mutations. Synonymous mutations in protein-coding genes do not alter protein sequences and are thus generally presumed to be neutral. Shen et al. constructed 8,341 yeast mutants and measured their fitness relative to wildtype. They found that three-quarters of synonymous mutations resulted in a significant reduction in fitness; the distribution of fitness effects was overall similar, albeit nonidentical [49].
IRIDA is not on the first national list of rare diseases issued by China, and the prevalence of IRIDA in China has not been estimated [50]. The National Rare Diseases Registry System (NRDRS) has not registered any IRIDA cases [51]. We demonstrated the power and limitations of the 100 k population genome database [52, 53] to calculate the prevalence of rare diseases, but gnomAD and the Trans-Omics for Precision Medicine (TOPMed) population are of predominantly non-Asian ancestry. The Chinese population genome project will fill this gap. Currently, NyuWa [54], Westlake BioBank for Chinese (WBBC) [55], and PGG. Han [56], China Metabolic Analytics Project (ChinaMAP) [57] have been released. We will estimate the prevalence of IRIDA and other rare diseases through the aggregation of Chinese population genome data.
The number of TMPRSS6 curated variants in the ClinVar database is far less than the number of variants we manually curated, and the state-of-the-art model EVE (evolutionary model of variant effect) uses the ClinVar dataset as the training set [58]. ClinGen Variant Curation Expert Panels (VCEPs) [59] define biocuration application of ACMG/AMP guidelines for sequence variant interpretation for specific genes or diseases. Additionally, the ClinGen Variant Curation Interface [30] is a variant classification platform for the application of evidence criteria from ACMG/AMP guidelines for curating variant classifications.
In conclusion, through a comprehensive analysis of genetic variation in TMPRSS6, we expanded our recognition of disease-causing mutations to 86 variants. IRIDA is a rare disease, and these data can help clinicians to diagnose IRIDA that is unlikely to represent a significant proportion of patients presenting with refractory iron deficiency or iron-deficiency anaemia.
Availability of data and materials
The datasets are available online in the Science Data Bank (ScienceDB) repository. https://doi.org/10.11922/sciencedb.01515.
Abbreviations
- TMPRSS6 :
-
Transmembrane serine protease 6
- IRIDA:
-
Iron refractory iron deficiency anaemia
- MAF:
-
Minor allele frequency
- ClinGen:
-
Clinical Genome
- NCBI:
-
National center for biotechnology information
- ACMG:
-
American college of medical genetics and genomics
- AMP:
-
Association for molecular pathology
- VCEP:
-
Variant curation expert panel
- CI:
-
Confidence interval
- gnomAD:
-
Genome aggregation database
- ID:
-
Iron deficiency
- IDA:
-
Iron deficiency anaemia
- PTVs:
-
Protein-truncating variants
- AC:
-
Allele count
- AF:
-
Allele frequency
- AN:
-
Allele number
References
Camaschella C. Iron-deficiency anemia. N Engl J Med. 2015;372(19):1832–43.
Camaschella C. Iron deficiency. Blood. 2019;133(1):30–9.
Pasricha SR, Tye-Din J, Muckenthaler MU, Swinkels DW. Iron deficiency. Lancet. 2021;397(10270):233–48.
Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L. Iron deficiency anaemia. Lancet. 2016;387(10021):907–16.
De Falco L, Sanchez M, Silvestri L, Kannengiesser C, Muckenthaler MU, Iolascon A, Gouya L, Camaschella C, Beaumont C. Iron refractory iron deficiency anemia. Haematologica. 2013;98(6):845–53.
Fletcher A, Forbes A, Svenson N, Wayne Thomas D. Guideline for the laboratory diagnosis of iron deficiency in adults (excluding pregnancy) and children. Br J Haematol. 2022;196(3):523–9.
Snook J, Bhala N, Beales ILP, Cannings D, Kightley C, Logan RP, Pritchard DM, Sidhu R, Surgenor S, Thomas W, et al. British Society of Gastroenterology guidelines for the management of iron deficiency anaemia in adults. Gut. 2021;70(11):2030–51.
Ramsay AJ, Hooper JD, Folgueras AR, Velasco G, Lopez-Otin C. Matriptase-2 (TMPRSS6): a proteolytic regulator of iron homeostasis. Haematologica. 2009;94(6):840–9.
Du X, She E, Gelbart T, Truksa J, Lee P, Xia Y, Khovananth K, Mudd S, Mann N, Moresco EM, et al. The serine protease TMPRSS6 is required to sense iron deficiency. Science. 2008;320(5879):1088–92.
Silvestri L, Pagani A, Nai A, De Domenico I, Kaplan J, Camaschella C. The serine protease matriptase-2 (TMPRSS6) inhibits hepcidin activation by cleaving membrane hemojuvelin. Cell Metab. 2008;8(6):502–11.
Folgueras AR, de Lara FM, Pendas AM, Garabaya C, Rodriguez F, Astudillo A, Bernal T, Cabanillas R, Lopez-Otin C, Velasco G. Membrane-bound serine protease matriptase-2 (Tmprss6) is an essential regulator of iron homeostasis. Blood. 2008;112(6):2539–45.
Ganz T. Systemic iron homeostasis. Physiol Rev. 2013;93(4):1721–41.
Silvestri L, Guillem F, Pagani A, Nai A, Oudin C, Silva M, Toutain F, Kannengiesser C, Beaumont C, Camaschella C, et al. Molecular mechanisms of the defective hepcidin inhibition in TMPRSS6 mutations associated with iron-refractory iron deficiency anemia. Blood. 2009;113(22):5605–8.
Wang CY, Babitt JL. Liver iron sensing and body iron homeostasis. Blood. 2019;133(1):18–29.
Camaschella C, Nai A, Silvestri L. Iron metabolism and iron disorders revisited in the hepcidin era. Haematologica. 2020;105(2):260–72.
Finberg KE, Heeney MM, Campagna DR, Aydinok Y, Pearson HA, Hartman KR, Mayo MM, Samuel SM, Strouse JJ, Markianos K, et al. Mutations in TMPRSS6 cause iron-refractory iron deficiency anemia (IRIDA). Nat Genet. 2008;40(5):569–71.
Melis MA, Cau M, Congiu R, Sole G, Barella S, Cao A, Westerman M, Cazzola M, Galanello R. A mutation in the TMPRSS6 gene, encoding a transmembrane serine protease that suppresses hepcidin production, in familial iron deficiency anemia refractory to oral iron. Haematologica. 2008;93(10):1473–9.
Guillem F, Lawson S, Kannengiesser C, Westerman M, Beaumont C, Grandchamp B. Two nonsense mutations in the TMPRSS6 gene in a patient with microcytic anemia and iron deficiency. Blood. 2008;112(5):2089–91.
Karczewski KJ, Francioli LC, Tiao G, Cummings BB, Alföldi J, Wang Q, Collins RL, Laricchia KM, Ganna A, Birnbaum DP, et al. The mutational constraint spectrum quantified from variation in 141,456 humans. Nature. 2020;581(7809):434–43.
Zhao T, Fan S, Sun L. The global carrier frequency and genetic prevalence of Upshaw-Schulman syndrome. BMC Genom Data. 2021;22(1):50.
Sayers EW, Bolton EE, Brister JR, Canese K, Chan J, Comeau DC, Connor R, Funk K, Kelly C, Kim S, et al. Database resources of the national center for biotechnology information. Nucleic Acids Res. 2022;50(D1):D20–6.
Kopanos C, Tsiolkas V, Kouris A, Chapple CE, Albarca Aguilera M, Meyer R, Massouras A. VarSome: the human genomic variant search engine. Bioinformatics. 2019;35(11):1978–80.
Cunningham F, Allen JE, Allen J, Alvarez-Jarreta J, Amode MR, Armean IM, Austine-Orimoloye O, Azov AG, Barnes I, Bennett R, et al. Ensembl 2022. Nucleic Acids Res. 2022;50(D1):D988–95.
UniProt C. UniProt: the universal protein knowledgebase in 2021. Nucleic Acids Res. 2021;49(D1):D480–9.
Chunn LM, Nefcy DC, Scouten RW, Tarpey RP, Chauhan G, Lim MS, Elenitoba-Johnson KSJ, Schwartz SA, Kiel MJ. Mastermind: a comprehensive genomic association search engine for empirical evidence curation and genetic variant interpretation. Front Genet. 2020;11: 577152.
Lee K, Wei CH, Lu Z. Recent advances of automated methods for searching and extracting genomic variant information from biomedical literature. Brief Bioinform. 2021;22(3):bbaa142.
Liu X, Li C, Mou C, Dong Y, Tu Y. dbNSFP v4: a comprehensive database of transcript-specific functional predictions and annotations for human nonsynonymous and splice-site SNVs. Genome Med. 2020;12(1):103.
Zhang J, Yao Y, He H, Shen J. Clinical interpretation of sequence variants. Curr Protoc Hum Genet. 2020;106(1): e98.
Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, Grody WW, Hegde M, Lyon E, Spector E, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17(5):405–24.
Preston CG, Wright MW, Madhavrao R, Harrison SM, Goldstein JL, Luo X, Wand H, Wulf B, Cheung G, Mandell ME, et al. ClinGen Variant Curation Interface: a variant classification platform for the application of evidence criteria from ACMG/AMP guidelines. Genome Med. 2022;14(1):6.
Holmes JB, Moyer E, Phan L, Maglott D, Kattman B. SPDI: data model for variants and applications at NCBI. Bioinformatics. 2020;36(6):1902–7.
Pawliczek P, Patel RY, Ashmore LR, Jackson AR, Bizon C, Nelson T, Powell B, Freimuth RR, Strande N, Shah N, et al. ClinGen allele registry links information about genetic variants. Hum Mutat. 2018;39(11):1690–701.
Lefter M, Vis JK, Vermaat M, den Dunnen JT, Taschner PEM, Laros JFJ. Next generation HGVS nomenclature checker. Bioinformatics. 2021;37(18):2811–7.
Freeman PJ, Hart RK, Gretton LJ, Brookes AJ, Dalgleish R. VariantValidator: accurate validation, mapping, and formatting of sequence variation descriptions. Hum Mutat. 2018;39(1):61–8.
Morales J, Pujar S, Loveland JE, Astashyn A, Bennett R, Berry A, Cox E, Davidson C, Ermolaeva O, Farrell CM, et al. A joint NCBI and EMBL-EBI transcript set for clinical genomics and research. Nature. 2022;604(7905):310–5.
Dion SP, Béliveau F, Désilets A, Ghinet MG, Leduc R. Transcriptome analysis reveals TMPRSS6 isoforms with distinct functionalities. J Cell Mol Med. 2018;22(4):2498–509.
Liu W, Pajusalu S, Lake NJ, Zhou G, Ioannidis N, Mittal P, Johnson NE, Weihl CC, Williams BA, Albrecht DE, et al. Estimating prevalence for limb-girdle muscular dystrophy based on public sequencing databases. Genet Med. 2019;21(11):2512–20.
Xiong Y, Wu Z, Yang W, Zhao X, Peng G, Tang K, Tian Z, Xing H, Rao Q, Wang M, et al. A novel splicing mutation of TMPRSS6 in a Chinese child with iron-refractory iron deficiency anaemia. Br J Haematol. 2015;171(4):647–9.
Hershko C, Camaschella C. How I treat unexplained refractory iron deficiency anemia. Blood. 2014;123(3):326–33.
Heeney MM, Guo D, De Falco L, Campagna DR, Olbina G, Kao PP, Schmitz-Abe K, Rahimov F, Gutschow P, Westerman K, et al. Normalizing hepcidin predicts TMPRSS6 mutation status in patients with chronic iron deficiency. Blood. 2018;132(4):448–52.
Donker AE, Schaap CC, Novotny VM, Smeets R, Peters TM, van den Heuvel BL, Raphael MF, Rijneveld AW, Appel IM, Vlot AJ, et al. Iron refractory iron deficiency anemia: a heterogeneous disease that is not always iron refractory. Am J Hematol. 2016;91(12):E482–90.
Girelli D, Nemeth E, Swinkels DW. Hepcidin in the diagnosis of iron disorders. Blood. 2016;127(23):2809–13.
Pagani A, Colucci S, Bocciardi R, Bertamino M, Dufour C, Ravazzolo R, Silvestri L, Camaschella C. A new form of IRIDA due to combined heterozygous mutations of TMPRSS6 and ACVR1A encoding the BMP receptor ALK2. Blood. 2017;129(25):3392–5.
Chambers JC, Zhang W, Li Y, Sehmi J, Wass MN, Zabaneh D, Hoggart C, Bayele H, McCarthy MI, Peltonen L, et al. Genome-wide association study identifies variants in TMPRSS6 associated with hemoglobin levels. Nat Genet. 2009;41(11):1170–2.
Benyamin B, Ferreira MA, Willemsen G, Gordon S, Middelberg RP, McEvoy BP, Hottenga JJ, Henders AK, Campbell MJ, Wallace L, et al. Common variants in TMPRSS6 are associated with iron status and erythrocyte volume. Nat Genet. 2009;41(11):1173–5.
Poggiali E, Andreozzi F, Nava I, Consonni D, Graziadei G, Cappellini MD. The role of TMPRSS6 polymorphisms in iron deficiency anemia partially responsive to oral iron treatment. Am J Hematol. 2015;90(4):306–9.
Buerkli S, Pei SN, Hsiao SC, Lee CT, Zeder C, Zimmermann MB, Moretti D. The <em>TMPRSS6</em> variant (SNP rs855791) affects iron metabolism and oral iron absorption - a stable iron isotope study in Taiwanese women. Haematologica. 2021;106(11):2897–905.
Sharma P, Bhatia P, Singh M, Das R, Jain R, Bansal D, Attri SV, Trehan A. A case series highlighting structured hematological, biochemical and molecular approach to clinical oral iron refractoriness in children: A pressing need for a 3-tier system for classification of variants in TMPRSS6 gene. Blood Cells Mol Dis. 2021;89: 102569.
Shen X, Song S, Li C, Zhang J: Synonymous mutations in representative yeast genes are mostly strongly non-neutral. Nature 2022.
Shi X, Liu H, Zhan S, Wang Z, Wang L, Dong C, Wang Y, Yao C, Ding J, Li Y. Rare diseases in China: analysis of 2014–2015 hospitalization summary reports for 281 rare diseases from 96 tertiary hospitals. Orphanet J Rare Dis. 2019;14(1):160.
Guo J, Liu P, Chen L, Lv H, Li J, Yu W, Xu K, Zhu Y, Wu Z, Tian Z, et al. National Rare Diseases Registry System (NRDRS): China’s first nation-wide rare diseases demographic analyses. Orphanet J Rare Dis. 2021;16(1):515.
Taliun D, Harris DN, Kessler MD, Carlson J, Szpiech ZA, Torres R, Taliun SAG, Corvelo A, Gogarten SM, Kang HM, et al. Sequencing of 53,831 diverse genomes from the NHLBI TOPMed Program. Nature. 2021;590(7845):290–9.
Karczewski KJ, Francioli LC, Tiao G, Cummings BB, Alfoldi J, Wang Q, Collins RL, Laricchia KM, Ganna A, Birnbaum DP, et al. The mutational constraint spectrum quantified from variation in 141,456 humans. Nature. 2020;581(7809):434–43.
Zhang P, Luo H, Li Y, Wang Y, Wang J, Zheng Y, Niu Y, Shi Y, Zhou H, Song T, et al. NyuWa genome resource: a deep whole-genome sequencing-based variation profile and reference panel for the Chinese population. Cell Rep. 2021;37(7): 110017.
Cong P-K, Bai W-Y, Li J-C, Yang M-Y, Khederzadeh S, Gai S-R, Li N, Liu Y-H, Yu S-H, Zhao W-W, et al. Genomic analyses of 10,376 individuals in the Westlake BioBank for Chinese (WBBC) pilot project. Nat Commun. 2022;13(1):2939.
Gao Y, Zhang C, Yuan L, Ling Y, Wang X, Liu C, Pan Y, Zhang X, Ma X, Wang Y et al: PGG.Han: the Han Chinese genome database and analysis platform. Nucleic Acids Res 2020, 48(D1):D971-d976.
Cao Y, Li L, Xu M, Feng Z, Sun X, Lu J, Xu Y, Du P, Wang T, Hu R, et al. The ChinaMAP analytics of deep whole genome sequences in 10,588 individuals. Cell Res. 2020;30(9):717–31.
Frazer J, Notin P, Dias M, Gomez A, Min JK, Brock K, Gal Y, Marks DS. Disease variant prediction with deep generative models of evolutionary data. Nature. 2021;599(7883):91–5.
Rivera-Muñoz EA, Milko LV, Harrison SM, Azzariti DR, Kurtz CL, Lee K, Mester JL, Weaver MA, Currey E, Craigen W, et al. ClinGen variant curation expert panel experiences and standardized processes for disease and gene-level specification of the ACMG/AMP guidelines for sequence variant interpretation. Hum Mutat. 2018;39(11):1614–22.
Acknowledgements
We acknowledge Genome Aggregation Database (gnomAD).
Funding
This study was supported by Yunnan Fundamental Research Projects (Grant No. 202101AU070007). The funding bodies had no role in the design of the study; the collection, analysis, and interpretation of data; or in writing the manuscript.
Author information
Authors and Affiliations
Contributions
FSH and ZT retrieved the literature and wrote the manuscript text, and SL designed the project and revised the manuscript and data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fan, S., Zhao, T. & Sun, L. The global prevalence and ethnic heterogeneity of iron-refractory iron deficiency anaemia. Orphanet J Rare Dis 18, 2 (2023). https://doi.org/10.1186/s13023-022-02612-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13023-022-02612-2