
Abstract
Background
Pituitary stalk interruption syndrome (PSIS) is a rare disease caused by congenital pituitary anatomical defects. The underlying mechanisms remain unclear, and the diagnosis is difficult. Here, integrated metabolomics and lipidomics profiling were conducted to study the pathogenesis of PSIS.
Methods
Twenty-one patients with PSIS (BD group) and twenty-three healthy controls (HC group) were enrolled. Basal information and seminal plasma samples were collected. Untargeted metabolomics and lipidomics analyses were performed using ultraperformance liquid chromatography-quadrupole time-of-flight mass spectrometry (UPLC-QTOF-MS).
Results
The metabolomics and lipidomics profiles of patients with PSIS changed. The prolactin signaling pathway and biosynthesis of amino acids were the main differentially modified metabolic pathways. The main differentially modified metabolites were triacylglycerols (TGs), phosphatidylethanolamine (PE), sphingomyelin (SM), ceramide (Cer) and phosphatidylcholines (PCs). Pregnenolones and L-saccharopine could achieve a diagnosis of PSIS.
Conclusions
Pregnenolones and L-saccharopine are potential biomarkers for a PSIS diagnosis.
Similar content being viewed by others


Introduction
Pituitary stalk interruption syndrome (PSIS) is a clinical syndrome characterized by the lack or thinning of the pituitary stalk, pituitary hypoplasia, and/or ectopic neurohypophysis. PSIS is a rare disease with an incidence of 1 in 200 000 [1]. Hormones secreted by the hypothalamus cannot be transported to the anterior and posterior pituitary through the pituitary portal system due to the interrupted pituitary stalk. Defects in growth and pubertal development are the main clinical manifestations. Hormone replacement therapy is required to promote sexual development, maintain sexual function and induce spermatogenesis [2, 3]. The diagnosis of PSIS is challenging, and magnetic resonance imaging (MRI) may be useful [4,5,6].
Metabolomics is commonly used to simultaneously analyze all metabolites in organisms. It helps identify the relationships between metabolites and pathological changes. Most of its research objects are small molecular substances with a molecular mass of less than 1000 Da [7]. Many biomarkers for diagnosis and monitoring therapy have been developed using this method. Previous studies of seminal plasma from infertile men show that metabolites, such as amino acids and fatty acids, are potential biomarkers [8, 8,9,10]. Therefore, we aimed to identify biomarkers of PSIS by metabolomics analysis, which may help improve the therapeutic effects on spermatogenesis. Here, integrated metabolomics and lipidomics analyses were performed to identify the specific metabolites associated with PSIS.
Materials and methods
Participants
In this study, 21 patients with PSIS (BD group) and 23 healthy controls (HC group) according to the 5th edition of the WHO Manual for the Laboratory Examination and Processing of Human Semen were recruited from Peking Union Medical College Hospital (PUMCH) from January 2020 to March 2021. The diagnostic criteria included (a) growth hormone deficiency and (b) a triad of an absent or thin pituitary stalk, pituitary hypoplasia, and/or ectopic neurohypophysis visible on magnetic resonance imaging (MRI). All patients and HCs enrolled were of Han Chinese ethnicity. The sample should be collected after a minimum of 2 days and a maximum of 7 days of sexual abstinence. If additional samples are required, the number of days of sexual abstinence should be as constant as possible at each visit.. All sex hormones were measured using an automated chemiluminescence immunoassay analyzer (Beckman Coulter UniCel DXI 800, Beckman Coulter; Brea, CA, USA). Sperm motility and concentration assessments were performed using computer-assisted sperm analysis systems (Suiplus SSA-II, Suiplus Software Co. Ltd.; Beijing, China). The microscope used with SSA-II was a Nikon 80i with a 20phase objective. The baseline information of all participants is listed in Table 1. Sample collection and laboratory parameters are described in Additional file 1: S1.
Materials and instruments
Chromatographic grade ammonium fluoride, 2-propanol, ammonium acetate, formic acid, ammonium hydroxide, ammonium formate, acetonitrile, and methyl tert-butyl ether (MTBE) were obtained from Sigma Aldrich. Mass spectrometry grade methanol was purchased from Thermo Fisher. The Q-Exactive Plus Orbitrap LC–MS/MS System was from Thermo Scientific. AB Triple TOF 6600 was purchased from AB Sciex (Massachusetts, USA). The Nexera LC-30A liquid chromatography system was from SHIMADZU. An ACQUITY UPLC BEH Amide column (1.7 μm, 2.1 mm × 100 mm) and ACQUITY UPLC CSH C18 column (1.7 µm, 2.1 mm × 100 mm) were obtained from Waters Corporation (Milford, MA, USA).
Sample preparation for metabolomics and lipidomics profiling
For metabolomics profiling, the seminal plasma sample was extracted by methanol/acetonitrile. In brief, precooled methanol/acetonitrile/water solution (2:2:1, v/v) was mixed with 10 μL of the sample and sonicated for 30 min. The samples were centrifuged at 14,000 × g for 20 min at 4 °C to obtain the supernatant. Then, it was dried in a vacuum centrifuge and redissolved in 100 μL acetonitrile/water (1:1, v/v). The samples were centrifuged at 14,000 × g for 15 min, and the supernatant was used for the analysis.
For lipidomics profiling, 240 μL precooled methanol, 200 μL water and 20 μL internal lipid standard mixture were homogenized with the seminal plasma sample. MTBE (800 μL) was added and sonicated for 20 min. Then, the samples were centrifuged at 14,000 × g for 15 min to obtain the supernatant. After drying under nitrogen, the samples were redissolved in 200 μL of 90% isopropanol/acetonitrile solution and centrifuged at 14,000 × g for 15 min. The final supernatant was used for lipidomics analysis. The whole process was performed under refrigeration.
Quality control
Equal amounts of the supernatants from the seminal plasma samples were mixed to prepare the quality control (QC) sample. The QC sample was used to determine the instrument state and evaluate the system’s stability during the entire experiment.
Mass spectrometry data acquisition and processing
A quadrupole time-of-flight 6600 (AB Sciex) was used for metabolomics data acquisition. Lipidomics data acquisition was performed using a Q-Exactive Plus Orbitrap LC–MS/MS System (Thermo Scientific). The gradients of both separations and the ESI source conditions are described in Supporting Information S2 and S3. Further information on both the separations and ESI source conditions is shown in Additional file 1: S2 and S3.
The metabolomics raw MS data were processed using ProteoWizard and XCMS software. The lipidomics raw MS data were processed using Lipid Search, including peak identification, peak extraction, and lipid identification (secondary identification). Further information is shown in Additional file 1: S4.
Statistical analysis
Data with a normal distribution are expressed as the mean (SD). Statistical analysis was performed using the R package. Student’s t-test at the univariate level was used to measure the significance of the metabolites, and p values < 0.05 were considered significant. MetaboAnalyst 5.0 (Xia Lab @ McGill Sweden) was used to perform chemometrics, cluster and biomarker analyses.
Results
Clinical characteristics of the patients with PSIS
All of the patients with PSIS had a history of malpresentation (100%). They were 24.6 ± 4.9 years old. Combined gonadotropins (HCG/HMT) were administered for 18 ± 6 months to induce spermatogenesis.The patients did not take other medications such as psychotropic drugs, which may interfere with the results of metabolomics and lipidomics profiling [11]. All of them experienced erections and seminal fluid production. Nonliquefaction occurred in 10/21 (47.6%) samples, and condensed semen occurred in 9/21 (42.8%) samples. Patients with PSIS had a smaller testicular volume (PSIS Group 5.9 ± 2.6 ml vs. HC Group 13.5 ± 3.1 ml), lower sperm counts (PSIS Group 20.4 ± 29.4 × 106 vs. HC Group 229.4 ± 118.6 × 106), sperm concentrations (PSIS Group 8.7 ± 13.2 × 106/mL vs. HC Group 96.1 ± 55.2 × 106/mL) and sperm motility (PSIS Group 33.9 ± 28.1% vs. HC Group 69.7 ± 12.3%). Patients with PSIS had lower levels of luteinizing hormone (LH) (PSIS Group 0.38 ± 0.59 IU/L vs. HC Group 3.59 ± 1.57 IU/L), serum follicle-stimulating hormone (FSH) (PSIS Group 1.29 ± 1.47 IU/L vs. HC Group 6.43 ± 4.34 IU/L) and testosterone (T) (PSIS Group 1.85 ± 1.03 ng/mL vs. HC Group 8.4 ± 12.7 ng/mL) (Table 1).
Metabolomics and lipidomic profiling of seminal plasma
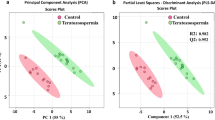
Using a UPLC–MS approach, we analyzed the metabolomics and lipidomic profiles of patients with PSIS. To characterize the differences, orthogonal projections to latent structures-discriminant analysis (OPLS-DA) plots were generated (Fig. 1A, Fig. 2A). As shown in our OPLS-DA charts, the PSIS and HC groups were separated in both ion modes. Many metabolites were decreased in patients with PSIS, as the colored dots in the volcano plot indicate significantly different molecules (Figs. 1B, 2B). The criteria were set as variable importance in the projection (VIP) > 1 and p < 0.05 (Student’s t-test).

(A) OPLS-DA model of metabolomics in ESI + ionization mode. (B) Volcano plot of metabolomics in ESI + ionization mode

(A) OPLS-DA model of lipidomics for PSIS (BD group, green) vs. control (HC, blue). (B) Volcano plot of lipidomics for PSIS (BD group) vs. HC
As Fig. 3A shows, in the metabolomics profiles, metabolites were significantly different among the different groups (Additional file 1: Table S1). Many lipid species, such as triacylglycerol (TG), sphingomyelin (SM), phosphatidylethanolamine (PE), phosphatidylcholines (PC), and ceramides (Cer), were decreased in the PSIS group (Fig. 3B, Additional file 1: Table S2). The KEGG pathway enrichment analysis showed that the prolactin signaling pathway and biosynthesis of amino acids were different in patients with PSIS (Fig. 4A). The size of the bubble indicates the P value, and the color indicates the significance of the enrichment degree. The overall changes in the pathway are shown in the differential abundance score (DAS) (Fig. 4B). The length represents the absolute value of the DA score, and the size indicates the number of metabolites. For lipid analysis, a bubble plot was used to display the significance of the differences and the classification information for different metabolites (Fig. 5). The size of the bubbles represents the significance of the differences (significant: 0.01 < p < 0.05; extremely significant: p < 0.01). As shown in Fig. 5, TG, SM, PE, PC and Cer were the main differential lipid molecules. The significantly different metabolites were identified with receiver operating characteristic (ROC) analysis. The diagnostic panel model was optimized by using multivariate exploratory ROC analysis. By combining PS and L-saccharopine, we achieved excellent differentiation of PSIS: PSIS vs. HC (AUC = 0.927, 95% Cl: 0.81–1) (Fig. 6).

(A) Heatmap of the top differential features in metabolomics. (B) Heatmap of the top different features in lipidomics

(A) KEGG enrichment analysis for the PSIS vs. HC groups. (B) Differential abundance score analysis for the PSIS vs. HC groups

Lipid group bubble plot for the PSIS vs. HC groups

The ROC curve of the panel generated by combining pregnenolone sulfate and L-saccharopine
Discussion
The baseline characteristics are after combined gonadotropins administration. The patients did not receive testosterone therapy before HCG/HMT treatment. This untargeted metabolomics and lipidomics study demonstrated that the prolactin signaling pathway and biosynthesis of amino acids were different in patients with PSIS. TGs, SM, PE, Cer and PCs were decreased in lipid profile analysis of the seminal fluid from PSIS patients.
TG is the core of lipoprotein and serves as an energy source for most tissues. Previous studies have shown that some kinds of fatty acids are potential biomarkers of semen quality [12]. Diacylglycerol (DG, DAG) is formed through the hydrolysis of TG. In our data, most DGs decreased in patients with PSIS, while DG(32:1e), DG(30:1e), and DG(21:5e) increased.
PC is the main component of biofilms, and it is composed of a hydrophilic head and a hydrophobic tail [13, 14]. PC(12:1e_20:0), PC(16:0_18:1), PC(16:0_20:1), PC(16:0_18:2), PC(36:1), PC(18:0_18:2), PC(18:0e_11:1), PC(18:1e_16:0), and PC(12:0e_23:1) were decreased in patients with PSIS. The changed composition and saturation of PC may impair the function of the membranes of sperm [13,14,15,16,17, 17, 18]. Phosphatidylethanolamine (PE) is the major component of these membranes.
In our data, most kinds of lipids decreased, which revealed a poor nutritional microenvironment. PE(16:1e_18:2), PE(18:1e_18:1), PE(18:0p_18:1), PE(16:1e_18:1), PE(16:0p_18:1), PE(18:0_16:0), PE(16:1e_22:6), PE(16:0_22:6), and PE(16:0_18:1) were the significantly different metabolites (Fig. 3B). The decreased PE may lead to inflammatory response disorders and cause semen nonliquefaction (13/21) and semen viscosity (12/21). The findings of our study support the results of a previous study showing that phosphatidylethanolamine binding protein 4 is a potential proteomic marker for semen quality [19, 20].
Cer is a metabolite of SM and it is the main component of the phospholipid bilayer sphingomyelin. SM(d38:2), SM(d40:2), SM(d36:1), SM(d34:1), SM(d42:1), and SM(d42:3) were significantly decreased in the patients with PSIS. Ceramide can participate in a variety of cell signaling pathways, such as cell growth, differentiation, and apoptosis. In our data, most kinds of lipids were decreased, which revealed the poor nutritional microenvironment [21, 22]. Patients with PSIS had a smaller testicular volume (PSIS Group 5.9 ± 2.6 ml vs. HC Group 13.5 ± 3.1 ml), lower sperm counts (PSIS Group 20.4 ± 29.4 × 106 vs. HC Group 229.4 ± 118.6 × 106), sperm concentrations (PSIS Group 8.7 ± 13.2 × 106/mL vs. HC Group 96.1 ± 55.2 × 106/mL) and sperm motility (PSIS Group 33.9 ± 28.1% vs. HC Group 69.7 ± 12.3%), which may be associated with the barren spermatogenesis microenvironment.
PS is a natural steroid synthesized from pregnenolone (P5), and it can be converted into endogenous steroid hormones such as progesterone (P4) and estrogen (E2). Neuroactive steroids synthesized directly in the brain are independent of peripheral sources and they rapidly alter neuronal excitability by binding to their receptors [23]. PS is endogenously present in the brain and is synthesized by glial cells, which modulate neurotransmission in various systems through presynaptic and postsynaptic mechanisms [24]. In addition, it can also promote sleep quality and improve memory, and it has many effects, such as anti-depression and anti-anxiety activity [25].
A previous study showed that PS could enhance prolactin (PRL) synthesis and secretion by triggering the activation of PKA, PKC and MAPK signaling. This is consistent with our data showing that the prolactin signaling pathway was the main differential metabolic pathway (Fig. 4B). PRL is a protein hormone secreted by anterior pituitary gland eosinophils that can promote the development and growth of mammary glands and stimulate the production of luteinizing hormone receptors. In our study, the patients with PSIS had lower LH (0.37 ± 0.57 IU/L vs. HC of 3.59 ± 1.57 IU/L), FSH (1.19 ± 1.49 IU/L vs. HC of 6.43 ± 4.34 IU/L) and T (1.74 ± 1.01 ng/mL vs. HC of 8.4 ± 12.7 ng/mL), which may be associated with their low level of PS.
Conclusions
This untargeted metabolomics and lipidomics profiling of seminal plasma showed that the prolactin signaling pathway and biosynthesis of amino acids were different in patients with PSIS, indicating the underlying mechanism of PSIS. Furthermore, most types of lipids, such as TG, PC, PE, SM and Cer, were decreased, revealing a poor nutritional microenvironment for spermatogenesis. Supplementation with these lipid metabolites may improve spermatogenesis, which needs to be verified in future studies.
Availability of data and materials
All data supporting the conclusions of this research article are included in the manuscript.
Abbreviations
- PSIS:
-
Pituitary stalk interruption syndrome
- MRI:
-
Magnetic resonance imaging
- TG:
-
Triacylglycerol
- PE:
-
Phosphatidylethanolamine
- SM:
-
Sphingomyelin
- Cer:
-
Ceramide
- PC:
-
Phosphatidylcholine
- FSH:
-
Follicle-stimulating hormone
- LH:
-
Luteinizing hormone
- T:
-
Testosterone
- E2:
-
Estradiol
- PRL:
-
Prolactin
- FT3:
-
Estradiol
- FT4:
-
Prolactin
- IGF1:
-
Insulin-like growth factor
- PR:
-
Progressive motility
- NP:
-
Non-progressive motility
References
Wang CZ, Guo LL, Han BY, Su X, Guo QH, Mu YM. Pituitary stalk interruption syndrome: from clinical findings to pathogenesis. J Neuroendocrinol. 2017;29(1).
Mao J, Xu H, Wang X, et al. Congenital combined pituitary hormone deficiency patients have better responses to gonadotrophin-induced spermatogenesis than idiopathic hypogonadotropic hypogonadism patients. Hum Reprod. 2015;30:2031–7.
Vergier J, Castinetti F, Saveanu A, Girard N, Brue T, Reynaud R. Diagnosis of endocrine disease: pituitary stalk interruption syndrome: etiology and clinical manifestations. Eur J Endocrinol. 2019;181(5):R199-209.
Argyropoulou MI, Kiortsis DN. MRI of the hypothalamic-pituitary axis in children. Pediatr Radiol. 2005;35:1045–55.
Di Iorgi N, Allegri AEM, Napoli F, Bertelli E, Olivieri I, Rossi A, Maghnie M. The use of neuroimaging for assessing disorders of pituitary development. Clin Endocrinol. 2012;76:161–76.
Pinto G, Netchine I, Sobrier ML, Brunelle F, Souberbielle JC, Brauner R. Pituitary stalk interruption syndrome: a clinicalbiological-genetic assessment of its pathogenesis. J Clin Endocrinol Metab. 1997;82:3450–4.
Nicholson JK, Lindon JC. Systems biology: metabonomics. Nature. 2008;455:1054–6.
Wu H, Xue R, Tang Z, et al. Metabolomic investigation of gastric cancer tissue using gas chromatography/mass spectrometry. Anal Bioanal Chem. 2010;396:1385–95.
Falsig AML, Gleerup CS, Knudsen UB. The influence of omega-3 fatty acids on semen quality markers: a systematic PRISMA review. Andrology. 2019;7(6):794–803.
Boguenet M, Bocca C, Bouet P-E, et al. Metabolomic signature of the seminal plasma in men with severe oligoasthenospermia. Andrology. 2020;8:1859–66.
Guo Y, Li X, Yan S, Li Y. Metabolomic alterations associated with Kallmann syndrome. Ann Transl Med. 2020;8(8):529.
Mazzilli R, Curto M, De Bernardini D, et al. Psychotropic drugs levels in seminal fluid: A new therapeutic drug monitoring analysis? Front Endocrinol (Lausanne). 2021;12: 620936.
Zerbinati C, Caponecchia L, Rago R, et al. Fatty acids profiling reveals potential candidate markers of semen quality. Andrology. 2016;4(6):1094–101.
Pietiläinen KH, Róg T, Seppänen-Laakso T, et al. Association of lipidome remodeling in the adipocyte membrane with acquired obesity in humans. PLoS Biol. 2011;9: e1000623.
Wymann MP, Schneiter R. Lipid signalling in disease. Nat Rev Mol Cell Biol. 2008;9:162–76.
Vorkas PA, Isaac G, Holmgren A, et al. Perturbations in fatty acid metabolism and apoptosis are manifested in calcific coronary artery disease: an exploratory lipidomic study. Int J Cardiol. 2015;197:192–9.
Vouk K, Ribič-Pucelj M, Adamski J, et al. Altered levels of acylcarnitines, phosphatidylcholines, and sphingomyelins in peritoneal fluid from ovarian endometriosis patients. J Steroid Biochem Mol Biol. 2016;159:60–9.
Zhao YY, Wang HL, Cheng XL, et al. Metabolomics analysis reveals the association between lipid abnormalities and oxidative stress, inflammation, fibrosis, and Nrf2 dysfunction in aristolochic acidinduced nephropathy. Sci Rep. 2015;5:12936.
Ried JS, Baurecht H, Stuckler F, et al. Integrative genetic and metabolite profiling analysis suggests altered phosphatidylcholine metabolism in asthma. Allergy. 2013;68:629–36.
Deepinder F, Chowdary HT, Agarwal A. Role of metabolomic analysis of biomarkers in the management of male infertility. Expert Rev Mol Diagn. 2007;7:351–8.
Bogatcheva NV, Sergeeva MG, Dudek SM, et al. Arachidonic acid cascade in endothelial pathobiology. Microvasc Res. 2005;69:107–27.
Zhu W, Zhang Y, Ren CH, et al. Identification of proteomic markers for ram spermatozoa motility using a tandem mass tag (TMT) approach. J Proteomics. 2020;210: 103438.
Mu H, Porsgaard T. The metabolism of structured triacylglycerols. Prog Lipid Res. 2005;44:430–48.
Masaki H, Kim N, Nakamura H, et al. Long-chain fatty acid triglyceride (TG) metabolism disorder impairs male fertility: a study using adipose triglyceride lipase deficient mice. Mol Hum Reprod. 2017;23(7):452–60.
Baulieu EE. Neurosteroids: a novel function of the brain. Psychoneuroendocrinology. 1998;23(8):963–87.
Bowlby MR. Pregnenolone sulfate potentiation of N-methyl-D-aspartate receptor channels in hippocampal neurons. Mol Pharmacol. 1993;43(5):813–9.
Reddy DS. Neurosteroids: endogenous role in the human brain and therapeutic potentials. Prog Brain Res. 2010;186:113–37.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Key Research and Development Program of China (2018YFE0207300) and Beijing Municipal Science & Technology Commission (Z211100002521021). This work is supported by the Beijing Key Clinical Specialty for Laboratory Medicine—Excellent Project (No. ZK201000).
Author information
Authors and Affiliations
Contributions
(I) Conception and design: X Li, Y Guo; (II) Administrative support: Y Li; (III) Provision of study materials or patients: Y Guo, G Luo, Y Si; (IV) Collection and assembly of data: X Li, Y Guo, X Wang; (V) Data analysis and interpretation: X Li; (VI) Manuscript writing: All authors; (VII) Final approval of the manuscript: All authors. All authors read and approved the final manuscript
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The collection of patient biospecimens was approved by the institutional committee that protects human subjects at PUMCH.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supporting information.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Guo, Y., Li, X., Wang, X. et al. Seminal plasma metabolomics and lipidomics profiling to identify signatures of pituitary stalk interruption syndrome. Orphanet J Rare Dis 17, 267 (2022). https://doi.org/10.1186/s13023-022-02408-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13023-022-02408-4