
Abstract
Objective
To study the influencing factors of myasthenic crisis in non-thymoma myasthenia gravis (MG) patients during perioperative period.
Methods
We retrospectively analyzed a total of 387 non-thymoma MG patients who underwent extended thymoma resection in the Department of Thoracic Surgery of Beijing Hospital from February 2011 to December 2021, recorded ASA score, Osserman classification, preoperative course, pyridostigmine dosage, operation method, operation time, and intraoperative blood loss, then analyzed the factors associated with postoperative myasthenic crisis by univariate and multivariate logistic regression.
Results
Osserman classification IIB + III + IV (P < 0.001), history of myasthenic crisis (P = 0.013), pyridostigmine dosage greater than 240 (P < 0.001), ASA score 2 and 3 (P = 0.001) are independent risk factors for myasthenic crisis.
Conclusion
Patients with poor Osserman classification, history of myasthenic crisis before surgery, larger preoperative dosage of pyridostigmine, and higher ASA scores should be highly alert to the occurrence of postoperative myasthenic crisis.
Similar content being viewed by others

Introduction
Myasthenia gravis (MG) is an autoimmune disease involving the neuromuscular junction. In 1672 Willis first described the clinical manifestations of MG patients, and in 1912 Saubruch found that thymectomy significantly improved the MG symptoms [1]. With the deepening understanding of myasthenia gravis, thymectomy has become an important part of the treatment. Five years after thymectomy, the complete stable remission rate of MG symptoms can reach more than 50% [2]. A prospective study [3] in 2016 confirmed with a higher level of evidence that MG patients could significantly benefit from thymectomy. Myasthenic crisis (MC) is the most dangerous complication of thymectomy, which can often significantly prolong the hospital stay, increase medical costs and even the risk of death. As the incidence of myasthenia gravis is very low (4.4–6.1/1 million) [4], there are few single-center studies with a large sample size, and it is difficult to unify the all kinds of criteria in meta-analysis with a large sample size [5]. It is also difficult to unify the standards of operation and perioperative management in multi-center studies. Due to the special MG ward in our hospital, there are many such patients, so comprehensive and massive data can be obtained, and the evaluation criteria of each patient are unified. We conducted this retrospective study in order to find out the risk factors of POMC, reduce the occurrence of POMC, or give early warning to avoid more serious complications caused by POMC.
Methods
Inclusion and Exclusion Criteria:
-
1.
Inclusion Criteria:
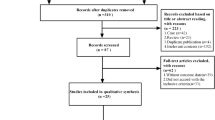
A total of 696 MG patients who was underwent thymectomy in Department of Thoracic Surgery, Beijing Hospital from February 2011 to December 2021.
-
2.
Exclusion Criteria:
-
a.
The patients without MG.
-
b.
The patients with thymoma.
-
a.
The surgical method was extended thymus resection, which included the whole thymus, the bilateral mediastinal fat and diaphragmatic angle fat. The en bloc resection was performed on the vast majority of patients, and the left and right thymus were removed separately only when the amount of tissue was extremely large and seriously obstructed the surgical field.
POMC should meet the following conditions: within one month after the operation, the patient needs endotracheal intubation or non-invasive ventilator assisted breathing for more than 24 h, or after the endotracheal intubation is removed but because of breathing weakness or inability to cough up intubated again.
All ASA scores were obtained by the same investigator excluding MG.
We investigated the preoperative, intraoperative and postoperative data. The preoperative data included: gender, age, other autoimmune diseases, history of myasthenic crisis, preoperative MG course, Osserman classification, preoperative pyridostigmine bromide dosage, immunosuppressants and glucocorticoid, comorbidities, ASA score, pulmonary function. The intraoperative data included: surgical methods, operation time, intraoperative blood loss. The postoperative data included: drainage volume over the first 3 days after operation, postoperative hospital stay, myasthenic crisis.
Statistical analyses were performed using IBM SPSS version 26.0 statistical software for Windows. All continuous data were presented as mean ± standard deviation and categorical variables were described using frequencies and percentage. The logistic regression analysis was applied for univariate and multivariate analysis to explore risk factors for POMC. Clinical factors that were found to have p values of < 0.10 in the univariate analysis were included in a stepwise multiple logistic regression analysis. The results were presented as odds ratios, 95% confidence intervals (CIs) and p value. All statistical tests were two-sided and P values < 0.05 was considered statistically significant.
Results
A total of 387 MG patients without thymoma (204 men, 183 women) were included in this study. The mean age was 45.9 years old (15–86 years). POMC occurred in 45 patients (11.6%).
The data of MG patients without thymoma are included as variables in logistic regression analysis in Table 1.
Logistic regression analysis is shown in Table 2. Univariate analysis showed age (P = 0.020), preoperative history of myasthenic crisis (P < 0.001), Osserman-stage IIB + III + IV (P < 0.001), preoperative daily dose of pyridostigmine bromide ≥ 240 mg (P < 0.001), ASA grade 2 and 3 (P = 0.001), low FEV1 (P < 0.001), low FEV1% (P = 0.001), low MVV% (P = 0.046), low DLCO% (P = 0.033), intraoperative blood loss > 1000 ml (P = 0.041), preoperative application of gamma globulin (P < 0.001) were risk factors for POMC.
Variables that showed a P value < 0.10 in univariate logistic regression analysis were entered into a multivariate logistic regression analysis. The result showed that preoperative history of myasthenic crisis (P = 0.013), Osserman-stage IIB + III + IV (P < 0.001), preoperative daily dose of pyridostigmine bromide ≥ 240 mg (P < 0.001), ASA grade 2 and 3 (P = 0.001) were independent risk factors for POMC.
Discussion
The incidence of POMC in non-thymoma MG in our study was 11.63%, which is lower than previous studies [5,6,7,8]. Osserman type IIb and above are independent risk factors for our POMC (P < 0.001), which is also a relatively well recognized result [5, 9,10,11,12,13]. These patients have muscle weakness in swallowing, chewing, articulation, and breathing because of the involvement of the bulbar-related muscle groups. In addition to inspiratory and expiratory muscles, facial, oropharyngeal, and laryngeal muscles are important to maintain respiratory function. Weakness in these muscles interferes with upper airway protection, swallowing, and secretion clearance, even lead to upper airway obstruction and respiratory failure [14]. In addition to the above reasons, clinically, we conclude that most of these symptoms are caused by intraoperative tracheal intubation stimulation, pyridostigmine bromide and other reasons that lead to more airway secretions and inability to cough up, plus the saliva is unable to swallow or spit out, which is easy to cause aspiration or blockage of airway. POMC can often not be avoided, even we adjust the dosage of pyridostigmine bromide and anisodamine in real time according to the patient's condition. In order to reduce the airway irritation caused by intraoperative tracheal intubation, almost all the surgical methods have been changed to thoracoscopic thymectomy through the subxiphoid approach in the past two years, enabling us to perform laryngeal mask-assisted ventilation instead of tracheal intubation. However, at present, the amount of data is not enough, and there are many other influencing factors, and the protective advantage to POMC has not yet been shown.
Our multivariate analysis showed that a history of MC was a predictive factors for POMC(P = 0.013), whereas preoperative MG severity was not, which was also mentioned in some other studies [5]. About 20% of MG patients develop MC in their lifetime and one-third of them have a second MC [15]. This means that if the patient has ever had severe MG symptoms, although the symptoms are well controlled before surgery, MC may still occur after surgery, anesthesia and other blows. Therefore, even if the symptoms of these patients are well controlled, they should not be taken lightly. Postoperative management needs to be strengthened to be alert to the occurrence of POMC.
Another independent risk factor for POMC was the preoperative dose of 240 mg or more of pyridostigmine bromide daily (P < 0.001). Other studies [5] may not be exactly 240 mg, but in general, POMC is more likely to occur at higher dose. Acetylcholinesterase inhibitor (AChEI) increases the concentration of acetylcholine by blocking acetylcholinesterase at the neuromuscular junction to improve muscle strength. The large doses of cholinesterase inhibitors will accelerate the destruction of postsynaptic acetylcholine receptors (AChRs) at the neuromuscular junction, which decreases the postoperative ability of patients to cough up sputum, causes excessive respiratory secretions, increase the risk of respiratory system infection. The above factors will increase the risk of POMC. On the other hand, the larger dosage reflects severer symptoms. Therefore, the dosage of pyridostigmine bromide should be adjusted to the minimum dose range that can control symptoms before surgery as far as possible.
In the past, it seems that no one regarded preoperative comorbidities and basic health status of patients as one of the evaluation indicators of POMC. Clinically, we found that patients with poor preoperative general condition may be more prone to POMC. Therefore, we used the American Society of Anesthesiologists (ASA) (2020 edition) system to assess the preoperative comorbidities and underlying health status of patients. ASA classification is designed primarily to predict and evaluate the risk of anesthesia in surgery, which was first proposed in 1941 [16]. It has been verified by a large number of clinical cases and modified for many times. The ASA score system is also significantly correlated with the incidence of postoperative complications in different surgical specialties [17,18,19,20]. In our study, we found that ASA score was an independent influencing factor of POMC (P = 0.001), indicating that patients with more preoperative comorbidities were more likely to develop POMC. ASA as a predictor of POMC has never been mentioned in previous studies and needs to be further validated.
In our study, 35 patients with Osserman classification IIb or above, and unsatisfactory MG symptom control, received preoperative gamma globulin. As a high-risk group, 13 of them achieved POMC, with an incidence rate of 37.14%. Many studies [21] believe that gamma globulin can reduce the incidence of POMC. In our univariate analysis, preoperative gamma globulin was a possible risk factor, but in multivariate analysis, it did not become an independent risk factor. However, Gamez et al. conducted a prospective randomized controlled study in 2019 [22], suggesting that the application of gamma globulin could not reduce the risk of postoperative POMC in patients with well-controlled preoperative MG symptoms.
It must be acknowledged that there are some deficiencies in this study: 1. This is a retrospective study; 2. Limited to conditions, many patients did not have MG-related antibody tests, and many patients only had AChR-Ab, but no MuSK-Ab and other tests; 3. Preoperative treatment is inconsistent, and some of the high-risk patients with POMC were treated with gamma globulin, which inevitably affected the results; 4. Some patients are unable to cooperate with the pulmonary function test before surgery, so the result of the pulmonary function may not be accurate.
Through the study of perioperative factors in 387 non-thymoma MG patients, we concluded that the independent risk factors for POMC were: history of previous crisis, preoperative MG Osserman stage IIb and or above, preoperative dose of pyridoxine bromide ≥ 240 mg, and poor ASA classification. Therefore, non-thymoma MG patients should be highly vigilant if combined with the above conditions, take countermeasures in advance, and timely deal with the MG crisis that may occur at any time to ensure the safety of patients.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Hughes T. The early history of myasthenia gravis. Neuromuscul Disord. 2005;15(12):878–86.
Zieliński M. Surgical approaches to myasthenia gravis: perspective of anatomy and radicality in surgery. Thorac Surg Clin. 2019;29(2):159–64.
Wolfe GI, et al. Randomized trial of thymectomy in myasthenia gravis. N Engl J Med. 2016;375(6):511–22.
Carr AS, et al. A systematic review of population based epidemiological studies in Myasthenia Gravis. BMC Neurol. 2010;10:46.
Liu C, et al. Assessment of the risks of a myasthenic crisis after thymectomy in patients with myasthenia gravis: a systematic review and meta-analysis of 25 studies. J Cardiothorac Surg. 2020;15(1):270.
Howard JF Jr, et al. Safety and efficacy of eculizumab in anti-acetylcholine receptor antibody-positive refractory generalised myasthenia gravis (REGAIN): a phase 3, randomised, double-blind, placebo-controlled, multicentre study. Lancet Neurol. 2017;16(12):976–86.
Sanders DB, Wolfe GI, Benatar M, et al. International consensus guidance for management of myasthenia gravis: executive summary. Neurology. 2016;87(4):419–25.
Sonett JR, Jaretzki A 3rd. Thymectomy for nonthymomatous myasthenia gravis: a critical analysis. Ann N Y Acad Sci. 2008;1132:315–28.
Xue L, et al. Risk factors of myasthenic crisis after thymectomy for thymoma patients with myasthenia gravis. Eur J Cardiothorac Surg. 2017;52(4):692–7.
Niu YD, Wang TS, Zhao S, Ding LX. Predictors of early postoperative crisis for myasthenia gravis. Chin J Gerontol. 2013;33:2362–4.
Chu XY, et al. Predictors of postoperative myasthenic crisis in patients with myasthenia gravis after thymectomy. Chin Med J. 2011;124(8):1246–50.
Akaishi T, et al. Preoperative risks of post-operative myasthenic crisis (POMC): a meta-analysis. J Neurol Sci. 2019;407:116530.
Lucchi M, et al. Association of thymoma and myasthenia gravis: oncological and neurological results of the surgical treatment. Eur J Cardiothorac Surg. 2009;35(5):812–6.
Putman MT, Wise RA. Myasthenia gravis and upper airway obstruction. Chest. 1996;109(2):400–4.
Nam TS, et al. Clinical characteristics and predictive factors of myasthenic crisis after thymectomy. J Clin Neurosci. 2011;18(9):1185–8.
Saklad M. Grading of patients for surgical procedures. Anesthesiology. 1941;2:281–4.
Liu Y, et al. Relationship between American Society of Anesthesiologists (ASA) grade and 1-year mortality in nonagenarians undergoing hip fracture surgery. Osteoporos Int. 2015;26(3):1029–33.
Sankar A, et al. Reliability of the American Society of Anesthesiologists physical status scale in clinical practice. Br J Anaesth. 2014;113(3):424–32.
Giannice R, et al. Perioperative morbidity and mortality in elderly gynecological oncological patients (>/= 70 Years) by the American Society of Anesthesiologists physical status classes. Ann Surg Oncol. 2004;11(2):219–25.
Mayhew D, Mendonca V, Murthy BVS. A review of ASA physical status - historical perspectives and modern developments. Anaesthesia. 2019;74(3):373–9.
Jensen P, Bril V. A comparison of the effectiveness of intravenous immunoglobulin and plasma exchange as preoperative therapy of myasthenia gravis. J Clin Neuromuscul Dis. 2008;9(3):352–5.
Gamez J, et al. Intravenous immunoglobulin to prevent myasthenic crisis after thymectomy and other procedures can be omitted in patients with well-controlled myasthenia gravis. Ther Adv Neurol Disord. 2019;12:1756286419864497.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
HT: project administration and supervision. PJ: conceptualization, methodology, data curation and writing original draft. FW: methodology, data curation, writing original draft and editing. YL, JW: data curation, writing original draft and editing. YS, WT, HY, CH, DL, QW, CM: data curation, writing review, and editing. All authors contributed to the article and approved the submitted version. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Our study was approved by the Ethics Committee of Beijing hospital (reference number 2020BJYYEC-010-01).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests" in this section.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jiao, P., Wu, F., Liu, Y. et al. Analysis of influencing factors of perioperative myasthenic crisis in 387 myasthenia gravis patients without thymoma in a single center. J Cardiothorac Surg 18, 20 (2023). https://doi.org/10.1186/s13019-023-02136-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13019-023-02136-1