
Abstract
Background
Coronary artery bypass grafting in situs inversus totalis patients has been seldom reported in the literature.
Case presentation
A 76-year-old woman visited our hospital for chest pain and dyspnea that had started about 5 years earlier. Coronary angiography revealed triple-vessel disease, and computed tomography showed situs inversus totalis. Coronary artery bypass grafting was performed. In this case, the main operating surgeon stood on the right side of the patient until cardiopulmonary bypass was established and then switched positions to the left side of the patient for anastomosis.
Conclusion
CABG was successfully completed in a patient with situs inversus totalis. The position shift helped improve the safety and ease of the surgery.
Similar content being viewed by others

Background
Dextrocardia with situs inversus totalis is a rare congenital anomaly in which all organs are mirrored compared to their normal localization [1]. We herein report a patient with situs inversus totalis who underwent coronary artery bypass grafting (CABG). We believe that the position of the operating surgeon is important in this clinical setting.
Case presentation
A 76-year-old woman visited our hospital for chest pain and dyspnea. The symptoms had started about five years before the visit and had gradually worsened. Her medical history included diabetes mellitus and hyperlipidemia. At the time of admission, her symptoms were Canadian Class 3. Her heart rate was 73/min, and her blood pressure was 150/45 mmHg. No rales or murmur were heard on auscultation.
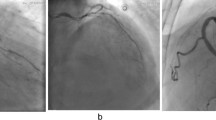
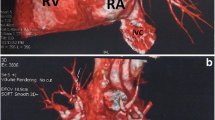
Electrocardiography with right chest lead showed ST depression in the V1r to V4r lead and ST elevation in the aVL lead. Transthoracic echocardiography revealed diffuse hypokinesis with a left ventricular ejection fraction of the 35%. Blood test findings were within normal limits. Computed tomography (CT) confirmed highly calcific coronary arteries and situs inversus totalis (Fig. 1). Coronary angiography demonstrated 99% stenosis of the proximal part of the morphologic left anterior descending artery (LAD), 99% stenosis of the right coronary artery (RCA), and 90% stenosis of the left circumflex artery (LCx) (Fig. 2). The treatment choice was discussed among the heart team, and CABG was recommended to the patient.

Preoperative computed tomography. All organs, including the cardiovascular system, are mirrored compared to their normal localization

Preoperative coronary angiography. a Stenosis of the left anterior descending artery by 99%, stenosis of the left circumflex artery by 90%. b Stenosis of the right coronary artery by 99%
During the operation, the surgeon first stood on the right side of the patient. After median sternotomy was performed, the left and right internal thoracic arteries (LITA and RITA) and saphenous vein graft (SVG) were harvested. Cardiopulmonary bypass was established by cannulation of the aorta and the physiological right atrium. At this time, the surgeon switched to the left side of the patient, placed a root cannula, and then cross-clamped the aorta. The SVG was anastomosed to the RCA, and the LITA was anastomosed to the LCx as free grafts. Finally, the RITA was anastomosed in situ to the LAD (Fig. 3). Surgery was completed without any problems. She was extubated four hours after surgery.

Intraoperative photographs. a View of the LCx. Approaching the anastomosis site from the right side of the patient is difficult. b End of the anastomosis
The post-operative course was uncomplicated. Post-operative coronary artery angiography showed a sufficient flow.
Discussion
Dextrocardia in combination with situs inversus totalis is a rare congenital anomaly, with a frequency of 1:10,000 [1, 2]. A total of 20% of situs inversus totalis patients are associated with Kartagener’s syndrome. Whereas cardiac abnormalities associated with isolated dextrocardia occur frequently, dextrocardia with situs inversus is associated with < 10% of cardiac abnormalities and has shown equal frequency to the normal population in terms of coronary artery disease [3]. Fabricius et al. first reported a case of dextrocardia in 1606, and Irvin et al. performed CABG for dextrocardia for the first time in 1980 [4, 5]. The first case of off-pump CABG for dextrocardia with situs inversus was reported by Tabry et al. in 2001 [6].
The primary point of argument concerning CABG for dextrocardia involves the standing position of the operating surgeon and the grafting design. In our search of MEDLINE using the PubMed interface, 26 of 37 cases in which CABG was used for dextrocardia between 1981 and 2021 referred to the standing position, with surgeons standing on the left side in 16 cases, the right side in 7 cases, and both sides in 3 cases [Table 1]. It is important for surgeons to be able to perform their operations easily, so the surgeon in the present case stood on the usual right side until cardiopulmonary bypass was established and then moved to the left side for anastomosis. This approach was particularly effective for anastomosing the free LITA to the LCx, as it is very difficult to perform such anastomosis from the same side of the left ventricular apex. The RITA was anastomosed to the LAD, which was more frequently used in previous case reports of CABG for dextrocardia. RITA-to-LAD anastomosis should be the first choice, as in cases of dextrocardia, this is considered theoretically equal to LITA-to-LAD anastomosis, which has been confirmed to have long-term patency [7]. Off-pump coronary bypass appears to be a simple and feasible option for dextrocardia when the surgeon has sufficient experience. We usually use a pump for uncomplicated multivessel bypass procedures in our institution and it was used in the present case because we wanted to avoid the risk of sudden hemodynamic compromise during off-pump bypass in this case with an anatomical abnormality.
Conclusions
CABG was successfully completed in a patient with situs inversus totalis. The operation was performed safely by switching the surgeon’s standing position and then selecting the most appropriate bypass grafts.
Availability of data and materials
Not applicable.
Abbreviations
- CABG:
-
Coronary artery bypass grafting
- CT:
-
Computed tomography
- LAD:
-
Left anterior descending artery
- RCA:
-
Right coronary artery
- LCx:
-
Left circumflex artery
- LITA:
-
Left internal thoracic artery
- RITA:
-
Right internal thoracic artery
- SVG:
-
Saphenous vein graft
- RA:
-
Radial artery
- GEA:
-
Gastroepiploic artery
References
Zhigalov K, Ponomarev D, Sozkov A, Kadyraliev B, Easo J, Weymann A. Coronary artery bypass grafting in a patient with situs inversus totalis. Am J Case Rep. 2019;20:806–9.
Subash S, Simha PP, Manjunatha N. Off-pump coronary artery bypass surgery in a patient with dextrocardia and situs inversus: anesthetic, surgical consideration and role of transesophageal echocardiography. Heart Views. 2017;18(3):100–3.
Hynes KM, Gau GT, Titus JL. Coronary heart disease in situs inversus totalis. Am J Cardiol. 1973;31(5):666–9.
Grey DP, Cooley DA. Dextrocardia with situs inversus totalis: Cardiovascular surgery in three patients with concomitant coronary artery disease. Cardiovasc Dis. 1981;8(4):527–30.
Irvin RG, Ballenger JF. Coronary artery bypass surgery in a patient with situs inversus. Chest. 1982;81(3):380–1.
Tabry IF, Calabrese J, Zammar H, Abou-Kasem K, Akeilan H, Gharbieh N, et al. Case report: off-pump total myocardial revascularization for dextrocardia and situs inversus. Heart Surg Forum. 2001;4(3):251–3.
Cameron A, Davis KB, Green G, Schaff HV. Coronary bypass surgery with internal-thoracic-artery grafts–effects on survival over a 15-year period. N Engl J Med. 1996;334(4):216–9.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
OA wrote the manuscript. WT did the literature search. TA and WT conceived and designed the report. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
We have obtained written informed consent from the patients to publish this report.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Oi, A., Tatsuishi, W., Mohara, J. et al. Coronary artery bypass grafting in a patient with situs inversus totalis: a case report. J Cardiothorac Surg 17, 56 (2022). https://doi.org/10.1186/s13019-022-01807-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13019-022-01807-9