
Abstract
Background
Developmental dysplasia of the hip (DDH) is a common cause of childhood disability, and the incidence of DDH shows significant familial aggregation. As the genetic factors of DDH remain unknown, the correlation between five candidate single nucleotide polymorphisms (SNPs) and DDH was evaluated in the Han Chinese population of Southwest China.
Methods
A case‒control association study was conducted in 276 patients with DDH and 318 healthy controls. SNP genotyping in the case and control groups was performed by SNPshot and multiple PCR. SNPs were genotyped in the case and control groups by multiplex PCR. The relationship between DDH and candidate SNPs was evaluated using the χ2 test.
Results
The genotype distributions of rs291412 in HIBCH and rs769956 in FTCDNL1 were different between the case and control groups (P < 0.05). After genetic model analysis, logistic regression analysis revealed that the C allele of rs291412 had a protective effect on DDH (OR = 0.605, P = 0.010) and that the G allele of rs769956 was a risk factor (OR = 2.939, P = 0.010).s.
Conclusion
These SNPs could be associated with susceptibility to DDH but larger population-based studies should confirm the current results.
Similar content being viewed by others


Background
Developmental dysplasia of the hip is a common hip joint deformity caused by incomplete acetabulum formation. This hip malformation changes the length of the hip muscle torque arm, the line of action, and the reaction force on the hip joint during walking [1, 2], resulting in higher than normal load and shear force in the joint. Clinical manifestations of this disease include dislocation, subluxation, acetabular dysplasia and hip instability [3, 4]. The overall prevalence of DDH is 1.52% in Chinese adults [5] and 1.7% in Chinese infants [6], with a high heritability of 83.59%±4.90% among siblings, and risk of the disease is at least twice as high in females than in males [7]. Mild DDH can heal itself in childhood, but if left uncorrected in infancy, DDH can lead to difficult rigid luxation of the femur head, leading to long spica casting treatments or surgical operations and further frequently leading to early total hip replacement [8, 9]. As the remodeling potential of the hip joint decreases with age, delayed treatment may result in increased surgical difficulty and frequency [10]; in general, additional surgery in adolescence requires less deformity correction after surgery for DDH in childhood [11]. Therefore, early diagnosis of DDH is crucial for its treatment and preventing complications [12]. At present, clinical diagnosis of DDH mainly relies on imaging methods [13], and the progress of related molecular diagnosis research is slow. Hence, it is necessary to study risk genes associated with DDH onset for early screening clinically.
The specific pathogenesis of DDH remains unknown. However, previous studies indicated that the formation of connective tissue, osteogenesis, chondrogenesis, cell growth, proliferation and differentiation during development may be involved [14, 15]. Moreover, the etiology of DDH is complex, and epidemiological studies have shown that genetic factors affect susceptibility [16, 17], presenting an autosomal dominant inheritance pattern in some families [18]. Accordingly, it is meaningful to consider genetic background while assessing the etiology of DDH formation.
Methods
Subjects
In this study, the subjects comprised 276 patients with DDH recruited from the Han Chinese population in Southwest China. Definitive diagnosis was made by two experienced orthopedic experts based on the results of physical examination and pelvic imaging. When clinical physical examination revealed one of the following positive signs, further imaging examination was performed: (1) asymmetrical dermatoglyphics of the bilateral thighs, buttocks, and perineum; (2) shorter lower limbs of the affected side and muscle strength lower than that of the healthy side; (3) hip discomfort or pain; (4) restricted hip abduction, with or without adduction deformity; (5) abnormal gait with limping or duck-like gait; (6) positivity for one of the Allis sign, Ortolani sign, Barlow sign, Nelaton test or in the abduction test. A definitive diagnosis was made when the imaging examination showed any of the following: (1) B-ultrasonography for patients aged 0–6 months with angle A less than 60 degrees. (2) specific indicators measured by imaging for a patient over 6 months old, including ① the femoral head epiphysis located in the upper and lower lateral Perkin quadrant; ②acetabular index > 25°; ③CE angle < 20°; ④ interrupted Shenton line; and ⑤ CT or MRI examination fore elderly or adult patients showing poor acetabulum alignment, acetabulum coverage rate < 75%, dislocation or subluxation. Patients with syndromic hip dislocation and other chronic diseases were excluded. The case group consisted of 65 males and 211 females, and the control group consisted of 318 individuals; those with congenital malformation, hereditary neuropathy, hip dislocation or family history of DDH were excluded. This study was approved by the ethics committee of 920th Hospital of Joint Logistics Support Force of Chinese People’s Liberation Army (2020-057-01), and informed consent was obtained from all participants and their families before enrollment in the trial.
Site selection
This study prescreened candidate SNPs in the Han Chinese population in Southwest China based on Pool-seq and gene functional candidate strategies. Peripheral blood DNA from the 276 patients was extracted using Axygen® Axyprep Blood Genomic DNA Miniprep Kit following the manufacturer’s instructions; the DNA was pooled at equal concentrations and subjected to Whole Exome Sequencing (WES) at 60X depth; the number of reads was obtained by sequencing, the WES were performed by the Beijing Novogene Corporation.
The pooled DNA were used to construct libraries using the Agilent SureSelect Human All Exon V6 kit. Subsequently, paired-end sequencing (PE150) was performed on the Illumina platform to generate FastQ files. After data cleaning and quality assessment, the reads were aligned to the human reference genome GRCh37/hg19 using BWA (Li et al., 2018). Qualified SNPs were called using SAMtools (Li et al., 2009) with specific criteria (QUAL ≥ 20; DP ≥ 50; MQ ≥ 30). Varcan2 [19] software was used to estimate SNP frequency in the case pool. Then, 1000 Genomes data for Asians were used as the control group, and the difference in locus frequency (1000G_EAS) between the case group was compared by the chi-square test. SNPs (P < 0.0001), with significantly different frequencies (case pool vs. East Asian population) in genes associated with DDH function selected as candidate sites.
Genotyping
The five SNPs (rs4823187 A/C/G, rs2426300 A/C/T, rs10146692 A/G, rs291412 C/T, rs769956 A/G) genotyping was performed by the SNaPshot technology using PCR-A300 (Hangzhou Langi Scientific Instrument Co., LTD.), which is a multiplex PCR-based next generation sequencing based on a primer extension-based method for genotyping known SNP positions.
After obtaining written informed consent, 3 ml of peripheral blood was collected; genomic DNA was extracted from 300 ml peripheral blood using Axygen® Axyprep Blood Genomic DNA Miniprep Kit following the manufacturer’s instructions. PCR primer design: Primer 5 was used to design multiple primers for specific amplification of candidate SNP sites. The primer sequences are shown in Table 1. The reaction was performed in a 15 µl volume consisting of 0.3 µl forward primer, 0.3 µl reverse primer, 1 µl DNA template, 7.5 µl PCR mix (Shanghai Yisheng Biotechnology Co., Ltd. ), and 5.9 µl ddH2O. The reaction conditions were as follows: predenaturation at 95℃ for 5 min, 35 cycles of denaturation at 94℃ for 20 s, annealing at 55℃ for 20 s, and extension at 72℃ for 40 s, and repair extension at 72℃ for 10 min.
PCR product purification: The reaction was performed in a 7 µl mixture consisting of 3 µl PCR product, 0.2 µl ExoI, 0.8 µl FastAP, 0.7 µl ExoI buffer, and 2.3 µl ddH2O. Purification conditions: 37 ℃ for 15 min, 80 ℃ for 15 min. The above purification reagents were purchased from Fermentas, Canada.Purified PCR product reaction: The reaction was performed in a 6 µl mixture consisting of 2 µl purified PCR product, 1 µl SNAPSHOT mix (ABI, USA), extension primer 0.2 µl/strip, and 2.8 µl ddH2O. Reaction conditions: 94 °C for 10 s, 52 °C for 5 s, 60 °C for 30 s, for a total of 30 cycles.One microliter of the extension product was added to 9 µl HiDi (ABI, USA), denatured at 95 °C for 3 min, and immediately placed in an ice water bath. Next-generation sequencing of the PCR product was performed using a 3730 XL gene sequencer (ABI, USA). The original image data were converted to sequence reads by base calling and analyzed using GeneMarker software.
Statistical analysis
SPSS (IBM Corporation, Armonk, NY, USA) was used for statistical analysis. Quantitative data are shown as the mean ± standard deviation (SD). Comparisons between 2 groups were performed using Student’s t test. The Hardy-Weinberg equilibrium (HWE) of the control group was evaluated by the chi-square test. The correlation between SNPs and DDH was evaluated. The relative risk of disease is expressed by the odds ratio (OR) and 95% confidence interval (95% CI). Bonferroni’s correction was applied for multiple tests. All statistical tests were two-tailed, and P < 0.05 was defined as statistically significant.
Results
Basic characteristics of the study subjects
A total of 609 subjects were recruited for this study, including 276 DDH patients and 318 healthy individuals. All patients with DDH were diagnosed by orthopedic experts according to their medical history, clinical symptoms and imaging results (hip X-ray, magnetic resonance imaging and ultrasound), including 67 males and 209 females. The control group was composed of 120 males and 213 females.
Pool-Seq screen for candidate genes
WES with 60X depth were performed. 179.8 G data was obtained, and the Q30 of these data was 93.44. At last, the allele frequencies of total 14,535 SNPs were obtained. The SNP frequencies obtained through Pool-seq were compared to those from the East Asian population in the 1000 Genomes Project. A chi-square test was conducted to identify positive SNPs (P < 0.0001).
SNPs were selected with the most significant P-values, while the genes in which these SNPs are located are functionally closely related to DDH. At last, the five candidate SNPs (rs4823187 in PARVB, rs2426300 in NFATC2, rs10146692 in DPF3, rs291412 in HIBCH, and rs769956 in FTCDNL1) were selected for genotyping in this study. Among them, the actin-binding protein encoded by PARVB plays a role in cytoskeletal tissue and cell adhesion and contains the calmodulin homologous domain for binding to actin filaments. NFATC2 is a member of the activated T nuclear factor (NFAT) family, which is related to inflammation and plays a central role in inducing gene transcription during the immune response. DPF3 encodes a member of the D4 protein family, which binds to acetylated histones acting as transcriptional regulators. The HIBCH gene encodes 3-hydroxyisobutyryl-CoA hydrolase. FTCDNL1 affects folate-binding activity and transferase activity and is associated with osteoporosis. The above candidate SNPs were examined in 276 DDH patients and 318 healthy controls to identify genetic associations with DDH.
Distribution of genotypes and alleles
All five candidate SNPs conformed to Hardy-Weinberg equilibrium in the control and DDH groups (HWE-P > 0.05; shown in Table 2), and the frequency of minor alleles was greater than 0.05, indicating that the frequency of each allele was genetically stable. The allele frequencies of the 5 SNPs in the control and DDH groups were compared using the chi-square test. It is worth noting that SNP rs4823187 in PARVB and SNP rs2426300 in NFATC2 were found to be allele loci after SNPshot typing. We assumed these alleles with lower frequencies to be mutated in the population and combined their frequencies for chi-square analysis [20]. SNP rs291412 in HIBCH and SNP rs769956 in FTCDNL1 showed differences between the DDH and control groups. In addition, the minor allele frequency (MAF) of rs4823187 in PARVB, rs10146692 in DPF3 and rs291412 in HIBCH was statistically lower in the case group than in the control group, though the MAF of rs2426300 in NFATC2 and rs769956 in FTCDNL1 was higher. Although the positive results of SNP rs291412 in HIBCH and SNP rs769956 in FTCDNL1 disappeared after multiple tests and Bonferroni correction, these two variants are probably related to the genetic susceptibility of DDH.
Analyses of the genetic model of the correlation between 5 candidate SNPs and DDH
The association between the above 2 SNPs and risk of DDH was evaluated using the assumption of various genetic models with low-frequency allele M: the dominant model, MM + MN vs. NN (as long as the M allele is carried, the disease risk is influenced), and the recessive model, MM vs. MN + NN (it is necessary to carry two M at the same time to influence the risk of carriers). According to the above hypothesis, the correlation between rs291412, rs769956 and genetic susceptibility to DDH was evaluated using the chi-square test, and the results are shown in Table 3. Under the hypothesis of the dominant model, SNP rs291412 in HIBCH showed significant differences between the DDH and control groups (OR = 0.605, P = 0.010), indicating that the rare genotype of HIBCH rs291412 has a protective effect against DDH. However, under the hypothesis of the recessive model, SNP rs769956 in FTCDNL1 showed significant differences between the DDH and control groups (OR = 2.939, P = 0.010), indicating that the common genotype of FTCDNL1 rs769956 is a risk factor for DDH.
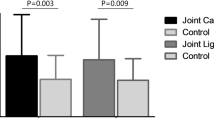
The expression relationship between these two variants and their corresponding genes was explored in the eQTL database of GTEx (https://www.gtexportal.org/). The results revealed that the three genotypes of rs291412 significantly influence expression of the HIBCH gene in pituitary and skeletal muscle tissues (Fig. 1) but that the presence of the T allele leads to reduce expression in these tissues (P = 1.2*10− 9; P = 4.5*10− 12). The three genotypes of rs769956 also significantly influence expression of the FTCDNL1 gene in tibial nerve tissue and skeletal muscle tissue (Fig. 2), whereas the presence of allele A reduces it (P = 4.9 * 10− 7; P = 6.4 * 10− 8).

Differential expression levels of various allelic genotypes of SNP rs291412 in HIBCH in pituitary tissue and skeletal muscle tissue

Differential expression levels of various allelic genotypes of SNP rs769956 in FTCDNL1 in skeletal muscle tissue and tibial nerve
Discussion
In this case‒control study, five candidate SNPs were prescreened by pooled sequencing, and the link to genetic susceptibility to DDH was investigated in these candidate SNPs (rs4823187 in actin-related PARVB, rs2426300 in T-cell-related NFATC2, rs10146692 in transcription-regulating factor-related DPF3, rs291412 in HIBCH encoding 3-hydroxyisobutyryl coenzyme A hydrolase, rs769956 in folate binding activity-related FTCDNL1). The results showed that the genetic variant rs291412 in HIBCH and rs769956 in FTCDNL1 can significantly reduce the risk of DDH onset.
DDH is a common disorder in children, and its risk increases with the presence of various factors, such as mechanical constraints in the uterus and abnormal position in the last three months, but it is also related to the postnatal environment and genetic susceptibility [21,22,23,24,25]. To reveal the genetic background of DDH, some candidate genes (including WISP-2 [26], CX3CR1 [27], and TXNDC3 [28]) responsible for susceptibility to DDH have been detected by molecular analysis and sequencing technology. However, in this study, differences in the above genes in the control and DDH groups were not revealed by pooled sequencing, which may be related to = different genetic backgrounds. As data from 1000 Genomes for Asians were used as controls in preliminary screening of candidate sites, we speculate that these DDH gene results may be difficult to replicate in different populations. This may be caused by different geographical regions or different environments and lifestyles among races or ethnic groups; this study only explored susceptibility genes for DDH in the Han population.
The HIBCH gene (containing 17 exons) is located at chromosome 2q32.2 and encodes HIBYL-CoA and β-hydroxypropiylcoA hydrolase. Mutations in this gene are associated with 3-hydroxyisobutyl-CoA hydrolase deficiency and accumulation of metabolic intermediates of valine. The HIBCH gene is widely expressed in human tissues such as the kidney, heart and skeletal muscle [29], and its alternative splicing results in multiple transcript variants. HIBCH deficiency is a rare autosomal recessive hereditary neurodegenerative disease characterized by a continuous decline in psychomotor ability, which can be clinically observed in young children with developmental delay, hypotonia, neurological degeneration and seizures [30,31,32]. The results of this study showed a significant association of SNP rs29141 in HIBCH with the DDH phenotype in the Han population of Southwest China, which suggests an increased risk for people carrying the minor allele of this SNP (P = 0.035). However, statistical significance was lost after Bonferroni correction, which indicates that the significant association of this SNP may lead to the first type of statistical error during simultaneous analysis of multiple SNPs. Nevertheless, considering the genetic heterogeneity of DDH and the small possibility of multiple DDH patients carrying the same susceptibility mutation, we believe that such sites with P values on the margin of statistical positivity are worthy of further attention. Furthermore, we verified the hypothesis of HIBCH gene polymorphism and susceptibility to isolated DDH. In the general population, low-frequency alleles are considered to be derived from mutations. HIBCH rs291412 is associated with susceptibility to DDH in the Han population of Southwest China, suggesting that the rare allele of HIBCH rs291412 (C allele) has a protective effect on susceptibility to DDH (OR = 0.605, P = 0.010).
Forminiotransferase cyclodeaminase N-terminal-like gene (FTCDNL1), located at chromosome 2q33.1, is widely expressed in various tissues, including bone. Mutations in this gene have been significantly associated with susceptibility to osteoporosis [33], which has also been verified in the Taiwan DDH population [34]. The results of this study showed a significant association of SNP rs769956 in FTCDNL1 with an increased risk of DDH in the Han population of Southwest China, suggesting that individuals carrying the common allele of FTCDNL1 rs769956 (G allele) have a potential risk factor (OR = 2.939, P = 0.010).
In addition, after querying the expression relationship of HIBCH rs291412 and FTCDNL1 rs769956 in the eQTL database of GTEx, we found that different genotypes of HIBCH rs291412 and FTCDNL1 rs769956 showed significant differences in expression in skeletal muscle. The pathogenesis of DDH is related to slow and stable accumulation of toxic methylacroyl-coA in mitochondria, as well as to rapid and intensive accumulation under conditions of insufficient energy, such as exercise or fever [35]. The most common pathophysiology from DDH to osteoarthritis is femoral bone malformation [36], and the mechanism by which DDH produces a destructive load on skeletal muscle is also related to abnormal skeletal muscle geometry and function [37]. The study of Sacha et al. [38] showed that the absence of HIBCH would lead to the absence of respiratory enzymes in skeletal muscle, resulting in hypotonia. This evidence suggests that differential expression of HIBCH and FTCDNL1 may lead to changes in skeletal muscle morphology and function, which may be related to the pathogenesis of DDH.
In summary, DDH is a complex muscle-joint disease, and we speculated that the pathological changes in muscles caused by DDH are related to deficiency of HIBCH and FTCDNL1, as well as to heterogeneity in the genetic background. Therefore, association analysis of susceptibility to DDH in different populations should be further investigated. This study is the first to suggest the relationship between HIBCH, FTCDNL1 and susceptibility to DDH.
Conclusion
This study shows for the first time the association of SNP rs291412 in HIBCH and SNP rs769956 in FTCDNL1 with the risk of DDH, suggesting that these sites are potential genetic susceptibility markers of DDH in the Chinese population.
Although the mechanisms by which HIBCH and FTCDNL1 cause DDH are largely unknown, these findings provide new insight into the complex genetic structure of DDH and may have some significance for the identification of high-risk individuals and genetic counseling.
Data availability
The datasets used or analysed during the current study are available from the corresponding author on reasonable request.
References
Haefeli PC, Steppacher SD, Babst D, Siebenrock KA, Tannast M. An increased iliocapsularis-to-rectus-femoris ratio is suggestive for instability in borderline hips. Clin Orthop Relat Res. 2015;473(12):3725–34. https://doi.org/10.1007/s11999-015-4382-y.
Song K, Gaffney BMM, Shelburne KB, Pascual-Garrido C, Clohisy JC, Harris MD. Dysplastic hip anatomy alters muscle moment arm lengths, lines of action, and contributions to joint reaction forces during gait. J Biomech. 2020;110:109968. https://doi.org/10.1016/j.jbiomech.2020.109968.
Weinstein SL, Mubarak SJ, Wenger DR. Fundamental concepts of developmental dysplasia of the hip. Instr Course Lect. 2014;63:299–305.
Chan EF, Farnsworth CL, Koziol JA, Hosalkar HS, Sah RL. Statistical shape modeling of proximal femoral shape deformities in Legg-Calvé-Perthes disease and slipped capital femoral epiphysis. Osteoarthritis Cartilage. 2013;21(3):443–9. https://doi.org/10.1016/j.joca.2012.12.007.
Tian FD, Zhao DW, Wang W, Guo L, Tian SM, Feng A, et al. Prevalence of Developmental Dysplasia of the hip in Chinese adults: a cross-sectional survey. Chin Med J. 2017;130(11):1261–8. https://doi.org/10.4103/0366-6999.206357.
Xu N, Xia B, Tao HW, Sun K, Liu QH, Chen WJ, et al. Epidemiological investigation and ultrasonic diagnosis of developmental dysplasia of the hip in Chinese infants a large multi-center cohort study. Medicine. 2022;101(2). https://doi.org/10.1097/md.0000000000028320.
Livingstone C. IGF2 and cancer. Endocr Relat Cancer. 2013;20(6):R321–39. https://doi.org/10.1530/erc-13-0231.
Mulpuri K, Song KM, Gross RH, Tebor GB, Otsuka NY, Lubicky JP, et al. The American Academy of Orthopaedic Surgeons evidence-based Guideline on Detection and Nonoperative Management of Pediatric Developmental Dysplasia of the hip in infants up to six months of age. J bone Joint Surg Am Volume. 2015;97(20):1717–8. https://doi.org/10.2106/jbjs.O.00500.
Terjesen T. Residual hip dysplasia as a risk factor for osteoarthritis in 45years follow-up of late-detected hip dislocation. J Child Orthop. 2011;5(6):425–31. https://doi.org/10.1007/s11832-011-0370-2.
Naik P. Remodelling in children’s fractures and limits of acceptability. Indian J Orthop. 2021;55(3):549–59. https://doi.org/10.1007/s43465-020-00320-2.
Kołodziejczyk K, Czubak-Wrzosek M, Kwiatkowska M, Czubak J. Hip dysplasia in adolescence: osteotomy in childhood improves the results of periacetabular osteotomy in adolescents and young adults: a prospective study. Bone Joint J. 2022;104–b(7):775–80. https://doi.org/10.1302/0301-620x.104b7.Bjj-2021-1771.R1.
Hattori T, Inaba Y, Ichinohe S, Kitano T, Kobayashi D, Saisu T, et al. The epidemiology of developmental dysplasia of the hip in Japan: findings from a nationwide multi-center survey. J Orthop Sci. 2017;22(1):121–6. https://doi.org/10.1016/j.jos.2016.08.009.
Elbourne D, Dezateux C, Arthur R, Clarke NM, Gray A, King A, et al. Ultrasonography in the diagnosis and management of developmental hip dysplasia (UK Hip Trial): clinical and economic results of a multicentre randomised controlled trial. Lancet. 2002;360(9350):2009–17. https://doi.org/10.1016/s0140-6736(02)12024-1.
Harsanyi S, Zamborsky R, Kokavec M, Danisovic L. Genetics of developmental dysplasia of the hip. Eur J Med Genet. 2020;63(9):103990. https://doi.org/10.1016/j.ejmg.2020.103990.
Harsanyi S, Zamborsky R, Krajciova L, Kokavec M, Danisovic L. Developmental Dysplasia of the hip: a review of etiopathogenesis, risk factors, and genetic aspects. Med (Kaunas). 2020;56(4). https://doi.org/10.3390/medicina56040153.
Feldman GJ, Peters CL, Erickson JA, Hozack BA, Jaraha R, Parvizi J. Variable expression and incomplete penetrance of developmental dysplasia of the hip: clinical challenge in a 71-member multigeneration family. J Arthroplasty. 2012;27(4):527–32. https://doi.org/10.1016/j.arth.2011.10.016.
Kapoor B, Dunlop C, Wynn-Jones C, Fryer AA, Strange RC, Maffulli N. Vitamin D and oestrogen receptor polymorphisms in developmental dysplasia of the hip and primary protrusio acetabuli–a preliminary study. J Negat Results Biomed. 2007;6:7. https://doi.org/10.1186/1477-5751-6-7.
Feldman GJ, Parvizi J, Levenstien M, Scott K, Erickson JA, Fortina P, et al. Developmental dysplasia of the hip: linkage mapping and whole exome sequencing identify a shared variant in CX3CR1 in all affected members of a large multigeneration family. J Bone Min Res. 2013;28(12):2540–9. https://doi.org/10.1002/jbmr.1999.
Reble E, Castellani CA, Melka MG, O’Reilly R, Singh SM. VarScan2 analysis of de novo variants in monozygotic twins discordant for schizophrenia. Psychiatr Genet. 2017;27(2):62–70. https://doi.org/10.1097/ypg.0000000000000162.
Klotz L, Norman S, Vieira JM, Masters M, Rohling M, Dubé KN, et al. Cardiac lymphatics are heterogeneous in origin and respond to injury. Nature. 2015;522(7554):62–7. https://doi.org/10.1038/nature14483.
Yang W, Jin G, Qian K, Zhang C, Zhi W, Yang D, et al. Comprehensive bioinformatics analysis of susceptibility genes for developmental dysplasia of the hip. Intractable Rare Dis Res. 2022;11(2):70–80. https://doi.org/10.5582/irdr.2022.01043.
Oh EJ, Min JJ, Kwon SS, Kim SB, Choi CW, Jung YH, et al. Breech Presentation in Twins as a risk factor for Developmental Dysplasia of the hip. J Pediatr Orthop. 2022;42(1):e55–8. https://doi.org/10.1097/bpo.0000000000001982.
He LP, Liu PZ, Wen YM, Wu J. Effect of temperature maintenance by forced-air warming blankets of different temperatures on changes in inflammatory factors in children undergoing congenital hip dislocation surgery. Chin Med J (Engl). 2020;133(15):1768–73. https://doi.org/10.1097/cm9.0000000000000846.
Ghosh S, Fryer AA, Hoban PR, Wynn-Jones C, Maffulli N. Fibrillin 1 gene with R2726W mutation is absent in patients with primary protrusio acetabuli and developmental dysplasia of the hip. Med Sci Monit. 2009;15(5):Cr199–202.
Aicale R, Tarantino D, Maccauro G, Peretti GM, Maffulli N. Genetics in orthopaedic practice. J Biol Regul Homeost Agents. 2019;33(2 Suppl 1):103–17. XIX Congresso Nazionale S.I.C.O.O.P. Societa’ Italiana Chirurghi Ortopedici Dell’ospedalita’ Privata Accreditata.
Ji X, Liu T, Zhao S, Li J, Li L, Wang E. WISP-2, an upregulated gene in hip cartilage from the DDH model rats, induces chondrocyte apoptosis through PPARγ in vitro. Faseb j. 2020;34(4):4904–17. https://doi.org/10.1096/fj.201901915R.
Li L, Wang X, Zhao Q, Wang E, Wang L, Cheng J, et al. CX3CR1 polymorphisms associated with an increased risk of developmental dysplasia of the hip in human. J Orthop Res. 2017;35(2):377–80. https://doi.org/10.1002/jor.23294.
Qiao L, Yan W, Dai J, Yao Y, Chen D, Xu Z, et al. A novel missense variant in TXNDC3 is associated with developmental dysplasia of the hip in Han Chinese population. Int J Clin Exp Pathol. 2017;10(10):10483–8.
Çakar NE, Görükmez O. 3-Hydroxyisobutyryl-CoA hydrolase (HIBCH) Deficiency cases diagnosed by only HIBCH Gene Analysis and Novel Pathogenic Mutation. Ann Indian Acad Neurol. 2021;24(3):372–8. https://doi.org/10.4103/aian.AIAN_192_20.
Schottmann G, Sarpong A, Lorenz C, Weinhold N, Gill E, Teschner L, et al. A movement disorder with dystonia and ataxia caused by a mutation in the HIBCH gene. Mov Disord. 2016;31(11):1733–9. https://doi.org/10.1002/mds.26704.
Tan H, Chen X, Lv W, Linpeng S, Liang D, Wu L. Truncating mutations of HIBCH tend to cause severe phenotypes in cases with HIBCH deficiency: a case report and brief literature review. J Hum Genet. 2018;63(7):851–5. https://doi.org/10.1038/s10038-018-0461-8.
Marti-Sanchez L, Baide-Mairena H, Marcé-Grau A, Pons R, Skouma A, López-Laso E, et al. Delineating the neurological phenotype in children with defects in the ECHS1 or HIBCH gene. J Inherit Metab Dis. 2021;44(2):401–14. https://doi.org/10.1002/jimd.12288.
Kou I, Takahashi A, Urano T, Fukui N, Ito H, Ozaki K, et al. Common variants in a novel gene, FONG on chromosome 2q33.1 confer risk of osteoporosis in Japanese. PLoS ONE. 2011;6(5):e19641. https://doi.org/10.1371/journal.pone.0019641.
Lu HF, Hung KS, Hsu YW, Tai YT, Huang LS, Wang YJ, et al. Association Study between the FTCDNL1 (FONG) and susceptibility to osteoporosis. PLoS ONE. 2015;10(10):e0140549. https://doi.org/10.1371/journal.pone.0140549.
Yamada K, Naiki M, Hoshino S, Kitaura Y, Kondo Y, Nomura N, et al. Clinical and biochemical characterization of 3-hydroxyisobutyryl-CoA hydrolase (HIBCH) deficiency that causes Leigh-like disease and ketoacidosis. Mol Genet Metab Rep. 2014;1:455–60. https://doi.org/10.1016/j.ymgmr.2014.10.003.
Gala L, Clohisy JC, Beaulé PE. Hip dysplasia in the Young Adult. J Bone Joint Surg Am. 2016;98(1):63–73. https://doi.org/10.2106/jbjs.O.00109.
Harris MD, Shepherd MC, Song K, Gaffney BMM, Hillen TJ, Harris-Hayes M, et al. The biomechanical disadvantage of dysplastic hips. J Orthop Res. 2022;40(6):1387–96. https://doi.org/10.1002/jor.25165.
Ferdinandusse S, Waterham HR, Heales SJ, Brown GK, Hargreaves IP, Taanman JW, et al. HIBCH mutations can cause Leigh-like disease with combined deficiency of multiple mitochondrial respiratory chain enzymes and pyruvate dehydrogenase. Orphanet J Rare Dis. 2013;8:188. https://doi.org/10.1186/1750-1172-8-188.
Acknowledgements
Not applicable.
Funding
Funded by Yunnan Major Science and Technology Project - Biomedical Major Project (2018ZF008); Yunnan Provincial Health Commission Clinical Center Construction Major Project (ZX20191001); CAMS Innovation Fund for Medical Sciences (CIFMS, 2021-I2M-1-024); Yunnan Science and Technology talents and platform Project (202005AC160011); Yunnan Training Programme for the advanced Talents of Health and Medical Technology (D-2018013). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Conceptualization: XHM, YTW, HS, CL; Data curation: YR, YQX, HS, CL; Formal analysis: YR, YQX, HS, CL; Funding acquisition: CL; Writing - original draft: XHM, YTW; Writing - review and editing: all authors.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of 920th Hospital of Joint Logistics Support Force of Chinese People’s Liberation Army (2020-057-01), and informed consent was obtained from all participants and their families before enrollment in the trial.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Meng, Xh., Weng, Yt., Rao, Y. et al. Two genetic variants in the HIBCH and FTCDNL1 genes are associated with susceptibility to developmental dysplasia of the hips among the Han Chinese population of Southwest China. J Orthop Surg Res 19, 464 (2024). https://doi.org/10.1186/s13018-024-04958-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-024-04958-8