
Abstract
Background
This Bayesian network meta-analysis investigated the available randomized control trials (RCTs) to point out which acupuncture protocol is the most effective for chronic aspecific low back pain (LBP). Efficacy was measured in terms of pain (Visual Analogic Scale, VAS) and disability (Roland Morris Disability Questionnaire, RMQ), Transcutaneous Electrical Nerve Stimulation (TENS).
Methods
PubMed, Google scholar, Embase, and Scopus were accessed in March 2022. All the RCTs comparing two or more acupuncture modalities for aspecific chronic LBP were accessed. Only studies which investigated the efficacy of acupuncture on patients with symptoms lasting a minimum of 1.5 months, or with at least three episodes in the previous 12 months, were considered eligible. The Review Manager Software (The Nordic Cochrane Collaboration, Copenhagen) was used for the methodological quality assessment. The STATA Software/MP, Version 14.1 (StataCorporation, College Station, Texas, USA), was used for the statistical analyses. The NMA was performed through the STATA routine for Bayesian hierarchical random-effects model analysis.
Results
Data from 44 RCTs (8338 procedures) were retrieved. 56% of patients were women. The mean age of the patients was 48 ± 10.6 years. The mean BMI was 26.3 ± 2.2 kg/m2. The individual group (95% confidence interval (CI) 2.02, 7.98) and the standard combined with TENS (95% CI 2.03, 7.97) demonstrated the highest improvement of the RMQ. The VAS score was lower in the standard combined with TENS group (95% CI 3.28, 4.56). Considering the standard acupuncture group, different studies used similar protocols and acupuncture points and the results could thus be compared. The equation for global linearity did not find any statistically significant inconsistency in any of the network comparison.
Conclusion
Verum acupuncture is more effective than sham treatment for the non-pharmacological management of LBP. Among the verum protocols, individualized acupuncture and standard acupuncture with TENS were the protocols that resulted in the highest improvement in pain and quality of life.
Level of Evidence
Level I, Bayesian network meta-analysis of RCTs.
Similar content being viewed by others


Introduction
Low back pain (LBP) is common, leading to relevant economic burden [1, 2]. On average, the lifetime prevalence of LBP is as high as 80% [3, 4]. LBP is aspecific in most cases, and no pathoanatomical cause can be found [5]. In such patients, management aims to reduce symptoms and disability, allowing the return to daily life activities and participation in physiotherapy [5]. Current guidelines recommend physiotherapy as a first-line treatment for chronic LBP [6]. As some patients do not experience sufficient benefit from physiotherapy alone, further options are required. Pharmacotherapy is the second step in the management of chronic aspecific LBP [6]. NSAIDs and opiates represent the most successful treatment options [7, 8]. However, potential side-effects of pharmacotherapy, along with the risk of opioids addiction, make this option viable and safe only in the short term. As the number of patients with chronic aspecific LBP increases, so does the demand for safe and effective therapies. Among these, acupuncture has been widely investigated in recent times as possible options, proving to be a safe and effective therapy for chronic aspecific LBP [9,10,11]. Many different acupuncture protocols have been proposed for the management of chronic aspecific LBP. This Bayesian network meta-analysis investigated the available randomized control trials (RCTs) to try and identify which acupuncture protocol is the most effective for chronic aspecific LBP. Efficacy was measured in terms of pain (Visual Analogic Scale, VAS) and disability (Roland Morris Disability Questionnaire, RMQ) to investigate the efficacy of acupuncture on different aspects of the patients’ overall quality of life.
Material and methods
Search strategy
This Bayesian network meta-analysis was conducted according to the PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of healthcare interventions [12]. A guide protocol was preliminary drafted:
-
P (population): Chronic low back pain;
-
I (intervention): Acupuncture;
-
C (comparison): Standardized, sham, individual, auricular, electroacupuncture, acupuncture combined with Transcutaneous Electrical Nerve Stimulation (TENS);
-
O (outcomes): VAS, RMQ.
Data source and extraction
Two authors (A.M. and A.B.) independently performed the literature search in April 2022. The following databases were accessed: PubMed, Google scholar, Embase, and Scopus. The following keywords were used in combination: low, lumbar, back, lower, spine, pain, disability, management, therapy, treatments, acupuncture, auricular, tens, electroacupuncture, auricular, individualized, standardized, visual analogic scale, vas, Roland Morris questionnaire. The same authors independently performed the initial screening. If the title and abstract matched the topic, the article full-text was accessed. A cross reference of the bibliographies was also performed. Disagreement was debated and solved by a third author (N.M.).
Eligibility criteria
All the RCTs comparing two or more acupuncture modalities for aspecific chronic LBP were accessed. Only studies which investigated the efficacy of acupuncture on patients with symptoms lasting a minimum of 1.5 months, or with at least three episodes in the previous 12 months were considered eligible. Only studies involving patients aged 18 to 75 were considered. Aspecific LBP was defined as pain that was not arising from a specific pathoanatomical condition [5]. Given the authors language capabilities, articles in English, German, Italian, French and Spanish were eligible. Only level I of evidence studies, according to Oxford Centre of Evidence-Based Medicine [13], were considered. Studies reporting data over acupressure or percutaneous electrical nerve stimulation were not considered. Studies reporting the efficacy of acupuncture in patients with acute pain were not included, nor were those investigating the cervicothoracic segments. Studies investigating patients with neurological deficits were excluded, along with studies including patients with radicular pain (unless the radicular pain was only a minor complaint). Editorials, reviews, letters, opinion, technical notes, comments were not eligible, nor were biomechanical, cadaveric, or animal studies. Only articles reporting quantitative data under the outcomes of interest were considered for inclusion. Missing data under the outcomes of interest warranted exclusion from this study.
Data extraction
Two authors (A.M. and A.B.) independently performed data extraction the resulting articles for inclusion. Study generalities (author, year, journal, design, length of the follow-up) and patient demographic at baseline were extracted (number of samples and related mean BMI and age, percentage of female). For every treatment, the following data were retrieved: VAS, RMQ, adverse events. The groups considered were standard acupuncture alone, standard acupuncture with TENS, electroacupuncture, individualized acupuncture, and auricular acupuncture. The treatment group was classified as individualized acupuncture when the treating physician chose the needling points for each patient, without following a specific protocol. The treatment was defined as standard acupuncture when all patients were treated with the same protocol. Sham acupuncture was defined as the needling of points other than the known acupuncture points: as shallow needling of acupuncture points may also elicit a fibroblast reaction, this method was considered as a form of verum acupuncture [14]. The association of acupuncture with electrostimulation was considered separately.
Risk of bias assessment
The risk of bias assessment was conducted by two authors (A.M. and A.B.) independently. The Review Manager Software (The Nordic Cochrane Collaboration, Copenhagen) was used for the methodological quality assessment. The following risk of bias were evaluated: selection, detection, reporting, attrition, and other source of bias. For each comparison, the risk of bias was investigated using funnel plots. Plot asymmetries relates to greater risk of bias.
Statistical analysis
The statistical analyses were conducted by the senior author (F.M.). Baseline comparability was assessed through the IBM SPSS software. The analysis of variance (ANOVA) was used for analysis, with P values > 0.1 considered satisfactory. All other treatments rather than standardized, individual, auricular, electroacupuncture, combined with TENS, sham acupuncture were included in the “control group” and excluded from the analysis. The STATA Software/MP, Version 14.1 (StataCorporation, College Station, Texas, USA) was used for the statistical analyses. The NMA was performed through the STATA routine for Bayesian hierarchical random-effects model analysis. The inverse variance method was used for analysis, with standardized mean difference (STD) effect measure. The overall inconsistency was evaluated through the equation for global linearity via the Wald test. If the P value < 0.5, the null hypothesis cannot be rejected, and the consistency assumption could be accepted at the overall level of each treatment. Both confidence (CI) and percentile (PrI) intervals were set at 95%. For each comparison, edge plots were performed to display amount and interpolations of direct comparisons; interval plots were performed to rank the treatments according to their effect measure; and asymmetry of the funnel plots was associated with the greater risk of publication bias.
Results
Search result
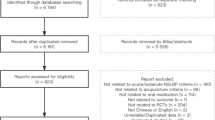
The literature search resulted in 817 RCTs. Four hundred and seven were excluded as they were duplicates. A further 330 studies were incompatible with the eligibility criteria: type of study (N = 89), not matching the topic of interest (N = 193), acupressure or percutaneous electrical nerve stimulation (N = 15), acute LBP (N = 11), concerning cervicothoracic segments (N = 5), presence of severe neurologic impairment or spine deformities (N = 3), acute setting (N = 2), old age (N = 1), language limitations (N = 2), other (N = 9). Another 13 studies were excluded as they did not report quantitative data under the outcomes of interest. This left 44 RCTs for the present study. The literature search results are shown in Fig. 1.

Flowchart of the literature search
Methodological quality assessment
Given the randomized design of the included studies, the risk of selection bias was low. Assessor blinding was performed in 75% (33 of 44) studies; however, the blinding methods were often biased, and the overall risk of detection bias was moderate. The risk of attrition and reporting biases were low to moderate, as was the risk of other bias. Concluding, the methodological quality assessment showed low to moderate risk of bias (Fig. 2).

Methodological quality assessment
Patient demographics
Data from 8338 procedures were retrieved. 56% of patients were women. The mean age of the patients was 48 ± 10.6 years. The mean BMI was 26.3 ± 2.2 kg/m2. The ANOVA test found moderate baseline comparability in symptoms duration (P > 0.05). Patient demographics are shown in Table 1.
Outcomes of interest
The individual group (SMD 5.00; 95% CI 2.02, 7.98) and the standard combined with TENS (SMD 5.00; 95% CI 2.03, 7.97) demonstrated the highest improvement of RMQ. The VAS score was lower in the standard combined with TENS group (SMD 3.92; 95% CI 3.28, 4.56). Considering the standard acupuncture group, different studies utilized similar protocols and acupuncture points and the results could thus be compared. The equation for global linearity did not find any statistically significant inconsistency in any of the network comparisons. Edge, interval, and funnel plots are shown in Fig. 3.

Results of the network comparisons
Discussion
According to the main findings of the present Bayesian network meta-analysis, individualized acupuncture and the standard protocol with TENS may represent the most effective acupuncture strategies for the management of chronic aspecific LBP. These two treatment protocols showed the highest improvements of VAS and RMQ. As verum acupuncture scored better than sham treatment, the present study points to the efficacy of acupuncture in the management of aspecific chronic LBP. This finding further supports current guidelines which recommend acupuncture as one of the possible first-line, non-pharmacological management modality for aspecific chronic LBP [6].
These results are consistent with previous studies [10, 11], which observed a superiority of acupuncture compared to sham treatment [57, 58]. A meta-analysis by Amaral et al. observed only moderate-quality evidence in favor of acupuncture treatment for LBP; however, this study focused only on trigger point acupuncture in the geriatric population, and the results are not directly comparable with those of the present cohort [9]. Nascimiento et al. also observed poor outcomes for acupuncture for LBP in the geriatric population [59]. While no specific characteristics could be highlighted in patients who responded to acupuncture for chronic pain [60], the role of age on the effectiveness of the therapy in the setting of LBP deserves further investigation. A meta-analysis by Mu and colleagues found that acupuncture has only limited effect on pain relief and improvement of the quality of life in the immediate to short term [61]. Li et al. highlighted that a treatment duration of at least 5 weeks is required to achieve 80% of the maximum analgesic effect [62] of acupuncture. Thus, the relatively short timeframe considered by Mu et al. (one to 12 weeks) [61], along with the high risk of bias of the included studies [61], may explain the differences in the observed results. The literature regarding the use of acupuncture in the acute setting is limited and, so far, no studies have been directed to analyze the literature regarding different types of acupuncture for the treatment of acute LBP. Thus, a direct comparison of the presented results with those of the acute setting is not possible. Overall, acupuncture seems to be modestly effective for the management of acute LBP, and the available studies agree that more high-quality work are required to gain more evidence around this topic [63, 64]. Considering the reluctance of many physicians to prescribe acupuncture in patients with chronic LBP, it is fundamental to highlight the efficacy of this treatment in comparison with sham acupuncture. However, the finding that individualized treatment is more effective than standard treatment suggests that a precise diagnosis of chronic LBP according to the criteria of traditional Chinese medicine and the choice of specific acupuncture points may be key for the efficacy of the treatment. This result confirms the clinical experience of the authors. The association of standard protocols with TENS yielded however results similar to those of individualized acupuncture.
This study has several limitations. The most important limitation is the heterogeneous protocols used. Given the randomized design of patient allocation, the risk of selection bias was low. However, some studies did not perform patients or personnel blinding, thus increasing the risk of detection and performance biases, respectively. General health measures were seldom reported, as were also information about the duration of previous symptoms, and type of pain (e.g., central sensitization). Previous conservative strategies were barely reported. Given the lack of quantitative data, the ethnicity of the patients was not analyzed separately. Given the heterogeneity of the protocols used, it was not possible to analyze the effects of the associations of acupuncture with other treatments such as pharmacological management and physio- and psychotherapy. Also, some acupuncture techniques such as moxibustion, cupping or scalp acupuncture were excluded from the study as the available data were not sufficient to grant inclusion. As a multimodal approach is often advisable to tackle the different organic and psychosocial aspects of chronic LBP [6, 65,66,67,68], further studies will be required to investigate the efficacy of different treatment associations and protocols. Furthermore, the available studies only allowed for a precise analysis of the effects of acupuncture in the population < 75 years old: targeted studies for this segment of the population will be required to investigate the efficacy of acupuncture in the elderly.
Conclusion
Verum acupuncture is more efficient than sham treatment for the non-pharmacological management of LBP. Among verum protocols, individualized acupuncture and standard acupuncture with TENS were the protocols that allowed for the highest improvement in pain and quality of life.
Availability of data and materials
The data underlying this article are available in the article and in its online supplementary material.
Abbreviations
- RCTs:
-
Randomized control trials
- LBP:
-
Low back pain
- VAS:
-
Visual analogic scale
- RMQ:
-
Roland Morris disability questionnaire
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- BMI:
-
Body mass index
- ANOVA:
-
Analysis of variance
- NMA:
-
Network meta-analysis
- STD:
-
Standardized mean difference
- CI:
-
Confidence interval
- PrI:
-
Percentile interval
References
Golob AL, Wipf JE. Low back pain. Med Clin North Am. 2014;98:405–28. https://doi.org/10.1016/j.mcna.2014.01.003.
Krismer M, van Tulder M. Strategies for prevention and management of musculoskeletal conditions. Low back pain (non-specific). Best Pract Res Clin Rheumatol. 2007;21:77–91. https://doi.org/10.1016/j.berh.2006.08.004.
Ganesan S, Acharya AS, Chauhan R, et al. Prevalence and risk factors for low back pain in 1355 young adults: a cross-sectional study. Asian Spine J. 2017;11:610–7. https://doi.org/10.4184/asj.2017.11.4.610.
Lee CA, Jang H-D, Moon JE, et al. The relationship between change of weight and chronic low back pain in population over 50 years of age: a nationwide cross-sectional study. Int J Environ Res Public Health. 2021. https://doi.org/10.3390/ijerph18083969.
Maher C, Underwood M, Buchbinder R. Non-specific low back pain. The Lancet. 2017;389:736–47. https://doi.org/10.1016/S0140-6736(16)30970-9.
Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American college of physicians. Ann Intern Med. 2017;166:514–30. https://doi.org/10.7326/M16-2367.
Migliorini F, Maffulli N, Baroncini A, et al. Opioids for chronic low back pain management: a Bayesian network meta-analysis. Expert Rev Clin Pharmacol. 2021;14:635–41. https://doi.org/10.1080/17512433.2021.1903316.
Migliorini F, Maffulli N, Eschweiler J, et al. Non-steroidal anti-inflammatory drugs and gabapentinoids for chronic lumbar pain: a Bayesian network meta-analysis of randomized controlled trials. Br Med Bull. 2021;138:85–95. https://doi.org/10.1093/bmb/ldab003.
Amaral LKB, Souza MB, Campos MGM, et al. Efficacy of conservative therapy in older people with nonspecific low back pain: a systematic review with meta-analysis and GRADE recommendations. Arch Gerontol Geriatr. 2020;90:104177. https://doi.org/10.1016/j.archger.2020.104177.
Huang J-F, Zheng X-Q, Chen D, et al. Can acupuncture improve chronic spinal pain? A systematic review and meta-analysis. Global Spine J. 2021;11:1248–65. https://doi.org/10.1177/2192568220962440.
Li Y-X, Yuan S-E, Jiang J-Q, et al. Systematic review and meta-analysis of effects of acupuncture on pain and function in non-specific low back pain. Acupunct Med. 2020;38:235–43. https://doi.org/10.1136/acupmed-2017-011622.
Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162:777–84. https://doi.org/10.7326/M14-2385.
Howick JCI, Glasziou P, Greenhalgh T, Heneghan C, Liberati A, Moschetti I, Phillips B, Thornton H, Goddard O, Hodgkinson M (2011) The 2011 Oxford CEBM Levels of Evidence. Oxford Centre for Evidence-Based Medicine Available at https://www.cebm.net/indexaspx?o=5653. www.https://www.cebm.net/
Miyazaki S, Hagihara A, Kanda R, et al. Applicability of press needles to a double-blind trial: a randomized, double-blind, placebo-controlled trial. Clin J Pain. 2009;25:438–44. https://doi.org/10.1097/AJP.0b013e318193a6e1.
Brinkhaus B, Witt CM, Jena S, et al. Acupuncture in patients with chronic low back pain: a randomized controlled trial. Arch Intern Med. 2006;166:450–7. https://doi.org/10.1001/archinte.166.4.450.
Camilotti BM, Leite N, Alberti D, et al. Effects of Ai Chi and Yamamoto new scalp acupuncture on chronic low back pain. Fisioter mov. 2015;28:723–30. https://doi.org/10.1590/0103-5150.028.004.ao09.
Ceccherelli F, Rigoni MT, Gagliardi G, et al. Comparison of superficial and deep acupuncture in the treatment of lumbar myofascial pain: a double-blind randomized controlled study. Clin J Pain. 2002;18:149–53. https://doi.org/10.1097/00002508-200205000-00003.
Cherkin DC, Eisenberg D, Sherman KJ, et al. Randomized trial comparing traditional Chinese medical acupuncture, therapeutic massage, and self-care education for chronic low back pain. Arch Intern Med. 2001;161:1081–8. https://doi.org/10.1001/archinte.161.8.1081.
Cherkin DC, Sherman KJ, Avins AL, et al. A randomized trial comparing acupuncture, simulated acupuncture, and usual care for chronic low back pain. Arch Intern Med. 2009;169:858–66. https://doi.org/10.1001/archinternmed.2009.65.
Cho Y-J, Song Y-K, Cha Y-Y, et al. Acupuncture for chronic low back pain: a multicenter, randomized, patient-assessor blind, sham-controlled clinical trial. Spine (Phila Pa 1976). 2013;38:549–57. https://doi.org/10.1097/BRS.0b013e318275e601.
Comachio J, Oliveira CC, Silva IFR, et al. Effectiveness of manual and electrical acupuncture for chronic non-specific low back pain: a randomized controlled trial. J Acupunct Meridian Stud. 2020;13:87–93. https://doi.org/10.1016/j.jams.2020.03.064.
Di Cesare A, Giombini A, Di Cesare M, et al. Comparison between the effects of trigger point mesotherapy versus acupuncture points mesotherapy in the treatment of chronic low back pain: a short term randomized controlled trial. Complement Ther Med. 2011;19:19–26. https://doi.org/10.1016/j.ctim.2010.11.002.
Giles LGF, Müller R. Chronic spinal pain syndromes: a clinical pilot trial comparing acupuncture, a nonsteroidal anti-inflammatory drug, and spinal manipulation. J Manipulative Physiol Ther. 1999;22:376–81. https://doi.org/10.1016/s0161-4754(99)70082-5.
Giles LGF, Muller R. Chronic spinal pain: a randomized clinical trial comparing medication, acupuncture, and spinal manipulation. Spine (Phila Pa 1976). 2003;28:1490–502. https://doi.org/10.1097/00007632-200307150-00003.
Grant DJ, Bishop-Miller J, Winchester DM, et al. A randomized comparative trial of acupuncture versus transcutaneous electrical nerve stimulation for chronic back pain in the elderly. Pain. 1999;82:9–13. https://doi.org/10.1016/S0304-3959(99)00027-5.
Haake M, Müller H-H, Schade-Brittinger C, et al. German Acupuncture Trials (GERAC) for chronic low back pain: randomized, multicenter, blinded, parallel-group trial with 3 groups. Arch Intern Med. 2007;167:1892–8. https://doi.org/10.1001/archinte.167.17.1892.
Hasegawa TM, Baptista AS, de Souza MC, et al. Acupuncture for acute non-specific low back pain: a randomised, controlled, double-blind, placebo trial. Acupunct Med. 2014;32:109–15. https://doi.org/10.1136/acupmed-2013-010333.
Hunter RF, McDonough SM, Bradbury I, et al. Exercise and auricular acupuncture for chronic low-back pain: a feasibility randomized-controlled trial. Clin J Pain. 2012;28:259–67. https://doi.org/10.1097/AJP.0b013e3182274018.
Inoue M, Kitakoji H, Ishizaki N, et al. Relief of low back pain immediately after acupuncture treatment–a randomised, placebo controlled trial. Acupunct Med. 2006;24:103–8. https://doi.org/10.1136/aim.24.3.103.
Itoh K, Itoh S, Katsumi Y, et al. A pilot study on using acupuncture and transcutaneous electrical nerve stimulation to treat chronic non-specific low back pain. Complement Ther Clin Pract. 2009;15:22–5. https://doi.org/10.1016/j.ctcp.2008.09.003.
Itoh K, Katsumi Y, Kitakoji H. Trigger point acupuncture treatment of chronic low back pain in elderly patients–a blinded RCT. Acupunct Med. 2004;22:170–7. https://doi.org/10.1136/aim.22.4.170.
Kalauokalani D, Cherkin DC, Sherman KJ, et al. Lessons from a trial of acupuncture and massage for low back pain: patient expectations and treatment effects. Spine (Phila Pa 1976). 2001;26(13):1418–24. https://doi.org/10.1097/00007632-200107010-00005.
Kennedy S, Baxter GD, Kerr DP, et al. Acupuncture for acute non-specific low back pain: a pilot randomised non-penetrating sham controlled trial. Complement Ther Med. 2008;16:139–46. https://doi.org/10.1016/j.ctim.2007.03.001.
Kerr DP, Walsh DM, Baxter D. Acupuncture in the management of chronic low back pain: a blinded randomized controlled trial. Clin J Pain. 2003;19:364–70. https://doi.org/10.1097/00002508-200311000-00004.
Leibing E, Leonhardt U, Köster G, et al. Acupuncture treatment of chronic low-back pain–a randomized, blinded, placebo-controlled trial with 9-month follow-up. Pain. 2002;96:189–96. https://doi.org/10.1016/s0304-3959(01)00444-4.
Liu L, Skinner MA, McDonough SM, et al. Acupuncture for chronic low back pain: a randomized controlled feasibility trial comparing treatment session numbers. Clin Rehabil. 2017;31:1592–603. https://doi.org/10.1177/0269215517705690.
Yong L, Min Y, Tao L, Xiaolong Z, Wen T, Mingyang G, Yonghe H. Effect of hand-ear acupuncture on chronic low-back pain: a randomized controlled trial. J Tradit Chin Med. 2019;39:587–94.
Macdonald AJ, Macrae KD, Master BR, et al. Superficial acupuncture in the relief of chronic low back pain. Ann R Coll Surg Engl. 1983;65:44–6.
Mendelson G, Selwood TS, Kranz H, et al. Acupuncture treatment of chronic back pain. Am J Med. 1983;74:49–55. https://doi.org/10.1016/0002-9343(83)91117-8.
Meng CF, Wang D, Ngeow J, et al. Acupuncture for chronic low back pain in older patients: a randomized, controlled trial. Rheumatology (Oxford). 2003;42:1508–17. https://doi.org/10.1093/rheumatology/keg405.
Molsberger AF, Mau J, Pawelec DB, et al. Does acupuncture improve the orthopedic management of chronic low back pain–a randomized, blinded, controlled trial with 3 months follow up. Pain. 2002;99:579–87. https://doi.org/10.1016/S0304-3959(02)00269-5.
Pach D, Yang-Strobel X, Lüdtke R, et al. Standardized versus individualized acupuncture for chronic low back pain: a randomized controlled trial. Evid Based Complement Alternat Med. 2013;2013: 125937. https://doi.org/10.1155/2013/125937.
Rajfur J, Pasternok M, Rajfur K, et al. Efficacy of selected electrical therapies on chronic low back pain: a comparative clinical pilot study. Med Sci Monit. 2017;23:85–100.
Sator-Katzenschlager SM, Scharbert G, Kozek-Langenecker SA, et al. The short- and long-term benefit in chronic low back pain through adjuvant electrical versus manual auricular acupuncture. Anesth Analg. 2004;98:1359–64. https://doi.org/10.1213/01.ane.0000107941.16173.f7.
Shankar N, Thakur M, Tandon OP, et al. Autonomic status and pain profile in patients of chronic low back pain and following electro acupuncture therapy: a randomized control trial. Indian J Physiol Pharmacol. 2011;55:25–36.
Szczurko O, Cooley K, Busse JW, et al. Naturopathic care for chronic low back pain: a randomized trial. PLoS ONE. 2007;2: e919. https://doi.org/10.1371/journal.pone.0000919.
Thomas KJ, MacPherson H, Thorpe L, et al. Randomised controlled trial of a short course of traditional acupuncture compared with usual care for persistent non-specific low back pain. BMJ. 2006;333:623. https://doi.org/10.1136/bmj.38878.907361.7C.
Witt CM, Jena S, Selim D, et al. Pragmatic randomized trial evaluating the clinical and economic effectiveness of acupuncture for chronic low back pain. Am J Epidemiol. 2006;164:487–96. https://doi.org/10.1093/aje/kwj224.
Yeung CKN, Leung MCP, Chow DHK. The use of electro-acupuncture in conjunction with exercise for the treatment of chronic low-back pain. J Altern Complement Med. 2003;9:479–90. https://doi.org/10.1089/107555303322284767.
Tsui MLK, Cheing GLY. The effectiveness of electroacupuncture versus electrical heat acupuncture in the management of chronic low-back pain. J Altern Complement Med. 2004;10:803–9. https://doi.org/10.1089/acm.2004.10.803.
Tsukayama H, Yamashita H, Amagai H, et al. Randomised controlled trial comparing the effectiveness of electroacupuncture and TENS for low back pain: a preliminary study for a pragmatic trial. Acupunct Med. 2002;20:175–80. https://doi.org/10.1136/aim.20.4.175.
Weiss J, Quante S, Xue F, et al. Effectiveness and acceptance of acupuncture in patients with chronic low back pain: results of a prospective, randomized, controlled trial. J Altern Complement Med. 2013;19:935–41. https://doi.org/10.1089/acm.2012.0338.
Yoo D-J, Jung J-Y, Chung S-H. Effects of the embedding acupuncture treatments for chronic low back pain patients. J Korean Med Rehabilit. 2015;25:105–12. https://doi.org/10.18325/jkmr.2015.25.4.105.
Yuan J, Purepong N, Hunter RF, et al. Different frequencies of acupuncture treatment for chronic low back pain: an assessor-blinded pilot randomised controlled trial. Complement Ther Med. 2009;17:131–40. https://doi.org/10.1016/j.ctim.2008.10.003.
Yun M, Shao Y, Zhang Y, et al. Hegu acupuncture for chronic low-back pain: a randomized controlled trial. J Altern Complement Med. 2012;18:130–6. https://doi.org/10.1089/acm.2010.0779.
Zaringhalam J, Manaheji H, Rastqar A, et al. Reduction of chronic non-specific low back pain: a randomised controlled clinical trial on acupuncture and baclofen. Chin Med. 2010;5:15. https://doi.org/10.1186/1749-8546-5-15.
Asano H, Plonka D, Weeger J. Effectiveness of acupuncture for nonspecific chronic low back pain: a systematic review and meta-analysis. Med Acupunct. 2022;34:96–106. https://doi.org/10.1089/acu.2021.0057.
Xiang Y, He J-Y, Tian H-H, et al. Evidence of efficacy of acupuncture in the management of low back pain: a systematic review and meta-analysis of randomised placebo- or sham-controlled trials. Acupunct Med. 2020;38:15–24.
Nascimento PRCd, Costa LOP, Araujo AC, et al. Effectiveness of interventions for non-specific low back pain in older adults. Syst Rev Meta-Anal Physiother. 2019;105:147–62. https://doi.org/10.1016/j.physio.2018.11.004.
Foster NE, Vertosick EA, Lewith G, et al. Identifying patients with chronic pain who respond to acupuncture: results from an individual patient data meta-analysis. Acupunct Med. 2021;39:83–90. https://doi.org/10.1177/0964528420920303.
Mu J, Furlan AD, Lam WY, et al. Acupuncture for chronic nonspecific low back pain. Cochrane Database Syst Rev. 2020;12:CD013814. https://doi.org/10.1002/14651858.CD013814.
Li C, Pei Q, Chen Y, et al. The response-time relationship and covariate effects of acupuncture for chronic pain: a systematic review and model-based longitudinal meta-analysis. Eur J Pain. 2020;24:1653–65. https://doi.org/10.1002/ejp.1617.
Su X, Qian H, Chen B, et al. Acupuncture for acute low back pain: a systematic review and meta-analysis. Ann Palliat Med. 2021;10:3924–36.
Lee J-H, Choi T-Y, Lee MS, et al. Acupuncture for acute low back pain: a systematic review. Clin J Pain. 2013;29:172–85. https://doi.org/10.1097/AJP.0b013e31824909f9.
Madhusudhan SK. Novel analgesic combination of tramadol, paracetamol, caffeine and taurine in the management of moderate to moderately severe acute low back pain. J Orthop. 2013;10(3):144–8. https://doi.org/10.1016/j.jor.2013.07.001.
Andrea De Giorgio, Padulo J, Goran K (2018) Effectiveness of yoga combined with back school program on anxiety, kinesiophobia and pain in people with non-specific chronic low back pain: a prospective randomized trial, 8: 104–112. https://doi.org/10.11138/mltj/2018.8.1.104
Dimer da Luz R, De Silva Silva M, Steffen Evaldt A, et al. Neuromuscular electrical stimulation associated with core stability exercises in nonspecific postural low back pain: a randomized clinical trial. Muscle Ligaments Tendons J. 2019;09:446. https://doi.org/10.32098/mltj.03.2019.20.
Depaoli Lemos VJ, Selau RC, Blos C, et al. Electroacupuncture and transcutaneous electrical nerve stimulation in chronic nonspecific low back pain: a blind randomized clinical trial. Muscle Ligaments Tendons J. 2021;11:719. https://doi.org/10.32098/mltj.04.2021.15.
Acknowledgements
None
Funding
Open Access funding enabled and organized by Projekt DEAL. No external source of funding was used.
Author information
Authors and Affiliations
Contributions
FM involved in conception and design of the study, literature search, data extraction, methodological quality assessment, writing, statistical analysis, interpretation of data, and final approval; AB involved in literature search, data extraction, methodological quality assessment, writing, and final approval; NM involved in revision and final approval; and FM and AK involved in supervision and final approval. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable
Competing interests
Professor Maffulli is Editor in Chief of the Journal of Orthopaedic Surgery and Research.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Baroncini, A., Maffulli, N., Eschweiler, J. et al. Acupuncture in chronic aspecific low back pain: a Bayesian network meta-analysis. J Orthop Surg Res 17, 319 (2022). https://doi.org/10.1186/s13018-022-03212-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-022-03212-3