
Abstract
Background
The interaction of functional and mechanical deficits in chronic ankle instability remains a major issue in current research. After an index sprain, some patients develop sufficient coping strategies, while others require mechanical support. This study aimed to analyze persisting functional deficits in mechanically unstable ankles requiring operative stabilization.
Methods
We retrospectively analyzed the functional testing of 43 patients suffering from chronic, unilateral mechanical ankle instability (MAI) and in which long-term conservative treatment had failed. Manual testing and arthroscopy confirmed mechanical instability. The functional testing included balance test, gait analysis, and concentric-concentric, isokinetic strength measurements and was compared between the non-affected and the MAI ankles.
Results
Plantarflexion, supination, and pronation strength was significantly reduced in MAI ankles. A sub-analysis of the strength measurement revealed that in non-MAI ankles, the peak pronation torque was reached earlier during pronation (maximum peak torque angle at 20° vs. 14° of supination, p < 0.001). Furthermore, active range of motion was reduced in dorsiflexion and supination. In balance testing, patients exhibited a significant increased perimeter for the injured ankle (p < 0.02). During gait analysis, we observed an increased external rotation in MAI (8.7 vs. 6.8°, p<0.02).
Conclusions
This study assesses functional deficits existent in a well-defined population of patients suffering from chronic MAI. Impairments of postural sway, gait asymmetries, and asymmetric isokinetic strength can be observed despite long-term functional treatment. The finding that pronation strength is particularly reduced with the foot in a close-to-accident position indicates potential muscular dysfunction in MAI. Possibly, these deficits alongside the underlying mechanical instability characterize patients requiring mechanical stabilization.
Similar content being viewed by others


Introduction
Perceived or subjective instability with feelings of giving way, pain, and recurrent sprains defines the clinical presentation of chronic ankle instability (CAI). This widespread phenomenon can be divided into the two etiologies of functional (FAI) and mechanical instability (MAI) [1]. The choice of the appropriate therapeutic approach for CAI patients requires the distinction between these two etiologies: functional deficits may best be addressed by functional, conservative therapy, since deficits in the sensorimotor system and postural control respond well to focused exercise regimes [2, 3]. Contrarily, MAI can only be treated mechanically using additional stabilization such as ankle taping, orthoses, or lateral ligament repair [4,5,6].
Concerning sensorimotor deficits, it has been described that postural control and strength are altered in FAI subjects [3, 7]. Impaired postural control has been one of the few factors which is consistently associated with functional impairment in CAI [3, 8, 9]. Furthermore, a recent systematic review found that impairments of peroneal reaction time and pronation strength strongly contribute to perceived ankle instability in a chronic population [10]. Also, strength deficits resulting from ankle injuries have been described especially in plantarflexion and pronation strength, while dorsiflexion and supination strength seems to remain rather unaffected [11, 12]. It is thought that spinal and cortical pathways may lead to an inhibition of neuromuscular activity and thus contribute to these persisting deficiencies in CAI patients [13].
Furthermore, it has been shown that CAI patients display alterations during gait as for instance a laterally deviated pressure distribution, an increased inversion angle, and a decreased foot clearance [14,15,16]. Whether or not these alterations during gait are caused by deficits in sensorimotor control, strength imbalance or other factors remains unclear [17,18,19]. However, CAI patients seem to benefit from locomotor training by improving mediolateral pressure shift during gait [18]. Furthermore, strengthening and increasing preactivation of the peroneus longus muscle have been shown to reduce ankle inversion during gait [14, 18]. On the other hand, also mechanical stabilization like ankle orthoses, taping, or operative stabilization improve gait performance by reducing maximal ankle inversion [20, 21], which can be attributed to the mechanical insufficiency which is destabilizing the joint during the ankle sprain mechanism itself [4]. Furthermore, the finding that functional performance also improves after mechanical stabilization like lateral ligament reconstruction or wearing an orthosis underlines the fact that the two etiologies are intertwined [20, 22], which of the observed alterations can be attributed to mechanical and/or functional insufficiencies is the focus of ongoing research.
Current literature suggests that a certain degree of mechanical instability cannot be compensated by functional training but may instead require mechanical stabilization [8, 23]. Whether an undetermined severity of mechanical insufficiency inevitably leads to an additional perception of instability, according to the model of Hiller et al. [24], remains unclear in current literature [4, 25].
Especially in the clinical approach to CAI patients, it is important to distinguish between those suffering from predominantly functional deficits and those patients suffering due to an insufficient mechanical stability [25, 26]. Ultimately, it may be suggested that only the latter will benefit from operative stabilization, while the others should be treated conservatively [2, 6, 27, 28]. As mentioned above, the exact definitions of CAI, FAI, and MAI have been subject to increasing debate in the last decade [29]. It is of note that many earlier studies did not differentiate the patients’ mechanical and functional insufficiencies possibly because quantifying mechanical ankle instability remains a diagnostic challenge [25]. At present, the extent to which FAI and MAI interact remains unclear [1, 10, 24, 30].
The aim of this study was to assess certain functional performance deficits in patients with unilateral, clinically apparent MAI which were scheduled for lateral ligament repair due to persisting symptoms despite previous long-term conservative treatment.
Methods
Study design
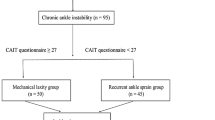
We executed a single group cross-sectional retrospective analysis with a random statistical sample of 43 patients with MAI scheduled for operative lateral ligament repair which met the eligibility criteria (Fig. 1). The experiment was approved by the local ethics committee (EKNZ 2019-00241); it was retrospectively registered at the German Registry of Clinical Trials (# DRKS00021681) and conducted in accordance with the latest version of the Declaration of Helsinki.

CONSORT flow chart. This figure shows the selection process of patients through the trial according to the criteria recommended in the CONSORT guidelines
Participants
We screened the records of 77 patients that were scheduled for ligament repair of the talocrural joint and synthesized 43 patients (22 female and 21 male, age of 26 ± 9.8 years height 1.73 ± 0.1 m, weight of 74.1 ± 14.8 kg) complying with inclusion criteria characteristic for MAI with reference to recent publications (Fig. 1) [26, 31]. All of these patients had performed functional testing prior to surgery to assess the extent of persisting unilateral, functional deficits. They included maximal isokinetic strength measurements [3, 7], posture [3, 8, 9], and gait control [15, 16].
Chronic ankle instability was defined according to the current recommendations with ongoing symptoms of at least 6 months including recurrent sprains reported by the patients, pain, and impairments with perceived instability during sportive activity [30]. Clinical examination including the anterior talar drawer and talar tilt test was performed by an orthopedic surgeon; procedures confirmed unilateral mechanical ankle instability [32]. The included population was further diagnosed using magnetic resonance imaging (MRI) findings of one or two lateral ligament injuries (ruptures, scar tissue) [33]. During surgery, the presence of MAI was confirmed arthroscopically according to the recommendations previously described in the literature [34].
Exclusion criteria were a history of injury other than ligamentous injuries, peroneal tendon injury, osteochondral lesions on MRI, injury to the syndesmotic, or to the deltoid ligament complex. Further exclusion criteria were bilateral history of ligamentous injury or ankle sprain, Beighton score greater than four [35], fracture of the contralateral side, or other neuromuscular injuries interfering with the measurement.
According to the established treatment algorithms, all patients had received a controlled conservative treatment by an athletic trainer or physical therapist including bilateral physical therapy, strength training, and sensorimotor training for a duration of at least 3 to 6 months prior to being scheduled for surgery [2, 26]. Thus, only patients with persisting perceived instability despite previous conservative treatment were scheduled for surgery.
In accordance with the definitions in current literature [30], this forms a very homogenous cohort of patients in which unilateral MAI is the predominant pathology.
Functional testing
The functional testing consisted of monoarticular and multiarticular tests characterized by a progressively increasing level of complexity [3, 7,8,9]. Isolated isokinetic strength testing was followed by a balance test (stabilometry) for the assessment of postural control and a gait analysis [15, 16] using a treadmill with integrated pedobarography.
Isokinetic maximal strength
Maximal strength was assessed by an isokinetic dynamometer (Humac Norm, CSMi, Stoughton, MA, USA) at a movement speed of 30°/s for plantar- and dorsiflexion. Patients laid in a prone position and the foot was tightly fixed to the footplate with Velcro straps, while the shank and the thigh were tied to the seat with a belt as described in the literature [36]. The plantarflexion/dorsiflexion axis of the upper ankle joint (best guessed by the intermalleolar axis) coincided with the rotation axis of the lever arm. For the measurements of supination and pronation, the patient was sitting semi-recumbent with the shank fixed at the leg support and the foot fixed to the footplate with Velcro straps [36, 37]. The axis of rotation was aligned with the axis of the lower ankle joint as defined by the dynamometer instructions. Prior to strength assessments, the patients performed three trials for familiarization. Recording sessions consisted of two sets with five repetitions (concentric-concentric) at maximum effort. Furthermore, active range of motion during the isokinetic strength testing was recorded. The uninjured leg was always measured first. Average measures of peak torque, peak torque angle, i.e., the angle where peak torque was reached, and range of motion out of the five trials were used for further analyses. To further evaluate the strength during the movement, we additionally extracted the torque produced across the range of motion (ROM) in steps of 5° starting from 20° of supination until 10° of pronation, since this active ROM was achieved by all participants. According to the most widely used definitions in the literature, for the purpose of this study, the most appropriate definitions of the movement around the ankle joint were supination and pronation even though internal and external rotation as well as eversion and inversion were naturally part of the motion [38, 39].
Postural control
For measuring postural control, a single-legged balance test was performed in a dynamic condition [40] on a ProKin Type B line system (TecnoBody, Dalmine, Italy). The subjects stood barefoot with orthograde upright posture and kept hands on their hips and directed their head forward. They were instructed to stand as still as possible, with the free leg not touching the other leg and the knee slightly flexed at each individual’s comfortable angle. Measurements started with the unaffected leg first and two trials were performed over a period of 30 s each, separated by 1 min breaks as previously described in the literature [41]. The center of pressure (COP) displacement was recorded and averaged for the medio-lateral and the anterior-posterior direction; the 90% ellipse of the COP’s area was calculated [42]. This has previously been used a valid and reliable measure of postural control [8, 41].
Gait analysis
Gait analysis was performed barefoot while walking on an automated treadmill equipped with integrated pressure distribution platform since overground measurement was not feasible in the available setting (FDM-T, zebris Medical GmbH, Isny, Germany). Walking speed was adjusted to the individual’s preferred gait speed between 4 and 6 km/h as described in current literatur e[43]. Spatiotemporal parameters were assessed using the integrated pressure plate. According to the literature [18, 44], the distribution of the plantar pressure along the sagittal line of the foot was measured during the stance phase and a deviation angle between the direction of gait and the sagittal orientation of the foot was calculated. Positive values equal an external rotation of the foot during stance phase. Additionally, the loading shift from posterior to anterior in percent of the stance phase was calculated to estimate gait symmetry. Deducted from the literature [45], this was done under the assumption that unequally distributed weight bearing with an increased time resting on the posterior part of the foot could be attributed to avoidance of proper active weight bearing and plantarflexion during gait.
Statistical analysis
For statistical comparison between the non-affected and the MAI ankle, a repeated measure analysis of variance with the factor “group” (MAI affected ankle, non-affected ankle) was calculated after checking for normal distribution using Kolmogorov-Smirnov test and sphericity with Mauchly’s test. The level of significance was set at p < 0.05. To correct for multiple testing and resulting cumulative type I error, Bonferroni corrections were applied in the sub-analysis of pronation strength by pronation angle with 15 measurements, resulting in a significance level at p < 0.003 for this analysis. Values are presented as means ± standard deviation.
The statistical analysis was performed using SPSS 24 (SPSS Inc., Chicago, USA).
Results
Strength measurements
Statistical analysis revealed a significant reduction in maximal pronation strength (− 14%, p < 0.05), supination strength (− 16%, p < 0.05), as well as in plantarflexion strength (− 21%, p < 0.05), while dorsiflexion did not show a significant difference for the MAI ankle compared to the non-affected ankle joint (Table 1). The peak torque angles differed significantly between the non-affected and the MAI ankle only for the pronation strength: the MAI ankles showed a peak torque at 14° of supination, while the non-affected ankles produced the maximum pronation strength already at a 20° supination angle (Table 1). This finding is supported by the sub-analysis of pronation strength with reference to the ankle joint position: the maximum torque occurs generally during the early phase of concentric pronation in which the foot is still supinated (Fig. 2). The maximum difference in torque between the MAI and non-MAI ankle is significantly different in the early phase of pronation reflected by a difference of 3.7 Nm (MAI at 10.4 Nm and non-MAI at 14.1 Nm torque, p < 0.003).

Isokinetic, concentric pronation strength according to the joint position. **p < 0.003, *p < 0.02
Active range of motion
Changes in active ROM are illustrated in Table 2. The active ROM showed a significantly increased dorsiflexion by 3.6° (p < 0.05) and a significant decrease of 3.2° in supination in the MAI compared to the non-affected ankle joint (p < 0.05). The differences during active plantarflexion of 2.2° and pronation (1.1°) did not reach statistical significance (both p = 0.06).
Postural control
As illustrated in Table 3, postural sway was increased in single leg stance when subjects stood on the MAI food compared to the not affected food. The MAI ankle had a 10% larger perimeter (COP-P) and a 28% augmented ellipse area of the center of pressure (COP-A) compared to the non-affected ankle.
Gait analysis
Spatiotemporal analysis of locomotion on the treadmill revealed that the MAI foot was significantly further externally rotated than the healthy contralateral foot by 1.9° (p < 0.05). The shift from rearfoot to forefoot as a measure of gait symmetry was not significantly different between the affected and the non-affected ankle (Table 4).
Discussion
This study assessed functional deficits existent in a population of patients suffering from unilateral MAI. According to the available evidence, we chose a testing setup that reflects the different modalities of potential functional impairments: strength measurements and range of motion to assess deficits in active joint control, a test for postural sway to control for sensorimotor deficits, and gait analysis for dynamic joint control during gait [8, 19, 27, 29, 30]. While it is clear that there are numerous functional tests in the assessment of chronic ankle instability, the tests chosen result in a sound impression of potential deficits [27, 30]. A significant reduction in strength, an impaired postural control, and subtle changes of kinematics during locomoting were observed unilaterally on the affected side. Applying our findings to patients with persisting subjective instability despite functional treatment may help to identify those patients that will benefit from mechanical stabilization, e.g., bracing or surgery.
Comparable to our data, several studies have provided evidence that concentric pronation and supination strength are impaired in CAI [10,11,12]. The novel finding in this study was that the joint angle in which the maximum pronation strength can be produced is significantly different between the two ankles (MAI 14° vs. non-MAI 20° of supination). The detailed analysis according to the joint position showed that it is especially in the early phase of pronation where a significant strength deficit exists (Fig. 2). This pattern is of high clinical relevance regarding joint stabilization during gait because it will limit the ability to actively prevent excessive supination once the joint comes close to a prone-to-injury position [14, 17, 46]. The etiology behind this observation may either be related to fear of pain approaching the end-range supination, which unfortunately was not systematically recorded; it may also be a shift in torque curve due to the general decrease in ROM. The strength deficits have further been attributed to neuromuscular impairment as well as muscle atrophy [7, 47]. Also, earlier studies revealed that delayed peroneal reaction time is a characteristic of CAI patients [48], which can be improved by functional training [18]. However, since long-term functional treatment had not lead to a sufficient alleviation of symptoms in this study’s population, it may be suggested that the combination of pronounced end-range strength deficits in pronation with clinically apparent, unilateral mechanical instability results in the inability to actively prevent an ankle sprain on the previously injured side. Whether or not these unilateral impairments of end-range pronation strength are caused by the mechanical instability itself, fear of pain or posttraumatic neuromuscular dysfunction cannot be concluded. However, in our view, these patients may not be able to develop a sufficient functional performance in order to cope with their mechanical deficits. In summary, the clinical application of this finding could be that patients presenting with deficits in the end-range pronation strength and clinically apparent mechanical ankle instability will benefit from mechanical treatment, e.g., operative ligament reconstruction.
The impairments of postural sway have been widely described in the literature [10]. However, in our population, the differences in balance testing of approximal 10% were not as pronounced as in other studies [3, 7]. Furthermore, it has been shown that functional adaptations like preparatory neuromuscular activation capacitate patients to cope with mechanical insufficiencies [3, 49, 50]. Since all patients in our population had received long-term conservative treatment, it may be assumed that in these patients, the potential benefit resulting from functional training had been exhausted. Since the modalities of conservative training were not controlled for in this observational study, we are unable to conclude the reasons why conservative treatment was not successful in individual cases. From a clinical point of view, it is important to reflect upon persisting unilateral functional deficits in unilateral mechanical instability. Potentially, the observed deficit in postural control may therefore be attributed to a mechanical instability that lays beyond functional compensation. This supports the finding that the mechanical deficit itself impairs functional performance [4, 8, 46]. Again, in a clinical setting this could mean that a certain degree of mechanical instability can never be compensated and in patients with persisting perceived instability (non-copers) may require operative stabilization. Future studies need to clarify whether different degrees of severity of MAI also show different degrees of the functional deficits reported in this study. Potentially, this will also allow to estimate the risk for associated injuries following lateral ankle instability and therefore increase the therapeutic value [1, 28, 51, 52]. To achieve this, however, a reproducible manner of quantitively assessing MAI is indispensable.
Several studies have also analyzed gait in patients suffering from chronic ankle instability [21, 52]. In our analysis, we aimed to monitor whether mechanical insufficiency leads to subtle gait imbalances. While walking at a preferred speed, the distribution of weight during the stance phase showed no difference between rear- and forefoot on either leg resulting in a harmonic gait pattern. However, the foot in which mechanical instability is present was set with a slightly increased external rotation of 1.9°. This is comparable to the findings in earlier publications, where CAI had not yet been further divided into MAI vs. FAI [15, 16]. This phenomenon of a more pronounced exorotated foot may be interpreted as a subconscious preventive adaptation leading to a broader mediolateral distribution of weight due to increased support surface which will help stabilizing the ankle joint during gait [14, 18, 21]. As a limitation, it needs to be respected that kinematic adaptations take place during treadmill walking as opposed to overground [43]. However, since we compared intra-subject differences, we consider our results valid in regard to gait adaptation as a component of unilateral MAI, since the observable differences, that take place due to the treadmill condition were assumed to affect both ankles in the same way [43, 53].
Finally, to underscore these novel findings, it is promising to continue developing means for quantifying mechanical ankle instability like 3D stress-MRI [54]. Future research may then be able to establish cutoff values of severe, chronic mechanical ankle instability in which functional treatment is likely to fail and early operative stabilization should be recommended.
In addition to quantifying the individual’s mechanical insufficiency, these findings will require future confirmation and a prospective study design including FAI-patients and postoperative analysis in a clinical setting.
As a limitation, in the present retrospective analysis, we were not able to quantify the amount of perceived instability via questionnaires. However, all patients agreed to undergo operative lateral ligament repair, which makes it evident that perceived instability and subjective malfunction must have been high. Unfortunately, we were unable to retrospectively distinguish those with predominantly pathological talar tilt vs. anterior drawer in order to correlate our findings to ATFL vs. CFL rupture, which should be a focus of additional research.
Conclusions
This retrospective analysis shows certain functional characteristics that persist in patients suffering from MAI despite functional treatment. Especially the maldistribution of peroneal strength could impede functional coping of mechanical deficits. This may support the observation that severe mechanical instability cannot be compensated and causes functional impairment itself. Thus, a certain degree of mechanical instability will eventually require operative stabilization. Future research should focus on quantifying mechanical ankle instability to verify this hypothesis.
Availability of data and materials
Data summarized in this study can be made available upon reasonable request.
Abbreviations
- CAI:
-
Chronic ankle instability
- MAI:
-
Mechanical ankle instability
- FAI:
-
Functional ankle instability
- ROM:
-
Range of motion
- COP:
-
Center of pressure
References
Hertel J, Corbett RO. An updated model of chronic ankle instability. J Athl Train. 2019;54:572–88.
Kaminski TW, Hertel J, Amendola N, Docherty CL, Dolan MG, Hopkins JT, et al. National Athletic Trainers’ Association position statement: conservative management and prevention of ankle sprains in athletes. J Athl Train. 2013;48:528–45.
Munn J, Sullivan SJ, Schneiders AG. Evidence of sensorimotor deficits in functional ankle instability: a systematic review with meta-analysis. J Sci Med Sport. 2010;13:2–12.
Gehring D, Faschian K, Lauber B, Lohrer H, Nauck T, Gollhofer A. Mechanical instability destabilises the ankle joint directly in the ankle-sprain mechanism. Br J Sports Med. 2014;48:377–82.
Lohrer H, Alt W, Gollhofer A. Neuromuscular properties and functional aspects of taped ankles. Am J Sports Med. 1999;27:69–75.
Maffulli N, Del Buono A, Maffulli GD, Oliva F, Testa V, Capasso G, et al. Isolated anterior talofibular ligament Brostrom repair for chronic lateral ankle instability: 9-year follow-up. Am J Sports Med. 2013;41:858–64.
Arnold BL, Linens SW, de la Motte SJ, Ross SE. Concentric evertor strength differences and functional ankle instability: a meta-analysis. J Athl Train. 2009;44:653–62.
Chen H, Li H-Y, Zhang J, Hua Y-H, Chen S-Y. Difference in postural control between patients with functional and mechanical ankle instability. Foot Ankle Int. 2014;35:1068–74.
Gribble PA, Hertel J, Plisky P. Using the Star Excursion Balance Test to assess dynamic postural-control deficits and outcomes in lower extremity injury: a literature and systematic review. J Athl Train. 2012;47:339–57.
Thompson C, Schabrun S, Romero R, Bialocerkowski A, van Dieen J, Marshall P. Factors contributing to chronic ankle instability: a systematic review and meta-analysis of systematic reviews. Sports Med. 2018;48:189–205.
Fraser JJ, Koldenhoven RM, Jaffri AH, Park JS, Saliba SF, Hart JM, et al. Foot impairments contribute to functional limitation in individuals with ankle sprain and chronic ankle instability. Knee Surg Sports Traumatol Arthrosc. 2018.
Wisthoff B, Matheny S, Struminger A, Gustavsen G, Glutting J, Swanik C, et al. Ankle strength deficits in a cohort of collegiate athletes with chronic ankle instability. J Sport Rehabil. 2018:1–22.
Kim K-M, Ingersoll CD, Hertel J. Altered postural modulation of Hoffmann reflex in the soleus and fibularis longus associated with chronic ankle instability. J Electromyogr Kinesiol. 2012;22:997–1002.
Delahunt E, Monaghan K, Caulfield B. Altered neuromuscular control and ankle joint kinematics during walking in subjects with functional instability of the ankle joint. Am J Sports Med. 2006;34:1970–6.
Morrison KE, Hudson DJ, Davis IS, Richards JG, Royer TD, Dierks TA, et al. Plantar pressure during running in subjects with chronic ankle instability. Foot Ankle Int. 2010;31:994–1000.
Schmidt H, Sauer LD, Lee SY, Saliba S, Hertel J. Increased in-shoe lateral plantar pressures with chronic ankle instability. Foot Ankle Int. 2011;32:1075–80.
Feger MA, Donovan L, Hart JM, Hertel J. Lower extremity muscle activation in patients with or without chronic ankle instability during walking. J Athl Train. 2015;50:350–7.
Feger MA, Hart JM, Saliba S, Abel MF, Hertel J. Gait training for chronic ankle instability improves neuromechanics during walking. J Orthop Res. 2017 [cited 2019 Apr 5]; Available from: http://doi.wiley.com/10.1002/jor.23639.
Hiller CE, Nightingale EJ, Lin C-WC, Coughlan GF, Caulfield B, Delahunt E. Characteristics of people with recurrent ankle sprains: a systematic review with meta-analysis. Br J Sports Med. 2011;45:660–72.
Gehring D, Wissler S, Lohrer H, Nauck T, Gollhofer A. Expecting ankle tilts and wearing an ankle brace influence joint control in an imitated ankle sprain mechanism during walking. Gait Posture. 2014;39:894–8.
Fereydounnia S, Shadmehr A, Attarbashi Moghadam B, Talebian Moghadam S, Mohsen Mir S, Salemi S, et al. Comparison of distal versus proximal-distal kinesio taping effects on gait initiation profile in athletes with functional ankle instability. Muscle Ligaments Tendons J. 2019;09:246.
Cho B-K, Park J-K, Choi S-M, SooHoo NF. The effect of peroneal muscle strength on functional outcomes after the modified Broström procedure for chronic ankle instability. Foot Ankle Int. 2018;39:105–12.
Li H-Y, Zheng J-J, Zhang J, Cai Y-H, Hua Y-H, Chen S-Y. The improvement of postural control in patients with mechanical ankle instability after lateral ankle ligaments reconstruction. Knee Surg Sports Traumatol Arthrosc. 2016;24:1081–5.
Hiller CE, Kilbreath SL, Refshauge KM. Chronic ankle instability: evolution of the model. J Athl Train. 2011;46:133–41.
Wenning M, Lohrer H, Gollhofer A, Gehring D. In vivo arthrometer measurements of mechanical ankle instability—a systematic review. J Orthop Res. 2019 [cited 2019 Apr 1]; Available from: https://onlinelibrary.wiley.com/doi/abs/10.1002/jor.24280.
Michels PH, Calder J, Matricali G, Glazebrook M, Guillo S, et al. Searching for consensus in the approach to patients with chronic lateral ankle instability: ask the expert. Knee Surg Sports Traumatol Arthrosc. 2018;26:2095–102.
Guillo S, Bauer T, Lee JW, Takao M, Kong SW, Stone JW, et al. Consensus in chronic ankle instability: aetiology, assessment, surgical indications and place for arthroscopy. Orthopaed Traumatol Surg Res. 2013;99:S411–9.
Malliaropoulos N, Ntessalen M, Papacostas E, Longo UG, Maffulli N. Reinjury after acute lateral ankle sprains in elite track and field athletes. Am J Sports Med. 2009;37:1755–61.
Delahunt E, Coughlan GF, Caulfield B, Nightingale EJ, Lin C-WC, Hiller CE. Inclusion criteria when investigating insufficiencies in chronic ankle instability. Med Sci Sports Exerc. 2010;42:2106–21.
Gribble PA, Delahunt E, Bleakley CM, Caulfield B, Docherty CL, Fong DT-P, et al. Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the International Ankle Consortium. J Athl Train. 2014;49:121–7.
Brown CN, Ko J, Rosen AB, Hsieh K. Individuals with both perceived ankle instability and mechanical laxity demonstrate dynamic postural stability deficits. Clin Biomech. 2015;30:1170–4.
van Dijk C, Lim LS, Bossuyt PM, Marti RK. Physical examination is sufficient for the diagnosis of sprained ankles. J Bone Joint Surg (Br). 1996;78:958–62.
Jung H-G, Kim N-R, Kim T-H, Eom J-S, Lee D-O. Magnetic resonance imaging and stress radiography in chronic lateral ankle instability. Foot Ankle Int. 2017;38:621–6.
Hintermann B, Boss A, Schä D. Arthroscopic findings in patients with chronic ankle instability. Am J Sports Med. 2002;30:402–9.
Yeo ED, Park JY, Kim JH, Lee YK. Comparison of outcomes in patients with generalized ligamentous laxity and without generalized laxity in the arthroscopic modified Broström operation for chronic lateral ankle instability. Foot Ankle Int. 2017;38:1318–23.
Gobbo S, Bergamin M, Bullo V, Bergamo M, Bocalini DS, di Blasio A, et al. Reliability of an isometric and isokinetic strength testing protocol of the knee and ankle in young adults. Muscle Ligaments Tendons J. 2019;09:348.
Amaral De Noronha M, Borges NG. Lateral ankle sprain: isokinetic test reliability and comparison between invertors and evertors. Clin Biomech. 2004;19:868–71.
Greiner TM. The jargon of pedal movements. Foot Ankle Int. 2007;28:109–25.
Wu G, Siegler S, Allard P, Kirtley C, Leardini A, Rosenbaum D, et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion--part I: ankle, hip, and spine. International Society of Biomechanics. J Biomech. 2002;35:543–8.
Zhao W, You H, Jiang S, Zhang H, Yang Y, Zhang M. Effect of Pro-kin visual feedback balance training system on gait stability in patients with cerebral small vessel disease. Medicine (Baltimore). 2019;98:e14503.
Muehlbauer T, Roth R, Mueller S, Granacher U. Intra and intersession reliability of balance measures during one-leg standing in young adults. J Strength Cond Res. 2011;25:2228–34.
Ritzmann R, Lee K, Krause A, Gollhofer A, Freyler K. Stimulus prediction and postural reaction: phase-specific modulation of soleus H-reflexes is related to changes in joint kinematics and segmental strategy in perturbed upright stance. Front Integr Neurosci. 2018;12:62.
Malatesta D, Canepa M, Menendez FA. The effect of treadmill and overground walking on preferred walking speed and gait kinematics in healthy, physically active older adults. Eur J Appl Physiol. 2017;117:1833–43.
Drewes LK, McKeon PO, Paolini G, Riley P, Kerrigan DC, Ingersoll CD, et al. Altered ankle kinematics and shank-rear-foot coupling in those with chronic ankle instability. J Sport Rehabil. 2009;18:375–88.
Novacheck TF. The biomechanics of running. Gait Posture. 1998;19.
Gutierrez GM, Knight CA, Swanik CB, Royer T, Manal K, Caulfield B, et al. Examining neuromuscular control during landings on a supinating platform in persons with and without ankle instability. Am J Sports Med. 2012;40:193–201.
Feger MA, Snell S, Handsfield GG, Blemker SS, Wombacher E, Fry R, et al. Diminished foot and ankle muscle volumes in young adults with chronic ankle instability. Orthopaed J Sports Med. 2016;4:232596711665371.
Hoch MC, Mckeon PO. Peroneal reaction time after ankle sprain: a systematic review and meta-analysis. Med Sci Sports Exerc. 2014;46:546–56.
Doherty C, Bleakley C, Hertel J, Caulfield B, Ryan J, Delahunt E. Single-leg drop landing movement strategies 6 months following first-time acute lateral ankle sprain injury: ankle sprain and landing performance. Scand J Med Sci Sports. 2015;25:806–17.
Eechaute C, De Ridder R, Maes T, Beckwée D, Swinnen E, Buyl R, et al. Evidence of a different landing strategy in subjects with chronic ankle instability. Gait Posture. 2017;52:62–7.
Malliaropoulos N, Bikos G, Meke M, Vasileios K, Valle X, Lohrer H, et al. Higher frequency of hamstring injuries in elite track and field athletes who had a previous injury to the ankle - a 17 years observational cohort study. J Foot Ankle Res. 2018;11:7.
Moisan G, Descarreaux M, Cantin V. Effects of chronic ankle instability on kinetics, kinematics and muscle activity during walking and running: a systematic review. Gait Posture. 2017;52:381–99.
Riley PO, Paolini G, Della Croce U, Paylo KW, Kerrigan DC. A kinematic and kinetic comparison of overground and treadmill walking in healthy subjects. Gait Posture. 2007;26:17–24.
Wenning M, Lange T, Paul J, Gollhofer A, Gehring D. Assessing mechanical ankle instability via functional 3D stress-MRI – a pilot study. Clin Biomech. 2019;S0268003318310362.
Acknowledgements
The first author was supported by the Berta-Ottenstein-Programme for Clinician Scientists, Medical Faculty of the Albert-Ludwigs University of Freiburg, Germany.
Funding
The study was carried out at and funded by the submitting institution Praxisklinik Rennbahn AG. The article processing charge was funded by the Baden-Wuerttemberg Ministry of Science, Research and Art and the University of Freiburg in the funding program Open Access Publishing.
Author information
Authors and Affiliations
Contributions
All authors substantially contributed to this manuscript, its conception (MW, JP), design (MW, RR, HS), the acquisition (MM), analysis (MW, DG, RR) and interpretation of data (all authors), draft, and revision of the manuscript (all authors). All author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the local ethics committee (EKNZ 2019-00241).
Consent for publication
All authors agreed to the final version and publication of this manuscript.
Competing interests
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wenning, M., Gehring, D., Mauch, M. et al. Functional deficits in chronic mechanical ankle instability. J Orthop Surg Res 15, 304 (2020). https://doi.org/10.1186/s13018-020-01847-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-020-01847-8