
Abstract
Background
Recent studies suggest that low-molecular-weight heparin (LMWH) may play a role in mitigating the severity of acute pancreatitis (AP). This systematic review and meta-analysis aims to synthesise existing evidence on the effectiveness and safety of LMWH in the treatment of moderately-severe and severe AP.
Methods
This systematic review and meta-analysis was conducted in accordance with the 2020 update of the PRISMA guidelines and the Cochrane Handbook for Systematic Reviews of Interventions. The systematic search was conducted in MEDLINE, the Cochrane Central Register of Controlled Trials, Scopus, and EMBASE, covering studies published up to February 2024. Randomised controlled trials (RCTs) and observational studies (n-RCTs) that reported the differences in the outcomes of AP for patients receiving LMWH in addition to the standard treatment (Intervention), compared to patients managed by standard treatment without LMWH (Control) were eligible. A random-effects model was used to calculate the pooled relative risk (RR) and mean differences (MD) with the corresponding 95% CI.
Results
Thirteen studies were included in the meta-analysis, all published between 2004 and 2022. Eight studies were RCTs, and five were n-RCTs. Data from 13,709 patients (6.971 Interventions and 6.738 Controls) were analysed. The comparison of Intervention and Control groups showed the superiority of LMWH to standard treatments in terms of overall mortality (RR = 0.44, 95% CI = 0.31; 0.64, P < 0.0001, I2 = 51%), acute necrotic collections (RR = 0.24, 95% CI = 0.09; 0.62, P = 0.003, I2 = 0%), and organ failure (RR = 0.67, 95% CI = 0.48; 0.93, P = 0.02, I2 = 78%). The Intervention group showed superior outcomes compared with the Control group for gastrointestinal bleeding (RR = 0.64, 95% CI = 0.44; 0.94, P = 0.02, I2 = 0%), length of hospital stay (MD= − 6.08, 95% CI = − 10.08; − 2.07, P = 0.003, I2 = 98%), need for operative interventions (RR = 0.50, 95% CI = 0.29; 0.87, P = 0.01, I2 = 61%), and vascular thrombosis (RR = 0.43, 95% CI = 0.31; 0.61, P < 0.00001, I2 = 0%).
Conclusions
Moderate to high-quality evidence suggests that early intervention with LMWH could improve the prognosis of non-mild AP in terms of mortality, organ failure, and decreased incidence of vascular thrombosis. In light of our findings, integrating LMWH into the treatment regimen for moderate-severe to severe AP is advocated.
Similar content being viewed by others

Background
Acute pancreatitis (AP) is a leading gastrointestinal cause of hospital admission, with an incidence ranging from 13 to 45 cases per 100.000 inhabitants/year [1]. The aetiology of AP is multifactorial, with gallstones and alcohol use being the most common causes [2]. AP encompasses a large spectrum of pancreatic inflammation that presents with varying degrees of severity, ranging from mild, self-limiting episodes to severe, life-threatening illness [3, 4]. Mortality in the early phase of AP is mainly attributed to multiorgan failure, whereas in the late phase, it is often caused by septic complications. In managing AP, supportive care with interventions such as fluid resuscitation, pain relief, and early nutritional support represents the cornerstone [5]. However, the role of pharmacological interventions in modifying the course of the disease and preventing complications remains an area of ongoing research.
Disturbances in pancreatic microcirculation resulting from the inflammatory cascade have been recognised as the primary factor in the development of AP, causing hypoxia and subsequent necrosis of the organ and affecting the course of the disease. This is probably related to the dysfunction of the balance between pro-inflammatory and anti-inflammatory responses. After premature pancreatic protease activation and extravasation of these activated digestive enzymes into the pancreas and peripancreatic tissues, cytokines and other inflammatory mediators are produced and released with excessive leukocyte activation. Pro-inflammatory cytokines, such as tumour necrosis factor (TNF)-α, interleukin (IL)-1β, IL-6, and IL-8, increase the capillary permeability with fluid loss, aggravating pancreatic injury. TNF-α damages the acinar cells and is probably responsible for pancreatic necrosis and damage to other organs, such as the lungs, liver, intestine, and spleen. Endothelin-1 (ET-1), nitric oxide, and other radicals damage the vascular endothelium, leading to microcirculatory disturbance and organ dysfunction. On the other hand, anti-inflammatory cytokines, such as IL-10, cause immunosuppression, and their excess levels may increase the rate of infectious complications in the later stages of severe disease [6, 7].
The role of coagulopathy in AP progression is evident. Extravasation of activated digestive enzymes from injured pancreatic acinar cells causes local vascular epithelial cell injury, tissue factor exposure, platelet activation, and coagulation cascade activation. The coagulation pathway is additionally activated by its close interplay with pro-inflammatory cytokines, which leads to micro and macro-thromboses. Pancreatic tissue oedema, increased pancreatic shunt, and systemic volume depletion further compromise the microcirculation, leading to reduced pancreatic perfusion, tissue necrosis, multiorgan failure, and death.
Recent studies suggest that low-molecular-weight heparin (LMWH) may play a role in mitigating the severity of AP, potentially by improving microcirculatory disturbances and reducing the incidence of necrosis and other complications, including vascular thrombosis [8]. Moreover, LMWH can decrease TNF-α production and block the initiation of inflammatory storms [9]. However, because patients with severe AP are perceived to be at increased risk of haemorrhage due to the nature of pancreatic/peripancreatic necrosis, anticoagulation has traditionally been very cautiously implemented and not recommended in current clinical guidelines [5, 10,11,12]. To date, sparse randomised controlled trials (RCTs) revealed decreased major complication rates after adding LMWH therapy to the standard of care for the management of moderately-severe and severe AP. Moreover, four meta-analyses that evaluated the effectiveness and safety of anticoagulants in severe AP confirmed that it can significantly improve disease prognosis. However, these meta-analyses were limited by relevant methodological issues [9, 13,14,15].
This systematic review and meta-analysis aims to synthesise existing evidence on the effectiveness and safety of adding LMWH in the treatment of moderately-severe and severe AP, providing clarity on its therapeutic value on disease progression, prevention of mortality, pancreatic necrosis, local and systemic complications and need for interventions, and guiding future clinical practice and research.
Materials and methods
This study was conducted and presented in accordance with the recommendations of the 2020 update of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [16], the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines [17], the Cochrane Handbook for Systematic Reviews of Interventions guidelines [18], and the AMSTAR II (A Measurement Tool to Assess systematic Reviews) criteria [19]. Two reviewers (M.P. and V.M.) independently conducted all stages of study identification, selection, quality assessment, and data extraction.
The review question, inclusion criteria, search strategy, outcomes, methods of the analysis, plan to investigate sources of heterogeneity and risk of bias assessment were established in advance and documented in the study protocol (PROSPERO CRD42024509850).
Definition of the PICO question
Patient/Problem, Intervention, Comparison, Outcome and Study design (PICOS) structure was implemented for the systematic review and meta-analysis.
Patient/problem
Studies involving patients diagnosed with moderately-severe and severe AP were included. AP diagnosis was based on clinical criteria, including abdominal pain, serum amylase, and/or lipase levels greater than three times the normal upper limit, and/or imaging findings consistent with AP [20]. Studies focusing on pregnant women or specific subgroups with conditions that significantly alter the natural course of AP (e.g., immunocompromised patients) were excluded. Studies examining chronic pancreatitis, as well as hypertriglyceridemia-induced AP in more than 30% of the population study, were excluded. Studies that did not specifically evaluate the role of LMWH or where LMWH was not a primary intervention being studied were excluded.
Intervention/exposure
Included studies must explicitly report using LMWH as a treatment modality in patients with AP. The dosage, frequency, and duration of LMWH treatment were specified or inferable. Both prophylactic and therapeutic uses of LMWH in the context of AP were considered. Studies evaluating LMWH in combination with other standard treatments for AP were included, provided the effect of LMWH could be isolated or analysed separately. Studies where LMWH was used for indications other than AP (such as solely for thromboprophylaxis in hospitalised patients) without consideration of its role in AP, were excluded. Similarly, studies where LMWH were used to treat splanchnic vein thrombosis (SVT) in the context of AP were excluded. Studies that did not differentiate the outcomes of LMWH treatment from other interventions used concurrently, making it impossible to attribute effects specifically to LMWH, were excluded.
Comparator/control
Comparison studies must include a control group receiving standard treatment for AP without the addition of LMWH. Standard treatment strategies for AP may include resuscitation, intravenous fluids, pain management, nutritional support, and monitoring for complications. The standard treatment regimen should clearly describe or refer to established clinical guidelines to compare care practices across different studies. Studies without a clearly defined control group receiving standard care for AP and studies where the control group received an intervention that significantly deviates from established clinical guidelines for AP without justification were excluded.
Types of studies included
Eligible studies were RCTs, non-randomised controlled trials (prospective and retrospective cohort studies, and case-control studies) (n-RCTs) of patients with moderately-severe and severe AP in which the intervention group receiving LMWH treatment in adjunct to conventional treatment was compared with controls receiving conventional treatment. Animal studies, case reports, case series, editorials, opinion pieces, narrative and systematic reviews, and meta-analyses were excluded.
Study identification
MEDLINE (via PubMed), the Cochrane Central Register of Controlled Trials, Scopus, and EMBASE were systematically searched for any relevant clinical study. The search covered studies published from the inception of each database up to February 2024. The search strategy combined text words and MeSH terms related to prophylactic LMWH (Intervention) versus standard treatment (Control) for moderately severe and severe AP: [pancreatitis, acute pancreatitis, antithrombotic, antithrombotics, prevention, control, prophylaxis, prophylaxies, heparin, thromboprophylaxis]. The complete search strategy is available in Supplementary Table 1 and is freely accessible in the protocol. Reference lists of included studies and relevant reviews were manually searched. The ‘’related articles’’ function in PubMed was used to identify any additional studies not captured by the electronic database searches. Grey literature searches were conducted in ClinicalTrials.gov, Google Scholar, and Open Grey.
Study screening and selection
All stages of study identification, selection, quality assessment, and data extraction were carried out independently by two reviewers (M.P. and V.M.). Inconsistencies were resolved by discussion between the two reviewers until a consensus was reached or based on an independent assessment by a third reviewer (P.M.).
The reviewers identified studies by reviewing the titles and abstracts, followed by a full-text review using the Rayyan web app for systematic reviews (https://www.rayyan.ai/). Only studies that reported at least one of the primary or secondary outcomes were included. Where there was an overlap in patient cohorts of two or more studies, and no difference in study interval was reported, the most recent report was included in the pooled analysis. A PRISMA 2020 flow diagram was used to document the screening and selection process, detailing the number of records identified, screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage.
Risk of bias assessment
Two authors (M.P. and V.M.) independently assessed the risk of bias using the Cochrane Risk of Bias 2.0 (RoB 2) tool [21] and assessed the risk of bias in observational studies using the Risk of Bias in Non-Randomised Studies of Intervention (ROBINS-I) tool [22]. The RoB 2 tool evaluated bias across five domains: bias arising from the randomisation process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in the measurement of the outcome, and bias in the selection of the reported result. The ROBINS-I tool assessed bias across seven domains: bias due to confounding, bias in the selection of participants, bias in the classification of interventions, bias due to deviations from intended interventions, bias due to missing data, bias in the measurement of outcomes, and bias in the selection of the reported result. Each domain within the tools was judged as “low risk”, “some concerns”, or “high risk” of bias, according to the guidelines provided by the respective assessment tool.
Quality of evidence assessment
Using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach, two authors (M.P. and V.M.) independently evaluated the quality of evidence for imprecision, inconsistency, indirectness, and publication bias and classified the quality of evidence as very low, low, moderate, or high [23]. A summary table of their findings using GRADEpro version 3.6.1 software (https://www.gradepro.org/) was created.
Study outcomes
Primary outcomes
The primary outcomes for this systematic review and meta-analysis were selected to evaluate the effectiveness and safety of LMWH and determine the clinical relevance of LMWH as a therapeutic intervention in the treatment of AP. The following pre-specified primary outcomes were reviewed:
-
Mortality rate This was measured as the number of deaths directly attributed to AP among the study population, reported during the in-hospital stay.
-
The severity of acute pancreatitis evolution The severity was assessed through clinical outcomes, including shock, pancreatic necrosis, and organ failure. Measurements taken during hospitalisation were included.
Secondary outcomes
Secondary outcome measures were evaluated to assess other potential benefits and drawbacks of prophylactic LMWH administration:
-
Physiological assessment and recovery of functions Cured illness, APACHE II score, need for ICU admission, ICU duration, time to symptomatic relief and intestinal recovery time, assessed during the acute phase of the illness and at discharge.
-
Complications Systemic inflammatory response syndrome (SIRS), local complications (e.g., necrosis, pseudocyst, abscess).
-
Length of hospital stay The total number of days from admission to hospital discharge.
-
Evolution parameters Need for operative treatments, CTSI score, necrosis score, and Balthazar score at follow-up during hospital stay throughout the course of LMWH.
-
Adverse events Any adverse events, including bleeding complications, vascular thrombosis, and heparin-induced thrombocytopenia. Adverse events were assessed throughout the course of LMWH treatment and at the follow-up period.
Data extraction
A double-blinded procedure was undertaken to increase the accuracy of the data extracted, and a predefined spreadsheet (Excel®, 2022; Microsoft, Redmond, Washington, USA) was used for data extraction. Data were independently extracted by two reviewers (M.P. and V.M.), and any discrepancies were resolved through consultation with a third reviewer (P.M.). For each study, the following informations were recorded:
-
Study characteristics Author(s), year of publication, country, study design, sample size, and setting.
-
Participant details Age, sex, severity of AP, baseline characteristics.
-
Interventions Type, dose, duration, and frequency of LMWH used; details of standard care in the comparator group.
-
Outcomes Data on primary and secondary outcomes, as specified, including measurement methods and timing of assessments.
-
Risk of bias Information relevant to assessing the risk of bias in each study.
Statistical analysis
Extracted data were tabulated and summarised, and meta-analyses were conducted for outcomes where data from two or more studies could be combined. All statistical analyses were performed using ReviewManager version 5.4.1 software and the RevMan Web (https://revman.cochrane.org/info). When continuous data were reported as the median and range, Hozo’s method was implemented to estimate the respective mean and standard deviation [24]. Besides the results for statistical heterogeneity, clinical and methodological heterogeneities were reviewed. Given the intrinsic heterogeneity of interventions, populations, study designs, methods, and statistical heterogeneity, the random-effects model was exclusively applied for the meta-analysis. Statistical heterogeneity of the results across studies was assessed using the Higgins’ I2 and chi-square tests. A P value of the Chi-square test less than 0.10 with an I2 value greater than 50% indicated substantial heterogeneity.
The measure of effect for dichotomous outcomes was the relative risk (RR) with 95% confidence intervals (CIs). The mean difference (MD) or standardised mean difference (SMD), where indicated, with 95% CIs, was used for continuous outcomes. A P value < 0.05 was considered statistically significant.
Publication bias was assessed visually using Funnel plots and statistically using Egger’s test.
Sensitivity analyses and analyses of subgroups
Sources of heterogeneity were explored through subgroup analyses for LMWH different doses (prophylactic vs. therapeutic), LMWH duration (< 8 days vs. 8–14 days) and AP severity (moderately-severe vs. severe). To assess the robustness of the findings, sensitivity analyses of clinically relevant outcomes using the leave-one-out method depending on the weight of each study included in the pooled analysis and based on the qualitative evaluation of the included studies were performed.
Results
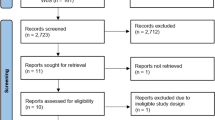
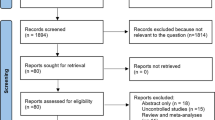
Based on the search strategy and inclusion criteria, a total of 1.162 references were identified through database searching. After excluding 477 duplicates, 685 records were identified. Grey literature review did not add any further records. Another 458 articles were further excluded due to violation of eligibility criteria. The selection process led to 227 articles eligible for full-text reading. Following exclusions (n = 216), reported in Fig. 1, and the adjunct of two studies identified by citation searching, 13 studies were considered eligible for quantitative synthesis, all published between 2004 and 2022 [25,26,27,28,29,30,31,32,33,34,35,36,37]. The inter-rater reliability for reviewers had a k value exceeding 0.90.

Flow chart of the study selection process according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA 2020)
Study characteristics
Eight studies were RCTs [25, 26, 30,31,32,33,34,35], and five were prospective or retrospective n-RCTs [27,28,29, 36, 37]. All studies together analysed data from 13,709 patients (6971 who received LMWH in the Intervention group and 6738 who received standard treatment in the Control group). Limiting the analysis to RCTs, 670 patients were allocated to the Intervention group and 670 to the Control group. The study characteristics are summarised in Table 1, while the baseline characteristics of the patients included in the systematic review and meta-analysis are reported in Supplementary Table 2. Two studies were conducted in India [25, 26], two in the United States [27, 28], six studies in China [29,30,31,32,33,34], one in Turkey [35], whereas for two studies, presented as conference abstracts, no country of origin was identified [36, 37]. Two studies [32, 33] were conducted on the same population of patients. However, the reviewers included both in the pooled analysis as different outcomes were analysed. All records analysed the outcomes of prophylactic LMWH compared with standard treatment without LMWH in patients with moderately-severe and severe AP from biliary origin, alcohol, idiopathic or other causes. One study [30] included 560 children who satisfied the diagnostic and classificatory criteria for AP. Sensitivity analyses were performed to assess the impact of this study on the final results.
Five studies focused on patients with severe AP [26, 30, 31, 33, 37], whereas three studies included patients with both moderately-severe and severe AP [25, 35, 36]. Zhou et al. [29] included patients with pancreatic necrosis without further indications of the stage of AP. For three studies, the AP stage was not specified [27, 28, 34]. Considerable heterogeneity among included studies concerning diagnostic criteria for moderately-severe and severe AP was found. Marked heterogeneity was also demonstrated in the dose and length of LMWH administration and outcomes evaluated. Overall, similar exclusion criteria were found, except for Han et al. [30], whose analysis was limited to children. The presence of chronic pancreatitis represented exclusion criteria in the study by Patil et al. [25] and Tozlu et al. [35]. Hypersensitivity to LMWH, pregnancy, lactating and coagulation disorders and end-stage chronic disease with Charlson’s Comorbidity Index ≥ five were listed as exclusion criteria in all the included studies. Type, dosage and length of LMWH treatment varied within the included studies, ranging from standard prophylactic regimens (1 mg/kg body weight LMWH subcutaneously, 12 hourly for seven days) to routine continuous, systematic anticoagulation with a therapeutic dose of LMWH (2 mg/Kg per day, or 40 mg/per day) (Table 1).
Risk of bias
Figures 2 and 3 present the risk of bias analysis. Regarding the RCTs, outcomes might have been influenced by bias arising from the randomisation process, as methods of patient allocation showed substantial variability and some concerns in the majority of included trials, deviations from intended interventions [31, 32, 34], missing outcome data [32, 34], measurement of the outcome [26, 34, 35], and selection of the reported results [26, 32]. Overall, only one RCT was considered at low risk of bias [25]. In contrast, three studies [30, 32, 35] and four studies [26, 31, 32, 34] were considered to have some concerns and at high risk of bias, respectively. Among the five n-RCTs, two were considered at moderate risk of bias [27, 29] and one at serious risk of bias [28]. For two studies [36, 37], no information was available to determine the risk of bias. Graphically, potential publication bias was not present for mortality, occurrence of organ failure, and need for any operative intervention during treatment. Funnel plots are available in Supplementary Fig. 1.

ROB2 Risk of Bias assessment of randomised controlled trials included in the systematic review and meta-analysis

ROBINS-I Risk of Bias assessment of non-randomised controlled trials included in the systematic review and meta-analysis
Baseline patient characteristics
Patients in the Intervention and Control groups did not significantly differ in terms of baseline characteristics regarding sex, age, aPTT, Balthazar score, Charlson’s comorbidity index, Computed Tomography Severity Index (CTSI), platelet count, serum amylase, and serum bilirubin. Conversely, albumin (SMD = 0.47, 95% CI = 0.21; 0.73, P = 0.0004, I2 = 0%) and APACHE II score (MD = 0.08, 95% CI = 0.05; 0.12, P < 0.00001, I2 = 0%) were higher in the Intervention group. PT time (MD= − 0.09, 95% CI = − 0.15; − 0.03, P = 0.002, I2 = 0%) was longer in the Control group (Supplementary Fig. 2, Supplementary Table 3, Supplementary Table 4).
Analysis of the primary outcomes
The comparison of Intervention and Control groups showed the superiority of LMWH to standard treatments in terms of overall mortality (11 studies, 13.320 patients; RR = 0.44, 95% CI = 0.31; 0.64, P < 0.0001, I2 = 51%, Test for subgroup differences P < 0.0001, I2 = 93.5%), mortality in severe AP (3 studies, 456 patients; RR = 0.33, 95% CI = 0.20; 0.54, P < 0.00001, I2 = 0%, Test for subgroup differences P = 0.94, I2 = 0%), acute necrotic collections (2 studies; 240 patients; RR = 0.24, 95% CI = 0.09; 0.62, P = 0.003, I2 = 0%), CTSI (5 studies, 1165 patients; MD = − 1.38, 95% CI= − 2.26; − 0.50, P = 0.002, I2 = 93%), organ failure (8 studies, 13,124 patients; RR = 0.67, 95% CI = 0.48; 0.93, P = 0.02, I2 = 78%, Test for subgroup differences P = 0.94, I2 = 0%), walled-off pancreatic necrosis (2 studies, 240 patients; RR = 0.24, 95% CI = 0.11; 0.53, P = 0.0004, I2 = 0%), number of patients with progress in CTSI (2 studies, 240 patients; RR = 0.24, 95% CI = 0.12; 0.47, P < 0.0001, I2 = 0%), and shock (3 studies, 12,090 patients; MD = 0.84, 95% CI = 0.72; 0.98, P = 0.02, I2 = 0%, Test for subgroup differences P = 0.42, I2 = 0%) (Fig. 4, Supplementary Table 5).

Meta-analysis of primary outcomes: A Mortality; B Acute necrotic collections; C CTSI; D Organ failure; E Walled-off pancreatic necrosis; F Shock
Subgroup analyses, performed according to study design, showed RCTs yielding a pooled effect favouring the Intervention group for mortality (7 studies, 1.340 patients; RR = 0.34, 95% CI = 0.25; 0.46, P < 0.00001, I2 = 0%), whereas organ failure was not statistically different (6 studies, 1.299 patients; RR = 0.60, 95% CI = 0.35; 1.02, P = 0.06, I2 = 76%).
Analysis of the secondary outcomes
In the analysis of secondary outcomes, the Intervention group showed superior outcomes compared with the Control group for APACHE II score (4 studies, 980 patients MD = − 1.81, 95% CI = − 2.63; − 0.98, P < 0.001, I2 = 90%, Test for subgroup differences P = 0.03, I2 = 79.9%), need for ICU admission (2 studies, 11,962 patients; RR = 0.77, 95% CI = 0.67; 0.89, P = 0.0003, I2 = 0%, Test for subgroup differences P = 0.89, I2 = 0%), mean time of tolerance to diet (3 studies, 374 patients; MD = − 2.55, 95% CI = − 4.99; − 0.12, P = 0.04, I2 = 98%), and systemic complications during treatment (3 studies, 933 patients; RR = 0.42, 95% CI = 0.32; 0.55, P < 0.00001, I2 = 0%, Test for subgroup differences P = 0.70, I2 = 0%). Conversely, regarding the rate of cured illness (3 studies, 925 patients; RR = 1.20, 95% CI = 0.87; 1.66, P = 0.26, I2 = 97%) and local complications (5 studies, 12,165 patients; RR = 0.62, 95% CI = 0.25; 1.55, P = 0.31, I2 = 84%, Test for subgroup differences P = 0.64, I2 = 0%), the two study groups showed no statistically significant difference (Supplementary Fig. 3, Supplementary Table 6).
The Intervention group showed superior outcomes compared with the Control group for gastrointestinal bleeding (4 studies, 1487 patients; RR = 0.64, 95% CI = 0.44; 0.94, P = 0.02, I2 = 0%, Test for subgroup differences P = 0.46, I2 = 0%), length of hospital stay (7 studies, 13,024 patients; MD = − 6.08, 95% CI = − 10.08; − 2.07, P = 0.003, I2 = 98%, Test for subgroup differences P = 0.48, I2 = 0%), need for operative interventions (any type) (7 studies, 1354 patients; RR = 0.50, 95% CI = 0.29; 0.87, P = 0.01, I2 = 61%, Test for subgroup differences P = 0.40, I2 = 0%), need for surgical intervention (3 studies, 959 patients; RR = 0.39, 95% CI = 0.24; 0.65, P = 0.0003, I2 = 0%), and vascular thrombosis (5 studies, 1167 patients; RR = 0.43, 95% CI = 0.31; 0.61, P < 0.00001, I2 = 0%, Test for subgroup differences P = 0.10, I2 = 63.2%).
Conversely, regarding the need for endoscopic intervention (3 studies, 255 patients; RR = 0.72, 95% CI = 0.27; 1.93, P = 0.51, I2 = 57%, Test for subgroup differences P = 0.77, I2 = 0%), Balthazar score (2 studies, 240 patients; MD = 0.01, 95% CI= − 0.11; 0.12, P = 0.90, I2 = 0%) and necrosis score (2 studies, 240 patients; MD = 0.02, 95% CI= − 0.31; 0.36, P = 0.89, I2 = 0%) the two study groups showed no statistically significant difference (Supplementary Fig. 4, Supplementary Table 7).
Subgroup analyses, performed according to study design, showed that in RCTs the Intervention group was superior in terms of APACHE II score (2 studies, 825 patients; MD = − 1.10, 95% CI = − 1.39; − 0.81, P < 0.00001, I2 = 0%), systemic complications (2 studies, 660 patients; RR = 0.42, 95% CI = 0.32; 0.55, P < 0.00001, I2 = 5%), vascular thrombosis (3 studies, 505 patients; RR = 0.15, 95% CI = 0.04; 0.55, P = 0.004, I2 = 0%), and need for operative intervention (5 studies, 1199 patients; RR = 0.42, 95% CI = 0.25; 0.69, P = 0.0007, I2 = 30%). Conversely, equivalent results between the two study groups were found for local pancreatic complications (3 studies, 340 patients; RR = 0.51, 95% CI = 0.15; 1.68, P = 0.27, I2 = 89%) and gastrointestinal bleeding (2 studies, 825 patients; RR = 0.54, 95% CI = 0.25; 1.18, P = 0.12, I2 = 45%).
Analysis of the laboratory parameters after treatment
Regarding laboratory parameters after treatment, no statistically significant difference was found between the Intervention and Control groups, in terms of platelets and albumin. Conversely, PT time (3 studies, 664 patients; MD = 0.72, 95% CI = 0.17; 1.27, P = 0.01, I2 = 81%) was longer in the Intervention group (Supplementary Fig. 5, Supplementary Table 8).
Sensitivity and subgroup analyses
The results of the sensitivity analyses done using the leave-one-out method showed that mortality was not impacted by any of the included studies, similar to what happened in the analyses of organ failure and the need for any type of operative intervention during treatment. However, the benefits of LMWH were less evident, in particular for organ failure and the need for operative treatment, when the study by Han et al. [30] was excluded.
Considering the different stages of the disease (moderately-severe vs. severe AP), the results of the subgroup analysis showed superior outcomes for the Intervention group in terms of mortality (8 studies, 1454 patients; RR = 0.34, 95% CI = 0.25; 0.45, P < 0.00001, I2 = 0%, Test for subgroup differences P = 0.48, I2 = 0%). The subgroup analysis showed superior results for the Intervention group in moderately-severe (3 studies, 338 patients; RR = 0.20, 95% CI = 0.05; 0.87, P = 0.03, I2 = 0%) and severe AP (5 studies, 1116 patients; RR = 0.34, 95% CI = 0.25;0.47, P < 0.00001, I2 = 0%). Regarding the need for any intervention (7 studies, 1354 patients; RR = 0.50, 95% CI = 0.29; 0.87, P = 0.01, I2 = 61%, Test for subgroup differences P = 0.93, I2 = 0%), the Intervention group was again superior. However, the subgroup analysis showed equivalent results between the two study groups for moderately-severe (3 studies, 338 patients; RR = 0.48, 95% CI = 0.21; 1.14, P = 0.10, I2 = 44%) and severe AP (4 studies, 1.016 patients; RR = 0.51, 95% CI = 0.22; 1.18, P = 0.12, I2 = 75%). The incidence of organ failure in the two groups was equivalent (6 studies, 1229 patients; RR = 0.64, 95% CI = 0.34; 1.21, P = 0.17, I2 = 74%, Test for subgroup differences P = 0.81, I2 = 0%). The subgroup analysis based on the disease severity resulted in similar results in the two study groups for moderately-severe (2 studies, 240 patients; RR = 0.45, 95% CI = 0.03; 6.93, P = 0.57, I2 = 67%) and severe AP (4 studies, 1059 patients; RR = 0.64, 95% CI = 0.32; 1.28, P = 0.21, I2 = 82%) (Supplementary Fig. 6).
In the subgroup analysis on the duration of LMWH (< 8 days vs. 8–14 days), the Intervention group showed superior results than the Control group in terms of mortality (9 studies, 1495 patients; RR = 0.34, 95% CI = 0.25; 0.45, P < 0.00001, I2 = 0%, Test for subgroup differences P = 0.88, I2 = 0%). The subgroup analysis resulted in superior outcomes of the Intervention group for LMWH < 8 days (5 studies, 646 patients; RR = 0.32, 95% CI = 0.19; 0.55, P < 0.0001, I2 = 0%) and 8–14 days (4 studies, 849 patients; RR = 0.34, 95% CI = 0.24; 0.49, P < 0.00001, I2 = 0%).
For organ failure, the Intervention group was favoured only in case of duration of the LMWH administration for 8–14 days (6 studies, 1299 patients; RR = 0.64, 95% CI = 0.34; 1.21, P = 0.17, I2 = 74%, Test for subgroup differences P = 0.18, I2 = 44.7%). The subgroup analysis based on the duration of LMWH resulted in similar results between the two study groups for the length of LMWH < 8 days (4 studies, 605 patients; RR = 0.83, 95% CI = 0.34; 2.05, P = 0.69, I2 = 85%) but superior results in the Intervention group when LMWH was administered for 8–14 days (2 studies, 694 patients; RR = 0.42, 95% CI = 0.28; 0.64, P < 0.0001, I2 = 0%).
In terms of need for any intervention (7 studies, 1354 patients; RR = 0.50, 95% CI = 0.29; 0.87, P = 0.01, I2 = 61%, Test for subgroup differences P = 0.93, I2 = 0%), the subgroup analysis based on the duration of LMWH showed similar results in the two study groups for LMWH < 8 days (3 studies, 505 patients; RR = 0.49, 95% CI = 0.21; 1.11, P = 0.09, I2 = 44%) and 8–14 days (4 studies, 849 patients; RR = 0.51, 95% CI = 0.22; 1.20, P = 0.12, I2 = 75%) (Supplementary Fig. 7).
When exploring potential differences based on the dose of LMWH (prophylactic vs. therapeutic), the subgroup analysis found no statistically significant differences between the two groups in terms of mortality (9 studies, 1208 patients; RR = 0.41, 95% CI = 0.29; 0.58, P < 0.00001, I2 = 0%, Test for subgroup differences P = 0.16, I2 = 48.6%) both favouring the Intervention group. The subgroup analysis showed similar results for prophylactic dose (4 studies, 554 patients; RR = 0.33, 95% CI = 0.20; 0.53, P < 0.00001, I2 = 0%) and therapeutic dose (5 studies, 654 patients; RR = 0.53, 95% CI = 0.32; 0.88, P = 0.01, I2 = 0%) in favour of LMWH. Regarding the need for any intervention, Intervention and Control groups showed equivalent results (6 studies, 794 patients; RR = 0.57, 95% CI = 0.32; 1.02, P = 0.06, I2 = 50%, Test for subgroup differences P = 0.76, I2 = 0%). The subgroup analysis showed similar results for prophylactic dose (4 studies, 554 patients; RR = 0.57, 95% CI = 0.27; 1.24, P = 0.16, I2 = 60%) and therapeutic dose (2 studies, 240 patients; RR = 0.43, 95% CI = 0.09; 2.21, P = 0.31, I2 = 59%).
Conversely, in terms of organ failure, the Intervention group showed superior results compared with the Control group when LMWH was administered at prophylactic dose (6 studies, 1012 patients; RR = 0.73, 95% CI = 0.43; 1.23, P = 0.24, I2 = 65%, Test for subgroup differences P = 0.19, I2 = 42.3%). The subgroup analysis based on the dose of LMWH showed superior results for prophylactic dose in the Intervention group (2 studies, 399 patients; RR = 0.51, 95% CI = 0.32; 0.81, P = 0.004, I2 = 0%) and equivalent results between the two study groups for therapeutic dose (4 studies, 613 patients; RR = 0.92, 95% CI = 0.43; 1.97, P = 0.84, I2 = 70%) (Supplementary Fig. 8).
GRADE quality of evidence assessment
According to the GRADE criteria, the systematic review and meta-analysis of RCTs and n-RCTs comparing Intervention with LMWH and Control with conventional treatment revealed that the overall quality of evidence was low for APACHE II score after treatment, occurrence of local complications during treatment, gastrointestinal bleeding, CTSI at follow-up, and length of hospital stay. The certainty of the evidence was moderate for the occurrence of organ failure and the need for operative intervention during treatment, whereas it was high for mortality and vascular thrombosis during treatment. The systematic review and meta-analysis of RCTs showed that the certainty of the evidence was very low for the occurrence of organ failure, local complications and gastrointestinal bleeding during treatment. Similarly, it was very low for CTSI at follow-up and length of hospital stay. The GRADE assessment revealed that the certainty of evidence was moderate for the occurrence of vascular thrombosis during treatment, whereas it was high for mortality and need for operative intervention (Figs. 5 and 6).

GRADE Assessment (RCTs and n-RCTs)

GRADE Assessment (RCTs)
Discussion
AP runs a severe course in a minority of patients for whom moderately-severe and severe forms of the disease develop. Pancreatic necrosis and multiple organ failure [38] are the most common causes of death in patients with AP [39, 40], and this small subset of courses is responsible for the burden of the disease [41].
The treatment of AP is currently based on symptomatic and supportive treatments, including pain management, fluid and electrolyte replacement, early nutritional support and, in the case of infected necrosis, antibiotic treatment and endoscopic or surgical step-up approaches for drainage [5, 10,11,12, 42].
The progression of AP, especially in the first 72 h, is accompanied by systemic inflammatory cascade activation, pancreatic microcirculatory disturbance and microthrombi formation. The present systematic review and meta-analysis summarised the current evidence on the efficacy and safety of anticoagulant prophylaxis with LMWH in moderately-severe and severe AP and revealed that the use of prophylactic LMWH can reduce mortality by approximately 56 − 66%, with a consistent effect in favour of the LMWH treatment arm in all the subgroup and sensitivity analyses. Although being often prescribed in clinical practice in the light of recent studies that have shown, besides its anti-thrombotic, the anti-inflammatory and anti-protease properties of LMWH, currently there is no consensus regarding its use in AP [5, 10, 12, 42,43,44]. Our results on the reduction in the incidence of mortality, which were deemed of critical importance according to the GRADE assessment system, had high degree of evidence and allowed us to conclude that, in the current state of scientific knowledge, the prophylactic administration of LMWH should be recommended in patients with non-mild acute AP, unless contraindicated for hypersensitivity reasons or coagulopathy.
In keeping with our findings, the results of the meta-analysis by He et al. [9] showed that the early adoption of LMWH therapy revealed its efficacy in improving prognosis by decreasing the mortality, incidence of multiorgan failure, and vascular thrombosis in patients with non-mild AP. Similarly, experimental and clinical investigations have shown that LMWH medication may reduce the damage to the pancreas, lungs, kidneys, and brain in severe AP, as well as prevent AP-mediated organ damage, by lowering serum ET-I levels and decreasing the activation of NF-kB to lower TNF-α and IL-6 levels [7, 9, 45].
The anti-inflammatory properties of LMWH are different from its anticoagulant activity. LMWH reduces the recruitment of inflammatory cells into the site of injury and leucocyte adhesion to vascular endothelial cells [46,47,48,49,50,51,52]. The meta-analysis by Qiu et al. [52] showed that WBC and C-reactive protein (CRP) levels were lower in patients treated with LMWH than with conventional treatments. As it appeared from the study by Tozlu et al. [35], early administration of LMWH improved the radiological picture with regression in most cases. Furthermore, most clinical parameters were better in the LMWH treatment group, with a lower rate of admission to the ICU, shorter time to oral feeding, hospital stay, and occurrence of necrosis compared with standard treatments. In keeping with these findings, the use of LMWH was shown to be correlated in our meta-analysis with a reduction in the incidence of organ failure, both in the entire group of studies analysed and in the RCTs, albeit with a low level of evidence.
In a recent systematic review and meta-analysis by Patoni et al. [13], both RCTs and observational studies reported results in favour of LMWH administration in terms of significantly decreased risk of mortality and multiple organ failure for patients treated with prophylactic anticoagulants compared to standard treatments. Moreover, the need for endoscopic or surgical interventions was significantly reduced by LMWH, concluding that LMWH reduces major complication rates in non-mild AP cases when initiated early after diagnosis.
Previous data have shown that anticoagulation therapy may cause massive upper gastrointestinal bleeding in AP [53], which is one of the reasons why LMWH has not been recommended as a conventional therapy in treating severe AP patients by currently established guidelines. However, the safety of LMWH use in severe and necrotising AP patients was repeatedly demonstrated in recent years. The meta-analysis by Yin et al. [54] pointed out that anticoagulation marginally increased the risk of bleeding in patients with AP, which was inconsistent with the findings of two previous meta-analyses [55, 56] and ours. Intuitively, there could be higher rates of haemorrhage in AP patients treated with therapeutic anticoagulation, in line with previous studies showing that therapeutic dosage of LMWH increases the risk of gastrointestinal bleeding in these patients. Although patients with underlying AP appear to have an additional risk of haemorrhage due to local complications that, in case of infected pancreatic necrosis or persistent symptoms, require endoscopic or percutaneous drainage [57], our findings revealed that LMWH does not increase the incidence of gastrointestinal bleeding, suggesting a favourable safety profile. In keeping with our findings, Qiu et al. [52] and Patoni et al. [13] showed that in their meta-analyses about LMWH usage in AP patients, none of the enrolled studies reported that LMWH would increase the risk of bleeding or prolong prothrombin time and activated partial thromboplastin time.
This evidence, although of low grade, allows us to consider the safety profile of the administration of LMWH as adequate. Nevertheless, this outcome is rarely reported in AP patients receiving prophylactic anticoagulants, so, further high-quality studies are needed to confirm this finding.
Our meta-analysis also revealed LMWH’s association with reduced organ failure and thrombotic events, reinforcing its beneficial impact beyond mere anticoagulation. In our study, the experimental group with LMWH showed a reduction in thrombotic events compared to the standard therapy group, with a high level of evidence and a lower use of operative treatments of interventional radiology, operative endoscopy and surgery during the treatment period. This result was judged to be of high quality in the analysis of RCTs, and moderate in all studies analysed. Splanchnic venous thrombosis (SVT), which includes the splenic, portal, and/or superior mesenteric veins, is reported to occur in imaging studies in patients with AP with an approximate incidence rate of 1-24% [58, 59]. In the study by Zhou et al. [29] early application of anticoagulation was found to reduce the incidence of SVT, while the incidence of bleeding was comparable between the two study groups.
Among the subgroup analyses that were carried out, the one based on the type of LMWH dose used showed how, both in prophylactic and therapeutic doses, the use of LMWH was able to reduce the incidence of mortality, while with regards to organ failure, the administration of prophylactic doses has proven to be more effective than the administration of a therapeutical dose. This result is of absolute importance since the fear of the onset of bleeding complications following the administration of therapeutic doses of LMWH could generate a reluctance towards the application of scientific evidence in this regard. The evidence that the reduction in the incidence of mortality in patients suffering from moderate-severe and severe AP already occurs with the use of prophylactic dosages of LMWH could represent a push towards the routine use of this clinical practice to a global level.
The analysis of the results performed in the subgroups of patients with moderate-severe and severe AP showed a reduction in mortality in both subgroups of patients following the administration of LMWH. This favourable effect was obtained with administration times of less than eight days and with longer administration times, from eight to 14 days. This result allows us to conclude that the administration of LMWH at a prophylactic dosage for a duration of less than eight days represents an appropriate regimen to reduce mortality in patients suffering from non-mild AP.
However, prolonged administration for a time interval between eight and 14 days appears to be related to a decrease in the incidence of organ failure, but large RCTs must confirm this data. Future studies should explore the optimal duration and dosage of LMWH treatment, particularly given the observed benefits of less than eight days of administration and the potential for extended administration to decrease organ failure incidence. These investigations will be crucial in refining treatment protocols and enhancing our understanding of LMWH’s therapeutic mechanisms, including its anti-inflammatory properties and influence on the coagulation cascade.
Using LMWH was also associated with reducing the length of hospital stay. Conversely, no statistically significant differences were detected between the two groups regarding the incidence of acute pancreatic fluid collections. This result opens a debate on whether the real benefit of LMWH in prophylaxis is mainly related to the drug’s action on the inflammatory cascade in the initial stages of the disease rather than to a local effect on reducing the development of walled-off necrosis, which instead and perhaps to a lesser extent, occurs in advanced stages.
Strengths and limitations
This systematic review and meta-analysis has several strengths. First, it is based on a robust GRADE methodology and, to date, it is the largest meta-analysis on the topic, with 13 studies and more than 13,000 included patients. Moreover, this meta-analysis excluded RCTs published in Chinese journals due to inappropriate randomisation procedures [52] and included the latest RCT published in May 2022 [13]. Our study did not pool together the therapeutic and preventive effects of LMWH therapy for statistical analysis as it was done previously [15]. According to GRADE, the certainty of evidence was high for the primary outcome measure, and it was highlighted by three impacting subgroup analyses, including the one for RCTs.
Several shortcomings also exist. The main limitation was the small number of included studies. Second, the risk of bias in included studies downgraded the quality of the results for some critical outcomes, including organ failure, gastrointestinal bleeding, and the need for operative interventions. Some planned analyses included few studies, especially when potential causes for heterogeneity were explored through subgroup analyses. Last, many critical outcomes, including organ failure, showed substantial heterogeneity deriving from the variability in the distribution of disease severity and study design differences.
Conclusions
This systematic review and meta-analysis supported the view that LMWH treatment is highly beneficial for the prognosis of moderately-severe and severe AP. In summary, moderate to high-quality evidence suggested early intervention with LMWH could improve the prognosis of non-mild AP in terms of mortality, organ failure, and decreased incidence of vascular thrombosis. Moreover, low to moderate quality of evidence suggested that LMWH in adjunct to conventional treatments may decrease the incidence of vascular bleeding the the length of hospital stay. In light of our findings, integrating LMWH into the treatment regimen for moderate-severe to severe AP is advocated, considering the balance between efficacy and safety. However, it is necessary to perform robust RCTs with higher power to confirm the reasonable dosage of LMWH therapy in non-mild AP further and explore the reasonable timing and course of LMWH therapy.
Availability of data and materials
All information is freely available by application to the Chief Investigator Mauro Podda (Department of Surgical Science, University of Cagliari).
References
Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology. 2013;144:1252–61. https://doi.org/10.1053/j.gastro.2013.01.068.
Wang GJ, Gao CF, Wei D, Wang C, Ding SQ. Acute pancreatitis: etiology and common pathogenesis. World J Gastroenterol. 2009;15:1427–30. https://doi.org/10.3748/wjg.15.1427.
van Santvoort HC, Bakker OJ, Bollen TL, Besselink MG, Ahmed Ali U, Schrijver AM, Boermeester MA, van Goor H, Dejong CH, van Eijck CH, van Ramshorst B, Schaapherder AF, van der Harst E, Hofker S, Nieuwenhuijs VB, Brink MA, Kruyt PM, Manusama ER, van der Schelling GP, Karsten T, Hesselink EJ, van Laarhoven CJ, Rosman C, Bosscha K, de Wit RJ, Houdijk AP, Cuesta MA, Wahab PJ, Gooszen HG, Dutch Pancreatitis Study Group. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology. 2011;141:1254–63. https://doi.org/10.1053/j.gastro.2011.06.073.
Forsmark CE, Vege SS, Wilcox CM. Acute Pancreatitis. N Engl J Med. 2016;375:1972–81. https://doi.org/10.1056/NEJMra1505202.
Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, Ball CG, Parry N, Sartelli M, Wolbrink D, van Goor H, Baiocchi G, Ansaloni L, Biffl W, Coccolini F, Di Saverio S, Kluger Y, Moore E, Catena F. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019;14:27. https://doi.org/10.1186/s13017-019-0247-0.
Antkowiak R, Bialecki J, Chabowski M, Domoslawski P. Treatment of microcirculatory disturbances in acute pancreatitis: Where are we now? Pancreas. 2022;51:415–21. https://doi.org/10.1097/MPA.0000000000002044.
Cuthbertson CM, Christophi C. Disturbances of the microcirculation in acute pancreatitis. Br J Surg. 2006;93:518–30. https://doi.org/10.1002/bjs.5316.
Chen Y, Zhou J, Li G, Tong Z, Dong J, Pan Y, Ke L, Li W, Li J. Early spontaneous abdominal bleeding is associated with poor outcome in moderate to severe Acute Pancreatitis patients: a Propensity Matched Study. Sci Rep. 2017;7:42607. https://doi.org/10.1038/srep42607.
He K, Zhang Y, Song K, Fan Z, Gong L, Shu H, Wu D. Randomized controlled trials of low molecular weight heparin in non-mild acute pancreatitis: a systemic review and meta-analysis. Thromb Res. 2023;221:26–9. https://doi.org/10.1016/j.thromres.2022.11.012.
Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013;13:e1–15. https://doi.org/10.1016/j.pan.2013.07.063.
Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis. Am J Gastroenterol. 2013;108:1400–16. https://doi.org/10.1038/ajg.2013.218.
Yokoe M, Takada T, Mayumi T, Yoshida M, Isaji S, Wada K, Itoi T, Sata N, Gabata T, Igarashi H, Kataoka K, Hirota M, Kadoya M, Kitamura N, Kimura Y, Kiriyama S, Shirai K, Hattori T, Takeda K, Takeyama Y, Hirota M, Sekimoto M, Shikata S, Arata S, Hirata K. Japanese guidelines for the management of acute pancreatitis: Japanese guidelines 2015. J Hepatobiliary Pancreat Sci. 2015;22:405–32. https://doi.org/10.1002/jhbp.259.
Patoni C, Bunduc S, Frim L, Veres DS, Dembrovszky F, Éliás AJ, Pálinkás D, Hegyi P, Erőss BM, Hegyi PJ. Low molecular weight heparin decreases mortality and major complication rates in moderately severe and severe acute pancreatitis-a systematic review and meta-analysis. Front Med (Lausanne). 2023;10:1241301. https://doi.org/10.3389/fmed.2023.1241301.
Qiu Q, Li GJ, Tang L, Guo Y, Wen LZ, Wang B, Chen DF, Liu KJ. The efficacy of low molecular weight heparin in severe acute pancreatitis: a systematic review and meta-analysis of randomized controlled trials. J Dig Dis. 2019;20:512–22. https://doi.org/10.1111/1751-2980.12815.
Wang H, Xu Y, Yang M, Zheng D, Chen L. Systematic review and meta-analysis of the safety and effectiveness of low molecular heparin for severe acute pancreatitis. Ann Palliat Med. 2021;10:11695–704. https://doi.org/10.21037/apm-21-3058.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of Observational studies in Epidemiology (MOOSE) group. JAMA. 2000;283:2008–12. https://doi.org/10.1001/jama.283.15.2008.
Higgins JPT, Thomas J, Chandler J, et al. editors. Cochrane handbook for systematic reviews of interventions version 6.4. http://www.training.cochrane.org/handbook. Accessed 14 Feb 2024.
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, Moher D, Tugwell P, Welch V, Kristjansson E, Henry DA. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. https://doi.org/10.1136/bmj.j4008.
Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, Tsiotos GG, Vege SS, Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–11. https://doi.org/10.1136/gutjnl-2012-302779.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM, Emberson JR, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JPT. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. https://doi.org/10.1136/bmj.l4898.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT, Boutron I, Carpenter JR, Chan AW, Churchill R, Deeks JJ, Hróbjartsson A, Kirkham J, Jüni P, Loke YK, Pigott TD, Ramsay CR, Regidor D, Rothstein HR, Sandhu L, Santaguida PL, Schünemann HJ, Shea B, Shrier I, Tugwell P, Turner L, Valentine JC, Waddington H, Waters E, Wells GA, Whiting PF, Higgins JP. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. https://doi.org/10.1136/bmj.i4919.
Schünemann HJ, Brennan S, Akl EA, Hultcrantz M, Alonso-Coello P, Xia J, Davoli M, Rojas MX, Meerpohl JJ, Flottorp S, Guyatt G, Mustafa RA, Langendam M, Dahm P. The development methods of official GRADE articles and requirements for claiming the use of GRADE—a statement by the GRADE guidance group. J Clin Epidemiol. 2023;159:79–84. https://doi.org/10.1016/j.jclinepi.2023.05.010.
Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5:13. https://doi.org/10.1186/1471-2288-5-13.
Patil B, Meena LN, Sharma DC, Agarwal G, Dadhich Y, Gupta G. Impact of low-molecular-weight heparin in the treatment of moderately severe and severe acute pancreatitis; a randomized, single blind, phase 3 control trial. Int J Surg. 2022;101:106621. https://doi.org/10.1016/j.ijsu.2022.106621.
Kumbha R, Bathena S, Anand HBM, Amavasya VV. Study of role of low molecular weight heparin in conjunction with conventional therapy in severe acute pancreatitis. Asian J Med Sci. 2022;13:109–16. https://doi.org/10.3126/ajms.v13i9.46834.
Kröner PT, Wallace MB, Raimondo M, Antwi SO, Ma Y, Li Z, Ji B, Bi Y. Systemic anticoagulation is associated with decreased mortality and morbidity in acute pancreatitis. Pancreatology. 2021;21:1428–33. https://doi.org/10.1016/j.pan.2021.09.003.
Vadlamudi RS, Matli VVK, Thoguluva Chandrasekar V, Kalakonda A, Rawlins SR. Chemoprophylaxis to prevent deep venous thrombosis in patients hospitalized for pancreatitis: beneficial or harmful? Cureus. 2021;13:e19645. https://doi.org/10.7759/cureus.19645.
Zhou J, Zhang H, Mao W, Ke L, Li G, Ye B, Zhang J, Lin J, Gao L, Tong Z, Li W. Efficacy and safety of early systemic anticoagulation for preventing splanchnic thrombosis in Acute Necrotizing Pancreatitis. Pancreas. 2020;49:1220–4. https://doi.org/10.1097/MPA.0000000000001661.
Han AH, Yu GQ, Yin HZ. Clinical effects of low-molecular-weight heparin combined with ulinastatin in children with acute pancreatitis. Trop J Pharm Res. 2016;15:1787–92. https://doi.org/10.4314/tjpr.v15i8.27.
DU JD, Zheng X, Huang ZQ, Cai SW, Tan JW, Li ZL, Yao YM, Jiao HB, Yin HN, Zhu ZM. Effects of intensive insulin therapy combined with low molecular weight heparin anticoagulant therapy on severe pancreatitis. Exp Ther Med. 2014;8:141–6. https://doi.org/10.3892/etm.2014.1694.
Lu XS, Qiu F, Li JQ, Fan QQ, Zhou RG, Ai YH, Zhang KC, Li YX. Low molecular weight heparin in the treatment of severe acute pancreatitis: a multiple centre prospective clinical study. Asian J Surg. 2009;32:89–94. https://doi.org/10.1016/s1015-9584(09)60017-8.
Lu XS, Qiu F, Li YX, Li JQ, Fan QQ, Zhou RG. Effect of lower-molecular weight heparin in the prevention of pancreatic encephalopathy in the patient with severe acute pancreatitis. Pancreas. 2010;39:516–9. https://doi.org/10.1097/MPA.0b013e3181c3c954.
Jiao HB, Qiao Z, Tan XL, Du JD, Fei Y, Wang DD, Li JY, Yao YM. Effects of anticoagulation therapy with low molecular weight heparin in acute pancreatitis. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2004;16:712–4.
Tozlu M, Kayar Y, İnce AT, Baysal B, Şentürk H. Low molecular weight heparin treatment of acute moderate and severe pancreatitis: a randomized, controlled,open-label study. Turk J Gastroenterol. 2019;30:81–7. https://doi.org/10.5152/tjg.2018.18583.
Chooklin S, Chuklin S, Shershen G. Enoxaparin in the management of moderately severe acute pancreatitis patients. Pancreas. 2020;49:1403.
Chuklin S, Chooklin S, Shershen G. Management of severe acute pancreatitis patients by enoxa parin. United Eur Gastroenterol J. 2019;7:226.
Podda M, Pellino G, Di Saverio S, Coccolini F, Pacella D, Cioffi SPB, Virdis F, Balla A, Ielpo B, Pata F, Poillucci G, Ortenzi M, Damaskos D, De Simone B, Sartelli M, Leppaniemi A, Jayant K, Catena F, Giuliani A, Di Martino M, Pisanu A. MANCTRA-1 Collaborative Group. Infected pancreatic necrosis: outcomes and clinical predictors of mortality. A post hoc analysis of the MANCTRA-1 international study. Updates Surg. 2023;75:493–522. https://doi.org/10.1007/s13304-023-01488-6.
Harris S, Nadkarni NA, Naina HV, Vege SS. Splanchnic vein thrombosis in acute pancreatitis: a single-center experience. Pancreas. 2013;42:1251–4. https://doi.org/10.1097/MPA.0b013e3182968ff5.
Garret C, Péron M, Reignier J, Le Thuaut A, Lascarrou JB, Douane F, Lerhun M, Archambeaud I, Brulé N, Bretonnière C, Zambon O, Nicolet L, Regenet N, Guitton C, Coron E. Risk factors and outcomes of infected pancreatic necrosis: retrospective cohort of 148 patients admitted to the ICU for acute pancreatitis. United Eur Gastroenterol J. 2018;6:910–8. https://doi.org/10.1177/2050640618764049.
Schepers NJ, Bakker OJ, Besselink MG, Ahmed Ali U, Bollen TL, Gooszen HG, van Santvoort HC, Bruno MJ, Dutch Pancreatitis Study Group. Impact of characteristics of organ failure and infected necrosis on mortality in necrotising pancreatitis. Gut. 2019;68:1044–51. https://doi.org/10.1136/gutjnl-2017-314657.
Podda M, Di Martino M, Ielpo B, Catena F, Coccolini F, Pata F, Marchegiani G, De Simone B, Damaskos D, Mole D, Leppaniemi A, Sartelli M, Yang B, Ansaloni L, Biffl W, Kluger Y, Moore EE, Pellino G, Di Saverio S, Pisanu A. The 2023 MANCTRA Acute biliary pancreatitis care bundle: a joint effort between human knowledge and Artificial Intelligence (ChatGPT) to optimize the care of patients with Acute biliary pancreatitis in Western Countries. Ann Surg. 2024;279:203–12. https://doi.org/10.1097/SLA.0000000000006008.
Crockett SD, Wani S, Gardner TB, Falck-Ytter Y, Barkun AN, American Gastroenterological Association Institute Clinical Guidelines Committee. American Gastroenterological Association Institute Guideline on Initial Management of Acute Pancreatitis. Gastroenterology. 2018;154:1096–101. https://doi.org/10.1053/j.gastro.2018.01.032.
National Guideline Centre (UK). Pancreatitis. London: National Institute for Health and Care Excellence (NICE); 2018.
Renzulli P, Jakob SM, Täuber M, Candinas D, Gloor B. Severe acute pancreatitis: case-oriented discussion of interdisciplinary management. Pancreatology. 2005;5:145–56. https://doi.org/10.1159/000085266.
Perretti M, Page CP. Heparin and inflammation: a new use for an old GAG? Gut. 2000;47:14–5. https://doi.org/10.1136/gut.47.1.14.
Kylänpää ML, Repo H, Puolakkainen PA. Inflammation and immunosuppression in severe acute pancreatitis. World J Gastroenterol. 2010;16:2867–72. https://doi.org/10.3748/wjg.v16.i23.2867.
Gray E, Mulloy B, Barrowcliffe TW. Heparin and low-molecular-weight heparin. Thromb Haemost. 2008;99:807–18. https://doi.org/10.1160/TH08-01-0032.
Mulloy B, Hogwood J, Gray E, Lever R, Page CP. Pharmacology of Heparin and related drugs. Pharmacol Rev. 2016;68:76–141. https://doi.org/10.1124/pr.115.011247.
Yan Y, Ji Y, Su N, Mei X, Wang Y, Du S, Zhu W, Zhang C, Lu Y, Xing XH. Non-anticoagulant effects of low molecular weight heparins in inflammatory disorders: a review. Carbohydr Polym. 2017;160:71–81. https://doi.org/10.1016/j.carbpol.2016.12.037.
Manfredi AA, Rovere-Querini P, D’Angelo A, Maugeri N. Low molecular weight heparins prevent the induction of autophagy of activated neutrophils and the formation of neutrophil extracellular traps. Pharmacol Res. 2017;123:146–56. https://doi.org/10.1016/j.phrs.2016.08.008.
Qiu F, Lu XS, Huang YK. Protective effect of low-molecular-weight heparin on pancreatic encephalopathy in severe acute pancreatic rats. Inflamm Res. 2012;61:1203–9. https://doi.org/10.1007/s00011-012-0517-8.
Park WS, Kim HI, Jeon BJ, Kim SH, Lee SO. Should anticoagulants be administered for portal vein thrombosis associated with acute pancreatitis? World J Gastroenterol. 2012;18:6168–71. https://doi.org/10.3748/wjg.v18.i42.6168.
Yin Y, Wang L, Gao F, Liu L, Qi X. Anticoagulation therapy for splanchnic vein thrombosis associated with acute pancreatitis: a systematic review and meta-analysis. Clin Appl Thromb Hemost. 2023;29:10760296231188718. https://doi.org/10.1177/10760296231188718.
Anis FS, Adiamah A, Lobo DN, Sanyal S. Incidence and treatment of splanchnic vein thrombosis in patients with acute pancreatitis: a systematic review and meta-analysis. J Gastroenterol Hepatol. 2022;37:446–54. https://doi.org/10.1111/jgh.15711.
Hajibandeh S, Hajibandeh S, Agrawal S, Irwin C, Obeidallah R, Subar D. Anticoagulation versus no anticoagulation for splanchnic venous thrombosis secondary to acute pancreatitis: Do we really need to treat the incidental findings? Pancreas. 2020;49:e84-5. https://doi.org/10.1097/MPA.0000000000001644.
Boxhoorn L, Voermans RP, Bouwense SA, Bruno MJ, Verdonk RC, Boermeester MA, van Santvoort HC, Besselink MG. Acute pancreatitis. Lancet. 2020;396:726–34. https://doi.org/10.1016/S0140-6736(20)31310-6.
Besselink MG. Splanchnic vein thrombosis complicating severe acute pancreatitis. HPB (Oxford). 2011;13:831–2. https://doi.org/10.1111/j.1477-2574.2011.00411.x.
Nadkarni NA, Khanna S, Vege SS. Splanchnic venous thrombosis and pancreatitis. Pancreas. 2013;42:924–31. https://doi.org/10.1097/MPA.0b013e318287cd3d.
Acknowledgements
None.
Funding
This research was funded by the University of Cagliari (Italy), Department of Surgical Science, Italian Ministry of University and Research (Ministero dell’Università e della Ricerca Italiano), PRIN (Progetti di Ricerca di Rilevante Interesse Nazionale) 2022, ID 202273A4YP, Grant Number F53D23006530006.
Author information
Authors and Affiliations
Contributions
MP: Conceptualization, data collection and curation, formal analysis, investigation, methodology, project administration, supervision, validation, original draft preparation, reviewing and editing; VM: Conceptualization, data collection and curation, formal analysis, investigation, methodology, validation, original draft preparation, reviewing and editing; PM: Conceptualization, data collection and curation, formal analysis, investigation, methodology, validation, original draft preparation, reviewing and editing; MDM: Conceptualization, data curation, formal analysis, investigation, methodology, validation, original draft preparation, reviewing and editing; BDS: Conceptualization, data curation, formal analysis, investigation, methodology, validation, original draft preparation, reviewing and editing; KJ: Conceptualization, data curation, formal analysis, investigation, methodology, validation, original draft preparation, reviewing and editing; MO: Conceptualization, data curation, formal analysis, investigation, methodology, validation, original draft preparation, reviewing and editing; FC: Conceptualization, data curation, formal analysis, investigation, methodology, validation, original draft preparation, reviewing and editing; MS: Conceptualization, data curation, formal analysis, investigation, methodology, validation, original draft preparation, reviewing and editing; FC: Conceptualization, data curation, formal analysis, investigation, methodology, validation, original draft preparation, reviewing and editing; BI: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, supervision, validation, original draft preparation, reviewing and editing; AP: Conceptualization, data collection and curation, formal analysis, investigation, methodology, project administration, supervision, validation, original draft preparation, reviewing and editing.
Corresponding author
Ethics declarations
Consent for publication
Not applicable. No patient information is disclosed.
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
No formal ethics approval was required by any of the ethics committees of the centres involved in this study due to its design (systematic review and meta-analysis of primary studies).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
13017_2024_558_MOESM2_ESM.doc
Supplementary Material 2: Table 2 Baseline Clinical Characteristics of the patients included in the systematic review and meta-analysis.
13017_2024_558_MOESM3_ESM.doc
Supplementary Material 3: Table 3 Baseline Laboratory Characteristics of the patients included in the systematic review and meta-analysis.
13017_2024_558_MOESM4_ESM.doc
Supplementary Material 4: Table 4 Baseline Laboratory Characteristics of the patients included in the systematic review and meta-analysis (2).
13017_2024_558_MOESM9_ESM.tiff
Supplementary Material 9: Figure 1 Funnel Plots for the assessment of the risk of publication bias: A: Mortality; B: Need for any type of operative intervention during treatment; C: Organ failure.
13017_2024_558_MOESM10_ESM.tiff
Supplementary Material 10: Figure 2 Forest plots for the assessment of the distribution of baseline characteristics: A: Sex; B: Age; C: aPTT; D: Balthazar score; E: Charlson's CI; F: CTSI; G: Platelet count; H: Serum amylase; I: Serum bilirubin; L: Serum albumin; M: APACHE II score.
13017_2024_558_MOESM11_ESM.tiff
Supplementary Material 11: Figure 3 Meta-analysis of secondary outcomes: A: APACHE II; B: ICU admission; C: Time to tolerance of diet; D: Systemic complications; E: Cured illness; F: Local complications.
13017_2024_558_MOESM12_ESM.tiff
Supplementary Material 12: Figure 4 Meta-analysis of secondary outcomes: A: Gastrointestinal bleeding; B: Length of hospital stay; C: Need for operative interventions; D: Need for surgical intervention; E: Vascular thrombosis; F: Balthazar score.
13017_2024_558_MOESM13_ESM.tiff
Supplementary Material 13: Figure 5 Meta-analysis of laboratory parameters after treatment: A: Platelets; B: Albumin; C: PT.
13017_2024_558_MOESM14_ESM.tiff
Supplementary Material 14: Figure 6 Subgroup analysis: Moderately-severe vs severe acute pancreatitis: A: Mortality; B: Need for operative intervention; C: Organ failure.
13017_2024_558_MOESM15_ESM.tiff
Supplementary Material 15: Figure 7 Subgroup analysis: Duration of LMWH therapy (<8 days vs 8-14 days): A: Mortality; B: Need for operative intervention; C: Organ failure.
13017_2024_558_MOESM16_ESM.tiff
Supplementary Material 16: Figure 8 Subgroup analysis: Dose of LMWH (Prophylactic vs Therapeutical): A: Mortality; B: Need for operative intervention; C: Organ failure.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Podda, M., Murzi, V., Marongiu, P. et al. Effectiveness and safety of low molecular weight heparin in the management of acute pancreatitis: a systematic review and meta-analysis. World J Emerg Surg 19, 30 (2024). https://doi.org/10.1186/s13017-024-00558-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13017-024-00558-3