
Abstract
Aim
To evaluate the patterns of loco-regional recurrences in head and neck cancer patients
Methods
Twenty-six out of 112 patients treated with primary or postoperative 3D CRT or IMRT for their primary and recurrent disease between 2007 and 2013 were included. The CT images of recurrent disease were rigidly registered with the primary CT images for each patient. To assess overlaps and overlap localization, the recurrence volume overlapping with the primary target volume was identified. For relapses occurring in the regional lymph nodes, the epicenter distance in recurrences and primary volumes and dose in recurrences were also identified. The recurrences were defined as in-field, marginal or out-of-field.
Results
The majority of the failures occurred within 1 year after completed primary treatment. The dose differences in recurrence volume were not statistically significant when patients were treated with IMRT or 3D CRT. Recurrence in 15/26 of the included patients occurred in the regional lymph nodes located fully or partly inside the primary target volume or the elective lymph node region. The majority of recurrences were recognized as in-field, independent of the primary treatment.
Conclusion
Recurrence in the majority of the patients occurred in the regional lymph nodes located in high dose area. The cause of recurrence may be due to inadequate total dose in the primary treatment and/or lack of optimal primary diagnosis leading to inadequate primary target delineation.
Similar content being viewed by others

Introduction
The incidence of oral cavity/pharynx and larynx cancer in Europe was estimated to 100,000 and 40,000, respectively, in 2012 [1]. In Norway, 800 patients were diagnosed with head and neck cancer (HNC) in 2014, representing 2.5% of the total incidence of malignant disease [2].
Management of HNC is multi-disciplinary; surgery, radiotherapy (RT) with or without concomitant chemotherapy. High dose RT (prescribing doses typically of 70 Gy) is necessary to achieve cure, but may result in side effects. The employment of three-dimensional conformal radiotherapy (3D CRT) and intensity-modulated radiotherapy (IMRT) have permitted treatment largely conforming to the disease extensions for the individual patient [3,4,5,6]. However, each year, 30–50% of patients with locally advanced HNC, experience loco-regional relapse [7]. Loco-regional recurrence is still one of the major causes of failure in HNC after radical treatment [7]. Therefore, it is important to evaluate the patterns of loco-regional recurrences in patients treated with 3D CRT and IMRT. Specifically, it is relevant to learn more about the cause of relapse, the dose delivered to the tissue in question and the proximity of the tumor recurrence to the original target structures. To address this issue, we have analyzed recurrence patterns in patients with recurrent HNC previously treated with 3D CRT and IMRT at our institution. A detailed mapping of the primary treatment, the patient dose distributions and subsequent recurrence patterns are provided.
Methods
Patients
We retrospectively reviewed the medical records of 112 patients with primary squamous cell carcinoma in the head and neck reirradiated between January 2007-December 2013. To be included in the current study the following criteria had to be fulfilled: i) re-irradiation for first relapse in the head and neck region, ii) radiotherapy for both primary and recurrent disease at Oslo University Hospital, iii) Computed Tomography (CT), and/or Positron Emission Tomography (PET)/magnetic resonance images (MRI) taken prior to RT, iv) available RT dose plans for the primary and recurrent disease which were technically possible to co-register, v) completed their planned curative primary radiation treatment.
Of the 112 patients, 26 patients fulfilled the inclusion criteria. The general characteristics of the patients and tumor site are detailed in Table 1. The patterns of recurrence were analyzed separately in 2 groups of patients based on the primary treatment they received; patients treated with primary RT (n = 10) and postoperative RT (n = 16). The time difference between primary RT and reirradiation varied between 4 and 63 months (Tables 2 and 3). At the time of recurrence, 16 of 26 patients had their gross tumor removed before reirradiation. In these patients, the gross tumor was delineated on the relapse RT CT images based on the diagnostic CT examination taken prior to relapse surgery.
Only 2 of the 26 patients received concomitant chemotherapy (Table 1). For the primary treatment, 12 of 26 patients received IMRT while 14 patients were treated with 3D CRT for their HNC disease as reported in Tables 2 and 3.
Tumor delineation
Tumor volumes were defined by an experienced radiation oncologist on simulation CT images acquired in conjunction with primary and recurrent RT, registered in some cases with MRI and/or Fluorodeoxyglucose (18 F-FDG) PET images. The gross tumor volume (GTV; GTVp for primary GTV and GTVr for recurrence GTV) was defined as the visible tumor based on all available diagnostic imaging as well as clinical examination. The high risk and standard risk areas with 10 mm margin to GTV was included in the clinical target volume (CTV, CTVp and CTVr). CTV also included non-dissected lymph nodes. The planning target volume (PTV, PTVp and PTVr) was constructed by expanding the corresponding CTV by 3 mm [8, 9].
Image registration and overlap definition
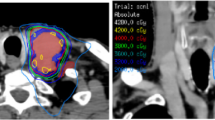
Relapse localization on CT images was further investigated by using the software module Oncentra Masterplan (version 4.3). The recurrence treatment planning CT for each included patient was exported to the respective primary dose plan-CT series. The exported recurrence dose plan CT was further rigidly registered with the primary dose plan-CT for each patient using available image registration tools. To achieve an optimal image registration, the information such as skull base, frontal bone and other bony structures were used. After CT image registration, the GTVr from the recurrence dose plan-CT was copied and pasted into the primary dose plan CT dataset. The HNC oncologist (JFE) also approved the quality of image registration for each included patient (Fig. 1).

Fusion display of primary (gray) and recurrence (pink) CT images
To assess overlaps, the GTVr overlapping with the GTVp in each primary CT slice was identified and delineated as illustrated in Fig. 2. For cases with relapses located fully or partly in the elective nodes, no overlap volume was assessed. Then the dose of both the primary RT plan and of the reirradiation plan in the overlap area was calculated.

Definition of overlap volume
To explain the cause of relapse, it was assessed whether the relapse occurred in the regional lymph nodes or not. The localization of the regional lymph node relapse was assessed by our oncologist.
The epicenter in GTVr and GTVp were defined, the dose and distance between the 2 epicenters were calculated. Epicenter was estimated from the center of mass. A mean epicenter distance value was calculated in cases with more than one GTVr.
The recurrence volumes were considered as in-field, marginal and out-of-field, if the dose in the epicenter of the recurrence volume was located in high, low or very low dose areas, respectively. Cases with their relapse located in 2 regional lymph nodes with different location, were labelled with 2 relapse site definitions but one mean epicenter dose.
Statistics
To assess the dose differences when employing IMRT or 3D CRT, a two-tailed independent T-test was employed. A p value < 0.05 was considered as statistically significant.
Ethics
All necessary approvals were obtained before the study was conducted. Written informed consent was obtained from all patients in accordance with the procedures of the Data Protection Office of whom also approved this study.
Results
The range of the total prescribed RT dose for primary HNC treatment was 50–70 Gy, as shown in Tables 2 and 3. In total 13 (50%) of the failures occurred within 1 year after primary treatment, 6 (23%) within 2 years and 7 (27%) within 3 to 5 years. In patients treated with postoperative RT compared to those treated with primary RT, the fraction of the recurrences occurring within 1 year was approximately 3 times higher. The fraction of patients with relapse within 2 years was 4 times higher in the patient group treated with primary RT compared to postoperative RT patient group. The fraction of patients with relapse within 3–5 years after primary treatment was identical in both patient groups.
The population-averaged median dose to the recurrence volume for 26 patients receiving either IMRT or 3D CRT was 65.3, and 45.1 Gy, respectively (Data not shown). No statistically significant dose differences were observed between the employed RT techniques.
Recurrence occurred in the regional lymph nodes in 4 out of 10 patients treated with primary RT compared to 11 out of 16 patients treated with postoperative RT as shown in Tables 4 and 5.
Total relapse dose in patients who received primary RT varied from 27 to 71 Gy and in the patients treated with postoperative RT from 2 to 66 Gy (Tables 4 and 5). The dose in epicenters and distance between epicenters in GTVr and GTVp are shown in the Tables 4 and 5.
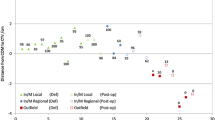
There were 1 and 3 out-of-field recurrences in patients treated with primary RT and postoperative RT, respectively. One of 10 patients treated with primary RT and 2 of 16 patients treated with postoperative RT had marginal relapses (Tables 6 and 7 and Fig. 3). Eight and 11 in-field recurrences were identified in patients treated with primary RT and postoperative RT, respectively (Tables 6 and 7 and Fig. 3). The GTVr and GTVp epicenter distance in patients treated with primary RT and postoperative RT was 0.4–6.1 and 1.2–13.7 cm, respectively. The average epicenter distance for in-field, marginal and out-of-field recurrences were 3.8, 6.3 and 9.4 cm.

Schematic representation of 26 recurrences included in this study. Patients treated with primary RT and postoperative RT are shown with case number in black and red, respectively
The size of recurrence volume varied between 6.5 to 76 ccm and 2.1 to 119.3 ccm in patients treated with primary RT and postoperative RT, respectively (Tables 6 and 7).
The mean overlap size for primary RT was 10.4 ccm (SD ± 8.6) compared to patient group receiving postoperative RT of 5.6 ccm (SD ± 11,8) (Tables 4 and 5) (p = 0.23).
Discussion
This study analyzed the failure patterns of 26 HNC patients treated with RT for their relapse disease. Our analyses show that the majority of the failures occurred within 1 year after completed primary treatment. There was no statistical difference in the doses to the recurrence volume in patients treated with IMRT or 3D CRT technique. The majority of the recurrence in the patients treated with postoperative RT occurred in the regional lymph nodes. The recurrent lymph nodes were located fully or partly inside the elective lymph node region in the majority of these patients. The majority of recurrences were recognized as in-field, independent of the primary treatment.
Due et al. [10] have analyzed the recurrence pattern in 39 HN squamous cell carcinoma patients with loco-regional failure treated with chemoradiation. Due and colleagues [10] reported that 96% of recurrences were located in the high dose region. Another study carried out by Soto et al. [11] showed that 100% (9/9) of the included HNC patients with loco-regional failure were located inside the primary GTV. The shorter average epicenter distance of 3.8 cm between GTVr and GTVp, the high epicenter dose in GTVr and the reported site of recurrences in this study show that the majority of recurrences (73%) are also located in high dose area in accordance with the studies of Due et al. and Sot et al. [10, 11].
In the study of Due et al. [10] all the included patients were treated with primary RT, while in the current study only 10 of the included patients received primary RT and 16 patients were treated with postoperative RT. Our results showed no correlation between the recurrence patterns and the kind of primary treatment the patients had received. The cause of relapse in the study of Due et al. [10] seems to be insufficient total dose to the primary GTV. However, in the present study the relapse could be due to: i) inadequate total dose to the primary target volume and/or ii) imprecise diagnostic imaging of the primary tumor volume leading to inadequate primary target delineation. In the majority of the cases (15/26) in our study, regional recurrences occurred in lymph nodes partly or fully located in the area of the primary GTV or elective lymph nodes. Therefore, it may be questioned whether the total dose in this area was adequate or not. In the marginal and out-of-field recurrences the cause of relapse seems to be due to the insufficient primary target delineation. Increased use of FDG-PET in defining the GTV as discussed in the study of Soto et al. [11] could probably improve the accuracy of the tumor definition.
IMRT and 3D CRT techniques are usually employed in the standard management of HNC patients. In only one of the marginal recurrences in this study IMRT technique was used in the delivery of their primary RT. Increased risk of marginal misses is often mentioned as one of the disadvantages associated with IMRT [12]. Precise target definition is therefore crucial to avoid marginal miss.
One limitation of the current study is the heterogeneity of the patient cohort and their stage of disease. However, it is important to stress that the goal of this study was to assess the relapse localization and the cause of it. Another limitation is that the CT slice thickness in primary and recurrence CT scans were not always identical. This may have resulted in less precise fusion of the primary and relapse CT scans. In general, some uncertainty can be associated with the rigid registration process because of anatomical changes between the primary and recurrence RT. However, our experienced oncologist has studied the detailed disease information in each medical record and diagnostic CT images and compared them with the recurrence localization assessed after registration. Another limitation when using rigid registration is inaccurate estimate of the dose distribution in the CT series of the recurrence volume.
Conclusion
The cause of recurrence in the majority of the patients seems to be inadequate dose to the primary treatment volume and in some few cases due to imprecise primary diagnostic imaging leading to inadequate primary target delineation. The majority of recurrences were recognized as in-field, independent of the primary treatment. Further investigation is necessary to evaluate the total RT dose needed to treat the primary HNC. Optimal diagnostic methods should be employed to avoid poor primary target delineation.
Abbreviations
- 18 F-FDG:
-
Fluorodeoxyglucose
- 3D CRT:
-
Three-dimensional conformal radiotherapy
- CT:
-
Computer tomography
- CTV:
-
Clinical target volume
- GTV:
-
Gross tumor volume
- HNC:
-
Head and neck cancer
- IMRT:
-
Intensity-modulated radiotherapy
- MRI:
-
Magnetic resonance images
- PET:
-
Positron emission tomography
- RT:
-
Radiotherapy
References
Braakhuis BJM, Leemans CR, Visser O. Incidence and survival trends of head and neck squamous cell carcinoma in the Netherlands between 1989 and 2011. Oral Oncol. 2014;50(7):670–5.
Cancer in Norway 2010, Cancer Registry of Norway, Institute for epidemiological cancer research.
Kam MK, Chau RM, Suen J, et al. Intensity-modulated radiotherapy in nasopharyngeal carcinoma: Dosimetric advantage over conventional plans and feasibility of dose escalation. Int J Radiat Biol Phys. 2003;56:145–57.
Xia P, Fu KK, Wong GW, et al. Comparison of treatment plans involving intensity-modulated radiotherapy for nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2000;48:329–37.
Chao KS, Deasy J, Markman J, Haynie J, Perez CA, Purdy JA, et al. A prospective study of salivary function sparing in patients with head-and-neck cancers receiving intensity modulated or three-dimensional radiation therapy: initial results. Int J Radiat Oncol Biol Phys. 2001;49:907–16.
Eisburch A, Marsh LH, Martel MK, Ship JA, Ten Haken R, Pu AT, et al. Comprehensive irradiation of head and neck cancer using conformal multisegmental fields: assessment of target coverage and noninvolved tissue sparing. Int J Radiat Oncol Biol Phys. 1998;41:559–68.
Jeong S, Yoo EJ, Kim JY, Han CW, Kim KJ, Kay CS. Re-irradiation of unresectable recurrent head and neck cancer: using Helical Tomotherapy as image-guided intensity-modulated radiotherapy. Radiat Oncol J. 2013;31(4):206–15.
Ng WT, Lee MC, Hung WM, et al. Clinical outcomes and patterns of failure after intensity-modulated radiotherapy for nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2011;79:420–8.
Dawson LA, Yoshimi A, Marsh L, et al. Patterns of local-regional recurrence following parotid-sparing conformal and segmental intensity-modulated radiotherapy for head and neck cancer. Int J Radiat Oncol Biol Phys. 2000;46:1117–26.
Due AK, Vogelius IR, Aznar MC, et al. Recurrences after intensity modulated radiotherapy for head and neck squamous cell carcinoma more likely to originate from regions with high baseline [18 F]-FDG uptake. Radiot Oncol J. 2014;111:360–5.
Soto SE, Kessøer ML, Piert M, et al. Correlation between pretreatment FDG-PET biological target volume and anatomical location of failure after radiation therapy for head and neck cancers. Radiot Oncol J. 2008;89:13–8.
Mendenhall WM, Amdur RJ, Palta JR. Intensity-modulated radiotherapy in the standard management of head and neck cancer: promises and pitfalls. J Clin Oncol. 2006;24(17):2618–23.
Acknowledgements
This study was supported by a grant from the Norwegian Cancer Society.
Funding
None
Availability of data and materials
Contact the corresponding author
Authors’ contributions
SJ carried out data collection, study design and drafted the manuscript. JFE contributed to data quality assurance. EM, ED and CDA contributed to study design, participated in the drafting of the manuscript and review. MHN contributed to the data collection. TF contributed to establish the employed rigid fusion method and contributed to the drafting of the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Obtained
Ethics approval and consent to participate
Obtained
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Johansen, S., Norman, M.H., Dale, E. et al. Patterns of local-regional recurrence after conformal and intensity-modulated radiotherapy for head and neck cancer. Radiat Oncol 12, 87 (2017). https://doi.org/10.1186/s13014-017-0829-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13014-017-0829-5