
Abstract
Background
The association between international migration and mental health is conditioned to several factors, and discrimination may play a significant role. Currently, Peru is one of the principal Venezuelan migrant-receiving countries in Latin America. There are around one million Venezuelan refugees and migrants in the country. This study evaluates the association between self-perceived discrimination and mental health problems in Venezuelan population living in Peru.
Method
We analyzed data from the Venezuelan Population Residing in Peru Survey 2018, a nationally representative urban sample aimed at collecting information on several dimensions of Venezuelan population wellbeing. We applied logistic regression models to assess the association between self-perceived discrimination and mental health problems. Moreover, we applied the propensity score matching method as a robustness check of our results.
Results
Of 9487 Venezuelans surveyed, 6806 included complete information. From this sample, 6.3% reported mental health problems related to fear, anger, anxiety, or stress. Logistic regression models showed that Venezuelans who perceived being discriminated against had 2.4 higher odds of presenting mental health problems than their non-discriminated counterparts. Moreover, propensity score matching models showed that Venezuelans who perceived being discriminated against increased by 3.5 percentage points their probability of presenting mental health problems compared to their non-discriminated counterparts.
Conclusions
There is evidence that self-perceived discrimination is associated with mental health deterioration in Venezuelan migrants living in Peru. Our findings are relevant in the current geopolitical context and could be useful in the decision making processes in international health.
Similar content being viewed by others


Background
International migration is a complex phenomenon that involves a multiplicity of economic, social and security contents given an increasingly interconnected world. The lives of international migrants are challenging and several social factors can affect their wellbeing during transit and settlement [1, 2]. Many migrants labor in informal jobs associated with human rights violations, undignified wages, and exploitation; and many live in low quality and overcrowded households [2, 3]. They have limited healthcare access, and many of them fear using the healthcare system when required [1]. They also experience multiple types of discrimination when trying to integrate into the host society [4, 5]. Consequently, the study of discrimination as a factor that affects the health of international migrants is a highly important matter.
Since the 2000s, international migration flows in Latin America have shown changes in direction and intensity. Currently, the “Venezuelan phenomenon” has brought essential repercussions in the region. The Venezuelan migration process is based on three phases, shifting from a migrant-receiving to a migrant-sending country [6]. The first phase began in 2000 after Hugo Chávez won the presidential election and implemented the “Socialism of the Twenty-First Century”. Venezuelans from the upper classes emigrated to developed countries, given their disagreements with Chavez’s radical reforms. The second phase corresponds to the end of the Latin American commodity growth. Venezuelan economy entered a great recession and migrant profile shifting, people from lower classes migrated to geographically proximate countries, such as Colombia. Finally, the third phase of migration began in 2015, after the election of Nicolas Maduro as president. The collapse of the Venezuelan economic leads to a severe humanitarian crisis, including a lack of food security and a broken public health system [6]. The current phase has to Peru as one of the principal migrant-receiving, with around one million Venezuelan migrants [7], significantly higher than internal migration flows [8]. Consequently, the Venezuelan migratory phenomenon is a unique and novel that deserves special attention and research.
The association between international migration and mental health is conditioned to several factors, and self-perceived discrimination may play a significant role. International migration has been discussed as a potential risk factor for mental health illness [9, 10]. Besides psychiatric illness, psychosocial factors may play a role in immigrants’ subjective wellbeing [9, 10]. Indeed, the literature suggests some plausible mechanisms to explain why there might be a higher prevalence of mental health illness in some vulnerable migrant groups [11,12,13]. Conflict and migration-related experiences, socioeconomic disadvantage, social marginalization, and a sense of sacrifice and sadness are critical elements for explaining this health disadvantage [12,13,14,15]. Evidence suggests that self-perceived discrimination among migrants profoundly affects their physical and psychological wellbeing in European and Asian countries [16,17,18,19,20,21]. In general, the relationship between the risk of mental illness and international migration continues to be complicated and difficult to disentangle. However, for Latin America, discrimination seems to be one of the main factors that could explain this problem.
Considering the above, this study aims to evaluate the association between self-perceived discrimination and mental health problems in the Venezuelan population living in Peru. The findings may help policymakers in a context where flows of Venezuelan migration may grow in coming years, as a complex humanitarian crisis is taking place in the region due to the largest Venezuelan exodus in history.
Methods
Design and data sources
We carried out a secondary cross-sectional analysis based on data from the 2018 Venezuelan Population Residing in Peru Survey (ENPOVE-2018), designed by the National Institute of Statistics and Informatics of Peru. The ENPOVE-2018 included a nationally representative urban sample of six Peruvian regions (Tumbes, La Libertad, Arequipa, Cusco, Lima, and Callao), which were selected since they reported the highest flows of Venezuelan migration. Likewise, the survey collected information on several dimensions of the Venezuelan population’s wellbeing, such as demographics, socioeconomic status, immigration status, discrimination, and violence characteristics. Data were collected from 26 November 2018 to 31 December 2018 through structured questionnaires applied by trained interviewers at home with every household member. The response rate was 99.6%.
Population, sampling, and sample
The ENPOVE-2018 survey involved 3611 households and 9487 Venezuelans residing in Peru. This survey used a probabilistic, stratified, and region-independent sampling, where sampling units were blocks and households with Venezuelan residents. Our study included only the working-age population (aged 14+ years) with health indicators available, including mental health characteristics. We also excluded the population with missing labor-income values.
Variables and measures
The outcome variable was the presence of mental health problems defined by the survey as adverse emotional and psychological reactions such as fear, anger, anxiety, or stress. This self-reported variable was built through a question with a binary answer (yes/no): “Since your arrival in Peru: Did you present with any problem associated with fearing, anger, anxiety, stress or similar?”
The main exposure was the self-perception of discrimination for being a Venezuelan immigrant. This self-reported variable was collected through a question with binary answer (yes/no): “Have you been discriminated against for Venezuelan immigrant status since your arrival in Peru?”
Moreover, we included the following control variables: sex (binary: male/female), age groups (ordinal in tertiles), marital status (binary: married or living together/other), minimum wage (binary: yes/no), education level (ordinal: no education/primary/secondary/tertiary), time spent in the country since arrival (ordinal: 6 months/6–12 months/+ 12 months in Peru), socioeconomic status constructed by INEI (ordinal: lower/middle/higher), and perceived social support (binary: yes/no).
Statistical analysis
All analyses were performed in Stata 15.0® (StataCorp, College Station, Texas, US) considered sampling weights [22]. We describe numeric variables using mean + standard deviation and categorical variables using relative/absolute frequencies. We tested a preliminary association between self-perceived discrimination and mental health problems by Pearson’s Chi-Squared test. The same procedure was done to show the association between control and outcome variables.
To assess the association between self-perceived discrimination and mental health problems, we estimated prevalence odds ratios with their 95% confidence intervals (CI) using logistic regression models at crude (cOR) and adjusted (aOR) by statistical (p-value under 0.2 in bivariate analysis) and epidemiological criteria (according to the classic confounding definition) [23]. In adjusted models, the minimum wage was not included due to collinearity with socioeconomic status. Moreover, we estimated marginal effects to measure changes in the likelihood of mental health problems given self-perceived discrimination. We considered statistically significant coefficients for a p < 0.05.
Finally, we performed a propensity score matching (PSM) [24, 25] approach as a robustness check. PSM approach is a useful technique to minimize selection bias arising from observable variables. In our analysis, the PSM allowed us to compare discriminated and non-discriminated Venezuelan immigrants with similar characteristics. We used different matching algorithms [24, 26], namely nearest neighbor matching, five nearest neighbor matching, radius matching, and kernel matching. Several studies suggest using kernel matching as the main statistic estimator and the rest as a sensitivity analysis [27, 28].
Results
Sample characteristics
Of 9487 Venezuelans surveyed, 7939 were working-age population, and full information was available for 6806 of them, represented 85.7% of the working-age sample (Descriptive characteristics of the non-included sample are in A1 Table). From the final sample, 39% have perceived discrimination due to their migration status, and 6.3% reported at least one mental health problem related to fear, anger, anxiety or stress. The mean age was 30.8 ± 0.2, 58% were male, 57% were married or living with their partner, and around 85% completed at least a secondary educational level. The mean monthly salary-income was 1116 ± 14.4 soles (approximately US$329), 33% earn less than minimum wage, around 30% had spent at least one year in Peru, only 1.4% had received social support from any institution in the country; and 11.9, 55.3 and 32.7% were qualified in the lower, middle and higher socioeconomic status, respectively (Table 1).
Differences by mental health problems
We found a significant association between mental health problems and self-perceived discrimination. Venezuelans who perceived being discriminated against showed a higher prevalence of mental health problems than their non-discriminated counterparts (p < 0.001). Moreover, we found a significant association between mental health problems and sex; female Venezuelans reported a higher prevalence of mental health problems than male counterparts (p < 0.001) (Table 2).
Association between perceived discrimination and mental health
In the unadjusted logistic regression model, Venezuelans who perceived being discriminated against had higher odds of reporting mental health problems than those who did not perceive discrimination (cOR:2.50, 95%CI:1.77–3.53). This result was similar in statistical (aOR:2.35, 95%CI:1.67–3.30) and epidemiological (aOR:2.39, 95%CI:1.69–3.37) adjusted models (Table 3). Other variables associated with mental health problems were sex and socioeconomic status. Findings from crude prevalence odds ratios are in A2 Table.
The marginal effects showed that Venezuelans who perceived being discriminated against had a 5% higher probability of presenting a mental health problem compared to those who did not perceive discrimination (p < 0.001) (Table 3).
Effect of perceived discrimination on mental health, propensity score matching
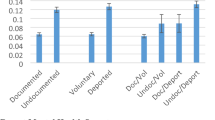
In our analysis, PSM models successfully reduced selection bias due to measured confounders from 5 to 1% in all cases approximately. On average, the final adjusted PSM models showed that Venezuelans who perceived being discriminated against increased in 3.5 percentage points their probability of presenting mental health problems compared to their non-discriminated counterparts (p < 0.01) (Table 4).
Discussion
Summary of main findings and international comparison
Our results show that self-perceived discrimination is associated with mental health problems among Venezuelans living in Peru, independent of relevant control variables. Migration is a core issue of global health in which multidisciplinary studies should analyze all phases of the process: before, during and after transit [1, 14, 29, 30]. There is a growing interest in developing research focused on post-migration stressors’ psychological effects in the settlement environment, where discrimination has a fundamental role [4, 10, 12]. Venezuelans face multiple challenges in living and surviving out of their country. Therefore, forced migration has significantly increased in the last two years [31, 32]. That has led to significant consequences on both Venezuela and Latin American countries, including the impacts on health [31, 33]. The current crisis in Venezuela and the subsequent migration is unprecedented in the region and Peru is a country that has received a significant proportion of Venezuelan migrants [7]. We found a higher prevalence and a higher probability of presenting mental health problems in Venezuelans with self-perceived discrimination compared to Venezuelans without this perception. Our study constitutes one of the first analysis of this association in Latin America and are relevant to the current geopolitical discussion. They could also be useful in international health policy decision-making processes related to international migration and population health issues.
Our findings are consistent with the literature regarding perceived discrimination, as previous studies found that it is associated with mental health alterations in migrant population. A meta-analytic review concluded that perceived discrimination’s pervasiveness has detrimental effects on psychological wellbeing [34]. A study of seven European countries reveal that the migrant population had a higher frequency of depressive symptoms and that discrimination was associated with this outcome [17]. In Norway, a study found that perceived discrimination was not associated with general health; however, it was associated with higher odds of mental health problems, even after controlling for socio-demographic and psychosocial variables [35]. In England, a study reported that discrimination experiences were associated with common mental disorders; however, magnitudes varied by migration status and race/ethnicity [18]. A Dominican Republic study suggested that perceived discrimination and humiliation contributed to Haitian migrant mental ill-health [19]. In Brazil, discrimination was associated with posttraumatic stress disorder, anxiety and depression symptoms in Haitian immigrants [16]. In summary, international evidence suggests that discrimination, as a social stressor, leads to mental health problems in migrant population. This association must be understood in a complex multifactorial context, even more in Latin-America [1, 9, 12].
The association between perceived discrimination and mental health problems could be influenced by different mechanisms, including social, psychological, and biological dimensions. First, discrimination has been identified as a post-migration stressor that negatively affects social integration and poor social integration contributes to a higher rate of inequality in mental health disorders [36, 37]. Secondly, acculturation stress increases mental health problems in immigrants and discrimination is an essential contributor to this problem [3, 38, 39]. Again, self-esteem has been recognized as an essential mediator over the effect of perceived discrimination on depression, anxiety and psychological wellbeing in migrants [5, 40]. Moreover, perceived discrimination has a direct effect on physical and mental health. Additionally, it indirectly affects stress response levels and health behaviors, conditioned by social support, stigma, and coping style [41]. Moreover, discrimination induced cortisol dysregulation, especially in immigrants and other racial/ethnic minorities [42, 43]. This psychobiological stress interacts with dopamine, serotonin and other neurotransmitters produce anxious and depressive symptoms [44]. Therefore, discrimination can lead to mental health problems via an intricate network of interrelated mechanisms.
Implications of our findings to policy and practice
The “Venezuelan phenomenon” is complex and challenging. The humanitarian crisis has naturally caused a massive migratory exodus, with varying degrees of receptiveness to immigrants in different countries of the region [32]. According to international evidence available, international migration directly impacts health outcomes in a population and, in turn, on public health policy decisions in each locality [3]. This process has essential repercussions in Venezuela and neighboring receiving countries, affecting several areas: health, education, labor and others [31,32,33]. Discrimination has been recognized as a problem that the migrant population in different latitudes must deal with [4, 45]. Furthermore, deterioration in mental health is a severe issue among migrant populations [11,12,13]. Hence, discrimination and mental health are essential trace markers of the humanitarian crisis and constitute indicators of a complex interaction between strategies implemented by receiving countries, the reaction of the host society and the immigrants’ response.
Approximately one million Venezuelan migrants live in Peru, 88.8% are formal residents or regularization processes for resident status. Most of them constitute an essential flow of human resources (with a high proportion of them with a higher education level) that have been reinserted into the Peruvian labor force (mainly at technical and manual activities) [7]. Among migrant populations, integration strategies could improve their mental health while increasing the acceptability of diversity, reducing discrimination towards immigrants, thereby contributing to better mental health [35, 46]. Community-level interventions providing immigrants opportunities to increase social networking among members of the same country and those native-born in a host country may be helpful resources for improving mental health among immigrants [21, 47]. It is plausible that one who has a better understanding of the host culture might have inspired opportunities to participate in social activities with host country members, leading to an improved sense of belonging, which are significant predictors of better mental health. All these considerations should be taken by health and social authorities at the national level in countries such as Peru, which are receiving large influxes of migrants, especially from Venezuela.
Limitations and strengths
Our study has several limitations. First, both mental health problems and perceived discrimination are self-reported, so selection and recall bias may affect outcomes reporting. Although there is controversy about measuring discrimination experiences, self-report is one valid way [48]. Second, we included in our analysis only factors identified in the ENPOVE-2018 survey. Other factors influence the association between perceived discrimination and mental health problems that we have not considered. Third, we do not have information about Venezuelans’ mental health problems before they arrived in Peru. Finally, with a cross-sectional survey, we cannot establish a causal effect of discrimination on mental health problems. Despite this, the main strengths of our study are that it is based on an urban nationally representative survey, and, to best of our knowledge, it is the first study that assesses the association between perceived discrimination and mental health problems in Venezuelan immigrants to Peru. Our findings are valuable for policymakers, public health and global health practitioners, as well as health professionals, given the structural and historical challenges of the Peruvian health system.
Conclusions
There is evidence that perceived discrimination is associated with the deterioration of mental health in Venezuelan migrants living in Peru, a complex and under-researched topic. Research related to this problem constitutes a highly relevant tool for health and healthcare decision-making in Latin American countries. Study findings support the call for the urgent health protection of Venezuelan migrants in Peru. This population reports high degrees of self-perceived discrimination and is struggling to maintain their mental health. Future research should continue developing this topic, mainly through a more profound understanding of mental health needs and protective strategies for Venezuelan immigrants, using longitudinal approaches to achieve more robust estimates and understanding of underlying causal mechanisms.
Availability of data and materials
Our study used information from the public domain (http://iinei.inei.gob.pe/microdatos/).
Abbreviations
- ENPOVE:
-
Venezuelan Population Residing in Peru Survey
- CI:
-
Confidence intervals
- cOR:
-
Crude odds ratios
- aOR:
-
Adjusted odds ratios
- PSM:
-
Propensity Score Matching
References
Cabieses B, Bernales M, van der Laat C. Health for all migrants in Latin America and the Caribbean. Lancet Psychiatry. 2016;3:402.
Wickramage K, Vearey J, Zwi AB, Robinson C, Knipper M. Migration and health: a global public health research priority. BMC Public Health BioMed Central. 2018;18:1–9.
Cabieses B. La compleja relación entre posición socioeconómica, estatus migratorio y resultados de salud. Value Health Reg Issues. 2014;5:1–6.
Choi DD, Poertner M, Sambanis N. Parochialism, social norms, and discrimination against immigrants. Proc Natl Acad Sci U S A. 2019;116:16274–9.
Urzúa A, Cabrera C, Carvajal CC, Caqueo-Urízar A. The mediating role of self-esteem on the relationship between perceived discrimination and mental health in south American immigrants in Chile. Psychiatry Res. 2019;271:187–94.
Carroll H, Luzes M, Freier LF, Bird MD. The migration journey and mental health: evidence from Venezuelan forced migration. SSM-Popul Health. 2020;10:100551.
Mendoza W, Miranda JJ. La inmigración venezolana en el Perú: desafíos y oportunidades desde la perspectiva de la salud. Rev Peru Med Exp Salud Pública. 2019;36:497–503.
Sánchez Aguilar A. Migraciones Internas en el Perú [Internet]. Organización Internacional para las Migraciones - OIM Lima; 2017 [cited 2019 Sep 6]. Available from: http://repository.oim.org.co/handle/20.500.11788/1490.
Alegría M, Álvarez K, DiMarzio K. Immigration and mental health. Curr Epidemiol Rep. 2017;4:145–55.
Meyer SR, Lasater M, Tol WA. Migration and mental health in low- and middle-income countries: a systematic review. Psychiatry. 2017;80:374–81.
Heeren M, Wittmann L, Ehlert U, Schnyder U, Maier T, Müller J. Psychopathology and resident status - comparing asylum seekers, refugees, illegal migrants, labor migrants, and residents. Compr Psychiatry. 2014;55:818–25.
Hynie M. The social determinants of refugee mental health in the post-migration context: a critical review. Can J Psychiatry Rev Can Psychiatr. 2018;63:297–303.
Lindert J, von Ehrenstein OS, Priebe S, Mielck A, Brähler E. Depression and anxiety in labor migrants and refugees–a systematic review and meta-analysis. Soc Sci Med. 2009;69:246–57.
Abubakar I, Aldridge RW, Devakumar D, Orcutt M, Burns R, Barreto ML, et al. The UCL-Lancet Commission on migration and health: the health of a world on the move. Lancet Lond Engl. 2018;392:2606–54.
Cabieses B, Tunstall H, Pickett KE, Gideon J, et al. Int J Equity Health. 2012;11:68.
Brunnet AE, Bolaséll LT, Weber JL, Kristensen CH. Prevalence and factors associated with PTSD, anxiety and depression symptoms in Haitian migrants in southern Brazil. Int J Soc Psychiatry. 2018;64:17–25.
Gkiouleka A, Avrami L, Kostaki A, Huijts T, Eikemo TA, Stathopoulou T. Depressive symptoms among migrants and non-migrants in Europe: documenting and explaining inequalities in times of socio-economic instability. Eur J Pub Health. 2018;28:54–60.
Hatch SL, Gazard B, Williams DR, Frissa S, Goodwin L, Hotopf M. Discrimination and common mental disorder among migrant and ethnic groups: findings from a South East London community sample. Soc Psychiatry Psychiatr Epidemiol. 2016;51:689–701.
Keys HM, Kaiser BN, Foster JW, Burgos Minaya RY, Kohrt BA. Perceived discrimination, humiliation, and mental health: a mixed-methods study among Haitian migrants in the Dominican Republic. Ethn Health. 2015;20:219–40.
Mewes R, Asbrock F, Laskawi J. Perceived discrimination and impaired mental health in Turkish immigrants and their descendents in Germany. Compr Psychiatry. 2015;62:42–50.
Ra CK, Huh J, Finch BK, Cho Y. The impact of perceived discrimination on depressive symptoms and the role of differentiated social support among immigrant populations in South Korea. Int J Equity Health. 2019;18:7.
StataCorp. Stata 15 Survey Reference Manual [Internet]. College Station, TX: Stata Press; 2017. Available from: https://www.stata.com/manuals/svy.pdf.
Rothman KJ, Greenland S, Lash TL. Modern Epidemiology. 3rd ed. Philadelphia, PA, USA: Lippincott Williams and Wilkins; 2008.
Caliendo M, Kopeinig S. Some practical guidance for the implementation of propensity score matching. J Econ Surv. 2008;22:31–72.
Dehejia RH, Wahba S. Propensity score-matching methods for nonexperimental causal studies. Rev Econ Stat. 2002;84:151–61.
Becker SO, Ichino A. Estimation of average treatment effects based on propensity scores. Stata J. 2002;2:358–77.
Heckman JJ, Ichimura H, Todd PE. Matching as an econometric evaluation estimator: evidence from evaluating a job training programme. Rev Econ Stud. 1997;64:605–54.
Smith JA, Todd PE. Does matching overcome LaLonde’s critique of nonexperimental estimators? J Econom. 2005;125:305–53.
Wild V, Dawson A. Migration: a core public health ethics issue. Public Health. 2018;158:66–70.
Larenas D, Cabieses B. Acceso a salud de la población migrante internacional en situación irregular: La respuesta del sector salud en Chile. Cuad Méd Soc. 2018;58:97–108.
Page KR, Doocy S, Reyna Ganteaume F, Castro JS, Spiegel P, Beyrer C. Venezuela’s public health crisis: a regional emergency. Lancet Lond Engl. 2019;393:1254–60.
Shepherd A. Crisis in Venezuela. BMJ. 2019;364:l1277.
Rodríguez-Morales AJ, Suárez JA, Risquez A, Cimerman S, Valero-Cedeño N, Cabrera M, et al. In the eye of the storm: infectious disease challenges for border countries receiving Venezuelan migrants. Travel Med Infect Dis. 2019;30:4–6.
Schmitt MT, Branscombe NR, Postmes T, Garcia A. The consequences of perceived discrimination for psychological well-being: a meta-analytic review. Psychol Bull. 2014;140:921–48.
Straiton ML, Aambø AK, Johansen R. Perceived discrimination, health and mental health among immigrants in Norway: the role of moderating factors. BMC Public Health. 2019;19:325.
Chen W, Wu S, Ling L, Renzaho AMN. Impacts of social integration and loneliness on mental health of humanitarian migrants in Australia: evidence from a longitudinal study. Aust N Z J Public Health. 2019;43:46–55.
Brydsten A, Rostila M, Dunlavy A. Social integration and mental health - a decomposition approach to mental health inequalities between the foreign-born and native-born in Sweden. Int J Equity Health. 2019;18:48.
Urzúa MA, Heredia BO, Caqueo-Urízar A. Mental health and stress by acculturation in immigrants from South America in northern Chile. Rev Med Chil. 2016;144:563–70.
Revollo H-W, Qureshi A, Collazos F, Valero S, Casas M. Acculturative stress as a risk factor of depression and anxiety in the Latin American immigrant population. Int Rev Psychiatry Abingdon Engl. 2011;23:84–92.
Urzúa A, Ferrer R, Godoy N, Leppes F, Trujillo C, Osorio C, et al. The mediating effect of self-esteem on the relationship between perceived discrimination and psychological well-being in immigrants. PLoS One. 2018;13:e0198413.
Pascoe EA, Smart RL. Perceived discrimination and health: a meta-analytic review. Psychol Bull. 2009;135:531–54.
Mewes R, Reich H, Skoluda N, Seele F, Nater UM. Elevated hair cortisol concentrations in recently fled asylum seekers in comparison to permanently settled immigrants and non-immigrants. Transl Psychiatry. 2017;7:e1051.
Zeiders KH, Hoyt LT, Adam EK. Associations between self-reported discrimination and diurnal cortisol rhythms among young adults: the moderating role of racial-ethnic minority status. Psychoneuroendocrinology. 2014;50:280–8.
Firk C, Markus CR. Review: serotonin by stress interaction: a susceptibility factor for the development of depression? J Psychopharmacol Oxf Engl. 2007;21:538–44.
Tahzib F, Davidovitch N, Labonte R. Migration, justice and health: reimagining the earth as one country and humankind its citizens. Public Health. 2019;172:105–7.
Shields-Zeeman L, Lewis C, Gottlieb L. Social and Mental Health Care Integration: The Leading Edge. JAMA Psychiatry. 2019;76:881–2.
Terry R, Townley G. Exploring the role of social support in promoting community integration: an integrated literature review. Am J Community Psychol. 2019;64:509–27.
Lewis TT, Cogburn CD, Williams DR. Self-reported experiences of discrimination and health: scientific advances, ongoing controversies, and emerging issues. Annu Rev Clin Psychol. 2015;11:407–40.
Acknowledgments
We are grateful to Karen Carpio for helpful comments and suggestions on draft versions of the paper.
Funding
The authors received no financial support for this study.
Author information
Authors and Affiliations
Contributions
EA, BM and BC initiated the research concept and wrote the draft manuscript. EMH, EA and BM analyzed the data, presented and interpreted results. EMH, AFM and BC presented the discussion and then reviewed and finalized the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: A1 Table.
Characteristics of the non-included sample. A2 Table. Unadjusted models for control variables.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mougenot, B., Amaya, E., Mezones-Holguin, E. et al. Immigration, perceived discrimination and mental health: evidence from Venezuelan population living in Peru. Global Health 17, 8 (2021). https://doi.org/10.1186/s12992-020-00655-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12992-020-00655-3