
Abstract
Introduction
Mental distress is a mental health problem which includes anxiety, depression and somatic symptoms. Mental health problems affect society as a whole and no group is immune to mental disorders; however, students have significantly high level of mental distress than their community peers.
Objective
The aim of the study is to assess magnitude of mental distress and its predictors among undergraduate health science students of Hawassa University, College of Medicine and Health Sciences, SNNPR, Ethiopia.
Methods
Institution-based cross-sectional study was conducted among 311 students. Simple random sampling technique was used to select the study participants. Data were collected using pre-tested and structured self-administered questionnaire. Mental distress among students was assessed using SRQ-20, which is validated in Ethiopia. Bivariate and multivariate logistic regression model was fitted to identify predictors of mental distress among students. An adjusted odds ratio with 95% confidence interval was computed to determine the level of significance with P-value less than 0.05.
Result
A total of 309 study participants were interviewed with a response rate of 99.34%. Among the total respondents 105 (34%) of them were found to have mental distress. In multiple logistic regression analysis, poor social support (AOR = 5.28; 95% CI (2.176–12.84) and current substances use (AOR = 12.83, 95% CI (7.13–23.13), were significant predictors of mental distress among respondents.
Conclusion and recommendations
The overall magnitude of mental distress among students was found to be high. Therefore, it is recommended that mental distress needs due attention and remedial action from policy-makers, college officials, non-governmental organizations, parents, students and other concerned bodies.
Similar content being viewed by others

Introduction
Mental distress is a mental health problem which includes anxiety, depression and somatic symptoms [1]. Currently mental distress is a major public mental health problem and a leading cause of disability worldwide, accounting for one-third of disability adjusted life years [2]. In Africa mental illness particularly, mental distress is an important public health challenge that is under-recognized as a public problem [3].
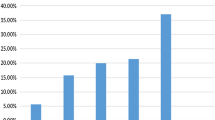
Studies conducted among undergraduate students in Canada showed that 30% of students had mental distress which was significantly higher than adults in the general population of Canada [4]. Also more than half of students in USA [5] and 53% of students in Australia had mental distress [6].
A study conducted in South Africa, Malaysia, Kenya and Ethiopia revealed the prevalence of common mental disorders among college students is 27% [3], 41.9% [7], 10.8% [8] and 21.6% [9], respectively.
In Ethiopia, mental distress accounts for 11% of the total burden of diseases [10]. Although mental health problems affect all society and no group is immune to psychiatric disorders, students have significantly high level of psychological distress than their community peers [11].
This is due to the fact that university students face multiple stressors such as academic load, constant pressure to succeed, competition with peers, financial problems, peer pressure, teacher or parental pressure as well as concerns about the future [12]. This can have negative effects on student’s ability to study and academic outcomes [13]. If not properly managed, such situation of stress may later lead students to develop mental distress [14].
Another study conducted in Ethiopia revealed that 32.6% of medical students experienced mental distress [15]. However, since this study was done only on medical students and with small sample size, it may not represent all university students in Ethiopia.
A cross-sectional study conducted in University of Gondar the prevalence of mental distress was 40.9% [16]. In a study conducted in Haramaya University, the prevalence of mental distress was found 19.3% [17] and in Hawassa University among medical students the prevalence was 30% [18]. Due to the fact that there were few published literatures regarding the issue in our country, especially among health science students, this study was conducted with the aim of serving as a baseline for further study and to recommend the concerned bodies to intervene on this target group of population.
Method
Study design and period
Institution-based cross-sectional study design was conducted to assess the magnitude of mental distress and its predictors among undergraduate health science students of Hawassa University, College of Medicine and Health Sciences, Hawassa City, SNNPR, Ethiopia, from January 29 to February 14/2017 GC which was exam-free period.
This study was conducted in Hawassa University College of Medicine and Health Sciences, undergraduate health science students in Hawassa located 275 km from Addis Ababa. The college is one of the eight colleges under Hawassa University. The college is established to teach medical, nursing, midwifery, public, environmental health, psychiatric nursing, optometry, anesthesiology, laboratory and radiology students. In the academic year 2016/2017 the college had enrolled a total of 1570 health science students.
Sample size determination and sampling procedures
The participants of this study were undergraduate health science students enrolled in the year 2016/2017 and attending classes in regular program under College of Medicine and Health Science.
Students were stratified based on the year of study. Since there was no study done among health science students, sample size was calculated by assuming the prevalence of mental distress 50%, 95% confidence interval and 5% margin of error. Considering the total population (N = 1170 health science students) correction formula was used and adding 10% for non-response the final sample size was 309. Simple random sampling technique was used to select the 309 study subjects to be included in the study.
Data collection instrument
Data were collected using self-administered technique. The English version of the first part of the tool contains socio-demographic characteristics of students. The second part of the questionnaire asks about behavioral factors, which includes history of substance use (alcohol use, chat chewing and cigarette smoking) of students and the third part of the questionnaire assesses about social support of students using 3-item Oslo Social Support Scale. The fourth part of the questionnaire is self-reporting questionnaire (referred to as SRQ-20). Self-reporting questionnaire was used to estimate the prevalence of mental distress among health science students. This self-reporting questionnaire is a standardized questionnaire having 20-item questions, originally developed by World Health Organization (WHO) designed to indicate mental distress. The tool is adopted from WHO and was validated in low- and middle-income countries including Ethiopia. Students who were found to have 8 or more symptoms of the 20-item self-reporting questionnaires (SRQ-20) in the last 4 weeks were considered as having mental distress. The cut-off point was used based on the reports from the validation study of SRQ-20 that gave the highest sensitivity and specificity which corresponds to a cut-off point of 7 [19].
Social support of the study participants was assessed using 12-item Multidimensional Scale of Perceived Social Support Tool [20]. The items are divided in to factor groups relating to the source of social support, namely family, friends and significant others. Each item is scored from one (very strongly disagree) to 7 (very strongly agree). The total sum of all the 12 items possibly ranges from 12 to 84. A score 69–84 considered as high level of social support, whereas a score of 49–68 and 12–48 were considered as moderate and low level of social support, respectively. The reliability of the tool was checked using Cronbach's alpha reliability test with a score of 0.82 (95% CI 0.801–0.837).
Pre-test was conducted on 5% of sample size in Dilla University to ensure the reliability of the tool with Cronbach's α = 0.79. The collected data were reviewed and checked for completeness by group members on each day.
Data processing and analysis
After the collected data were reviewed and checked for completeness before data entry, the incomplete data were discarded (questionnaires were incomplete). Data were cleaned, edited, coded and entered into Epi-info version 3.5.1 and exported in to SPSS version 20 software for analysis and we used both descriptive and analytical statistical procedures. Descriptive statistics like percentage mean and standard deviation was used for the presentation of demographic data and magnitude of mental distress. Tables were also used for data presentation. Each independent variable against the dependent variable was tested for having statistical significant association using binary logistic regression. Multiple logistic regression analysis was done for those variables with P-value less than or equal to 0.2 during binary logistic regression analysis.
Ethical consideration
Ethical clearance was obtained from the institutional review board (IRB) of Hawassa University. Ethical review board approved the methods of data collection and forms of consent. Each questionnaire was prepared with the written consent attached with it to offer the consent for the respondents verbally and participants willing to be interviewed had signed and finally the obtained consents were kept with the questionnaire. The respondents were informed that their inclusion in the study is voluntary and they are free to withdraw from the study if they are not willing to participate. Anonymity was maintained to ensure confidentiality.
Result
Socio-demographic characteristics of study participants
A total of 309 other health science students were assessed, of which 193 (62.5%) were males and 115 (37.2%) of them were second year students. Respondents’ age ranged from 18 to 35 years, with a mean (± SD) of 22.2 (± 2.48) years. The higher percentages of the respondents were from urban background 208 (67.3%). Majority of the participants 130 (42.1%) were followers of Orthodox religion (Table 1).
Social support of respondents
In the assessment of social support using 3-item Oslo Social Support Scale (OSS-3), out of 309 students, more than half of the respondents 231 (74.7%) had strong social support and the rest 78 (25.2%) had poor social support.
Magnitude of mental distress
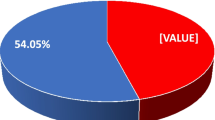
Magnitude of mental distress using SRQ-20, with a cut-off point of 7 and above was 34% (95% CI 32.3, 35.7) (105 students out of 309 students). The distribution of SRQ-20 showed a mean value of 5.27 (± 4.31) ranging from 0 to 20.
Factors associated with mental distress
During multiple logistic regression analysis, poor social support (AOR = 5.28; 95% CI (2.176–12.84), and current substances use (AOR = 12.84, 95% CI (7.13–23.13), were significant predictors of mental distress among students (Table 2).
Discussion
The magnitude of mental distress among students in this study was found to be 34%. The finding in the current study is lower compared to studies in USA (57%) [5], Australia (53%) [6], Brazil (44.7%) [21], Gondar (40.9) [16]. The variation might be due to the socio-cultural, environmental factors. Also time variation, the improvement of infrastructure and a service option provided by school authorities from time to time could be the reason for the variation.
However, the magnitude in the current study was higher when compared with studies in France (25.7%) [13], Norway (22.9%) [22] and Iceland (22.5%) [23] and Australia (19.2%). This could be due to the different instrument used in other studies or it could be a real difference. However, nearly similar prevalence was reported in Ethiopia revealed that 32.6% of medical students experienced mental distress [15].
Substance use was found to be a strong predictor of mental distress (AOR = 12.84, 95% CI (7.13–23.13), the odds of students who ever use substance were 12.8 times more likely to have mental distress as compared to the odds of students who never use substance. This finding is in line with other studies in Ethiopia [9] and Sao Paulo, Southeastern Brazil [24]. This might be because, substance use leads to inefficiency in life function, impaired relationship and sleep deprivation. Furthermore, substance use is associated with increased absenteeism from class and poor academic performance which can further lead to mental distress in students.
In this study, social support was also found to be another determinant factor for mental distress in students (AOR = 5.28; 95% CI (2.176–12.835). Having low level of social support from significant others were positively associated with mental distress. In this study, the odds of students with low social support were 5.3 times more likely to have mental distress as compared to those students with good social support. This finding is also in line with study conducted in Norwegian [22]. This could be due to its effect on hypothalamic pituitary adrenocortical (HPA) system in reducing genetic and environmental vulnerabilities. Furthermore, it is also important for maintaining good physical and mental health [25].
Conclusion and recommendation
The prevalence of mental distress among students was found to be high. Having low social support and ever use of substance were strong predictors of mental distress.
Therefore, it is recommended that mental distress needs due attention and remedial action from policy-makers, college officials, non-governmental organizations, parents, students and other concerned bodies. Programs aimed at preventing mental distress need to address these identified factors of mental distress against students.
Limitation
The cross-sectional nature of the study design does not confirm definitive cause-and-effect relationship. Also, the study may be prone to reporting bias since the data were collected based on self-reported information.
Availability of data and materials
All analyzed and generated data are included in this article and its supporting document.
References
Giang KB, Dzung TV, Kullgren G, Allebeck P. Prevalence of mental distress and use of health services in a rural district in Vietnam. Glob Health Action. 2010;15:3. https://doi.org/10.3402/gha.v3i0.2025.
World Health Organizations. The global burden of disease. Geneva: World Health Organizations; 2008.
Havenaar JM, Geerlings MI, Vivian L, Collinson M, Robertson B. Common mental health problems in historically disadvantaged urban and rural communities in South Africa: prevalence and risk factors. Soc Psychiatry Psychiatr Epidemiol. 2007;7(1007):294–9. https://doi.org/10.1007/s00127-007-0294-9.
Adlaf EM, Gliksman L, Demers A. The prevalence of elevated psychological distress among Canadian undergraduates. J Am College Health. 2007;50:67–72. https://doi.org/10.1080/07448480109596009.
Mosley TH, Perrin SG, Neral SM, Dubbert PM. Stress, coping, and well-being among third-year medical students. Acad Med. 2008;69(9):765–7. https://doi.org/10.1097/00001888-199409000-00024.
Stallman HM. Prevalence of psychological distress in university students—implications for service delivery. AustFam Physician. 2008;37(8):673–7.
MohdSidik S, Rampal L, Kaneson N. Prevalence of emotional disorders among medical students in a Malaysian university. Asia Pacific Fam Med. 2008;2(4):213–7. https://doi.org/10.1111/j.1444-1683.2003.00089.x.
Jenkins R, Njenga F, Okonji M, Kigamwa P, Baraza M, Ayuyo J, et al. Prevalence of common mental disorders in a rural district of Kenya, and socio-demographic risk factors. Int J Environ Res Public Health. 2012;9:1810–9. https://doi.org/10.3390/ijerph9051810.
Dessie Y, Ebrahim J, Awoke T. Mental distress among university students in Ethiopia: a cross sectional survey. Pan Afr Med J. 2013;15:95. https://doi.org/10.11604/pamj.2013.15.95.2173.
Abdulahi H, Haile Mariam D, Kebede D. Burden of disease analysis in rural Ethiopia. Ethiop Med J. 2001;39(4):271–81.
Cvetkovski S, Reavley NJ, Jorm AF. The prevalence and correlates of psychological distress in Australian tertiary students compared to their community peers. Aust N Z J Psychiatry. 2012;46(5):457–67.
Sreeramareddy CT, Shankar OR, Binu VS, Mujhopadhyay C, Ray B, Menezes RG. Psychological morbidity sources of stress and coping strategies among undergraduate medical students in Nepal. BMC Med Educ. 2007;7:26. https://doi.org/10.1186/1472-6920-7-26.
Verger P, Gilbert F, KovessMasfety V. Psychiatric disorders in students in six French universities: 12-month prevalence, comorbidity, impairment and help-seeking. Soc Psychiatry Psychiatr Epidemiol. 2010;45:189–99. https://doi.org/10.1007/s00127-009-0055-z.
Tyseen R, Vaglum P, Gronvold NT, Ekeberg O. Factors in medical school that predict postgraduate mental health problems in need of treatment a nationwide and longitudinal study. Med Educ. 2010;35:110–20. https://doi.org/10.1046/j.1365-2923.2001.00770.x.
Alem A, Araya M, Melaku Z, Wendimagegn D, Abdulahi A. Mental distress in medical students of Addis Ababa University. Ethiop Med J. 2005;43(3):159–66.
Berihun AD, Telake AB, Resom BG. Prevalence of mental distress and associated factors among undergraduate students of University of Gondar, northwest Ethiopia: a cross-sectional institutional based study. PLoS ONE. 2015;10(3):e0119464.
Alemayaw G. Assessment of prevalence, determinants and effects of mental distress among Alemaya University students. Addis Ababa: Addis Ababa University; 2005.
Biniam M, Birahanu B. Prevalence of mental distress and associated factors among Hawassa university medical students, southern Ethiopia: a cross sectional study. BMC Res Notes. 2016;9(1):485.
World Health Organization, Division of Mental Health, A user's guide to self-reporting questionnaire (SRQ), 1994. https://apps.who.int/iris/handle/10665/61113.
Zimet GD, Powell SS, Farley GK, Werkman S, Berkoff KA. Psychometric characteristics of the multidimensional scale of perceived social support. J Personality Assessment. 1990;55:610–7.
Lima MC, Domingues MD, Cerqueria AT, Abreu RC. Prevalence and risk factors of common mental disorders among medical students. Rev SaúdePública. 2006;40(6):1035–41.
Nerdrum P, Rustøen T, Rønnestad M. Student psychological distress: a psychometric study of 1750 Norwegian 1st-year undergraduate students. Scandinavian J Edu Res. 2006;50:95–109.
Bernhardsdottir J, Vilhjalmsson R. Psychological distress among university female students and their need for mental health services. J Psychiatr Ment Health Nurs. 2013;20(8):672–8.
Gallagher RP. National survey of counseling center directors. Monograph the International Association of Counseling Services. 2010.
Ozbay F, Johnson DC, Dimoulas E, Morgan CA, Charney D, Southwick S. Social support and resilience to stress: from neurobiology to clinical practice. Psychiatry (Edgmont (Pa: Township)). 2007;4(5):35–40.
Acknowledgements
We would like to acknowledge study participants for devoting their time and providing us important information during data collection.
Funding
No funding was received for this research work.
Author information
Authors and Affiliations
Contributions
AB and BD participated in the conception, design of the study, reviewing proposal and data analysis. AB, BD and TY participated in reviewing and writing the report. AB prepared the manuscript for publication. TY and BD have participated in supervising the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bedaso, A., Duko, B. & Yeneabat, T. Predictors of mental distress among undergraduate health science students of Hawassa University, College of Medicine and Health Sciences, Hawassa, SNNPR, Ethiopia: a cross-sectional study. Ann Gen Psychiatry 19, 6 (2020). https://doi.org/10.1186/s12991-020-0258-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12991-020-0258-y