
Abstract
Background
The causative agents of diarrhea, rotavirus B (RVB) and rotavirus C (RVC) are common in adults and patients of all age groups, respectively. Due to the Rotavirus A (RVA) vaccination program, a significant decrease in the number of gastroenteritis cases has been observed globally. The replacement of RVA infections with RVB, RVC, or other related serogroups is suspected due to the possibility of reducing natural selective constraints due to RVA infections. The data available on RVB and RVC incidence are scant due to the lack of cheap and rapid commercial diagnostic assays and the focus on RVA infections. The present study aimed to develop real-time RT‒PCR assays using the data from all genomic RNA segments of human RVB and RVC strains available in the Gene Bank.
Results
Among the 11 gene segments, NSP3 and NSP5 of RVB and the VP6 gene of RVC were found to be suitable for real-time RT‒PCR (qRT‒PCR) assays. Fecal specimens collected from diarrheal patients were tested simultaneously for the presence of RVB (n = 192) and RVC (n = 188) using the respective conventional RT‒PCR and newly developed qRT‒PCR assays. All RVB- and RVC-positive specimens were reactive in their respective qRT‒PCR assays and had Ct values ranging between 23.69 and 41.97 and 11.49 and 36.05, respectively. All known positive and negative specimens for other viral agents were nonreactive, and comparative analysis showed 100% concordance with conventional RT‒PCR assays.
Conclusions
The suitability of the NSP5 gene of RVB and the VP6 gene of RVC was verified via qRT‒PCR assays, which showed 100% sensitivity and specificity. The rapid qRT‒PCR assays developed will be useful diagnostic tools, especially during diarrheal outbreaks for testing non-RVA rotaviral agents and reducing the unnecessary use of antibiotics.
Similar content being viewed by others

Introduction
Diarrhea is a global health problem associated with approximately 1.7 to 5 billion cases per year and 19.11% of deaths from diarrhea in 2019 [1,2,3]. Despite improvements in general sanitation, hygiene, diarrheal treatments, and the use of rotavirus A (RVA) vaccines, diarrhea is a main contributor to childhood mortality, especially in lower- and medium-income countries [4]. A significant decrease in pediatric gastroenteritis cases after RVA vaccination was suspected to reduce natural selective constraints, and replace RVA infections with rotavirus B (RVB), rotavirus C (RVC), or other related serogroups [5]. Recently, dehydration, age, sex-specific vulnerabilities, and causes of diarrhea other than RVA were demonstrated to be important risk factors for childhood diarrheal mortality [4]. Among the non-RVA Rota viral agents, RVB, RVC, and other enteric viruses, namely, noroviruses, adenoviruses, and astroviruses, are the main causative agents.
RVB is known to infect humans and porcine, bovine, murine, and caprine animal species [6,7,8,9,10]. RVB infection with severe watery, cholera-like diarrhea has been documented in large diarrheal epidemics in China, India, Bangladesh, Myanmar, and Nepal [5, 9, 11,12,13,14,15]. The limited studies documented to date have shown the dominance of RVB infections in adults/adolescents, especially in outbreak cases. The occurrence of RVB in diarrheal outbreaks in children [16] and sporadic cases has also been documented [12, 17, 18].
RVC infections are widespread and enzootic in porcine species [19]. The etiological role of human RVC strains has been documented in a small number of sporadic and outbreak cases among all age groups [20,21,22].
To date, data on diarrhea incidence and etiologies among populations older than five years are scarce [1]. There was a 50% increase in the number of adults older than 70 years (from 1990 to 2016), and nearly three-quarters of diarrhea deaths occurred in individuals older than five years, with a particularly high burden in adults older than 70 years [1]. Identification of diarrhea as a major public health problem among adults/adolescents as well as older individuals highlights the need for studies on diarrheal etiology [1, 23].
On the basis of the scarcity of studies on RVB/RVC, investigations of diarrhea patients in all age groups from different geographical regions are necessary to determine the exact prevalence rate and circulation pattern of these diseases in the human population. To correctly diagnose disease and enable successful prevention and control actions, accurate pathogen identification is essential. Probe-based real-time RT‒PCR (qRT‒PCR) assays, which are known for minimal chances of cross-contamination, are highly sensitive, specific, quick, and useful for quantitative estimation of the viral genome. By adding different fluorophores for each probe, multiplex assays can also be developed for the simultaneous detection of different targets. This study focused on the development of qRT‒PCR assays for the detection of RVB and RVC infections among diarrheal patients.
Materials and methods
Designing primers and probes
The suitability of the 11 genes for the detection of RVB and RVC was determined by using nucleotide sequence data retrieved from GenBank (www.ncbi.nlm.nih.gov). Multiple nucleotide sequences obtained were aligned with CLUSTAL W utilizing 24, 26, 23, 44, 32, 63, 23, 92, 23, 32, and 22 sequences (complete or partial) of the VP1, VP2, VP3, VP4, VP6, VP7, NSP1, NSP2, NSP3, NSP4 and NSP5 genes of RVB strains, respectively [24]. The nucleotide sequence data consisted of 119, 60, 84, 37, 38, 37, 39, 40, 39, 56, and 38 strains for the VP7, VP4, VP6, VP1, VP2, VP3, NSP1, NSP2, NSP3, NSP4 and NSP5 genes of human RVC strains, respectively. Primers and probes were designed and finalized using the Primer Quest tool from IDT (https://www.idtdna.com/pages/tools/primerquest) and modified manually. All sets of primers and probes used were examined for self-annealing sites, hairpin loop formation, 3’ complementarities, and melting temperatures (Tm) using the IDT oligonucleotide calculator tool (http://www.idtdna.com/analyzer/Applications/OligoAnalyzer).
Preparation of the reference RNA standard
A portion of the NSP5 gene (608 bp) of the RVB strain was amplified using the primers RVB_NSP5F (TAA TAC GAC TCA CTA TAG GGA GAG TCAGTAGACGGCTGGAAACGTTG) and RVB_NSP5R (TAA TAC GAC TCA CTA TAG GGA GAG AATATAACTCAAGAGGTTRACCC), with the T7 promoter sequence at the 5’ end of both primers. Similarly, the VP6 gene of RVC (1335 bp) was amplified using the primers RVC_VP6F [TAA TAC GAC TCA CTA TAG GGA GAG CTCATTCACAATGGATGTACTTTTTTC (13–39)] and RVC_VP6R [TAA TAC GAC TCA CTA TAG GGA GAG CATAGTTCACATTTCATCCTTCTGGGGA (1348–1321)]. The amplification of the respective PCR products was confirmed by agarose gel electrophoresis. Amplicons were cleaned by using a Qiagen direct PCR purification kit (Cat No- 28,104 Qiagen, Hilden, Germany). In vitro, transcribed (IVT) RNA was synthesized using a T7 Riboprobe® System (Cat No: P1440; Promega, USA) according to the manufacturer's instructions. The concentration of synthetic fragments of transcribed RNA was measured by fluorometric analysis (Qubit, Thermo Scientific). A standard curve was generated by plotting the log dilution of the RNA transcripts against the Ct value to determine the sensitivity of the assays. The copy number (RNA concentration) was calculated by using the equation Copy number (molecules/µL) = [concentration (ng/µL) × 6.022 × 1023 (molecules/mol)]/[length of amplicon X 340 (g/mol) × 109 (ng/g)], as described earlier [25]. To determine the viral loads of RVB and RVC in the fecal specimens, serial tenfold dilutions of RNA transcripts were prepared and used as standards in the assay runs.
Specimens
Fecal specimens (n = 192) collected from Maharashtra, India, were shortlisted for validation of the RVB qRT‒PCR assay. The panel consisted of known positive specimens for RVB (n = 31), RVA (n = 45), norovirus (n = 12), adenovirus (n = 15), astrovirus (n = 9), and enterovirus (n = 5), and negative specimens for all viral agents (n = 75) according to methods described previously [15, 26,27,28,29,30]. Similarly, a qRT‒PCR assay for RVC was performed on fecal specimens (n = 188) that were positive for RVC (n = 8), porcine RVC (n = 16), RVA (n = 45), RVB (n = 5), norovirus (n = 12), adenovirus (n = 15), astrovirus (n = 9), and enterovirus (n = 5) and negative for all viral agents (n = 73).
RNA extraction, Conventional RT‒PCR and qRT‒PCR assays
The supernatant of 30% of the fecal suspensions was subjected to RNA extraction using the automated MagMAX Viral/Pathogen Nucleic Acid Isolation Kit (Applied Biosystems, USA) according to the manufacturer’s instructions. Conventional RT‒PCR assays for RVB/RVC detection were used as the gold standard and were carried out as described earlier [15, 22].
The qRT‒PCR assays were carried out using the primers and probes described in Table 1. Briefly, the qRT‒PCR mixture consisted of Invitrogen™ SuperScript™ III Platinum™ One-Step qRT‒PCR master mix (17 µl) (Applied Biosystems, Foster City, CA, USA) containing 0.5 µl of each of the forward and reverse primers as well as the probe (10 µM concentration each) and 8 µl of RNA. The thermal cycling procedure consisted of denaturation for 5 min at 95 °C, cDNA synthesis at 50 °C for 30 min, and RT inactivation at 95 °C for 1 min, followed by 45 cycles of denaturation at 95 °C for 15 s, annealing, and extension at 60 °C for 1 min performed on a CFX96 Real-Time Detection System (Bio-Rad). A sample was considered positive if its sigmoidal amplification curve crossed the threshold line before 40 cycles. A nontemplate control was used in each of the assays. To avoid cross-contamination, RNA was extracted from standard preparations and fecal specimens in separate laboratories.
Statistical analysis
Statistical analysis of the data was performed using One-way ANOVA with Tukey's post hoc test, Student's t test and Pearson's correlation coefficient with the software jamovi v.2.3.26 [31]. Retrieved from https://www.jamovi.org.
Results
Among the 11 gene segments, conserved nucleotide stretches suitable for designing the primers and probes were observed in NSP3 and NSP5 of RVB and the VP6 gene of RVC. The designed primers and probes were examined for self-annealing sites, hairpin loop formation, 3’ complementarities, and melting temperatures (Tm) using the IDT oligonucleotide calculator tool and found suitable for real-time RT-PCR assay. However, the primers and probes were synthesized for the NSP5 gene of RVB and the VP6 gene of RVC and were labeled with 6-FAM and VIC reporter dyes, respectively, at the 5’ end and evaluated for the detection of RVB and RVC. The GenBank accession numbers of the strains refer to the locations of the primers and probes, and the sizes of the PCR products are described in Table 1.
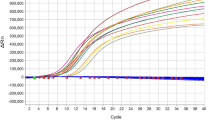
Fecal specimens collected from sporadic and outbreak cases of AGE were tested simultaneously for the presence of RVB (n = 192) and RVC (n = 188) using the respective conventional RT‒PCR and newly developed qRT‒PCR assays. All RVB (n = 31) and RVC (n = 8) positive specimens were reactive according to the qRT‒PCR assays and presented Ct values ranging between 23.69 and 41.97 and between 11.49 and 36.05, respectively (Fig. 1). All known positive and negative specimens for other viral agents were nonreactive, and comparative analysis showed 100% concordance with conventional RT‒PCR assays.

A representative amplification curve of RVB-positive (a) and RVC-positive (b) specimens determined via qRT‒PCR
To determine the efficiency of the qRT‒PCR assays, serial tenfold dilutions (101–109) of RNA transcripts from RVB/RVC were used as standards in assay runs along with template and nontemplate controls. The plot of Ct values versus log transcript copy number of RVB indicated a linear correlation with an R2 value of 0.999, and the efficiency of the assay was calculated to be 95.3% (Fig. 2a). Analysis of the calibration data indicated that the range of the quantitative analysis was from 12.3 × 109 to 12.3 × 102 copies per reaction, corresponding to Ct values of 13.25–37.32. Similarly, after using serial tenfold dilutions (101—109) of the RNA transcripts of RVC, a linear correlation was observed, with R2 values of 0.992 and a 110.2% efficiency for the assay (Fig. 2b). Analysis of the calibration data indicated that the range of the quantitative analysis was from 4.3 × 109 to 4.3 × 102 copies per reaction, corresponding to Ct values of 16.65—39.3, respectively.

Amplification curves of serial tenfold dilutions of RNA transcripts and the linear relationship between the log transcript copy number and the number of quantitation cycles. The relative fluorescence units on the Y axis refer to the fluorescence emission of a reaction minus the background fluorescence
RVB (n = 31) and RVC (n = 8) positive specimens presented viral loads between 9.11 × 108 and 3.57 × 104 (Table 2) and between 6.61 × 1012 and 2.62 × 105 copies per reaction, respectively. One-way ANOVA with Tukey's post hoc test was performed to compare the severity of the patients with mild (n = 3), moderate (n = 12), or severe (n = 15) disease with the corresponding RVB viral load, and the results were not significantly different. Tukey’s post hoc test showed no significant difference in the mean log viral load of RVB between each pair of severity groups. Student's t test was used to compare the mean log viral load of RVB between females (7.09 ± 1.19) and males (7.13 ± 0.921), and the difference was not significant. Pearson's correlation coefficient (r) between age and the log viral load of RVB was 0.036, which indicated no significant correlation. Due to the small sample size, a similar analysis was not possible for RVC-positive specimens.
Discussion
The evaluation of 11 genomic RNA segments indicated the suitability of the NSP3 and NSP5 genes of the human RVB and the VP6 gene of the human RVC strains for the design of primers and probes. The primers and probes synthesized for the NSP5 (RVB) and VP6 (RVC) genes were validated using conventional RT‒PCR assays and showed 100% concordance. The specificity of the primers and probes was confirmed by testing fecal specimens positive for other enteric viruses as well as specimens negative for all viral agents. The use of qRT‒PCR assays (VP7 gene-based) for the detection of human RVC strains was previously reported [32, 33], but not for RVB strains. Rotaviruses continuously accumulate point mutations and undergo reassortment events [34], therefore, timely evaluation of earlier primers and probes using the strains available thus far is necessary. The sequences of the primers and probes reported earlier were checked using multiple sequence alignment of all the available strains in Genbank (n = 23) for the VP7 gene of the RVC. Due to the variable site at the extension site of DNA polymerase or the high number of variable sites or IDT criteria, few of these mutations were found to be unsuitable for qRT‒PCR. The newly developed qRT‒PCR assays displayed 100% sensitivity and specificity when the respective conventional RT‒PCR assays were used as the gold standard.
Analysis of the viral load in the RVB-positive stool specimens revealed no correlation with the severity of the diarrheal disease or age of the patient, and the viral loads were comparable between male and female patients (Table 2). The main limitation of the present study is the small number of RVC-positive specimens available for validation of the assay, and all the RVB-positive specimens included in the study were collected from adult diarrheal patients of two outbreaks reported earlier near Pune city [5, 15]. The absence of RVB in pediatric sporadic cases (hospitalized between 2021 and 2023) observed in the present study is similar to the findings of an earlier study indicating circulation of RVB in the Mumbai and Surat cities of Western India in outbreak cases, with its absence in sporadic cases of gastroenteritis in children [35]. A lower attack rate in children than in adolescents and adults has been documented in multiple outbreaks due to RVB [15, 36,37,38]. The resistance of the pediatric population to RVB infections was suspected to be due to cross-protection with other serotypes, especially RVA, or may be due to changes in cell receptors and maternal and local immunity [5]. However, the increase in porcine RVC infections in piglets vaccinated with the porcine RVA G5P [8] vaccine documented in Brazil [39] suggests the need for additional studies on non-RVA rotaviral infections.
Sporadic and low rates of infection indicate an evolutionarily stable host‒pathogen relationship, and subtle genetic alterations are suspected to increase pathogenicity, leading to widespread epidemics [40]. The development of a rapid qRT‒PCR assay for the detection of RVB and RVC will be of great help in the future to monitor the role of non-RVA rotaviral agents in sporadic and outbreak cases and, in turn, to reduce the unnecessary use of antibiotics.
Availability of data and materials
No datasets were generated or analysed during the current study.
References
Vos T, Barber RM, Bell B, Bertozzi-Villa A, Biryukov S, Bolliger I, et al. (Global Burden of Disease Study 2013 Collaborators). Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743–800. https://doi.org/10.1016/s0140-6736(15)60692-4.
Du Y, Chen C, Zhang X, Yan D, Jiang D, Liu X, Yang M, Ding C, Lan L, Hecht R, Zhu C, Yang S. Global burden and trends of rotavirus infection-associated deaths from 1990 to 2019: an observational trend study. Virol J. 2022;19(1):166. https://doi.org/10.1186/s12985-022-01898-9.PMID:36266651;PMCID:PMC9585833.
Dattani S, Spooner F, Ritchie H and Roser M. (2023) - "Diarrheal diseases". Published online at OurWorldInData.org. Retrieved from: 'https://ourworldindata.org/diarrheal-diseases' [Online Resource].
Hartman RM, Cohen AL, Antoni S, Mwenda J, Weldegebriel G, Biey J, Shaba K, de Oliveira L, Rey G, Ortiz C, Tereza M, Fahmy K, Ghoniem A, Ashmony H, Videbaek D, Singh S, Tondo E, Sharifuzzaman M, Liyanage J, Batmunkh N, Grabovac V, Logronio J, Serhan F, Nakamura T. Risk Factors for Mortality Among Children Younger Than Age 5 Years With Severe Diarrhea in Low- and Middle-income Countries: Findings From the World Health Organization-coordinated Global Rotavirus and Pediatric Diarrhea Surveillance Networks. Clin Infect Dis. 2023;76(3):e1047–53. https://doi.org/10.1093/cid/ciac561.
Joshi MS, Lole KS, Barve US, Salve DS, Ganorkar NN, Chavan NA, Shinde MS, Gopalkrishna V. Investigation of a large waterborne acute gastroenteritis outbreak caused by group B rotavirus in Maharashtra state. India J Med Virol. 2019;91(10):1877–81. https://doi.org/10.1002/jmv.25523.
Chasey D, Bridger JC, McCrae MA. A new type of atypical rotavirus in pigs. Arch Virol. 1986;89(1–4):235–43. https://doi.org/10.1007/BF01309892. (PMID: 3013130).
Eiden JJ, Nataro J, Vonderfecht S, Petric M. Molecular cloning, sequence analysis, in vitro expression, and immunoprecipitation of the major inner capsid protein of the IDIR strain of group B rotavirus (GBR). Virology. 1992;188(2):580–9. https://doi.org/10.1016/0042-6822(92)90512-n. (PMID: 1316675).
Chang KO, Parwani AV, Smith D, Saif LJ. Detection of group B rotaviruses in fecal samples from diarrheic calves and adult cows and characterization of their VP7 genes. J Clin Microbiol. 1997;35(8):2107–10. https://doi.org/10.1128/jcm.35.8.2107-2110.1997.PMID:9230391;PMCID:PMC229912.
Krishnan T, Sen A, Choudhury JS, Das S, Naik TN, Bhattacharya SK. Emergence of adult diarrhea rotavirus in Calcutta. India The Lancet. 1999;353(9150):380–1. https://doi.org/10.1016/S0140-6736(05)74954-0.
Chen Q, Wang L, Zheng Y, Zhang J, Guo B, Yoon KJ, Gauger PC, Harmon KM, Main RG, Li G. Metagenomic analysis of the RNA fraction of the fecal virome indicates high diversity in pigs infected by porcine endemic diarrhea virus in the United States. Virol J. 2018;15(1):95. https://doi.org/10.1186/s12985-018-1001-z.PMID:29801460;PMCID:PMC5970503.
Wu H, Taniguchi K, Urasawa T, Urasawa S. Serological and genomic characterization of human rotaviruses detected in China. J Med Virol. 1998;55(2):168–76. https://doi.org/10.1002/(sici)1096-9071(199806)55:2%3c168::aid-jmv14%3e3.0.co;2-e. (PMID: 9598939).
Sanekata T, Ahmed MU, Kader A, Taniguchi K, Kobayashi N. Human group B rotavirus infections cause severe diarrhea in children and adults in Bangladesh. J Clin Microbiol. 2003;41(5):2187–90. https://doi.org/10.1128/JCM.41.5.2187-2190.2003.PMID:12734276;PMCID:PMC154663.
Alam MM, Pun SB, Gauchan P, Yokoo M, Doan YH, Tran TN, Nakagomi T, Nakagomi O, Pandey BD. The first identification of rotavirus B from children and adults with acute diarrhea in kathmandu, Nepal. Trop Med Health. 2013;41(3):129–34. https://doi.org/10.2149/tmh.2013-15. Epub 2013 Jul 4. PMID: 24155654; PMCID: PMC3801157.
Aung MS, Nahar S, Aida S, Paul SK, Hossain MA, Ahmed S, Haque N, Ghosh S, Malik YS, Urushibara N, Kawaguchiya M, Sumi A, Kobayashi N. Distribution of two distinct rotavirus B (RVB) strains in the north-central Bangladesh and evidence for reassortment event among human RVB revealed by whole genomic analysis. Infect Genet Evol. 2017;47:77–86. https://doi.org/10.1016/j.meegid.2016.11.001.
Joshi MS, Ganorkar NN, Ranshing SS, Basu A, Chavan NA, Gopalkrishna V. Identification of group B rotavirus as an etiological agent in the gastroenteritis outbreak in Maharashtra. India J Med Virol. 2017;89(12):2244–8. https://doi.org/10.1002/jmv.24901.
Dai GZ, Sun MS, Liu SQ, Ding XF, Chen YD, Wang LC, Du DP, Zhao G, Su Y, Li J, et al. First report of an epidemic of diarrhea in human neonates involving the new rotavirus and biological characteristics of the epidemic virus strain (KMB/R85). J Med Virol. 1987;22(4):365–73. https://doi.org/10.1002/jmv.1890220409. (PMID: 3040899).
Malik YP, Chandrashekar KM, Sharma K, Prasad M, Prasad G. Evidence for Occurrence of Human group B rotavirus in Central India Based on Characterization of NSP2 Gene. Indian J Virol. 2011;22(2):98–103. doi: https://doi.org/10.1007/s13337-011-0046-z. Epub 2011 Aug 11. PMID: 23637510; PMCID: PMC3550739.
Lahon A, Maniya NH, Tambe GU, Chinchole PR, Purwar S, Jacob G, Chitambar SD. Group B rotavirus infection in patients with acute gastroenteritis from India: 1994–1995 and 2004–2010. Epidemiol Infect. 2013;141(5):969–75. https://doi.org/10.1017/S0950268812001537. Epub 2012 Jul 20. PMID: 22813354; PMCID: PMC9151812.
Saif LJ, Jiang B. Nongroup A rotaviruses of humans and animals. Curr Top Microbiol Immunol. 1994;185:339–71. https://doi.org/10.1007/978-3-642-78256-5_11. (PMID: 8050284).
Rahman M, Banik S, Faruque AS, Taniguchi K, Sack DA, Van Ranst M, Azim T. Detection and characterization of human group C rotaviruses in Bangladesh. J Clin Microbiol. 2005;43(9):4460–5. https://doi.org/10.1128/JCM.43.9.4460-4465.2005.PMID:16145092;PMCID:PMC1234047.
Tiku VR, Jiang B, Kumar P, Aneja S, Bagga A, Bhan MK, Ray P. First study conducted in Northern India that identifies group C rotavirus as the etiological agent of severe diarrhea in children in Delhi. Virol J. 2017;14(1):100. https://doi.org/10.1186/s12985-017-0767-8.PMID:28558823;PMCID:PMC5450416.
Joshi MS, Jare VM, Gopalkrishna V. Group C rotavirus infection in patients with acute gastroenteritis in outbreaks in western India between 2006 and 2014. Epidemiol Infect. 2017(b);145(2):310–315. https://doi.org/10.1017/S0950268816002363. Epub 2016 Oct 26. PMID: 27780494; PMCID: PMC9507622.
Srivastava S, Banerjee S, Debbarma S, Kumar P, Sinha D. Rural-urban differentials in the prevalence of diarrhea among older adults in India: Evidence from Longitudinal Aging Study in India, 2017–18. PLoS ONE. 2022;17(3): e0265040. https://doi.org/10.1371/journal.pone.0265040.PMID:35294455;PMCID:PMC8926275.
Tamura K, Stecher G, Peterson D, Filipski A, Kumar S. MEGA6: Molecular evolutionary genetics analysis version 6.0. Mol Biol Evol 2013;30:2725–2729.
Mijatovic-Rustempasic S, Tam KI, Kerin TK, Lewis JM, Gautam R, Quaye O, et al. Sensitive and specific quantitative detection of rotavirus A by one-step real-time reverse transcription-PCR assay without antecedent double-stranded-RNA denaturation. J Clin Microbiol. 2013;51:3047–54. https://doi.org/10.1128/JCM.01192-13.
Kang G, Arora R, Chitambar SD, et al. Multicenter, hospital-based surveillance of rotavirus disease and strains among Indian children aged <5 years. J Infect Dis. 2009;200:S147–53. https://doi.org/10.1086/605031.
Sapkal GN, Bondre VP, Fulmali PV, Patil P, Gopalkrishna V, Dadhania V, Ayachit VM, Gangale D, Kushwaha KP, Rathi AK, Chitambar SD, Mishra AC, Gore MM. Enteroviruses in patients with acute encephalitis, uttar pradesh. India Emerg Infect Dis. 2009;15(2):295–8. https://doi.org/10.3201/eid1502.080865.PMID:19193277;PMCID:PMC2657625.
Kojima S, Kageyama T, Fukushi S, et al. Genogroup-specific PCR primers for detection of Norwalk-like viruses. J Virol Methods. 2002;100(1–2):107–14. https://doi.org/10.1016/s0166-0934(01)00404-9.
Allard A, Albinsson B, Wadell G. Rapid typing of human adenoviruses by a general PCR combined with restriction endonuclease analysis. J Clin Microbiol. 2001;39(2):498–505. https://doi.org/10.1128/JCM.39.2.498-505.2001.
Belliot G, Laveran H, Monroe SS. Detection and genetic differentiation of human astroviruses: phylogenetic grouping varies by coding region. Arch Virol. 1997;142(7):1323–34. https://doi.org/10.1007/s007050050163.
R Core Team. R: A Language and environment for statistical computing. (Version 4.1) [Computer software]. 2021. Retrieved from https://cran.r-project.org. (R packages retrieved from MRAN snapshot 2022–01–01).
Logan C, O’Leary JJ, O’Sullivan N. Real-time reverse transcription-PCR for detection of rotavirus and adenovirus as causative agents of acute viral gastroenteritis in children. J Clin Microbiol. 2006;44(9):3189–95. https://doi.org/10.1128/JCM.00915-06.PMID:16954246;PMCID:PMC1594742.
Mori K, Hayashi Y, Akiba T, Nagano M, Tanaka T, Hosaka M, Nakama A, Kai A, Saito K, Shirasawa H. Multiplex real-time PCR assays for the detection of group C rotavirus, astrovirus, and Subgenus F adenovirus in stool specimens. J Virol Methods. 2013;191(2):141–7. https://doi.org/10.1016/j.jviromet.2012.10.019. (Epub 2012 Nov 14 PMID: 23159674).
Patton JT. Rotavirus diversity and evolution in the postvaccine world. Discov Med. 2012;13(68):85–97. PMID: 22284787; PMCID: PMC3738915.
Chitambar S, Gopalkrishna V, Chhabra P, Patil P, Verma H, Lahon A, Arora R, Tatte V, Ranshing S, Dhale G, Kolhapure R, Tikute S, Kulkarni J, Bhardwaj R, Akarte S, Pawar S. Diversity in the enteric viruses detected in outbreaks of gastroenteritis from Mumbai, Western India. Int J Environ Res Public Health. 2012;9(3):895–915. https://doi.org/10.3390/ijerph9030895. Epub 2012 Mar 14. PMID: 22690171; PMCID: PMC3367285.
Chitambar SD, Lahon A, Tatte VS, Maniya NH, Tambe GU, Khatri KI, Desai HS, Ugare MR, Kulkarni SV, Waghmare AP. Occurrence of group B rotavirus infections in the outbreaks of acute gastroenteritis from western India. Indian J Med Res. 2011;134(3):399–400. PMID: 21985827; PMCID: PMC3193725.
Kelkar SD, Zade JK, Dindokar AR, Dhale GS, Vaishya SS. Outbreak of diarrhea in Daman and detection of group B rotavirus from three adult cases. Natl Med J India. 2007;20(1):47 (PMID: 17557528).
Wang SS, Cai RF, Chen J, Li RJ, Jiang RS. Etiologic studies of the 1983 and 1984 outbreaks of epidemic diarrhea in Guangxi. Intervirology. 1985;24(3):140–6. https://doi.org/10.1159/000149633. (PMID: 2999028).
Molinari BL, Possatti F, Lorenzetti E, Alfieri AF, Alfieri AA. Unusual outbreak of postweaning porcine diarrhea caused by single and mixed infections of rotavirus groups A, B, C, and H. Vet Microbiol. 2016;193:125–32. https://doi.org/10.1016/j.vetmic.2016.08.014.
Sen A, Kobayashi N, Das S, Krishnan T, Bhattacharya SK, Naik TN. The evolution of human group B rotaviruses. Lancet. 2001;357(9251):198–9. https://doi.org/10.1016/S0140-6736(00)03596-0. (PMID: 11213100).
Acknowledgements
We express our gratitude to the Director of the Indian Council of Medical Research-National Institute of Virology (ICMR-NIV) for their constant support during this period. We would also like to acknowledge the technical assistance provided by Mrs. Nutan Chavan. The funds for this project were graciously provided by the ICMR-NIV and the Indian Council of Medical Research, Ministry of Health and Family Welfare, Government of India.
Funding
The funds for the project were provided by the ICMR-National Institute of Virology, Indian Council of Medical Research, Ministry of Health and Family Welfare, Government of India.
Author information
Authors and Affiliations
Contributions
M.J.: key role in the study design, execution of the study and writing of the manuscript; retrieval and sorting of the data from GenBank and implementation of the analysis; M.S.: conducting all the laboratory work; M.L.: overall execution of the study. All the authors approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
NIV/IEC/February/2024/D-9 dated 7/2/2024.
Consent for publication
All the authors approved the final manuscript for publication.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Joshi, M.S., Shinde, M.S. & Lavania, M. Evaluation of different genomic regions of rotavirus B and rotavirus C for development of real-time RT‒PCR assays. Virol J 21, 94 (2024). https://doi.org/10.1186/s12985-024-02369-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12985-024-02369-z