
Abstract
Background
Children with developmental coordination disorder (DCD) have impaired online motor control. Researchers posit that this impairment could be due to a deficit in utilizing the internal model control process. However, there is little neurological evidence to support this view because few neuroimaging studies have focused specifically on tasks involving online motor control. Therefore, the aim of this study was to investigate the differences in cortical hemodynamic activity during an online movement adjustment task between children with and without DCD.
Methods
Twenty children with DCD (mean age: 9.88 ± 1.67 years; gender: 14M/6F) and twenty age-and-gender matched children with typical development (TD) (mean age: 9.87 ± 1.59 years; gender: 14M/6F) were recruited via convenience sampling. Participants performed a double-step reaching task under two conditions (with and without online adjustment of reaching). Cortical hemodynamic activity during task in ten regions of interest, including bilateral primary somatosensory cortex, primary motor cortex, premotor cortex, superior parietal cortex, and inferior parietal cortex was recorded using functional near-infrared spectroscopy. In the analyses, change in oxyhemoglobin (ΔHbO) concentration was used to characterize hemodynamic response. Two-way analyses of variance were conducted for each region of interest to compare hemodynamic responses between groups and conditions. Additionally, Pearson’s r correlations between hemodynamic response and task performance were performed.
Results
Outcome showed that children with DCD required significantly more time to correct their reaching movements compared to the control group (t = 3.948, P < 0.001). Furthermore, children with DCD have a significantly lower ΔHbO change in the left superior parietal cortex during movement correction, compared to children with TD (F = 4.482, P = 0.041). Additionally, a significant negative correlation (r = − 0.598, P < 0.001) was observed between the difference in movement time of reaching and the difference in ΔHbO between conditions in the left superior parietal cortex.
Conclusions
The findings of this study suggest that deficiencies in processing real-time sensory feedback, considering the function of the superior parietal cortex, might be related to the impaired online motor control observed in children with DCD. Interventions could target this issue to enhance their performance in online motor control.
Similar content being viewed by others


Background
Coordinated action is crucial for efficiently completing daily activities in the face of dynamic environment. To achieve it, the ability to continuously monitor and seamlessly adjust movements in response to the changing environmental conditions during an action, known as ‘online motor control’, is necessary [1, 2]. Online motor control typically develops rapidly during childhood (e.g. 6–12 years old); however, in children with Developmental Coordination Disorder (DCD), this development might be affected [3, 4]. DCD is a common neurodevelopmental disorder beginning in childhood [5]. Children with DCD are found to have difficulties in acquisition and execution of coordinated motor skills compared to their typically developing peers of the same chronological age, affecting their performance in daily activities and academic tasks [5,6,7]. An in-depth understanding of online motor control in children with DCD is necessary to inform early interventions, thereby avoiding possible irreversible effects on their future lives.
The online motor control of children with DCD is commonly examined using a double-step paradigm for upper limb reaching movement [3, 8, 9]. In this paradigm, the movement target shifts to a different location after the movement is started, requiring the performers to quickly and successfully correct their movement direction to reach the new target and complete the task. Children with DCD were found to exhibit impaired online motor control in terms of task performance and kinematic outcomes [3, 4, 8, 10,11,12]. For instance, Hyde and Wilson [3, 8] observed that children with DCD exhibited significantly longer movement times and had more delayed initiation of corrective actions than children with typical development (TD). Conversely, Adams et al. [2] and Plumb et al. [9] argued that children with DCD might not have impairment in online motor control, as no significant differences were found in time used for movement correction between groups. The inconsistency in the results between those studies may stem from the variations in task difficulty. Regardless, an in-depth investigation into the neurological underpinnings of online motor control deficits in children with DCD becomes necessary, no matter whether to reconcile these differences or to advance the development of targeted interventions.
Over the past few decades, the availability of neuroimaging techniques such as functional magnetic resonance imaging, functional near-infrared spectroscopy (fNIRS), and electroencephalography has enabled researchers to explore motor control from neuroscientific perspectives. Among these, fNIRS captures the hemodynamic response to neuronal activity in the cerebral cortex by measuring changes in the concentrations of oxyhemoglobin and deoxyhemoglobin [13]. Compared to other techniques, fNIRS is relatively robust to motion artifacts and offers a real-life testing environment, making it the most suitable for assessing online motor control in children with DCD using the double-step reaching protocol [14, 15]. However, one major limitation of fNIRS is that it can only map cortical activations.
Literature have suggested that the online motor control in the double-step paradigms can be achieved through a neural process known as the ‘internal model’ [16, 17]. Generally, in this neural process, the sensory consequences of the initial reaching movement are first predicted from the efference copy of issued motor commands (i.e., internal feedback). Subsequently, these predictions are with sensory feedback that reveals the relative position of the moving limb and target. If a mismatch arises due to a target shift, an error signal is generated to adapt motor commands to correct movement in real time [3, 18]. In the process, two cortical regions, including the motor cortex (located in the frontal lobe) and the parietal lobe, are involved. The parietal lobe is proposed to be vital for constructing internal feedback and acquiring external sensory feedback [10, 19]. Concurrently, it is posited to facilitate the comparison and detection of discrepancies between predicted sensory consequences and actual sensory feedback [20, 21]. Later, the motor cortex is responsible for generating motor commands for initial and corrective movements [21]. As a result, the function of these two regions is crucial for online motor control.
Atypical brain functions in children with DCD that might be associated with online motor control have been observed in the abovementioned regions. Zwicker et al. [22, 23] found significantly lower activation in the parietal lobe in children with DCD than in children with TD when performing a trail-tracing task. Similar findings indicating reduced activation in the parietal lobe of children with DCD during motor tasks such as hand rotation, finger adduction/abduction, and target tracking have been reported in other neuroimaging studies [24,25,26,27,28,29]. In addition, Caçola et al. [14] identified abnormal activation in the motor cortex of children with DCD during fine motor movements. However, it is important to note that most neuroimaging studies merely revealed differential brain activation patterns in the two regions between children with and without DCD during movement that was executed repeatedly. A link between these abnormalities and poor online motor control was not directly established by a specialized paradigm (e.g., double-step task). Thus, there is a need for research that is meticulously tailored to explicitly probe the functioning of motor cortex and parietal lobe during online motor control in children with DCD [30].
Therefore, the aim of this study was to compare cortical hemodynamic activity in the motor cortex and parietal lobe in children with and without DCD when performing a modified double-step task using fNIRS. The specific research questions were as follows:
-
(1)
Do children with DCD spend longer time correcting movement in the double-step reaching task?
-
(2)
Do children with DCD show lower activation changes in the motor cortex and parietal lobe, if they spend more time correcting movement in the double-step reaching task?
-
(3)
Which regions exhibit changes in activation associated with slower performance, if any, in the double-step reaching task?
Material and methods
Participants
Participants were recruited using convenience sampling by posters placed on social media. Children with DCD were included in the study if they satisfied four specific criteria from the Diagnostics and Statistical Manual of Mental Disorders, Fifth Edition: (a) scored below the 5th percentile in the Hong Kong Fine Motor Test for the School-aged (HKFMTS) [31] (see Supplemental material A for details); (b) scored below age-specific cut off in the Developmental Coordination Disorder Questionnaire (DCDQ) (criterion B); (c) showed an early onset of symptoms as reported by parents (criterion C); and (d) had no intellectual or visual impairment, or other physical and neurological conditions as reported by parents (criterion D). Children with left-hand dominance were excluded from the study.
The control group consisted of children with typical development (TD) who met the following inclusion criteria: (a) age- and gender-matched with the DCD participants; (b) right-handed; and (c) had no intellectual or visual impairments or any other physical or neurological conditions as reported by parents. Children in the TD group were also assessed using the HKFMTS and DCDQ, ensuring that they achieved the scores within the normal range.
For both groups of children with TD and DCD, the DCDQ was first administered by sending an online questionnaire to parents after receiving their expression of interest in participating in the study. A contact person was available to answer parents’ questions about the meaning of items in the DCDQ. The HKFMTS was conducted after confirming that children fulfilled the requirements for being TD or probable-DCD based on the DCDQ results. The HKFMTS was administered in a quiet room by two trained occupation therapy students in the pediatric neuroscience lab at university campus. Eligible children were then invited to the fNIRS study on another day within one month. Both ethics approval and participant consent were obtained; details can be found in the Declarations section. Table 1 provides a summary of the demographics and details of the children involved in the study.
Study design
Prior to the experiment, participants were seated upright on a chair with adjustable seat height, seat depth, and footrest height in front of a fixed table and a computer monitor. A press button was placed on the table, and three pencils for manipulation were placed upright at coordinates of − 30°, 0°, and 30° with respect to the press button. The center of the press button was set 30 cm from each pencil and 50 cm from the monitor (Fig. 1A).

Illustration of the A experimental set-up and B task paradigm. A Participants were instructed to sit on the chair and remain close to the backrest throughout the experiment. They were also asked to place their right hand on the right side of the button (but not press it), maintain their forearm horizontally with the upper arm perpendicular to it, and rest their left hand on their left thigh as the starting position. B The task was initiated with participants placing their right palm on the start button. After a random interval of 1 to 2 s, they were signaled to reach the target. During their ongoing reaching, there is a 67% probability that the target remained unchanged and a 33% chance that it shifted to a different target, as depicted in the monitor. The time limit for this movement was 5 s. Upon reaching the target, the participants automatically returned their hand to the starting position and then rested for a 20-s period before proceeding with the next trial
At the onset of the experiment, participants were directed to press the button with their right palm. A white cross then appeared on the monitor serving as a preparatory signal. Following a random interval of 1 to 2 s, the white cross transitioned to a slide featuring three images depicting the positions (left, middle, and right) of three pencils, coupled with an auditory cue that signaling the start of the reaching movement. One of the three images was highlighted to prompt participants about the target pencil. Initially, the middle image was always highlighted. However, once the participant’s palm left the button, this image could either stay highlighted (non-jump trial) or switch off, with one of the lateral images (left or right) lighting up (jump trial), each with an equal probability of occurring. Participants were informed about these possibilities beforehand and instructed to execute their movements swiftly and accurately. They were then required to return their hand to the starting point and wait for the next trial. Each trial lasted about 5 s and was followed by a 20-s rest period. All stimuli were presented using E-Prime (version 2.10, Psychology Software Tool, USA).
The experimental setup consisted of two runs, each containing 24 trials—16 non-jump and 8 jump trials, randomized throughout. Each run lasted around 10 min, separated by a 3-min rest interval. The entire session was recorded using a synchronized camera system, specifically the Logitech C270 HD webcam, which is capable of Full HD 720p resolution at 30 Hz. In addition, preceding the formal testing phase (before participants were fitted with the fNIRS cap and probes), a practice session with 12 trials (8 non-jump and 4 jump) was given to acquaint participants with the task.
fNIRS measurement
The cortical hemodynamic activity during the task was recorded using a multichannel fNIRS optical topography system (ETG-4000, Hitachi Medical Co., Japan) with near-infrared light at wavelengths of 695 nm and 830 nm; its sampling rate was 10.0 Hz. Two 3 × 5 probe sets with eight sources and seven detectors were fastened in a customized EEG cap and placed on the participants’ head, resulting in 2 × 22 channels in total (Fig. 2). Specifically, the two probes were symmetrically positioned with channel 21/25 aligned to the ‘C1/C2’ point of the international 10/20 system, and the alignment of channels 3-12-21/25–36-43 corresponded to the ‘C5–C1/C6–C2’ line. The distance between each probe was 3 cm. The ‘Cz’ point on the cap served as a reference marker to ensure consistent positioning across participants. Additionally, a 3D-magnetic space digitizer (EZT-DM401, Hitachi Medical Corporation, Japan) was employed to document the 3D location of each probe on the participant’s head. These coordinates were subsequently registered into Montreal Neurological Institute coordinates using the AtlasViewer toolbox for meticulous probe-set placement verification [32]. Table 2 depicts the cortical regions (i.e., regions of interest; ROIs) covered by the probe arrangement in the present study, according to the estimation of probabilistic anatomical locations of channels based on the Brodmann area atlas.

Arrangement of fNIRS channels
Data analysis
Initially, trials with non-compliance were excluded from subsequent analysis. These non-compliant trials included those in which participants did not complete the movement within the 5-s time limit, failed to reach the correct target pencil, or had significant movement from other body segments during the action. These trials were identified using the videos recorded by the synchronized camera. The excluded data accounted for approximately 7% of the total dataset.
Behavioral data analysis
To evaluate the behavioral performance of the task, movement time difference (MTdiff) was computed by subtracting the movement time of the jump condition from the non-jump condition. Movement time was defined as the duration between reaching initiation and completion. Reaching initiation was identified as the point when the participants’ hand left the press button, while completion was marked by the moment when the participants touched the pencil. The timing of all these events was determined by analyzing the videos recorded by the synchronized camera during the experiment.
fNIRS data processing and analysis
The recorded original fNIRS signals were analyzed using HOMER2 [33]. First, noisy channels were identified and pruned. Subsequently, all normal fNIRS signals were converted into optical density. Motion artifacts were then corrected using wavelet filtering (inter-quartile range = 0.1), a method suggested to yield promising outcomes in the pediatric population [34]. Next, a bandpass filter ranging from 0.01 to 0.1 Hz was applied to remove the slow drifts and cardiac pulsation signal. After that, optical density was converted into the concentration change of oxyhemoglobin concentration (ΔHbO) and deoxyhemoglobin concentration (ΔHbR) using the modified Beer–Lambert law with a partial pathlength factor of 6. Finally, the resulting data were block averaged within a period from 3 s before the task to 12 s after the task as the time-series concentration changed.
ΔHbO was utilized for further analysis due to its higher contrast-to-noise ratio compared to ΔHbR [35]. ΔHbO was averaged over a time window ranging from 5 to 10 s after task onset as activation amplitude for each trial. This is based on the understanding that ΔHbO requires approximately 5 s to achieve a stable change and typically peaks within 5 to 10 s after movement onset during motor tasks [36, 37]. Notably, in the current study, ΔHbO peaked at approximately 7 to 8 s post task onset according to the time-series data.
Statistical analysis
An independent sample t test was first used to investigate the difference in behavioral performance by comparing the MTdiff between children with DCD and TD. To visualize the cortical hemodynamic response for the task at the group level, we calculated the between-condition difference in activation amplitude using a paired t test and generated t-maps for both groups using the BrainNet Viewer toolbox, according to the previously registered MNI coordinates [38]. The channel-wise t values are reported in Supplemental material B and for visualization purposes only (i.e., not for interpretation). Furthermore, the average activation amplitude of each ROI was analyzed to explore the effects of group and condition on cortical activities. A 2 × 2 mixed ANOVA was performed on activation amplitude in each ROI, involving group (DCD v.s. TD) as a between-subjects factor and condition (non-jump v.s. jump) as a within-subjects factor. Additionally, Pearson’s r correlation coefficients of the between-condition difference in activation amplitude in those ROIs with identified significant differences in the former test and MTdiff were calculated to further examine the association between cortical responses and behavioral performance. Effect sizes (including Cohen’s d for t-tests, partial η2 for ANOVAs, and r2 for correlations) were calculated to aid in interpreting the study results. All statistical analyses were executed using SPSS (version 22, IBM, USA) with a significance level set at 0.05 and a confidence interval of 95%.
Results
Behavioral results
The mean MTdiff for each group is shown in Fig. 3. The MTdiff of the DCD group [mean (SD): 463 ms (88 ms)] was significantly larger than that of the TD group [371 ms (55 ms)] (t = 3.948, P < 0.001, Cohen’s d = 1.25).

Movement time difference (mean ± SD) for the task in the TD group and DCD group. Independent t-test revealed a significant group difference (P < 0.001)
fNIRS results
A visual representation of cortical activity responses to the task for both groups is shown in Fig. 4. Generally, both groups demonstrated equal or higher activation in the left hemisphere during the jump condition, whereas changes in activation in the right hemisphere were comparatively modest. Notably, the TD group exhibited a more pronounced activation change in the left hemisphere, particularly in the parietal region, relative to the DCD group (see Supplemental material B for channel-wise results).

Visualization of the cortical activity for the task in the TD group (left) and DCD group (right). The color bar indicates the t values rendered over on a 3D head model, the warm color (e.g., yellow to red) (positive t values) represents cortical activation increased in the jump condition compared to the non-jump condition, and the cold color (e.g., green to blue) (negative t values) represents cortical activation decreased in the jump condition compared to the non-jump condition
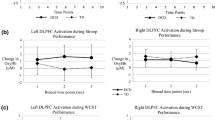
For the left superior parietal cortex (SPC), two-way ANOVA revealed a significant main effect of condition (F = 14.536, P = 0.001, partial η2 = 0.277) and group (F = 4.302, P = 0.045, partial η2 = 0.102), as well as an interaction effect of condition and group (F = 4.482, P = 0.041, partial η2 = 0.106) on ΔHbO (see Fig. 5A). A post hoc test of the simple main effect suggested that the condition effect was significant only in the TD group (t = 4.908, P < 0.001, Cohen’s d = 1.10), and it was not observed in the DCD group (t = 1.077, P = 0.296, Cohen’s d = 0.24). The significant group effect can only be found in the jump condition (t = 2.715, P = 0.010, Cohen’s d = 0.88) but not in the non-jump condition (t = 0.872, P = 0.389, Cohen’s d = 0.28). In addition, a significant main effect of condition (F = 13.307, P = 0.001, partial η2 = 0.259) was found in the left inferior parietal cortex (IPC) but not of group or an interaction of condition * group (see Fig. 5B). No significant differences were found in the other regions (see Supplemental material C for complete means, SDs and statistical results).

Average activation amplitude (mean ± SE) in the A left superior parietal cortex (L. SPC) and B left inferior parietal cortex (L.IPC). Two-way ANOVA revealed a significant interaction effect (P = 0.041), as well as significant main effects of group (P < 0.001) and condition (P = 0.045) in the L. SPC, and a significant main effect of condition (P = 0.001) in the L. IPC. Significance in the test of simple main effects of L.SPC is further displayed on the plot, where * represents P < 0.05, ** represents P < 0.001, and *** represents P < 0.001
Correlation between behavioral performance and cortical activation
As shown in Fig. 5, significant negative correlations were found between MTdiff and the difference in activation amplitude in the left SPC, irrespective of whether the TD and DCD groups were combined (r = − 0.598, P < 0.001, r2 = 0.36) (Fig. 6A) or analyzed separately (r = − 0.496, P = 0.026, r2 = 0.25 for TD; r = − 0.560, P = 0.010, r2 = 0.31 for DCD) (Fig. 6B, C). No such significant correlation was found in the left IPC (r = − 0.156, P = 0.357, r2 = 0.02).

Correlation between behavioral performance and cortical activation in the A left superior parietal cortex (L. SPC) of both groups, B left superior parietal cortex of the TD group, and C left superior parietal cortex of the DCD group
Discussion
In this study, we compared behavioral performance and cortical activation of the motor and parietal cortex during the double-step reaching task between children with TD and DCD. Children with DCD exhibited poorer task performance (i.e., spending more time correcting their movement) than their TD peers. Correspondingly, they displayed a relatively lower increase in activation in the left hemisphere, with a significant difference noted in the left SPC during movement correction. A significant negative correlation also emerged between left SPC activation and task performance. These findings suggest that children with DCD showed poor online motor control, which may be related to insufficient SPC activation.
Behaviorally, our results revealed a notable delay among children with DCD in real-time correction of their reaching movements. Despite this, their ability to accurately reach the true target in jump trials almost paralleled that of their TD counterparts. Our finding aligns, to a certain extent, with the majority of previous studies that have identified deficits in online motor control in individuals with DCD [3, 4, 11]. Our neuroimaging results may further unpack these behavioral phenomena, providing additional insight into the underlying neural mechanisms and contributing to our understanding of online motor control deficits in children with DCD.
Our neuroimaging results broadly highlighted a significantly increased activation within the left parietal cortex in response to movement correction for both groups. Obviously, it is not surprising that both children with TD and DCD may predominantly rely on the left hemisphere for the right-handed task used in the current study. The significant interaction effect found in left SPC activation, together with the notable correlation between change in its activation and movement time difference, might suggest the influence of left SPC functioning on observed behavioral difference in online motor control in children with DCD. Previous studies have also addressed the role of the SPC in controlling movement in real time. A study involving monkeys, for instance, identified a parallel pattern of SPC inactivation while assessing the adjustment of hand movements [39]. Considering that the SPC is centrally implicated in facilitating motor corrections by integrating real-time visual and proprioceptive sensory feedback [40–42], we speculate that the challenge in processing real-time sensory signals regarding the relative position of their hand and the target, stemming from the under-activation of the SPC in children with DCD, contributes to their slower online movement correction. This may account for the lack of a significant difference between the two groups of children in Adam’s study [2]. It is possible that their movement correction task in the transverse plane was less demanding in terms of sensory information acquisition compared to the 3D movement correction task applied in the current and previous studies [3, 4, 8, 10, 11].
Regarding the IPC, the presented results only demonstrated a significant condition effect, but with the absence of a significant group by condition interaction effect. This indicates that both groups modulated their IPC activation depending on the task condition, without a noticeable difference. As suggested, the IPC contributes to predicting movement consequences and comparing them with actual outcomes for forthcoming motor commands [40, 43, 44]. It is plausible that both DCD and TD children, despite their different proficiencies, utilize the IPC similarly for movement prediction and correction during tasks. As a result, children with DCD were able to reach the true target in one go in most of the jump trials, as observed in the current study and suggested in several previous studies [2,3,4]; this seems to distinguish them from individuals with complete parietal cortex lesions, whose hand movements cannot be updated when a sudden target jump occurs but fully complete the movement to the original target position before moving toward the new target [45, 46].
The observed difference in SPC activation during the double-step reaching task may provide added evidence for the theory of internal model deficits in children with DCD; it underscores a possible impairment in the processing of real-time sensory feedback during ongoing movements, a fundamental component of the internal model control process. This aligns with findings from other neuroimaging studies, confirming a consistent challenge in DCD [23, 27, 29]. By contrast, the current study did not identify a difference in IPC activation between groups, suggesting no difference in the production of internal feedback for monitoring and correcting movement during double-step tasks. This result does not conclusively indicate an absence of challenges within this domain of internal model control in children with DCD. Previous neuroimaging studies involving tracing/tracking tasks have identified diminished IPC activation in children with DCD [23, 24]. It is supposed that children with DCD may have a threshold limitation in IPC activation; thus, they find it difficult to handle tasks that require constant and intensive generation of internal feedback (i.e., tracking or tracing tasks).
The current study had several limitations. First, cerebellar activation was not captured in the study due to the limitations of fNIRS. Given the relative importance of the cerebellum in the internal model process, this study was unable to fully interpret the neurological underpinnings of online motor control deficits in children with DCD [47]. Future research that uses more advanced methods capable of measuring whole-brain activity to explore online motor control is needed to confirm the findings of the present study. Second, prolonged wear of fNIRS probes can lead to discomfort for children. To ensure that participants could complete the tasks comfortably, we had to restrict the total test duration. Consequently, we opted for a non-jump/jump ratio of 67%/33%, deviating from the more common 80%/20% ratio [3, 8], to allow for an adequate number of jump trials within the limited time; this might have led participants to become more accustomed to the jump trials, potentially yielding more favorable results in their behavioral performance and cortical responses. Third, to complete the entire task sequence, participants were needed to perform additional actions beyond the double-step reaching, such as pressing a button and returning their hands to the starting position. Cortical activation resulting from these actions was also captured in the collected data. Thus, a minor incongruity may exist between the observed cortical activation outcomes related to the double-step reaching task in this study and the actual situation. Last, this study only removed physiological noise by filtering when handling fNIRS data, which might lead to incomplete signal correction and biased results. Future studies using motor paradigms may consider additional strategies for dealing with physiological noise, such as applying depth-sensitive instrumentation or incorporating measurements of systemic physiology in the analysis [48].
The current study revealed a possible mechanism for online motor control deficit in children with DCD. That is, a relatively low hemodynamic response within the SPC might impede real-time sensory signal processing, potentially compromising the children’s ability to swiftly adjust their reaching movements. Therapeutic strategies might be oriented toward enhancing the functionality of this region or developing compensatory mechanisms to enhance the real-time motor correction capabilities of children with DCD. In addition, our neurobehavioral findings may support the presence of internal model deficits in DCD. It also possibly informs a nuanced aspect of DCD’s internal model control process, where deficiencies across various components may become apparent in response to increasing demands on it. Future research should further explore the dynamic functioning of various components engaged in the internal model process, such as movement prediction, sensory feedback processing and integration, movement updating and correction, in the face of different motor tasks and real-life movement, to pinpoint the nature of the internal model deficit in children with DCD. Such research can enhance the understanding of how the internal model impacts the everyday activities of DCD, thereby informing the development of targeted rehabilitation strategies.
Conclusions
In this study, we investigated cortical hemodynamic activity during online motor control in children with DCD using fNIRS. The results indicated that children with DCD showed delayed movement corrections during the task and significantly lower activation in the left SPC but not IPC than TD peers. These findings point to insufficiency in processing real-time sensory feedback as a potential cornerstone in the online motor control deficit observed in DCD. These insights may indicate the potential benefits of interventions focusing on enhancing sensory feedback processing to enhance online motor control in children with DCD. Furthermore, the results of the current study may offer additional insights into the internal model deficit inherent in DCD and call for further investigation into the precise manifestations of this deficit across diverse motor tasks and real-life activities.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
- DCD:
-
Developmental coordination disorder
- DCDQ:
-
Developmental Coordination Disorder Questionnaire
- fNIRS:
-
Functional near-infrared spectroscopy
- HKFMTS:
-
Hong Kong Fine Motor Test for the School-aged
- IPC:
-
Inferior parietal cortex
- MTdiff:
-
Movement time difference
- ROI:
-
Region of interest
- SPC:
-
Superior parietal cortex
- TD:
-
Typical development
- ΔHbO:
-
Concentration change of oxyhemoglobin concentration
- ΔHbR:
-
Concentration change of deoxyhemoglobin concentration
References
Gaveau V, Pisella L, Priot A-E, Fukui T, Rossetti Y, Pélisson D, et al. Automatic online control of motor adjustments in reaching and grasping. Neuropsychologia. 2014;55:25–40.
Adams IL, Lust JM, Wilson PH, Steenbergen B. Testing predictive control of movement in children with developmental coordination disorder using converging operations. Br J Psychol. 2017;108(1):73–90.
Hyde C, Wilson PH. Dissecting online control in developmental coordination disorder: a kinematic analysis of double-step reaching. Brain Cogn. 2011;75(3):232–41.
Ruddock S, Piek J, Sugden D, Morris S, Hyde C, Caeyenberghs K, et al. Coupling online control and inhibitory systems in children with developmental coordination disorder: goal-directed reaching. Res Dev Disabil. 2015;36:244–55.
Zwicker JG, Missiuna C, Harris SR, Boyd LA. Developmental coordination disorder: a review and update. Eur J Paediatr Neurol. 2012;16(6):573–81.
Bo J, Lee C-M. Motor skill learning in children with developmental coordination disorder. Res Dev Disabil. 2013;34(6):2047–55.
Wilson PH, Ruddock S, Smits-Engelsman B, Polatajko H, Blank R. Understanding performance deficits in developmental coordination disorder: a meta-analysis of recent research. Dev Med Child Neurol. 2013;55(3):217–28.
Hyde C, Wilson PH. Online motor control in children with developmental coordination disorder: chronometric analysis of double-step reaching performance. Child Care Health Dev. 2011;37(1):111–22.
Plumb MS, Wilson AD, Mulroue A, Brockman A, Williams JH, Mon-Williams M. Online corrections in children with and without DCD. Hum Mov Sci. 2008;27(5):695–704.
Fuelscher I, Williams J, Enticott PG, Hyde C. Reduced motor imagery efficiency is associated with online control difficulties in children with probable developmental coordination disorder. Res Dev Disabil. 2015;45:239–52.
Ruddock S, Caeyenberghs K, Piek J, Sugden D, Hyde C, Morris S, et al. Coupling of online control and inhibitory systems in children with atypical motor development: a growth curve modelling study. Brain Cogn. 2016;109:84–95.
Wilmut K, Wann J, Brown J. Problems in the coupling of eye and hand in the sequential movements of children with developmental coordination disorder. Child Care Health Dev. 2006;32(6):665–78.
Boas DA, Elwell CE, Ferrari M, Taga G. Twenty years of functional near-infrared spectroscopy: introduction for the special issue. London: Elsevier; 2014. p. 1–5.
Caçola P, Getchell N, Srinivasan D, Alexandrakis G, Liu H. Cortical activity in fine-motor tasks in children with developmental coordination disorder: a preliminary fNIRS study. Int J Dev Neurosci. 2018;65:83–90.
Hyde C, Fuelscher I, Williams J. Neurophysiological approaches to understanding motor control in DCD: current trends and future directions. Curr Dev Disord Rep. 2019;6:78–86.
Kawato M, Wolpert D. Internal models for motor control. Sens Guid Mov. 1998;218:291–307.
Kawato M. Internal models for motor control and trajectory planning. Curr Opin Neurobiol. 1999;9(6):718–27.
Shadmehr R, Smith MA, Krakauer JW. Error correction, sensory prediction, and adaptation in motor control. Annu Rev Neurosci. 2010;33(1):89–108.
Hyde CE, Wilson PH. Impaired online control in children with developmental coordination disorder reflects developmental immaturity. Dev Neuropsychol. 2013;38(2):81–97.
Blakemore S-J, Sirigu A. Action prediction in the cerebellum and in the parietal lobe. Exp Brain Res. 2003;153(2):239–45.
Shadmehr R, Krakauer JW. A computational neuroanatomy for motor control. Exp Brain Res. 2008;185(3):359–81.
Zwicker JG, Missiuna C, Harris SR, Boyd LA. Brain activation of children with developmental coordination disorder is different than peers. Pediatrics. 2010;126(3):e678–86.
Zwicker JG, Missiuna C, Harris SR, Boyd LA. Brain activation associated with motor skill practice in children with developmental coordination disorder: an fMRI study. Int J Dev Neurosci. 2011;29(2):145–52.
Kashiwagi M, Iwaki S, Narumi Y, Tamai H, Suzuki S. Parietal dysfunction in developmental coordination disorder: a functional MRI study. NeuroReport. 2009;20(15):1319–24.
Debrabant J, Gheysen F, Caeyenberghs K, Van Waelvelde H, Vingerhoets G. Neural underpinnings of impaired predictive motor timing in children with developmental coordination disorder. Res Dev Disabil. 2013;34(5):1478–87.
Licari MK, Billington J, Reid SL, Wann JP, Elliott CM, Winsor AM, et al. Cortical functioning in children with developmental coordination disorder: a motor overflow study. Exp Brain Res. 2015;233(6):1703–10.
Debrabant J, Vingerhoets G, Van Waelvelde H, Leemans A, Taymans T, Caeyenberghs K. Brain connectomics of visual-motor deficits in children with developmental coordination disorder. J Pediatr. 2016;169(21–7): e2.
Kashuk SR, Williams J, Thorpe G, Wilson PH, Egan GF. Diminished motor imagery capability in adults with motor impairment: an fMRI mental rotation study. Behav Brain Res. 2017;334:86–96.
Reynolds JE, Billington J, Kerrigan S, Williams J, Elliott C, Winsor AM, et al. Mirror neuron system activation in children with developmental coordination disorder: a replication functional MRI study. Res Dev Disabil. 2019;84:16–27.
Fuelscher I, Caeyenberghs K, Enticott PG, Williams J, Lum J, Hyde C. Differential activation of brain areas in children with developmental coordination disorder during tasks of manual dexterity: an ALE meta-analysis. Neurosci Biobehav Rev. 2018;86:77–84.
Hong Kong Occupational Therapy Association. Fine motor test for the school-aged manual. Hong Kong: Hong Kong Occupational Therapy Association Limited; 2021.
Aasted CM, Yücel MA, Cooper RJ, Dubb J, Tsuzuki D, Becerra L, et al. Anatomical guidance for functional near-infrared spectroscopy: AtlasViewer tutorial. Neurophotonics. 2015;2(2): 020801.
Huppert TJ, Diamond SG, Franceschini MA, Boas DA. HomER: a review of time-series analysis methods for near-infrared spectroscopy of the brain. Appl Opt. 2009;48(10):D280–D98
Hu X-S, Arredondo MM, Gomba M, Confer N, DaSilva AF, Johnson TD, et al. Comparison of motion correction techniques applied to functional near-infrared spectroscopy data from children. J Biomed Opt. 2015;20(12): 126003.
Strangman G, Culver JP, Thompson JH, Boas DA. A quantitative comparison of simultaneous BOLD fMRI and NIRS recordings during functional brain activation. Neuroimage. 2002;17(2):719–31.
Aarabi A, Osharina V, Wallois F. Effect of confounding variables on hemodynamic response function estimation using averaging and deconvolution analysis: an event-related NIRS study. Neuroimage. 2017;155:25–49.
Leff DR, Orihuela-Espina F, Elwell CE, Athanasiou T, Delpy DT, Darzi AW, et al. Assessment of the cerebral cortex during motor task behaviours in adults: a systematic review of functional near infrared spectroscopy (fNIRS) studies. Neuroimage. 2011;54(4):2922–36.
Xia M, Wang J, He Y. BrainNet viewer: a network visualization tool for human brain connectomics. PLoS ONE. 2013;8(7): e68910.
Battaglia-Mayer A, Ferrari-Toniolo S, Visco-Comandini F, Archambault PS, Saberi-Moghadam S, Caminiti R. Impairment of online control of hand and eye movements in a monkey model of optic ataxia. Cereb Cortex. 2013;23(11):2644–56.
Macuga KL, Frey SH. Differential contributions of the superior and inferior parietal cortex to feedback versus feedforward control of tools. Neuroimage. 2014;92:36–45.
Archambault P, Ferrari-Toniolo S, Caminiti R, Battaglia-Mayer A. Visually-guided correction of hand reaching movements: the neurophysiological bases in the cerebral cortex. Vis Res. 2015;110:244–56.
Glover S. Separate visual representations in the planning and control of action. Behav Brain Sci. 2004;27(1):3–24.
Kraeutner SN, El-Serafi M, Lee J, Boe SG. Disruption of motor imagery performance following inhibition of the left inferior parietal lobe. Neuropsychologia. 2019;127:106–12.
van Elk M. The left inferior parietal lobe represents stored hand-postures for object use and action prediction. Front Psychol. 2014;5:333.
Archambault PS, Caminiti R, Battaglia-Mayer A. Cortical mechanisms for online control of hand movement trajectory: the role of the posterior parietal cortex. Cereb Cortex. 2009;19(12):2848–64.
Gréa H, Pisella L, Rossetti Y, Desmurget M, Tilikete C, Grafton S, et al. A lesion of the posterior parietal cortex disrupts on-line adjustments during aiming movements. Neuropsychologia. 2002;40(13):2471–80.
Ito M. Control of mental activities by internal models in the cerebellum. Nat Rev Neurosci. 2008;9(4):304–13.
Yücel MA, Lühmann AV, Scholkmann F, Gervain J, Dan I, Ayaz H, et al. Best practices for fNIRS publications. Neurophotonics. 2021;8(1): 012101.
Acknowledgements
The authors acknowledge all the children and their parents for their participation in this study. We also express our sincere thanks to the undergraduate occupational therapy students for their work in carrying out clinical assessments for participant screening.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Author information
Authors and Affiliations
Contributions
Q.H. contributed to the conception and design of the work, the acquisition, analysis, and interpretation of data, and also drafted and revised the main text as well as created all figures and tables. M.Y. contributed to the interpretation of data and revised the paper. K.F. contributed to the conception of the work and revised the paper. C.C. contributed to the conception and design of the work, and revised the paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the review board of the Hong Kong Polytechnic University (HSEARS20210416006-01). Written informed consent from all children or their guardians was obtained before conducting our research.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huang, Q., Yeung, M.K., Fong, K.N.K. et al. Cortical activity during online motor control in children with and without developmental coordination disorder: a cross-sectional functional near-infrared spectroscopy study. J NeuroEngineering Rehabil 21, 160 (2024). https://doi.org/10.1186/s12984-024-01465-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12984-024-01465-z