
Abstract
Background
Major Depressive Disorder (MDD) is associated with interoceptive deficits expressed throughout the body, particularly the facial musculature. According to the facial feedback hypothesis, afferent feedback from the facial muscles suffices to alter the emotional experience. Thus, manipulating the facial muscles could provide a new “mind-body” intervention for MDD. This article provides a conceptual overview of functional electrical stimulation (FES), a novel neuromodulation-based treatment modality that can be potentially used in the treatment of disorders of disrupted brain connectivity, such as MDD.
Methods
A focused literature search was performed for clinical studies of FES as a modulatory treatment for mood symptoms. The literature is reviewed in a narrative format, integrating theories of emotion, facial expression, and MDD.
Results
A rich body of literature on FES supports the notion that peripheral muscle manipulation in patients with stroke or spinal cord injury may enhance central neuroplasticity, restoring lost sensorimotor function. These neuroplastic effects suggest that FES may be a promising innovative intervention for psychiatric disorders of disrupted brain connectivity, such as MDD. Recent pilot data on repetitive FES applied to the facial muscles in healthy participants and patients with MDD show early promise, suggesting that FES may attenuate the negative interoceptive bias associated with MDD by enhancing positive facial feedback. Neurobiologically, the amygdala and nodes of the emotion-to-motor transformation loop may serve as potential neural targets for facial FES in MDD, as they integrate proprioceptive and interoceptive inputs from muscles of facial expression and fine-tune their motor output in line with socio-emotional context.
Conclusions
Manipulating facial muscles may represent a mechanistically novel treatment strategy for MDD and other disorders of disrupted brain connectivity that is worthy of investigation in phase II/III trials.
Similar content being viewed by others

Introduction
Major Depressive Disorder (MDD) is a heterogeneous mental illness with complex and poorly understood pathophysiology, conceptualized as a disorder combining affective, behavioral, and cognitive symptoms [1]. In Western countries, somatic symptoms dominate the symptomatology in about two-thirds of cases [2,3,4]. Clinicians and researchers who have explored the association between depression and somatization have proposed that MDD is a disorder of impaired interoception and disturbed afferent bodily signals [5, 6]. In light of this hypothesis, treatments for MDD targeting disrupted interoceptive inference in emotional states, or “mind-body” interventions, have been under active investigation. Some notable examples include vagus nerve stimulation [7], botulinum toxin A (BONT-A) injections [8], and stellate ganglion block [9]. Another novel intervention based on a similar mechanistic model is functional electrical stimulation (FES), where some preliminary research has demonstrated modulatory effects on mood in healthy participants [10] and patients with MDD [11] when applied to the facial muscles involved in emotional expression.
FES is a neuromuscular stimulation technique that delivers a low-energy electrical current to skeletal muscles, causing them to contract and generate functional and purposeful movement [12]. In the literature, its function is often defined as the activation of neuromuscular units that may or may not be under voluntary control [13]. At the neural level, such activation induces changes in the afferent inputs projecting from those neuromuscular units, leading to the activation of the corresponding circuits within the central nervous system (CNS) [14,15,16,17]. The therapeutic applications of the FES have been extensively researched in stroke [18,19,20] and spinal cord injury (SCI) [21, 22]. FES has been used as a prosthesis to replace lost function and as a form of rehabilitation to retrain function, with the end goal of enabling a patient to execute movement without the assistance of a stimulation device. Furthermore, FES has been successfully used to restore both motor and sensory function [23], with common examples including auditory and visual neuroprostheses to reinstate hearing and vision, respectively.
Recent studies have shown that functional recovery post-FES is accompanied by plasticity in the CNS, increasing activity in regions where the activated muscles are represented topographically [14,15,16,17]. With the mechanisms of neuroplasticity being transdiagnostic [24], this narrative review introduces the basic principles of FES, provides an overview of prevailing clinical applications in psychiatry, and discusses its prospects as a tool for non-invasively altering neural circuits in MDD.
Emotions and facial expressions in depression: four hypotheses
Facial expressions corresponding to six or more emotions (e.g., fear, anger, happiness, sadness, surprise, and disgust) are well-defined and considered universal across cultures [25,26,27]. These expressions can be voluntary (routed through the pyramidal motor system; i.e., motor cortex) or involuntary (routed through the extrapyramidal motor system; i.e., subcortical nuclei) [10]. The latter reflects “genuine” emotional experiences: for example, a voluntary smile without emotional input is produced for social purposes and generally involves only the zygomaticus major muscle, which raises the corners of the lips. In contrast, a spontaneous expression of positive emotion is more likely also to involve the orbicularis oculi muscles, which form “crows-feet” wrinkles at the lateral canthi of the eyes; a combination known as a “Duchenne smile” [28, 29]. Voluntarily generating and purposefully holding a facial expression has been demonstrated to be capable of eliciting a corresponding emotion [30, 31], which suggests that “mind-body” interventions modulating facial expressions may benefit individuals with disorders of disturbed affect, such as MDD.
Electromyographic studies of automatic facial expression highlight the differences between patients with MDD and healthy controls in facial expression changes characterizing particular social situations [32,33,34]. Research investigating facial expressions in MDD points to the attenuation of voluntary smiles produced by the zygomaticus major muscle [35, 36]. Yet, there is no consensus regarding other facial expressions: some studies report an attenuation of the facial musculature associated with negative-valence emotions [32, 36, 37], whereas others report their potentiation [38,39,40]. Possible explanations of these findings stem from four main hypotheses explaining facial behavior in depression: (i) the mood-facilitation hypothesis, (ii) the emotion-context insensitivity hypothesis, (iii) the social risk hypothesis, and (iv) the facial feedback hypothesis.
The mood-facilitation hypothesis states that affective states match the likelihood and intensity of corresponding facial expressions, with depression characterized by potentiated facial expressions in response to negative-valence states and attenuated facial expressions in response to positive-valence states [41, 42]. The emotion-context insensitivity hypothesis, however, postulates that depression is a defensive motivational state of disengagement from the environment; it is directed toward conserving resources by inhibiting overall emotional reactivity, which manifests in attenuated facial expressions [43]. Third, the social risk hypothesis views depression as a reflection on one’s engagement with the social context, particularly with threats of social exclusion [44]. Facial expressions are tailored to the social context (primarily through signaling submission and withdrawal) to protect oneself from anticipated social exclusion in the form of rejection or contempt. Thus, patients with severe depression will likely smile less and display facial expressions associated with scorn. In contrast, those with less severe depression are more likely to show signals indicating that they are willing to affiliate with the social context [34].
Another prominent theory explaining the association between facial expressions and affective states is the facial feedback hypothesis. Rooted in Charles Darwin’s and William James’s early views [45, 46], it posits that facial movement directly influences emotional experience [47]. Specifically, the physiological activation of facial muscles associated with expressions corresponding to specific emotions directly elicits those emotional states, whereas the lack of such activation leads to their suppression or total absence [48]. Different versions of the facial feedback hypothesis argue about the relative importance of facial feedback in the initiation of affective states [49]. The necessity version holds that no emotion can be experienced without facial feedback [50]. On the opposite end, the sufficiency version claims that facial movement alone can elicit an associated emotion [51]. Lastly, the modulation version views the emotional experience as elicited by some external stimulus or cue outside of one’s own facial movements, whereby a signal from facial afferents plays a modulatory role in initiating and maintaining the affective state [52].
A substantial body of work has been devoted to studying the association between facial movements and specific emotions. Human facial movements have been taxonomized by the Facial Action Coding System (FACS), with attempts to systematically categorize the physical manifestation of emotions [53]. The classical approach involves asking participants to generate specific facial expressions and record changes in self-reported emotional experiences [49]. Studies using this approach generally conclude that the induction of smile-related facial expressions leads to enhanced positive affect. In contrast, the inhibition of smile-related expressions through the activation of antagonistic muscle groups leads to its diminution [52, 54,55,56]. A second approach involves the presentation of emotionally charged stimuli and instructing participants to suppress induced facial movements or to constantly maintain neutral facial expressions [49]. This paradigm results in a reported decrease of both positive and negative emotions upon voluntary suppression of facial expressions and bodily movements [57,58,59].
Functional electrical stimulation for major depressive disorder
The neurorehabilitative effects of FES in stroke [18,19,20] and SCI [21, 22], with the associated changes in the plasticity of the CNS [12, 60, 61], raise the possibility that FES could be successfully used to treat psychiatric disorders of disrupted brain connectivity, such as MDD [62]. Peripheral bottom-up activation through sensorimotor channels appears to modulate depression symptoms [63], wherein the amygdala serves as a gateway assigning emotional significance to sensory and motor events [64, 65]. Some notable examples of mood-regulatory effects of sensorimotor systems are depressive symptoms associated with inadequate vision and hearing impairment [66, 67]. Other recognized phenomena include psychomotor agitation and retardation [68, 69], stress- or emotion-induced postural adjustments and gait [70], as well as an ameliorative effect of physical exercise on mood [71].
It is hypothesized that through the activation of the zygomaticus major and orbicularis oculi muscles (Fig. 1), FES may generally upregulate the activity of sensorimotor systems due to the direct effect of electrical stimulation on muscle contraction and increase in muscle tone. In turn, this has the potential to directly facilitate neuroplastic rewiring of the primary and secondary motor cortices and modulate extrapyramidal pathways involved in the generation of involuntary motor expressions of emotions – a physiological mechanism largely informed by neurorehabilitative effects of FES in stroke and SCI [12, 60, 61]. The subcortical nuclei of the extrapyramidal system are tentatively linked to the metacognitive component of facial expressions, bridging patterns of specific motor activity with emotions [72, 73]. Given this perspective, repetitive activation of the zygomaticus major and orbicularis oculi (the “Duchenne smile” muscles) would strengthen the extrapyramidal pathway associated with positive emotions, whereas breaking the habit of activating the procerus and corrugator supercilii “frown” muscles would weaken the extrapyramidal pathway associated with negative emotions. This may lead to mood improvements and could potentially account for restoring perturbed sensorimotor balance responsible for symptoms of psychomotor retardation or agitation. In this section, we review existing evidence concerning the effect of FES on mood modulation and introduce a potential neural pathway that may be targeted by FES.

Bilateral functional electrical stimulation of facial muscles. Cutaneous electrode placement for the functional electrical stimulation of bilateral zygomaticus major and orbicularis oculi muscles for the treatment of major depressive disorder. Created with BioRender.com, RRID:SCR_018361.
Functional electrical stimulation modulates emotions in healthy individuals
Zariffa et al. (2014) conducted a proof-of-concept study with transcutaneous facial FES of the “Duchenne smile” muscles to examine the ability of a single FES session to modulate mood-related effects [10]. They hypothesized that FES might enhance the mood-related effects of voluntarily activating facial muscles with close neural connections to the subcortical nuclei regulating emotions, such as the amygdala. Twelve healthy participants, who received FES and were asked to voluntarily move the target muscles at the time of stimulation, were compared to 12 participants in a control group who performed the same procedure without any stimulation. Study outcomes were the scores on the Positive and Negative Affect Schedule-X (PANAS-X) [74], which asks a participant to rate 60 words or expressions describing feelings on a 1 to 5 scale according to how strongly they feel a particular emotion while completing the assessment. Those who received FES experienced changes on the “determined,” “daring,” “scared,” and “concentrating” base items of the PANAS-X, indicating that those emotions relevant to MDD could potentially be modulated by FES.
Functional electrical stimulation improves symptoms of major depressive disorder
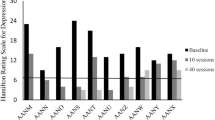
Kapadia et al. (2019) conducted an open-label mixed-methods study on individuals with moderate-to-severe MDD, exploring whether 10 FES sessions would lead to improvements in depressive symptoms [11]. In this study, 10 participants with MDD received FES of the “Duchenne smile” muscles three times per week. Stimulation parameters were 150 µs biphasic pulses (pulse width of the first phase), 60 Hz, with amplitude in the range of 1–15 mA, delivered for 20–25 min [10, 11]. The pulse duration and frequency were chosen during protocol development in the healthy volunteer study [10]. The pulses were asymmetric with a 150 µs leading cathodic phase. The cathode was placed over the muscles’ motor point for muscle activation. Stimulation amplitudes were adjusted at each session such that the targeted muscles achieved visible contractions with no excessive discomfort or unwanted movement (e.g., the closing of the eye). All participants received 10 sessions of FES. Because several study participants requested more FES sessions around the midpoint of the study (after 4–5 participants were already treated), the study protocol was amended to allow up to 40 FES sessions. After the amendment was introduced, the participants were invited to continue therapy for up to 40 sessions if they wished (5 of the 10 participants requested to undergo 40 FES sessions). All participants adhered to the treatment protocol.
The results were promising: participants experienced early improvements in depressive symptoms as measured by the Hamilton Depression Rating Scale (HAM-D) [75] and Inventory of Depressive Symptomology (IDS) [76]. After completing 10 sessions, participants experienced a mean improvement on the HAM-D by 8.1 (SD = 5.3) points (p = .005) and on the IDS by 14.0 (SD = 11.1) points (p = .008) (Fig. 2). Eight participants (80%) showed a reduction of at least 30%, with 5 (50%) showing clinical response (defined as a reduction in the HAM-D by at least 50%) and 6 (60%) entering remission (defined as a HAM-D total score of 7 or below). Reported adverse events were minimal and typically included redness or skin irritation underneath the stimulation site, and muscle soreness or discomfort. FES was well-tolerated, with the potential to be administered with limited clinician oversight.

Functional electrical stimulation improves symptoms of major depressive disorder. Distributions of depression scores measured in participants with major depressive disorder (n = 10) at baseline and after 10 sessions of bilateral functional electrical stimulation (FES) of the zygomaticus major and orbicularis oculi muscles. Both the (A) Hamilton Depression Rating Scale (HAM-D, p = .005); and (B) Inventory of Depressive Symptomatology (IDS, p = .008) scores were significantly reduced post-FES. Created with RAWGraphs 2.0 beta, using the data from Kapadia et al. (2019) [11].
Neurobiological mechanisms and target circuitry: role of the amygdala and emotion-to-motor transformation loop
Although patterns of neural activity corresponding to facial expressions are distributed across multiple facial motor brain areas, the neurons of the amygdala appear to play a key regulatory role. The amygdala functions within the larger network organization of the human brain, sending excitatory signals to the hypothalamic-pituitary-adrenal axis, brainstem, and other limbic structures (e.g., anterior cingulate cortex, anterior insula) and receiving inhibitory projections from ventral striatum and frontal cortex [77]. The amygdala is the structure most robustly engaged in emotional processing [78,79,80]: functional magnetic resonance imaging (fMRI) connectivity studies have identified that it constitutes one of the key nodes within the salience and emotion network – a set of brain regions responsible for integrating sensory information to facilitate the allocation of attention toward significant stimuli, leading to behavioral decisions [64, 65]. Further, cellular studies [81, 82] have shown that an increase in the firing rate of amygdala neurons mainly occurs after the onset of the muscular activity corresponding to the movement of a facial muscle. In a common face processing network, MDD patients exhibit hyperactivation of the amygdala in response to negative stimuli and hypoactivation in response to positive stimuli, which forms mood-congruent processing bias [83].
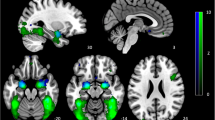
Facial expressions are motor events generated through a sequence of reciprocal transformations between sensory and motor processes informed by interoceptive bodily afferent inputs and extracted socio-emotional significance of perceived signals [81]. Neurons of the amygdala appear to be critical in (i) the sensory monitoring of generated facial expressions, (ii) selecting an appropriate facial expression upon evaluation of the social context, and (iii) being involved in the monitoring of the facial expression of self and others through a proposed mirror neuron system [81, 84, 85]. Moreover, original research [86,87,88,89] and review articles [81, 82] point to the existence of the emotion-to-motor transformation loop (EMTL) - a limbic-motor arc that adjusts facial expressions based on the socio-emotional information coming from the environment (Fig. 3). The amygdala is the central node of EMTL, which receives input, functions as the decision-making processing center, and projects the output [24, 87, 88]. Anatomically, it forms a closed loop with the anterior face area of the midcingulate (M3) and the anterior cingulate cortex [90]. In a feedback manner, neurons of area M3 project back to the basal nuclei of the amygdala, giving rise to further feedback projections to all subdivisions of the cingulate cortex [84, 90, 91]. Other evidence points to the role of interoceptive afferents projecting to the amygdala and area M3 through the insula via the glossopharyngeal and vagus nerves [92, 93]. Therefore, the neurophysiological activity of the facial muscles induced by FES may send patterned proprioceptive and interoceptive bottom-up inputs to the amygdala through the cranial nerves and the brainstem, thus leading to neuroplastic changes in the EMTL.

Emotion-to-motor transformation loop. Contraction of facial muscles relays proprioceptive (magenta) and interoceptive (purple) afferent signals to the amygdala (AMYG) via the trigeminal, glossopharyngeal, and vagus nerves and corresponding brainstem nuclei. AMYG forms a feedback loop with the anterior face area of the midcingulate cortex (M3). The AMYG-M3 connectivity establishes the processing center responsible for decision-making to select and produce a facial expression in response to a particular emotional context. These limbic inputs further calibrate the final motor output of the corticobulbar motor system, where the contraction of the upper (green) and lower (orange) face muscles is modulated via two separate anatomical pathways and the facial nerve. Dashed arrows represent afferent inputs, dotted arrows represent the processing center, and solid arrows represent efferent outputs. Abbreviations: AMYG, amygdala; CN V, cranial nerve V (trigeminal); CN VII, cranial nerve VII (facial); CN IX, cranial nerve IX (glossopharyngeal); CN X, cranial nerve X (vagus); INS, insula; LC, locus coeruleus; LFN, lateral facial nucleus; M1, primary motor cortex; M3, anterior face area of the midcingulate cortex; M4, caudal face area of the midcingulate cortex; MFN, medial facial nucleus; MTN, mesencephalic trigeminal nucleus; NTS, nucleus tractus solitarius; PBN, parabrachial nuclei; PMCvl, ventrolateral regions of the premotor cortex; SMA, supplementary motor area. Created with BioRender.com, RRID:SCR_018361.
With active FES applied to the zygomaticus major and orbicularis oculi “Duchenne smile” muscles, their respective contraction would potentiate proprioceptive and interoceptive afferent signals associated with a genuine smile. The proprioceptive afferents convey signals of the physical state of the agent’s face; whereas interoceptive afferents convey signals of the emotional state of the agent, signals of “social justification” to make a facial expression, and signals of self-awareness of one’s body. These afferent inputs would be relayed to the amygdala via the trigeminal, glossopharyngeal, and vagus nerves and corresponding brainstem nuclei; as well as the insula, in the case of interoceptive afferents. The feedback loop between the amygdala and area M3 establishes the processing center responsible for selecting and producing a facial expression [81, 90, 93,94,95]. These limbic inputs further calibrate the final motor output of the corticobulbar motor system, where the contraction of upper (e.g., orbicularis oculi) and lower face (e.g., zygomaticus major) muscles is modulated via two separate anatomical pathways, involving supplementary motor area (SMA) for the upper face and caudal face area of the midcingulate (M4) and ventrolateral premotor cortex (PMCvl) for the lower face. Motor output modified by the limbic inputs further readjusts the proprioceptive and interoceptive signals that arise from the contracted facial muscles, forming a feedback loop.
Repetitive administration of active FES may thus activate both the upper (i.e., orbicularis oculi) and lower (i.e., zygomaticus major) face muscles, which will induce a sustained “Duchenne smile” experience. Through mechanisms of Hebbian plasticity, enhancement in motor contractility of the orbicularis oculi would upregulate M3 and SMA – parts of the ascending segment of the EMTL that calibrate the motor output to upper face muscles specifically. Moreover, the prolonged experience of the “Duchenne smile” and the associated experience of positive emotions would modify afferent input to the amygdala itself with reduced neuronal activity. Together, these two processes would potentiate the EMTL pathway responsible for the conversion of associated emotional experiences to motor events, leading (through the feedback loop) to amygdala downregulation and increased functional connectivity with the nodes of EMTL and downstream networks.
The existence of EMTL is supported by studies of BONT-A paired with fMRI [48, 96]. In these studies, using BONT-A to induce paralysis of frown muscles interrupted the activity of such circuitry and dampened emotional distress signals associated with frowning in depression [48, 96]. This led to improvements in mood and decreased activity in the amygdala, with baseline activity of the amygdala restored after the paralysis had expired [96]. Evidence from these BONT-A studies supports the notion that depressive symptoms and low mood can be improved in a “bottom-up” fashion by modulating facial muscles through the amygdala circuitry, which is congruent with the neuroplastic effects of FES.
Considerations for future studies
FES of the facial musculature is a novel experimental treatment that requires thorough investigation. To date, two preliminary studies (one in healthy individuals and one in individuals with MDD) yielded positive results regarding both the feasibility and effects of FES as a potential intervention for MDD [10, 11]. Further clinical trials are needed to demonstrate its superiority over placebo and non-inferiority over existing therapies. In regard to studying FES for MDD in future trials, one of the main goals is to optimize the number of sessions and stimulation parameters to target specific neuromuscular units with minimum discomfort and muscle fatigue. Further clinical innovations are required to make FES a more accessible therapy, such as devising a take-home FES system to make it customizable and to enable easy positioning of facial FES electrodes. Other potential avenues of research might include exploring the efficacy of regular physiotherapeutic exercises of the zygomaticus major and orbicularis oculi muscles to treat symptoms of MDD.
Stimulation parameters
Pulse duration, current amplitude, and frequency of FES have been researched extensively and have been recently reviewed for motor retraining in individuals with neurological conditions [12, 18,19,20, 97,98,99,100,101]. For motor rehabilitation, the typically used values for muscles with intact peripheral innervation are pulse duration in the range of 150–400 µs (first phase) and the frequency of 30-50 Hz, while the exact amplitude is typically adjusted on a per-patient basis to produce a functional yet comfortable muscle contraction based on the activated target, stimulation pattern, and total duration of stimulation [10, 11, 21, 97, 101, 102].
Although the goal of motor rehabilitation using FES in individuals with stroke and SCI differs from FES for MDD (motor rehabilitation vs. mood improvements), both focus on the principles of neuroplasticity. FES, combined with a voluntary effort by the participant, results in a successful execution of the desired movement, thereby completing the afferent-efferent loop, which facilitates neuroplastic changes. Based on this hypothesis, FES may strengthen the neural connections in the primary motor cortex and amygdala, leading to improved mood-related symptoms. Preliminary studies from our laboratory have used asymmetric pulses with a 150 µs leading cathodic phase, 1–15 mA amplitude, and 60 Hz pulse frequency to stimulate facial muscles [10, 11]. Although these parameters were well-tolerated by participants, further studies are required to determine the optimal stimulation parameters for facial muscles. Importantly, factors such as the stimulator (e.g., rise time of the stimulation), electrodes, and waveforms may also affect comfort and amplitude of the delivered current required for muscle activation [102, 103].
Dosing, adverse effects, and contraindications
Although significant work has been undertaken to understand the effects of FES in neurorehabilitation, no studies have systematically examined the optimal dosing or adverse events associated with FES. In some studies, a minimum of 20 FES sessions were needed to detect a change in function, and 40 FES sessions were required to see a difference in the quality of life [104]. No significant adverse events have been reported regarding the tolerability and safety of FES. Common mild adverse events include redness underneath the electrodes, which typically dissipates within 24 h, and occasional muscle fatigue or soreness, which also typically resolves within 24 h without intervention [101, 105]. FES has some contraindications, including metal implants at the stimulation site, pacemakers, open wounds or rash at the electrode placement site [101, 106], uncontrolled autonomic dysreflexia [107], and epilepsy [108]. Moreover, target motor neurons have to be accessible for placement of the stimulation electrodes. Finally, the patient must be cognitively able to follow the instructions and actively participate in the therapy process to obtain maximal therapeutic benefits from FES. It is thus expected that adverse events and contraindications for the FES paradigm in MDD would not differ from those characterizing FES in neurorehabilitation, despite anatomical differences in the stimulation site and motor unit size.
Clinical innovations
Whereas pilot studies of FES therapy for MDD are encouraging, potential areas of further innovation have been identified. One of the most important concerns is the accessibility of treatment while preserving compliance. In the pilot studies, participants indicated that coming into the clinic was challenging and suggested that using a device at home would help [11]. A home-based FES device would likely facilitate access to this intervention. One challenge for a home-based FES device, particularly from a research perspective, would be the standardization of training time and electrode positioning [109]. Given the success of the in-person stimulation paradigm, one option would be to start the stimulation at the clinic for educational purposes, followed by virtually supervised home-based stimulation sessions and FES self-administration. A method to facilitate donning the electrodes in the correct positions and keeping them attached to an individual’s face would help with usability and compliance. The design of FES accessories, such as masks with customized locations for compatible novel electrodes, could eliminate the requirement for a physiotherapist to be present at every session and would also prevent the electrodes from falling off during treatment. Importantly, electrode detachment was another issue identified during FES sessions for MDD [11].
One study has demonstrated that home-based administration of another electrical stimulation modality for MDD, specifically the transcranial direct current stimulation (tDCS), was feasible when participants visited the clinic once, followed by 3 virtual sessions to get acquainted with the procedure [110]. Home-administered tDCS improved depressive symptoms; however, it was noted that computer literacy and manual dexterity requirements were limitations. In line with these observations, one recent review stated that appropriate training, the usability of the technique, appropriate ability and skills of the users, and some social interaction were all desirable for the effective use of remote electrical stimulation therapies [111]. To develop FES as a home-administered therapy, tracking the use of the device and facilitating correct electrode placements will be needed. Following the supervised use of the device, logs could be created to track its use either on paper or through mobile applications.
Novel endophenotypes and biomarkers
The optimal frequency and duration of FES treatment required to induce acute response remain unknown, as is the course of positive therapeutic response. To better tailor FES therapy sessions to each participant, future studies shall focus on evaluating specific endophenotypes of MDD that characterize and predict treatment response to FES. One of the approaches could be using the Research Domain Criteria (RDoC) framework [112], with the effects of FES assessed in a pre- and post-treatment fashion on selected metrics corresponding to the 6 functional domains of negative valence, positive valence, cognition, social processes, arousal and regulatory processes, and sensorimotor processes. For instance, RDoC studies could include psychometric, behavioral, neuroimaging, physiological, and molecular metrics to provide mechanistic insight into how FES leads to changes in mood, how the EMTL and its nodes are modulated, and which patients may benefit from FES. In the long run, predictive biomarkers would facilitate the development of preventive FES therapy with optimal duration and frequency that patients could self-deliver at home. It would also prompt a better understanding of the progression of MDD post-FES, leading to personalized FES therapies.
Conclusions
Rooted in facial feedback and neuroplasticity theories, FES is a promising novel intervention for MDD with established safety, feasibility, and practicality. This narrative review summarizes a theoretical foundation behind the link between facial expressions and depression, reviewing evidence supporting the use of repetitive FES for MDD and its putative mechanisms of action. The use of FES for MDD is supported by feasibility and preliminary positive results. However, this area of research now requires the design and development of further phase II/III clinical trials that would focus on comparing its superiority over placebo (e.g., sham FES) and non-inferiority over other interventions. If proven efficacious, transcutaneous facial FES therapy could offer an alternative neuromodulation-based treatment modality for MDD or other psychiatric disorders of disrupted brain connectivity, which would pose a minimal-to-no risk of adverse effects and would be easy to administer.
Data availability
Not applicable to this review article as no datasets were generated or analyzed.
Abbreviations
- AMYG:
-
Amygdala
- CN IX:
-
Cranial nerve IX (glossopharyngeal)
- CN V:
-
Cranial nerve V (trigeminal)
- CN VII:
-
Cranial nerve VII (facial)
- CN X:
-
Cranial nerve X (vagus)
- CNS:
-
Central nervous system
- FES:
-
Functional electrical stimulation
- fMRI:
-
Functional magnetic resonance imaging
- HAM-D:
-
Hamilton Depression Rating Scale
- IDS:
-
Inventory of Depressive Symptomatology
- INS:
-
Insula
- LC:
-
Locus coeruleus
- LFC:
-
Lateral facial nucleus
- M1:
-
Primary motor cortex
- M3:
-
Anterior face area of the midcingulate cortex
- M4:
-
Caudal face area of the midcingulate cortex
- MDD:
-
Major depressive disorder
- MFN:
-
Medial facial nucleus
- MTN:
-
Mesencephalic trigeminal nucleus
- NTS:
-
Nucleus tractus solitarius
- PANAS-X:
-
Positive and Negative Affect Schedule-X
- PBN:
-
Parabrachial nuclei
- PMCvl:
-
Ventrolateral regions of the premotor cortex
- RDoC:
-
Research Domain Criteria
- SCI:
-
Spinal cord injury
- SMA:
-
Supplementary motor area
- tDCS:
-
Transcranial direct current stimulation
References
Kennedy SH. Core symptoms of major depressive disorder: relevance to diagnosis and treatment. Dialog Clin Neurosci. 2008;10:271–7.
Tylee A, Gandhi P. The importance of somatic symptoms in depression in primary care. Prim Care Companion J Clin Psychiatry. 2005;7:167–76.
Kirmayer LJ, Robbins JM, Dworkind M, Yaffe MJ. Somatization and the recognition of depression and anxiety in primary care. AJP. 1993;150:734–41.
Simon GE, VonKorff M, Piccinelli M, Fullerton C, Ormel J. An International Study of the relation between somatic symptoms and Depression. N Engl J Med. 1999;341:1329–35.
Khalsa SS, Lapidus RC. Can Interoception Improve the Pragmatic Search for Biomarkers in Psychiatry? Front Psychiatry. 2016;7.
Eggart M, Lange A, Binser M, Queri S, Müller-Oerlinghausen B. Major depressive disorder is Associated with impaired interoceptive accuracy: a systematic review. Brain Sci. 2019;9:131.
Lv H, Zhao Y, Chen J, Wang D, Chen H. Vagus nerve stimulation for Depression: a systematic review. Front Psychol. 2019;10:64.
Arnone D, Galadari H, Rodgers CJ, Östlundh L, Aziz KA, Stip E, et al. Efficacy of onabotulinumtoxinA in the treatment of unipolar major depression: systematic review, meta-analysis and meta-regression analyses of double-blind randomised controlled trials. J Psychopharmacol. 2021;35:910–8.
Kerzner J, Liu H, Demchenko I, Sussman D, Wijeysundera DN, Kennedy SH, et al. Stellate Ganglion Block for Psychiatric Disorders: a systematic review of the Clinical Research Landscape. Chronic Stress. 2021;5:247054702110551.
Zariffa J, Hitzig SL, Popovic MR. Neuromodulation of emotion using functional Electrical Stimulation Applied to facial muscles. Neuromodulation: Technol Neural Interface. 2014;17:85–92.
Kapadia N, Zivanovic V, Moineau B, Downar J, Zariffa J, Popovic MR. Functional electrical stimulation of the facial muscles to improve symptoms in individuals with major depressive disorder: pilot feasibility study. BioMed Eng OnLine. 2019;18:109.
Marquez-Chin C, Popovic MR. Functional electrical stimulation therapy for restoration of motor function after spinal cord injury and stroke: a review. BioMed Eng OnLine. 2020;19:34.
Kralj A, Vodovnik L. Functional electrical stimulation of the extremities: part 1. J Med Eng Technol. 1977;1:12–5.
Furlan JC, Pakosh M, Craven BC, Popovic MR. Insights on the potential mechanisms of Action of Functional Electrical Stimulation Therapy in Combination with Task-Specific training: a scoping review. Neuromodulation: Technology at the Neural Interface; 2022. p. 1094715922002884.
Field-Fote EC. Electrical Stimulation Modifies Spinal and Cortical Neural Circuitry: Exercise and Sport Sciences Reviews. 2004;:155–60.
Kimberley TJ, Lewis SM, Auerbach EJ, Dorsey LL, Lojovich JM, Carey JR. Electrical stimulation driving functional improvements and cortical changes in subjects with stroke. Exp Brain Res. 2004;154:450–60.
Beaumont E, Guevara E, Dubeau S, Lesage F, Nagai M, Popovic M. Functional electrical stimulation post-spinal cord injury improves locomotion and increases afferent input into the central nervous system in rats. J Spinal Cord Med. 2014;37:93–100.
Howlett OA, Lannin NA, Ada L, McKinstry C. Functional electrical stimulation improves activity after stroke: a systematic review with Meta-analysis. Arch Phys Med Rehabil. 2015;96:934–43.
Eraifej J, Clark W, France B, Desando S, Moore D. Effectiveness of upper limb functional electrical stimulation after stroke for the improvement of activities of daily living and motor function: a systematic review and meta-analysis. Syst Rev. 2017;6:40.
Nascimento LR, da Silva LA, Araújo Barcellos JVM, Teixeira-Salmela LF. Ankle-foot orthoses and continuous functional electrical stimulation improve walking speed after stroke: a systematic review and meta-analyses of randomized controlled trials. Physiotherapy. 2020;109:43–53.
Luo S, Xu H, Zuo Y, Liu X, All AH. A review of functional electrical stimulation treatment in spinal cord Injury. Neuromol Med. 2020;22:447–63.
Alashram AR, Annino G, Mercuri NB. Changes in spasticity following functional electrical stimulation cycling in patients with spinal cord injury: a systematic review. J Spinal Cord Med. 2022;45:10–23.
Peckham PH, Knutson JS. Functional electrical stimulation for neuromuscular applications. Annu Rev Biomed Eng. 2005;7:327–60.
Price RB, Duman R. Neuroplasticity in cognitive and psychological mechanisms of depression: an integrative model. Mol Psychiatry. 2020;25:530–43.
Ekman P, Friesen WV. Unmasking the face: a guide to recognizing emotions from facial clues. Oxford, England: Prentice-Hall; 1975.
Ekman P, Cordaro D. What is meant by calling Emotions Basic. Emot Rev. 2011;3:364–70.
Cowen AS, Keltner D, Schroff F, Jou B, Adam H, Prasad G. Sixteen facial expressions occur in similar contexts worldwide. Nature. 2021;589:251–7.
Ekman P, Davidson RJ, Friesen WV. The Duchenne smile: emotional expression and brain physiology. II. J Pers Soc Psychol. 1990;58:342–53.
Messinger DS, Fogel A, Dickson KL. All smiles are positive, but some smiles are more positive than others. Dev Psychol. 2001;37:642–53.
Wiswede D, Münte TF, Krämer UM, Rüsseler J. Embodied emotion modulates neural signature of performance monitoring. PLoS ONE. 2009;4:e5754.
Ekman P, Davidson RJ. Voluntary smiling changes Regional Brain Activity. Psychol Sci. 1993;4:342–5.
Gehricke J-G, Shapiro D. Reduced facial expression and social context in major depression: discrepancies between facial muscle activity and self-reported emotion. Psychiatry Res. 2000;95:157–67.
Schwartz GE, Fair PL, Salt P, Mandel MR, Klerman GL. Facial expression and imagery in Depression: an Electromyographic Study. Psychosom Med. 1976;38:337–47.
Girard JM, Cohn JF, Mahoor MH, Mavadati S, Rosenwald DP. Social risk and depression: Evidence from manual and automatic facial expression analysis. In: 2013 10th IEEE International Conference and Workshops on Automatic Face and Gesture Recognition (FG). Shanghai, China: IEEE; 2013. p. 1–8.
Gaebel W, W�lwer W. Facial expressivity in the course of schizophrenia and depression. Eur Archives Psychiatry Clin Neurosciences. 2004;254.
Trémeau F, Malaspina D, Duval F, Corrêa H, Hager-Budny M, Coin-Bariou L, et al. Facial expressiveness in patients with Schizophrenia compared to depressed patients and nonpatient comparison subjects. AJP. 2005;162:92–101.
Berenbaum H, Oltmanns TF. Emotional experience and expression in schizophrenia and depression. J Abnorm Psychol. 1992;101:37–44.
Brozgold AZ, Borod JC, Martin CC, Pick LH, Alpert M, Welkowitz J. Social Functioning and Facial Emotional expression in Neurological and Psychiatric Disorders. Appl Neuropsychol. 1998;5:15–23.
Schwartz GE, Fair PL, Salt P, Mandel MR, Klerman GL. Facial muscle patterning to affective imagery in depressed and nondepressed subjects. Science. 1976;192:489–91.
Girard JM, Cohn JF, Mahoor MH, Mavadati SM, Hammal Z, Rosenwald DP. Nonverbal social withdrawal in depression: evidence from manual and automatic analyses. Image Vis Comput. 2014;32:641–7.
Rosenberg EL. Levels of analysis and the Organization of Affect. Rev Gen Psychol. 1998;2:247–70.
Watson D, Clark LA, Carey G. Positive and negative affectivity and their relation to anxiety and depressive disorders. J Abnorm Psychol. 1988;97:346–53.
Rottenberg J, Gross JJ, Gotlib IH. Emotion context insensitivity in major depressive disorder. J Abnorm Psychol. 2005;114:627–39.
Allen NB, Badcock PBT. The Social Risk Hypothesis of Depressed Mood: Evolutionary, Psychosocial, and neurobiological perspectives. Psychol Bull. 2003;129:887–913.
Darwin C. The expression of the emotions in man and animals. London: John Murray; 1872.
James W. The principles of psychology. Henry Holt and Company; 1913.
Tourangeau R, Ellsworth PC. The role of facial response in the experience of emotion. J Personal Soc Psychol. 1979;37:1519–31.
Hennenlotter A, Dresel C, Castrop F, Ceballos-Baumann AO, Wohlschläger AM, Haslinger B. The link between facial feedback and neural activity within central circuitries of emotion—new Insights from Botulinum Toxin–Induced Denervation of Frown muscles. Cereb Cortex. 2009;19:537–42.
Davis JI, Senghas A, Ochsner KN. How does facial feedback modulate emotional experience? J Res Pers. 2009;43:822–9.
Keillor JM, Barrett AM, Crucian GP, Kortenkamp S, Heilman KM. Emotional experience and perception in the absence of facial feedback. J Int Neuropsychol Soc. 2002;8:130–5.
Ekman P, Levenson RW, Friesen WV. Autonomic nervous system activity distinguishes among emotions. Science. 1983;221:1208–10.
Strack F, Martin LL, Stepper S. Inhibiting and facilitating conditions of the human smile: a nonobtrusive test of the facial feedback hypothesis. J Personal Soc Psychol. 1988;54:768–77.
Ekman P, Friesen W. Facial action coding system: a technique for the measurement of Facial Movement. Palo Alto, CA: Consulting Psychologists Press; 1978.
Soussignan R. Duchenne smile, emotional experience, and autonomic reactivity: a test of the facial feedback hypothesis. Emotion. 2002;2:52–74.
Matsumoto D. The role of facial response in the experience of emotion: more methodological problems and a meta-analysis. J Personal Soc Psychol. 1987;52:769–74.
Adelmann PK, Zajonc RB. Facial efference and the experience of emotion. Annu Rev Psychol. 1989;40:249–80.
Duclos SE, Laird JD. The deliberate control of emotional experience through control of expressions. Cogn Emot. 2001;15:27–56.
Bush LK, Barr CL, McHugo GJ, Lanzetta JT. The effects of facial control and facial mimicry on subjective reactions to comedy routines. Motiv Emot. 1989;13:31–52.
McCanne TR, Anderson JA. Emotional responding following experimental manipulation of facial electromyographic activity. J Personal Soc Psychol. 1987;52:759–68.
Karamian BA, Siegel N, Nourie B, Serruya MD, Heary RF, Harrop JS, et al. The role of electrical stimulation for rehabilitation and regeneration after spinal cord injury. J Orthop Traumatol. 2022;23:2.
Grahn PJ, Lavrov IA, Sayenko DG, Van Straaten MG, Gill ML, Strommen JA et al. Enabling Task-Specific Volitional Motor Functions via Spinal Cord Neuromodulation in a Human With Paraplegia. Mayo Clinic Proceedings. 2017;92:544–54.
Zhang J, Wang J, Wu Q, Kuang W, Huang X, He Y, et al. Disrupted brain connectivity networks in Drug-Naive, first-episode major depressive disorder. Biol Psychiatry. 2011;70:334–42.
Canbeyli R. Sensorimotor Modulation of Mood and Depression: In Search of an Optimal Mode of Stimulation. Front Hum Neurosci. 2013;7.
Geng H, Li X, Chen J, Li X, Gu R. Decreased Intra- and Inter-Salience Network Functional Connectivity is Related to Trait Anxiety in Adolescents. Front Behav Neurosci. 2016;9.
Jenkins LM, Stange JP, Barba A, DelDonno SR, Kling LR, Briceño EM, et al. Integrated cross-network connectivity of amygdala, insula, and subgenual cingulate associated with facial emotion perception in healthy controls and remitted major depressive disorder. Cogn Affect Behav Neurosci. 2017;17:1242–54.
Hackenberg B, Döge J, O’Brien K, Bohnert A, Lackner KJ, Beutel ME, et al. Tinnitus and its relation to Depression, anxiety, and Stress—A Population-Based Cohort Study. JCM. 2023;12:1169.
Sabel BA, Wang J, Cárdenas-Morales L, Faiq M, Heim C. Mental stress as consequence and cause of vision loss: the dawn of psychosomatic ophthalmology for preventive and personalized medicine. EPMA J. 2018;9:133–60.
Buyukdura JS, McClintock SM, Croarkin PE. Psychomotor retardation in depression: Biological underpinnings, measurement, and treatment. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35:395–409.
Sampogna G, Del Vecchio V, Giallonardo V, Luciano M, Fiorillo A, Diagnosis. Clinical features, and therapeutic implications of agitated Depression. Psychiatr Clin North Am. 2020;43:47–57.
Adkin AL, Carpenter MG. New Insights on emotional contributions to human postural control. Front Neurol. 2018;9:789.
Xie Y, Wu Z, Sun L, Zhou L, Wang G, Xiao L, et al. The Effects and Mechanisms of Exercise on the treatment of Depression. Front Psychiatry. 2021;12:705559.
Loonen AJM, Ivanova SA. Circuits regulating pleasure and happiness: the evolution of reward-seeking and misery-fleeing behavioral mechanisms in vertebrates. Front Neurosci. 2015;9.
Govoni S, Racchi M, Masoero E, Zamboni M, Ferini-Strambi L. Extrapyramidal symptoms and antidepressant drugs: neuropharmacological aspects of a frequent interaction in the elderly. Mol Psychiatry. 2001;6:134–42.
Watson D, Clark LA. The PANAS-X: Manual for the Positive and Negative Affect Schedule-Expanded Form. Ames, IA:University of Iowa.
Hamilton M, A RATING SCALE FOR, DEPRESSION. J Neurol Neurosurg Psychiatry. 1960;23:56–62.
Rush AJ, Gullion CM, Basco MR, Jarrett RB, Trivedi MH. The Inventory of Depressive Symptomatology (IDS): psychometric properties. Psychol Med. 1996;26:477–86.
Yan X, Amygdala. Childhood Adversity and Psychiatric Disorders. In: Ferry B, editor. The Amygdala - A Discrete Multitasking Manager. InTech; 2012.
García-García I, Kube J, Gaebler M, Horstmann A, Villringer A, Neumann J. Neural processing of negative emotional stimuli and the influence of age, sex and task-related characteristics. Neurosci Biobehavioral Reviews. 2016;68:773–93.
Sabatinelli D, Fortune EE, Li Q, Siddiqui A, Krafft C, Oliver WT, et al. Emotional perception: Meta-analyses of face and natural scene processing. NeuroImage. 2011;54:2524–33.
Müller VI, Höhner Y, Eickhoff SB. Influence of task instructions and stimuli on the neural network of face processing: an ALE meta-analysis. Cortex. 2018;103:240–55.
Gothard KM. The amygdalo-motor pathways and the control of facial expressions. Front Neurosci. 2014;8.
Gothard KM, Mosher CP, Zimmerman PE, Putnam PT, Morrow JK, Fuglevand AJ. New perspectives on the neurophysiology of primate amygdala emerging from the study of naturalistic social behaviors. WIREs Cogn Sci. 2018;9.
Stuhrmann A, Suslow T, Dannlowski U. Facial emotion processing in major depression: a systematic review of neuroimaging findings. Biol Mood Anxiety Disord. 2011;1:10.
Gothard KM, Battaglia FP, Erickson CA, Spitler KM, Amaral DG. Neural responses to facial expression and face identity in the Monkey Amygdala. J Neurophysiol. 2007;97:1671–83.
Dapretto M, Davies MS, Pfeifer JH, Scott AA, Sigman M, Bookheimer SY, et al. Understanding emotions in others: mirror neuron dysfunction in children with autism spectrum disorders. Nat Neurosci. 2006;9:28–30.
Aoki S, Smith JB, Li H, Yan X, Igarashi M, Coulon P, et al. An open cortico-basal ganglia loop allows limbic control over motor output via the nigrothalamic pathway. Elife. 2019;8:e49995.
Grèzes J, Valabrègue R, Gholipour B, Chevallier C. A direct amygdala-motor pathway for emotional displays to influence action: a diffusion tensor imaging study: a direct Limbic Motor Anatomical Pathway. Hum Brain Mapp. 2014;35:5974–83.
Rizzo G, Milardi D, Bertino S, Basile GA, Di Mauro D, Calamuneri A, et al. The limbic and Sensorimotor Pathways of the human amygdala: a structural connectivity study. Neuroscience. 2018;385:166–80.
Livneh U, Resnik J, Shohat Y, Paz R. Self-monitoring of social facial expressions in the primate amygdala and cingulate cortex. Proc Natl Acad Sci USA. 2012;109:18956–61.
Morecraft RJ, McNeal DW, Stilwell-Morecraft KS, Gedney M, Ge J, Schroeder CM, et al. Amygdala interconnections with the cingulate motor cortex in the rhesus monkey. J Comp Neurol. 2007;500:134–65.
Amaral DG, Price J, Pitkanen A, Carmichael S. Anatomical organization of the primate amygdaloid complex. The Amygdala: A Functional Analysis. New York, NY:Wiley; 1992. 1–66.
Craig AD. How do you feel? Interoception: the sense of the physiological condition of the body. Nat Rev Neurosci. 2002;3:655–66.
Vogt BA, Pandya DN. Cingulate cortex of the rhesus monkey: II. Cortical afferents. J Comp Neurol. 1987;262:271–89.
Morecraft RJ, Louie JL, Herrick JL, Stilwell-Morecraft KS. Cortical innervation of the facial nucleus in the non-human primate. Brain. 2001;124:176–208.
Morecraft RJ, Stilwell–Morecraft KS, Rossing WR. The motor cortex and facial expression:: New Insights from Neuroscience. Neurologist. 2004;10:235–49.
Kim MJ, Neta M, Davis FC, Ruberry EJ, Dinescu D, Heatherton TF, et al. Botulinum toxin-induced facial muscle paralysis affects amygdala responses to the perception of emotional expressions: preliminary findings from an A-B-A design. Biol Mood Anxiety Disord. 2014;4:11.
Popovic MR, Kapadia N, Zivanovic V, Furlan JC, Craven BC, McGillivray C. Functional electrical stimulation therapy of Voluntary grasping Versus only Conventional Rehabilitation for patients with Subacute Incomplete Tetraplegia: a Randomized Clinical Trial. Neurorehabil Neural Repair. 2011;25:433–42.
Kapadia N, Zivanovic V, Popovic M. Restoring Voluntary grasping function in individuals with incomplete chronic spinal cord Injury: pilot study. Top Spinal Cord Injury Rehabilitation. 2013;19:279–87.
Kapadia NM, Nagai MK, Zivanovic V, Bernstein J, Woodhouse J, Rumney P, et al. Functional electrical stimulation therapy for recovery of reaching and grasping in severe chronic Pediatric Stroke Patients. J Child Neurol. 2014;29:493–9.
Kapadia N, Masani K, Catharine Craven B, Giangregorio LM, Hitzig SL, Richards K, et al. A randomized trial of functional electrical stimulation for walking in incomplete spinal cord injury: Effects on walking competency. J Spinal Cord Med. 2014;37:511–24.
Kapadia N, Moineau B, Popovic MR. Functional electrical stimulation therapy for retraining reaching and grasping after spinal cord Injury and Stroke. Front Neurosci. 2020;14:718.
Baker LL, editor. Neuromuscular electrical stimulation: a practical guide. 4th ed. Downey, CA: Los Amigos Research & Education Institute, Inc; 2000.
Garcia-Garcia MG, Jovanovic LI, Popovic MR. Comparing preference related to comfort in torque-matched muscle contractions between two different types of functional electrical stimulation pulses in able-bodied participants. J Spinal Cord Med. 2021;44:215–24.
Hebert DA, Bowen JM, Ho C, Antunes I, O’Reilly DJ, Bayley M. Examining a new functional electrical stimulation therapy with people with severe upper extremity hemiparesis and chronic stroke: a feasibility study. Br J Occup Therapy. 2017;80:651–9.
Warms CA, Backus D, Rajan S, Bombardier CH, Schomer KG, Burns SP. Adverse events in cardiovascular-related training programs in people with spinal cord injury: a systematic review. J Spinal Cord Med. 2014;37:672–92.
ELECTROPHYSICAL AGENTS - Contraindications And Precautions. An evidence-based Approach to clinical decision making in physical therapy. Physiotherapy Can. 2010;62:1–80.
Ashley EA, Laskin JJ, Olenik LM, Burnham R, Steadward RD, Cumming DC, et al. Evidence of autonomic dysreflexia during functional electrical stimulation in individuals with spinal cord injuries. Spinal Cord. 1993;31:593–605.
Anderson KD, Wilson JR, Korupolu R, Pierce J, Bowen JM, O’Reilly D, et al. Multicentre, single-blind randomised controlled trial comparing MyndMove neuromodulation therapy with conventional therapy in traumatic spinal cord injury: a protocol study. BMJ Open. 2020;10:e039650.
Puls WC, Jarvis JC, Ruck A, Lehmann T, Guntinas-Lichius O, Volk GF. Surface electrical stimulation for facial paralysis is not harmful. Muscle Nerve. 2020;61:347–53.
Alonzo A, Fong J, Ball N, Martin D, Chand N, Loo C. Pilot trial of home-administered transcranial direct current stimulation for the treatment of depression. J Affect Disord. 2019;252:475–83.
Caughlin S, Mehta S, Corriveau H, Eng JJ, Eskes G, Kairy D, et al. Implementing Telerehabilitation after Stroke: Lessons learned from canadian trials. Telemedicine and e-Health. 2020;26:710–9.
Insel T, Cuthbert B, Garvey M, Heinssen R, Pine DS, Quinn K, et al. Research Domain Criteria (RDoC): toward a new classification Framework for Research on Mental Disorders. AJP. 2010;167:748–51.
Acknowledgements
Figures for this article were created with RAWGraphs 2.0 beta (https://app.rawgraphs.io) and BioRender.com, RRID:SCR_018361 (https://biorender.com).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
ID: Conceptualization, Investigation, Methodology, Project administration, Resources, Visualization, Writing – original draft, Writing – review & editing. ND: Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing. SNI: Investigation, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing. FGN: Validation, Writing – review & editing. JZ: Validation, Writing – review & editing. SHK: Validation, Writing – review & editing. NOR: Validation, Writing – review & editing. JFC: Validation, Writing – review & editing. MRP: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Writing – review & editing. BHM: Conceptualization, Investigation, Methodology, Supervision, Validation, Writing – review & editing. VB: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Writing – review & editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
Ilya Demchenko, Naaz Desai, Stephanie N. Iwasa, Fatemeh Gholamali Nezhad, and Nicholas O. Rule declare no conflict of interest. José Zariffa is the patent inventor for functional electrical stimulation to modulate affect (US-9259576-B2; approved on February 16, 2016); the patent belongs to University Health Network; he has received research support from the Natural Sciences and Engineering Research Council of Canada, Craig H. Neilsen Foundation, Heart and Stroke Foundation of Canada, Wings for Life Spinal Cord Research Foundation, Ontario Ministry of Colleges and Universities, and Praxis Spinal Cord Institute. Sidney H. Kennedy has received honoraria or research funds from Abbott, Alkermes, Allergan, Boehringer Ingelheim, Brain Canada, Canadian Institutes of Health Research, Janssen, Lundbeck, Lundbeck Institute, Merck, Ontario Brain Institute, Ontario Research Fund, Otsuka, Pfizer, Servier, Sunovion, Sun Pharmaceuticals, Xian-Janssen, and holds stock in Field Trip Health. Jeffrey F. Cohn reports grants or contracts from National Institutes of Health and National Science Foundation, and royalties/licenses from the University of Pittsburgh. He receives consulting fees from RealEyes, Xtrodes, Skylyte, has a patent approved on image normalization for facial analysis (US11244206), holds a leadership or fiduciary role at IEEE International Conference on Automatic Face and Gesture Recognition and Association for Affective Computing Society, and holds stock in Deliberate AI and Embodied. Milos R. Popovic is the inventor of the patent for facial electrical stimulation to modulate affect belonging to University Health Network, is the Chief Technology Officer and the Director of Myndtec, Inc., a company that manufactures transcutaneous functional electrical stimulators. He is the Director of KITE, Toronto Rehabilitation Institute – University Health Network (Toronto, ON, Canada) and reports grants or contracts from Connaught Innovation Award, Brain Canada, Mitacs, Webster Foundation, Dean Strategic Funding at the University of Toronto, Natural Sciences and Engineering Research Council of Canada, and Canadian Fund for Innovation. He has a patent approved on February 16, 2016 (USA US-9259576-B2) with Dr. S. Hitzig and Dr. J. Zariffa “Functional electrical stimulation method, use and apparatus for mood alteration”; the patent belongs to University Health Network. He is consulting for a company Fourier Intelligence, which designs rehabilitation robotics technologies, and holds stock in MyndTec. Benoit H. Mulsant holds and receives support from the Labatt Family Chair in Biology of Depression in Late-Life Adults at the University of Toronto. He currently receives or has received for the past three years research support from Brain Canada, Canadian Institutes of Health Research, Center for Addiction and Mental Health Foundation, Patient-Centered Outcomes Research Institute, National Institute of Health, Capital Solution Design LLC (software used in a study funded by Center for Addiction and Mental Health Foundation), and HAPPYneuron (software used in a study funded by Brain Canada). He has also been an unpaid consultant to Myriad Neuroscience for the past three years. Venkat Bhat is supported by an Academic Scholar Award from the Department of Psychiatry at the University of Toronto; he has received research support from the Canadian Institutes of Health Research, Brain & Behavior Foundation, Ministry of Health/Ontario Medical Association Innovation Funds, New Frontiers in Research Fund, Department of National Defense (Government of Canada), and an investigator-initiated trial from Roche Canada.
Ethics approval and consent to participate
Not applicable to this review article as no original human data are reported.
Consent for publication
Not applicable to this review article as no original human data are reported.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Demchenko, I., Desai, N., Iwasa, S.N. et al. Manipulating facial musculature with functional electrical stimulation as an intervention for major depressive disorder: a focused search of literature for a proposal. J NeuroEngineering Rehabil 20, 64 (2023). https://doi.org/10.1186/s12984-023-01187-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12984-023-01187-8