
Abstract
Background
Impaired balance during walking is a common problem in people with incomplete spinal cord injury (iSCI). To improve walking capacity, it is crucial to characterize balance control and how it is affected in this population. The foot placement strategy, a dominant mechanism to maintain balance in the mediolateral (ML) direction during walking, can be affected in people with iSCI due to impaired sensorimotor control. This study aimed to determine if the ML foot placement strategy is impaired in people with iSCI compared to healthy controls.
Methods
People with iSCI (n = 28) and healthy controls (n = 19) performed a two-minute walk test at a self-paced walking speed on an instrumented treadmill. Healthy controls performed one extra test at a fixed speed set at 50% of their preferred speed. To study the foot placement strategy of a participant, linear regression was used to predict the ML foot placement based on the ML center of mass position and velocity. The accuracy of the foot placement strategy was evaluated by the root mean square error between the predicted and actual foot placements and was referred to as foot placement deviation. Independent t-tests were performed to compare foot placement deviation of people with iSCI versus healthy controls walking at two different walking speeds.
Results
Foot placement deviation was significantly higher in people with iSCI compared to healthy controls independent of walking speed. Participants with iSCI walking in the self-paced condition exhibited 0.40 cm (51%) and 0.33 cm (38%) higher foot placement deviation compared to healthy controls walking in the self-paced and the fixed-speed 50% condition, respectively.
Conclusions
Higher foot placement deviation in people with iSCI indicates an impaired ML foot placement strategy in individuals with iSCI compared to healthy controls.
Similar content being viewed by others

Background
Impaired balance during walking is a common problem in people with incomplete spinal cord injury (iSCI) [1]. Indeed, individuals with iSCI experience reduced functional ambulation [2] and increased fall risk [3]. Hence, improving dynamic balance is essential to them. Characterizing balance control during walking and how dynamic balance is affected in people with iSCI is crucial for designing and improving effective intervention strategies. However, only few studies have investigated balance control during walking in people with iSCI [4,5,6,7,8,9].
Balance control requires coordination of the center of mass (COM) relative to the base of support (BOS). During walking, the relation between the COM and BOS is typically modulated by a combination of the hip, ankle, and foot placement strategy [10, 11]. Basically, the hip and ankle strategies involve adjustments to the COM by rotating the body around the respective joints [10,11,12]. The foot placement strategy involves adjustments to the BOS by controlling the location and timing of foot placement [10, 11]. The foot placement strategy modulates the relation between the COM and BOS at relatively low actuation costs, because it only requires movement of the swing leg. Consequently, foot placement is the dominant mechanism to maintain balance in the mediolateral (ML) direction during walking in healthy subjects [13, 14].
Literature suggests that ML foot placement is based on COM kinematics [15,16,17,18,19]. This was first observed in simulations, where stable walking was achieved by positioning the foot at a fixed distance lateral to the extrapolated COM (i.e., the COM position adjusted for its velocity) [15]. The relation between ML foot placement and COM kinematics was also observed in experiments investigating foot placement modulation in healthy subjects [16,17,18,19]. For example, in the work of Vlutters et al. [18], healthy subjects showed foot placement adjustments proportional to the ML COM velocity when being perturbed in the ML direction during walking. Furthermore, Wang and Srinivasan [19] showed that ML foot placement can be predicted by the ML COM position and velocity, suggesting that the ML foot placement strategy comprises a strong relation between ML COM kinematics and ML foot placement.
Adjusting foot placement based on COM kinematics requires an adequate estimate of the COM state and sufficient ability to move the swing leg. The COM kinematics must be estimated using visual, vestibular, and proprioceptive information [14], which inputs are used to control the placement of the swing leg, for instance, by modulating the activity of the hip abductor muscles to make step adjustments in the ML direction [20]. Because iSCI potentially affects the afference of sensory information as well as the conduct of efferent neural signals to the muscles [1], it may easily impact the ML foot placement strategy. Indeed, impaired foot placement after spinal cord injury has already been suggested by Day and colleagues [4]. Their results revealed higher variability in ML foot placement relative to the COM position in people with iSCI compared to healthy controls. Moreover, in the study of Arora et al. [7], people with iSCI generated less soleus activation in the swing leg after slip perturbations, suggesting impaired muscle control in balance-challenging conditions. Cornwell et al. [6] examined the effect of walking speed on gait stability and concluded that individuals with iSCI were able to maintain lateral stability when walking at a fast speed, even when their lateral balance was challenged. Furthermore, their results suggested a weaker coordination between COM state and lateral foot placement in people with iSCI compared to healthy controls, implying an impaired ML foot placement strategy. However, they instructed participants to maintain their COM within a narrow target lane, which may yield different results than unrestricted walking. Therefore, more research is necessary to evaluate the ML foot placement strategy in people with iSCI during regular straight walking.
The main purpose of this study was to determine if the ML foot placement strategy is impaired in people with iSCI compared to healthy controls. More specifically, this study investigated the relation between ML COM kinematics and ML foot placement during straight walking in both populations. We hypothesized that the ML foot placement strategy would be impaired in people with iSCI [6].
Methods
Participants
Participants were people with iSCI that had been referred to the GRAIL (gait real-time analysis interactive lab) training by a rehabilitation physician to improve their gait capacity and dynamic balance. Inclusion criteria were: (1) a motor incomplete spinal cord injury with a traumatic or non-traumatic cause (American spinal injury association impairment scale (AIS) C or D), (2) 6 months post injury, (3) ability to walk in a self-paced mode on the GRAIL without using the handrails, and (4) age ≥ 18 years. Subjects were excluded if they had pre-injury impairments of the nervous system, or lower limbs, or any other impairment that might affect balance control. Healthy controls were included if they were 18 years or older without a history of neurological or musculoskeletal problems. The study was approved by the regional medical ethics committee of Arnhem-Nijmegen (2019–5255). All participants provided written informed consent under the Declaration of Helsinki.
Data collection
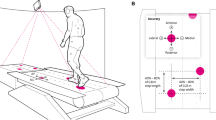
Participants were tested on an instrumented split-belt treadmill (GRAIL, Motek Medical BV, The Netherlands). Kinematic data were acquired using an eight-camera motion capture system (VICON, Oxford, United Kingdom). Reflective markers were placed on 19 anatomical landmarks: 7th cervical vertebra and left and right acromion process, humeral lateral epicondyle, ulnar styloid process, anterior superior iliac spine (ASIS), posterior superior iliac spine (PSIS), femoral lateral epicondyle, lateral malleolus, metatarsal II, and calcaneus. Marker data were sampled at 100 Hz.
Protocol
All participants performed a two-minute walk test (2MWT) at a self-paced speed on the treadmill. The participants with iSCI performed the 2MWT at the start of their first training session. The speed of the belt was adjusted in real-time to the anterior–posterior position and velocity of the pelvis to allow participants to walk at a self-selected walking speed (self-paced mode), which is a suitable alternative to fixed-speed treadmill walking in gait analysis [21, 22]. In the self-paced mode, walking on the front part of the treadmill results in acceleration proportional to the difference between the pelvis position and middle of the belt, and to the velocity of the pelvis. Likewise, walking on the back part of the treadmill results in deceleration. The participants were instructed to walk at a comfortable walking speed. The healthy controls performed one extra 2MWT at a fixed speed equal to 50% of their mean self-paced walking speed (preferred speed) to analyze the effects of walking speed on their ML foot placement strategy, and because this speed was presumed to be similar to the preferred walking speed of the participants with iSCI [23]. A fixed speed was selected because walking in the self-paced mode at 50% of the preferred speed is challenging, and previous research found no significant differences between self-paced and fixed-speed walking [21, 22]. Before the 2MWTs, participants performed one to four one-minute practice rounds to familiarize themselves with walking on the treadmill. To ensure safety, all participants wore a safety harness attached to a rail on the ceiling, without body weight support.
Data analysis
Data were processed using MATLAB (R2019b, MathWorks). The first 20 and last 5 seconds of each 2MWT were excluded from the analysis to remove the start and stop phases. Gaps in the ASIS and PSIS marker data were automatically filled using the rigid body method as previously described [24]. Cubic spline fill was used for the remaining markers when a gap was no more than 10 samples. Marker data were filtered with a 4th order zero-phase low-pass Butterworth filter with a cut-off frequency of 20 Hz.
Hip joint centers were estimated using the regression method reported by Dumas et al. [25]. Marker data and hip joint centers were used to estimate the COM location of nine segments (torso and head, upper leg, lower leg and foot, upper arm, forearm and hand) as described by Tisserand et al. [26]. The whole-body COM location was computed using a weighted sum of the segment COM locations. Gaps in the whole-body COM, resulting from gaps in the marker data, were filled using the pattern fill method as described by Camargo et al. [24]. The average location of the ASIS and PSIS markers was used as the donor pattern.
Marker data of the feet were used to detect gait instances [27]. Heel strike was defined as the instant at which the anterior–posterior velocity of the calcaneus marker reversed with respect to the walking direction. Toe-off was defined as the instant at which the velocity of the metatarsal II marker reversed to the positive walking direction. Step width was defined as the distance between the left and right calcaneus marker at the instant of midstance.
To study the foot placement strategy of a participant, linear regression was used to predict the ML foot placement (FP) based on ML COM position and velocity at heel strike [19, 28,29,30]. We used the following regression equation:
in which \({\beta }_{pos}\) and \({\beta }_{vel}\) are the regression coefficients of the COM position and velocity, respectively, and \(\varepsilon\) the model error. Foot placement was defined as the demeaned ML distance between the left and right calcaneus markers at midstance. The COM position was defined with respect to the calcaneus marker of the stance foot at mid stance, and both predictors were demeaned.
Outcome measures
The accuracy of the foot placement strategy was evaluated by the root mean square error (RMSE) between the predicted and actual foot placements. The RMSE was selected as primary outcome measure and referred to as foot placement deviation.
To confirm adherence to the foot placement strategy, the goodness of the fit of the linear regression model was evaluated with the coefficient of determination (R2), here referred to as foot placement adherence. Substantial adherence to the foot placement strategy was considered when the coefficient of determination was larger than 0.26 [31]. In addition, the within-subject standard deviation (SD) of actual foot placement was determined, because foot placement adherence is influenced by the dispersion of the actual ML foot placement.
Step width was selected as a secondary outcome measure, because wider steps have previously been linked to instability during walking [32, 33] and a reduced foot placement strategy [34].
Statistical analysis
Participant characteristics of both groups were compared with independent t-tests for continuous variables and Chi-square tests for nominal variables. Foot placement deviation of people with iSCI was compared with values obtained from healthy controls at different walking speeds using independent t-tests, whereas a difference in foot placement deviation between different walking speeds in healthy controls was tested with a dependent t-test. Likewise, group differences in foot placement adherence, in the SD of actual foot placement, and in step width were tested with independent t-tests, whereas differences between different walking speeds within the healthy control group were tested with dependent t-tests. We performed the Student's independent t-test when the assumption of homogeneity of variance was met and the Welch's independent t-test when this assumption was not met (resulting in fractional degrees of freedom). When the assumption of normality was violated, non-parametric equivalent tests were performed. The level of significance (α) was adjusted for the number of tests performed (3) and set at 0.017.
Results
Participants
In total, 30 people with iSCI and 19 healthy controls participated. Two persons with iSCI were not included in the analysis due to incomplete marker data, resulting in 28 people with iSCI. Participant characteristics are reported in Table 1. No significant differences in sex and age were found between both groups. The weight and height of the iSCI group were higher compared to controls, but no significant difference in body mass index (BMI) was found between groups (t(45) = 1.94, p = 0.058). Walking speed of the participants with iSCI was significantly lower compared to healthy controls walking in the self-paced (SP) condition (t(41.7) = − 7.35, p < 0.001), but not significantly different from their fixed-speed 50% (FS50) condition (t(32.0) = 1.61, p = 0.116).
Foot placement deviation
The actual ML foot placements and predicted ML foot placements of a representative participant from both groups are shown in Fig. 1. At group level, foot placement deviation of people with iSCI walking in the self-paced condition was higher compared to healthy controls independent of walking speed (SP: t(45) = 5.21, p < 0.001; FS50: t(45) = 4.06, p < 0.001; Fig. 2A, Table 2). Participants with iSCI exhibited 0.40 cm (51%) and 0.33 cm (38%) higher foot placement deviation compared to healthy controls walking in the self-paced and the FS50 condition, respectively. No significant difference in foot placement deviation was found between healthy controls walking in the self-paced and the FS50 condition (z = 2.01, p = 0.044).

Actual mediolateral (ML) foot placement versus predicted ML foot placement of a person with incomplete spinal cord injury (iSCI) walking in the self-paced condition (A) and of a healthy control walking in the self-paced condition (B) and the fixed-speed 50% condition (C). RMSE indicates the root mean square error between the actual and predicted foot placements, referred to as foot placement deviation. R2 indicates the coefficient of determination of the fit, referred to as the foot placement adherence

Raincloud plots of foot placement deviation (RMSE) (A) and foot placement adherence (R2) (B) of people with incomplete spinal cord injury (iSCI) and healthy controls (HC) walking in the self-paced (SP) or fixed-speed 50% (FS50) condition. Dots represent the individual datapoints and bars the mean ± standard deviation (A) or median and 25th and 75th percentile (B). *p < 0.017
Foot placement adherence
All participants except one iSCI participant showed substantial foot placement adherence (R2 ≥ 0.26). At group level, foot placement adherence of people with iSCI was lower compared to healthy controls walking in the self-paced condition (z = 3.62, p < 0.001; Fig. 2B, Table 2), but there was no longer a significant difference when people with iSCI were compared to controls in the FS50 condition (z = − 1.19, p = 0.233). In addition, foot placement adherence was lower in healthy controls walking in the FS50 condition compared to walking in the self-paced condition (z = − 3.67, p < 0.001).
Foot placement variability
No significant difference in the SD of actual foot placement was found between people with iSCI and healthy controls walking in the self-paced condition (t(44.0) = 1.99, p = 0.053; Fig. 3A, Table 2). When compared to healthy controls walking in the FS50 condition, participants with iSCI exhibited 0.88 cm (46%) higher SD of actual foot placement (t(45) = 3.74, p < 0.001). Moreover, healthy controls walking in the self-paced condition exhibited 0.47 cm (25%) higher SD of actual foot placement compared to walking in the FS50 condition (t(18) = 4.18, p < 0.001).

Raincloud plots of the standard deviation (SD) of the actual foot placement (A) and step width (B) of people with incomplete spinal cord injury (iSCI) and healthy controls (HC) walking in the self-paced (SP) or fixed-speed 50% (FS50) condition. Dots represent the individual datapoints and bars the mean ± standard deviation. *p < 0.017
Step width
Step width of people with iSCI was higher compared to healthy controls independent of walking speed (SP: t(40.9) = 5.45, p < 0.001; FS50: t(41.4) = 5.44, p < 0.001; Fig. 3B, Table 2). Participants with iSCI walked with 5.59 cm (44%) and 6.73 cm (59%) wider steps compared to healthy controls walking in the self-paced and the FS50 condition, respectively. No significant difference in step width was found between healthy controls walking in the self-paced condition and the FS50 condition (t(18) = 2.33, p = 0.032).
Discussion
In the current study, we found that—independent of walking speed—the accuracy of the ML foot placement strategy during walking in people with iSCI was reduced compared to healthy controls.
Foot placement deviation
Congruent with our hypothesis, people with iSCI showed significantly higher foot placement deviation compared to healthy controls, indicating an impaired ML foot placement strategy. This finding is in line with the results of Cornwell et al. [6] and Day et al. [4], who found indications of a weaker coordination between COM state and lateral foot placement in individuals with iSCI. An impaired ML foot placement strategy in people with iSCI could be explained by two important underlying mechanisms. The first mechanism is the impaired proprioceptive information from body structures below the lesion level [1] that could impede the estimation of the COM state and the spatial location of the feet. Indeed, changes in ML foot placement during walking have been observed in healthy subjects when proprioceptive information from muscle spindles was manipulated through muscle vibration [35]. The second mechanism is the decreased muscle coordination in people with iSCI [1], which affects the ability to control the swing leg and therefore limits the coordination of foot placement. In line with this notion, previous research observed a smaller magnitude of soleus activation in the swing leg after slip perturbations in people with iSCI compared to healthy controls [7], implying impaired muscle control in balance-challenging conditions. Moreover, decreased coordination of foot placement has been observed in people with stroke performing a hip abduction tracking task [36], suggesting that reduced control of the swing leg may limit coordination between COM movement and foot placement. With the current study, we cannot determine to what extent impaired proprioceptive information and/or decreased muscle coordination underly the impaired foot placement strategy in people with iSCI. Therefore, future research should focus on disentangling the role of both mechanisms on the foot placement strategy, which can help design and optimize interventions for people with iSCI. Nevertheless, current interventions could focus on provoking more lateral COM excursion and velocity to specifically train the coordination between COM kinematics and ML foot placement. Examples of such interventions are perturbation-based balance training [37] or walking adaptability training [38].
Foot placement adherence and variability
All participants except one participant with iSCI showed substantial adherence to the foot placement strategy, indicating that both people with iSCI and healthy controls use the foot placement strategy during walking. People with iSCI had significantly lower foot placement adherence compared to healthy controls walking at a self-paced speed. However, when corrected for walking speed, the significant group difference in foot placement adherence disappeared. It should be acknowledged that foot placement adherence is influenced by the within-subject SD of actual foot placement, i.e., a larger SD of actual foot placement results in larger foot placement adherence. In line with previous research [4], participants with iSCI walking at a self-paced speed showed a significantly larger SD of actual foot placement compared to healthy controls walking at 50% of their preferred speed (see Figs. 1 and 3A). As a result, a valid comparison of foot placement adherence between both groups is hard to make.
Step width
Participants with iSCI had a larger step width compared to healthy controls. Increased step width has previously been linked to instability during walking [32, 33]. Healthy subjects increased step width when perturbed in the ML direction [39] or while walking on a destabilizing surface [40]. In contrast, individuals with iSCI decreased step width when walking stability was increased by external lateral stabilization [9]. Moreover, healthy subjects decreased modulation of foot placement based on the COM state in response to an increased (imposed) step width [34]. These results suggest that wider steps increase postural stability and therefore reduce the demand for accurate foot placement modulation. Therefore, it is likely that people with iSCI increased their step width to improve postural stability, thereby compensating for a decreased foot placement strategy.
Effect of walking speed
The walking speed of the participants with iSCI was significantly lower compared to healthy controls walking in the self-paced condition. Therefore, an effect of walking speed on the foot placement strategy should be considered. Healthy controls showed similar foot placement deviation while walking at 50% of their preferred walking speed compared to walking at a self-paced (preferred) speed, suggesting no effect of walking speed on the ML foot placement strategy. In the literature, conflicting results regarding the effect of walking speed on the ML foot placement strategy have been reported. Wang and Srinivasan [19] found no effect of walking speed on the prediction of ML foot placement based on the upper body state. Likewise, Stimpson et al. [41] observed that speed-dependent differences in the ML foot placement strategy largely disappeared at the end of a step. In contrast, Cornwell et al. [6] and van Leeuwen et al. [30] found a stronger correlation between COM state and ML foot placement at fast walking speeds. Of note, all studies assessed foot placement adherence (R2) to evaluate the foot placement strategy. As mentioned before, foot placement adherence is influenced by the within-subject SD of actual foot placement. Because this latter parameter increases at faster walking speeds [6, 41, 42], the effect of walking speed on foot placement adherence is hard to extrapolate.
Limitations
Participants with iSCI were included if they were able to walk in a self-paced mode on the GRAIL without using the handrails. This resulted in a group of individuals who were mild to moderately affected. Therefore, the results cannot be generalized to all individuals with iSCI. As a higher impairment level in iSCI potentially affects their sensorimotor control more, it can be expected that the ML foot placement strategy is more severely impaired in individuals with a higher impairment level. Further research is necessary to evaluate the relation between the ML foot placement strategy and the level of impairment in people with iSCI.
Healthy controls walking in the FS50 condition exhibited 0.47 cm lower SD of actual foot placement compared to walking in the self-paced condition. This decrease in SD of actual foot placement when walking in the FS50 condition could be the result of a difference in treadmill mode (i.e., fixed speed versus self-paced). Yet, Sloot et al. [21] showed that step width variability increased with only 1 mm when walking in a fixed-speed mode compared to a self-paced mode. Therefore, we anticipate that the treadmill mode itself had only little effect on the SD of actual foot placement.
Finally, the healthy controls in this study were not sex- or age-matched to the participants with iSCI. Nevertheless, we aimed to include healthy controls in a similar age category as the majority of people with iSCI (age ≥ 45 years) [43]. Furthermore, we found no significant difference in age and sex between both groups.
Conclusion
This study found a higher foot placement deviation in people with iSCI compared to healthy controls independent of walking speed, indicative of an impaired ML foot placement strategy. Moreover, our results suggested that people with iSCI tended to compensate for this decreased foot placement strategy by increasing their step width. Future research should focus on improving the foot placement strategy by targeted balance training.
Availability of data and materials
The data used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AIS:
-
American spinal injury association impairment scale
- ASIS:
-
Anterior superior iliac spine
- BMI:
-
Body mass index
- BOS:
-
Base of support
- COM:
-
Center of mass
- FAC:
-
Functional ambulation categories
- FP:
-
Foot placement
- FS50:
-
Fixed-speed 50%
- GRAIL:
-
Gait real-time analysis interactive lab
- HC:
-
Healthy controls
- iSCI:
-
Incomplete spinal cord injury
- ML:
-
Mediolateral
- RMSE:
-
Root mean square error
- PSIS:
-
Posterior superior iliac spine
- SD:
-
Standard deviation
- SP:
-
Self-paced
- 2MWT:
-
Two-minute walk test
References
Wirz M, van Hedel HJA. Balance, gait, and falls in spinal cord injury. Handb Clin Neurol. 3rd ed. Elsevier; 2018, 367–84.
van Hedel HJA. Gait speed in relation to categories of functional ambulation after spinal cord injury. Neurorehabil Neural Repair. 2009;23:343–50.
Brotherton SS, Krause JS, Nietert PJ. Falls in individuals with incomplete spinal cord injury. Spinal Cord. 2007;45:37–40.
Day KV, Kautz SA, Wu SS, Suter SP, Behrman AL. Foot placement variability as a walking balance mechanism post-spinal cord injury. Clin Biomech. 2012;27:145–50.
Lemay JF, Duclos C, Nadeau S, Gagnon D, Desrosiers É. Postural and dynamic balance while walking in adults with incomplete spinal cord injury. J Electromyogr Kinesiol. 2014;24:739–46.
Cornwell T, Woodward J, Ochs W, Gordon KE. Stabilization strategies for fast walking in challenging environments with incomplete spinal cord injury. Front Rehab Sci. 2021;2:1–14.
Arora T, Musselman KE, Lanovaz JL, Linassi G, Arnold C, Milosavljevic S, et al. Reactive balance responses to an unexpected slip perturbation in individuals with incomplete spinal cord injury. Clin Biomech. 2020;78: 105099.
Ochs WL, Woodward J, Cornwell T, Gordon KE. Meaningful measurements of maneuvers: people with incomplete spinal cord injury ‘step up’ to the challenges of altered stability requirements. J Neuroeng Rehabil. 2021;18:1–13.
Matsubara JH, Wu M, Gordon KE. Metabolic cost of lateral stabilization during walking in people with incomplete spinal cord injury. Gait Posture. 2015;41:646–51.
Reimann H, Fettrow TD, Thompson ED, Agada P, McFadyen BJ, Jeka JJ. Complementary mechanisms for upright balance during walking. PLoS ONE. 2017;12:1–16.
Reimann H, Fettrow T, Jeka JJ. Strategies for the control of balance during locomotion. Kinesiol Rev. 2018;7:18–25.
Blenkinsop GM, Pain MTG, Hiley MJ. Balance control strategies during perturbed and unperturbed balance in standing and handstand. R Soc Open Sci. 2017;4:1–12.
Winter DA. Human balance and posture control during standing and walking. Gait Posture. 1995;3:193–214.
Bruijn SM, van Dieën JH. Control of human gait stability through foot placement. J R Soc Interface. 2018;15:1–11.
Hof AL. The “extrapolated center of mass” concept suggests a simple control of balance in walking. Hum Mov Sci. 2008;27:112–25.
Hof AL, Vermerris SM, Gjaltema WA. Balance responses to lateral perturbations in human treadmill walking. J Exp Biol. 2010;213:2655–64.
Hof AL, van Bockel RM, Schoppen T, Postema K. Control of lateral balance in walking. Experimental findings in normal subjects and above-knee amputees. Gait Posture. 2007;25:250–8.
Vlutters M, van Asseldonk EHF, van der Kooij H. Center of mass velocity-based predictions in balance recovery following pelvis perturbations during human walking. J Exp Biol. 2016;219:1514–23.
Wang Y, Srinivasan M. Stepping in the direction of the fall: the next foot placement can be predicted from current upper body state in steady-state walking. Biol Lett. 2014;10:1–5.
Rankin BL, Buffo SK, Dean JC. A neuromechanical strategy for mediolateral foot placement in walking humans. J Neurophysiol. 2014;112:374–83.
Sloot LH, van der Krogt MM, Harlaar J. Self-paced versus fixed speed treadmill walking. Gait Posture. 2014;39:478–84.
Theunissen K, van Hooren B, Plasqui G, Meijer K. Self-paced and fixed speed treadmill walking yield similar energetics and biomechanics across different speeds. Gait Posture. 2022;92:2–7.
Lapointe R, Lajoie Y, Serresse O, Barbeau H. Functional community ambulation requirements in incomplete spinal cord injured subjects. Spinal Cord. 2001;39:327–35.
Camargo J, Ramanathan A, Csomay-Shanklin N, Young A. Automated gap-filling for marker-based biomechanical motion capture data. Comput Methods Biomech Biomed Engin. 2020;23:1180–9.
Dumas R, Chèze L, Verriest JP. Adjustments to McConville et al. and Young et al. body segment inertial parameters. J Biomech. 2007;40:543–53.
Tisserand R, Robert T, Dumas R, Chèze L. A simplified marker set to define the center of mass for stability analysis in dynamic situations. Gait Posture. 2016;48:64–7.
Zeni JA, Richards JG, Higginson JS. Two simple methods for determining gait events during treadmill and overground walking using kinematic data. Gait Posture. 2008;27:710–4.
Mahaki M, Bruijn SM, van Dieën JH. The effect of external lateral stabilization on the use of foot placement to control mediolateral stability in walking and running. PeerJ. 2019;7(e7939):1–15.
Hoogstad LA, van Leeuwen AM, van Dieën JH, Bruijn SM. Can foot placement during gait be trained? Adaptations in stability control when ankle moments are constrained. J Biomech. 2022;134:1–7.
van Leeuwen AM, van Dieën JH, Daffertshofer A, Bruijn SM. Active foot placement control ensures stable gait: effect of constraints on foot placement and ankle moments. PLoS ONE. 2020;15:1–19.
Cohen J. Multiple regression and correlation analysis. Statistical power analysis for the behavioral sciences. 2nd ed. New York: Lawrence Erlbaum Associates; 1988, 407–65.
van Vugt Y, Stinear J, Claire Davies T, Zhang Y. Postural stability during gait for adults with hereditary spastic paraparesis. J Biomech. 2019;88:12–7.
Hak L, Houdijk H, van der Wurff P, Prins MR, Mert A, Beek PJ, et al. Stepping strategies used by post-stroke individuals to maintain margins of stability during walking. Clin Biomech. 2013;28:1041–8.
Perry JA, Srinivasan M. Walking with wider steps changes foot placement control, increases kinematic variability and does not improve linear stability. R Soc Open Sci. 2017;4:1–9.
Roden-Reynolds DC, Walker MH, Wasserman CR, Dean JC. Hip proprioceptive feedback influences the control of mediolateral stability during human walking. J Neurophysiol. 2015;114:2220–9.
Dean JC, Embry AE, Stimpson KH, Perry LA, Kautz SA. Effects of hip abduction and adduction accuracy on post-stroke gait. Clin Biomech. 2017;44:14–20.
Unger J, Chan K, Lee JW, Craven BC, Mansfield A, Alavinia M, et al. The effect of perturbation-based balance training and conventional intensive balance training on reactive stepping ability in individuals with incomplete spinal cord injury or disease: a randomized clinical trial. Front Neurol. 2021;12:1–13.
van Dijsseldonk RB, de Jong LAF, Groen BE, van der Hulst MV, Geurts ACH, Keijsers NLW. Gait stability training in a virtual environment improves gait and dynamic balance capacity in incomplete spinal cord injury patients. Front Neurol. 2018;9:1–12.
Hak L, Houdijk H, Steenbrink F, Mert A, van der Wurff P, Beek PJ, et al. Speeding up or slowing down?: Gait adaptations to preserve gait stability in response to balance perturbations. Gait Posture. 2012;36:260–4.
Onushko T, Boerger T, van Dehy J, Schmit BD. Dynamic stability and stepping strategies of young healthy adults walking on an oscillating treadmill. PLoS ONE. 2019;14:1–12.
Stimpson KH, Heitkamp LN, Horne JS, Dean JC. Effects of walking speed on the step-by-step control of step width. J Biomech. 2018;68:78–83.
Wu AR, Simpson CS, van Asseldonk EHF, van der Kooij H, Ijspeert AJ. Mechanics of very slow human walking. Sci Rep. 2019;9:1–10.
Toda M, Nakatani E, Omae K, Fukushima M, Chin T. Age-specific characterization of spinal cord injuries over a 19-year period at a Japanese rehabilitation center. PLoS ONE. 2018;13:e095120.
Acknowledgements
The authors would like to thank all participants for their participation and Yara Luijten, Lysanne de Jong, Rosanne van Dijsseldonk, Patrick Koomen, and Ellen Moons for their contribution to data collection.
Funding
This work was supported by the Dutch Research Council (NWO) (P16-05; Wearable Robotics: Exo-Aid for augmenting human physical capacities).
Author information
Authors and Affiliations
Contributions
Design of the study: EZ, EA, NK; data analysis: EZ, EA, NK; writing the first draft: EZ; revision of the first draft: EA, MV, AG, NK. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the regional medical ethics committee of Arnhem-Nijmegen (2019-5255). All participants provided written informed consent under the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zwijgers, E., van Asseldonk, E.H.F., Vos-van der Hulst, M. et al. Impaired foot placement strategy during walking in people with incomplete spinal cord injury. J NeuroEngineering Rehabil 19, 134 (2022). https://doi.org/10.1186/s12984-022-01117-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12984-022-01117-0