
Abstract
Background
The Turkish and Syrian earthquake on February 6th 2023, was one of the deadliest earthquakes in the last decade. It affected approximately 26 million people and left at least 50.000 dead. In this paper, we analyzed the psychological impact and the relationship between mental health factors, earthquake-related experiences and stressors, and resources related to the earthquake, 4 months after the event.
Methods
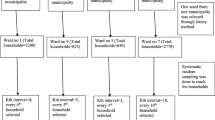
We conducted an analytical cross-sectional study, applying a survey to 320 adults (18–93 years old) in Adiyaman, Turkey. Post-traumatic stress disorder (PTSD) symptoms were assessed using the PC-PTSD, general psychiatric morbidity using the GHQ-12, together with questions focusing on suicidality, drug abuse, as well as experiences, related stressors and received support related to the earthquake.
Results
We found a high prevalence of general mental health symptoms, and of PTSD. Fear of aftershocks and the loss of close family members were found to be risk factors for such symptoms. We didn’t find significant differences in the GHQ or the PC-PTSD scores when considering ethnicity, religion or financial income.
Conclusions
High levels of general mental health symptoms and PTSD symptoms were found 4 months after the earthquake and need to be addressed in all groups, independently from potential religious, social or ethnic backgrounds. The results indicate a large psychiatric and material burden on the entire sample and some priority needs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
On February 6th 2023, a series of large earthquakes hit southeast Turkey and northern Syria, measuring up to 7.8 on the Richter scale. More than 50.000 people died and millions were injured [1]. According to the World Health Organization (WHO), about 26 million people were affected by this disaster, of whom 5.08 million are considered vulnerable, including 1.4 million children [2]. By February 15th 2023 3858 aftershocks were recorded [3]. The earthquakes have affected an area of about 400 km2, including Turkish industrial cities of Gaziantep, Adana and the surrounding cities of Hatay, Malatya, Kilis, Diyarbakir and Adiyaman. After the earthquake, strong aftershocks and extreme winter weather impacted the rescue efforts badly, increasing the physical and psychological burden on the survivors.
While non-man-made disasters, like natural catastrophes, are less likely to cause PTSD symptoms than man-made disasters, the reported prevalence is still very high. (1) Further, even if the earthquake itself was not man-made, it has to be considered, that man-made faults can worsen the situation, e.g. poor early warning systems, injustice treatment of the survivors like unequally distributed aid. When only looking at one-time non-man-made causes for PTSD, earthquakes seem to have a higher incidence for PTSD in survivors than other disasters like strokes or floods [4].
According to the American Psychological Association, Post-Traumatic Stress disorder (PTSD) may affect some people after extremely traumatic events, such as combat situations, terrorist attacks, crimes, accidents, or natural disasters, and usually lasts longer than 30 days after the traumatic event. PTSD symptoms include painful flashbacks, recurrent dreams or nightmare, avoidance of places or activities that recall traumatic experiences, feelings of guilt, a higher physiological arousal which can lead to concentration and memory problems, exaggerated startle responses and sleeping problems [5].
Studies with survivors of earthquakes generally show, that many survivors develop acute or long term stress reactions [6,7,8,9,10]. Five months after the earthquake in Bam, Iran, in December 2006, 58% of the respondents suffered from severe mental health issues as measured by the GHQ-12 [8]. A study four years after the two severe earthquakes in Turkey 1999 found out that 25% of the survivors, who were relocated to other places out of the region, suffered from PTSD and 11% from depression [11], showing that even four years after the disasters and after being relocated to lower-risk areas for earthquakes, the mental health consequences are still high. A meta-analysis including over 46 studies showed a combined incidence of PTSD in survivors of earthquakes of 23.66% [4]. When survivors were diagnosed up until 9 months after the earthquake, the combined incidence was even higher, about 28.76%, after more than 9 months it was 19.48% [4]. However, the included studies were very heterogeneous, describing earthquakes between 4.3 and 9.0 on the Richter scale and reporting PTSD prevalence between 1.20% [12] and 84.8% [13] %.
In most post-earthquake studies female gender, earthquake exposure, loss of family members, lower income, education and damage or loss of house were associated with higher psychological distress [4, 7, 8]. Only some studies also indicated age as a risk factor for PTSD and general psychological morbidity after earthquakes e.g. the 2008 Sichuan (Chinese province) earthquake [14]. Those variables were also predictors of PTSD symptoms severity [7].
Most studies report an increase of suicides after an earthquake [15,16,17], while some found a reduction after natural disasters [18, 19]. Variables like the received support, the severity of the disaster and the social cohesion, as well as the period of the study, might explain the decrease or increase [20, 21].
This highlights the importance of mental health interventions after earthquakes, as untreated mental health problems can increase the risk of suicidal behaviors. However, some survivors may turn to unhealthy coping mechanisms, such as alcohol abuse, to manage their emotional distress.
This is supported by the self-medication hypothesis, which suggests that individuals with mental health conditions, including PTSD, may use substances like alcohol to self-medicate and alleviate their symptoms [22]. Following this line of thought, a study on Italian college students after the L'Aquila earthquake in 2009 found a 43.8% increase in alcohol consumption [23]
The study aimed to primarily collect data on psychological distress in the aftermath of the February 6th 2023 earthquake. At the same time, this study wanted to explore risk factors for developing PTSD and a decrease in psychiatric well-being, as well as to identify protective factors. Assessing this data shortly after the earthquake can help with analyzing problems that need to be addressed in further interventions.
2 Methods
The study was led by the Institute of Psychotherapy and Psychotraumatology at the University of Duhok and the Institute for Transcultural Health Science—Cooperative State University Stuttgart. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects/patients were approved by the Institute for Psychotherapy and Psychotraumatology, University of Dohuk No.I (IPP-07-02-2023). We also received permission from the Turkish Medical Association and the local government to conduct the interviews in the city of Adiyaman.
2.1 Sample
The study sample included 130 male and 180 female participants. The age range was 18 to 93 with M = 41.01 years, SD = 13.01. All participants live in the city of Adiyman in Turkey and experienced the earthquake first-hand. The earthquake of February 6th 2023 measured a magnitude of 7.8 and struck 126 km (78 mi) west-southwest of Adiyaman, the town was heavily affected by the earthquake. Since the February earthquake the town was hit by a lot of smaller quakes [24].
The data was assessed in June 2023, 4 months after the great earthquake. The interviews were conducted by a local team of mental health professionals, including psychologists and social workers, who were also included in the development of the study design. Non-governmental organizations and professionals working in the field helped with reaching out to the participants. The interviews were carried out one-on-one in a face-to-face direction. Since there was no specific location that could be used for the interviews, they were carried out in container cities, tent areas, coffee houses, cafes and restaurants. The interviewers tried to find places that were calm and free of distractions, but sometimes this was not possible due to the conditions. Each interview lasted between 40 and 60 min.
The interviewers are native speakers in Kurdish and Turkish, but all of them speak Turkish. Therefore, the interviewers did the interviews in Turkish. The interviews were carried out after the participants were informed and written consent was given.
2.2 Measures
2.2.1 GHQ-12
We selected the General Health Questionnaire (GHQ-12), which is a well-established instrument promoted by the WHO and many researchers in the field to elicit data on health, especially on different aspects of mental health, and to identify those community members in need of treatment and support (2). The GHQ-12 is a 12-item long, internationally used screening instrument to detect a variation of psychological disorders and stress. It is a valid and reliable instruments across many cultures [25,26,27,28]. The Turkish version exhibits an internal consistency figure of 0.78, with sensitivity and specificity rates standing at 74% and 84% respectively [25, 29]. We used the bi-modal 4-point-GHQ-Scoring (0-0-1-1) for each item, meaning the total scores rank from 0 to 12, with higher scores indicating worse conditions. The conventional 3/4 cut-off for the questionnaire was used to define cases of general psychiatric morbidity [30].
2.2.2 PC-PTSD-5
To screen for PTSD, the Primary Care PTSD Screen for DSM-5 (PC-PTSD-5), developed by the National Center for PTSD, was used [31]. Consisting of 5 yes–no items, it is the shortest, but still reliable established instrument for the identification of those suffering from PTSD symptoms. The Turkish version demonstrates excellent diagnostic accuracy (AUC = 0.941). A score of 3 maximizes sensitivity (κ[1] = 0.93), 4 maximizes efficiency (κ[0.5] = 0.63), and 5 maximizes specificity (κ[0] = 0.70) [32]. The recommended cut-off between 3 and 4 was used to distinguish individuals with a high chance of having PTSD [32].
2.2.3 Earthquake-related experiences
Earthquake-related experiences were evaluated with questions from different inventories from prior earthquakes [23], that were adapted for the current situation. It was asked whether people were trapped or injured during the earthquake, whether they felt like they would die, how many family members and how many other relatives or friends they have lost, if they have lost their place of living (possible answer yes/no, if yes space for an open answer what kind of accommodation they have lost), what their current accommodation is (possible answers: “in a tent”, “no accommodation right now”, “stay with friends or family”, “I continue to stay at home”, “not displaces or able to go back home”, “Other”. The answer “other” had a possibility to fill in a written statement on the kind of accommodation)., how they are currently financed (multiple answers possible: “Work”, “family members”, “savings”, “social assistance”), and if they have gotten any governmental or non-governmental support (multiple answers possible: “governmental”, “non-governmental”, “no”).
Further, it was asked, if they were in need of medical and/or psychological/psychiatric support and whether it was given to them. Possible answers to each of these questions were “yes” and “no”. The question “are you in fear of aftershocks?” was rated with a 5-point Likert scale (0 = not at all, 1 = almost never, 2 = sometimes, 3 = yes, most of the time, 4 = Yes, all the time). At the end, an open question was asked: “What do you need most right now?”.
2.2.4 Suicidality
To assess suicidal ideation and suicide attempts, the question on suicidal ideation from the BDI-II [33] was adapted and asked twice. Once the question referred to the time before the earth level, once to the time of the survey. Further, it was asked about suicide attempts and whether people have, in consequence, asked for help. Again, these questions once referred to the time before and once to the time after the earthquake. And it was asked, whether any family members had attempted suicide.
2.2.5 Drug abuse
Because of the experiences of the psychologist and social workers on site, that many survivors use drugs as a dysfunctional coping mechanism, we have also added additional questions about alcohol and substance abuse and self-medication. Two questions from the The Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV (AUDADIS-IV) are asked that were also used to assess lifetime self-medication with alcohol and drugs in the PTSD section of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) [34]:
“Did you ever drink alcohol to improve your mood or to make yourself feel better when you were having some of these reactions to a stressful event?”
‘‘Did you ever take any drugs or medicine ON YOUR OWN, that is, without a prescription, in greater amounts or more often than prescribed to help improve your mood or make yourself feel better when you were having some of these reactions to a stressful event?’’
As well as four more questions on the increase of different substance use post-earthquake as used by Bianchini et al. [23], asking whether the use of alcohol, tobacco and other substances has increased since the earthquake compared to the time before.
All questions were carefully reviewed and discussed with psychologists and trauma experts from our team in Germany and the local mental health experts in Turkey and Iraq. The local team verified the complete survey and translated the demographic questions and the questions on the earthquake-related experiences.
2.3 Statistical analyses
The PC-PTSD-5 and GHQ-12 were computed according to the manual. Frequencies, percentages and standard deviations were calculated for descriptive data. To assess gender disparities in GHQ and PC-PTSD scores, the Mann–Whitney U-test was employed due to the non-normal distribution of data. Mann–Whitney U-test was also utilized to compare Kurdish and Turkish participants, Sunni and Alevite participants, and individuals who experienced the loss of close family members to those who did not.
To apply the Mann–Whitney U-test for assessing age differences, participants aged up to 50 and those over 50 were divided into groups. To compare the differences between the level of education, individuals who had a high school degree or higher education were compared to individuals without a high school degree.
Multivariate and bivariate logistic regressions were used to identify risk factors for general psychiatric morbidity and PTSD symptoms. Alpha = 0.05 was used as the significance level for all tests.
Data were analyzed using IBM SPSS Statistics 28.0.1.0 (SPSS Inc, Chicago, Ill).
3 Results
The study sample included 130 male and 180 female participants, one person didn’t name their gender. The age range was 18 to 93 with M = 41.01 years, SD = 13.01. Further demographic data can be seen in Table 1. 249 participants answered that they have at least one child, amount ranging from 1 to 11 (M = 3.09, SD = 1.66).
3.1 Characteristics of earthquake experiences
The characteristics of the earthquake experiences can be found in Table 2. Yet, while n = 73 answered that they haven’t lost their home, and n = 241 lost their home. That might be because of the instability and the level of destruction of the houses after the earthquake. Furthermore, n = 255 (81.2%) people answered that they had not lost any close family members. Of those who have lost close family members (n = 59), the amount of losses ranged from 1 to 17, M = 2.86, SD = 2.98). 280 (87.5%) people answered that they have lost other relatives and friends, with amount of lost people ranging from one to n = 300, only n = 19 people answered that they haven’t lost any relatives or friends and n = 15 didn’t give an answer to that question.
To the question “Are you in fear of aftershocks?” 31.3% answered “4 = Yes, all the time”, 32.2% “3 = yes, most of the time”, 18.8% “2 = sometimes”, 17.8% “1 = almost never” and only 2.2% said “0 = not at all”. Showing that 63.5% of the sample is in fear of aftershocks at least most of the time, with a total M = 2.75, SD = 1.12.
In total, n = 76 people said that they needed medical support after the earthquake, and out of those 75.9% (n = 60) said it was given to them. About n = 128 people said they needed psychological/psychiatric help after the earthquake, and out of those (26.56% (n = 34) reported that it was given to them.
3.2 Addiction
On the questions on addiction, no affirmative responses were given regarding self-administration of drugs or medication without a prescription to alleviate mood or cope with reactions to stressful events. Only one person responded that he uses marijuana regularly, and no one responded that they use any of the other illegal drugs regularly (marijuana, bali, thinner, morphine, cocaine, methamphetamine, bonzai, heroin, ecstasy). 46.3% (n = 148) answered that they smoke and out of those 75.86% (n = 110) answered, that their smoking has increased since the earthquake. 41% (n = 41) out of the complete sample said that they drink alcohol at least sometimes and out of those, 31.71% (n = 13) that their drinking has increased since the earthquake.
3.3 Posttraumatic Stress Disorder (PTSD)
Data with missing values were excluded so the answers of n = 314 are considered in the PTSD analysis. Six participants had completed the demographic data, but a number of answers were missing from the psychological test, so we did not include them in the analysis. With a cut-off between 3 and 4, meaning that a sum of 4 or 5 out of 5 is considered a high chance of having PTSD, n = 117 people fulfilled the PTSD criteria at the assessment time. These are 36.9% of the total sample, 35.3% (n = 49) of the men and 38.4% (n = 68) of the women. The total scores of all participants ranged from 0 to 5 with M = 2.83 and SD = 1.46.
3.4 General mental health
For the general mental health analysis missing values were counted as 0, with total scores from the 314 participants ranging from 0 to 12, with M = 5.92 and SD = 3.40, with the threshold between 1 and 2 279 people (87.2%) had a critical level. 263 participants (82.2%) reached a cut-off between 2 and 3.
The expected correlation between the scales was tested. Since they are not normally distributed (Shapiro–Wilk-Test and graphic analysis), Spearman correlation was used. GHQ sum and PC-PTSD scores are correlated strongly (Cohen, 1988), Spearman’s ρ = 0.543, p < 0.001.
3.5 Group differences
There was no statistically significant difference observed between male (n = 139, M = 5.56, SD = 3.58) and female (n = 180, M = 6.19, SD = 3.24) participants in terms of the GHQ scores, U = 11187.00, Z = −1.626, p = 0.104. Similarly, no statistically significant difference in the PC-PTSD scores was found between male (n = 139, M = 2.63, SD = 1.61) and female (n = 177, M = 2.99, SD = 1.31) participants, U = 10852.00, Z = −1.840, p = 0.066.
No statistically significant difference was found in PC-PTSD scores (U = 9564.00, Z = −1.635, p = 0.102) or in GHQ scores (U = 9594.50, Z = −1.876, p = 0.061) between these groups.
The participants age up to 50 (n = 227, M = 2.99, SD = 1.45) showed significantly higher PTSD scores compared to their older counterparts (n = 90, M = 2.44, SD = 1.42), U = 7955.00, Z = −3.143, p = 0.002. However, no significant age-related variation in general psychiatric morbidity was found (U = 10198.00, Z = −0.298, p = 0.766).
In neither of the total sums of the inventories was a significant difference between participants belonging to the Sunnis or the Alevites. Not in the PC-PTSD scores, U = 6069.00, Z = −2.491, p 0 0.013, nor in the GHQ scores, U = 6778.00, Z = −1.553, p = 0.121.
There was no significant difference between a lower education and a higher education (n = 149) in terms of the GHQ scores, U = 12103.00, Z = −0.410, p = 0.675. Nor was there a difference in the PC-PTSD scores, U = 10903.00, Z = −1.673, p = 0.094,
There was a statistically significant difference in PC-PTSD scores between the ones who lost close family (n = 56. M = 3.23, SD = 1.54) and the ones who did not (n = 261, M = 2.75, SD = 1.43), U = 5849.50, Z = −2.398, p = 0.016. There was also a statistically significant difference in the GHQ scores, U = 5446.00, Z = −3.106, p = 0.002).
3.6 Regression analysis
Table 3 shows the risk factors for symptoms of PTSD among the participants. In the bivariate analysis, higher fear of aftershocks, younger age (≤ 50 years) and having lost family members were factors for a higher total PC-PTSD score. Yet, the correlated R2 was very weak. N = 317, R2 = 0.079, corr R2 = 0.071; F (3,313) = 9.001; p < 0.001.
Table 4 shows the risk factors for symptoms of general psychiatric morbidity among the survivors. In the bivariate analysis having lost one or more family members and higher fear of aftershocks were significant risk factors for higher general psychiatric morbidity. Yet, the correlated R2 was very weak, N = 319, R2 = 0.058, corr R2 = 0.052; F (2,317) = 9.701; p < 0.001.
To determine whether PTSD symptoms or general psychiatric morbidity predicted increased suicidal ideation following the earthquake, beyond what was predicted by pre-existing suicidality, a further regression analysis was conducted. Results indicated that PC-PTSD scores did not significantly contribute to this prediction (p > 0.05), while GHQ scores provided additional explanatory value, as depicted in Table 5. Pre-existing suicidal ideation emerged as the strongest predictor for heightened suicidal thoughts post-earthquake.
The answers to the open question " What do you need most right now?” were categorized by two different raters, into the categories of housing, financial support, work, psychological support, medical support, safety, food and/or water, solidarity, clothes/diapers/etc., education/school (for self or children) and “other”. People gave multiple answers. N = 180 (n = 102 male) people have answered that question. The distribution of the answers can be seen in Table 6, R2 = 0.455, corr R2 = 0.451; F (2,308) = 128.52; p < 0.001.
4 Discussion
Our results show that 4 months after the earthquake survivors display a high rate of PTSD symptoms as well as general psychiatric morbidity. Using the stricter cut-off criteria, 36.9% of the sample fulfilled the screening criteria for PTSD. This prevalence is higher than in some other post-earthquake assessments [4]. Comparing it to a meta-analysis on post-traumatic stress disorder among survivors after earthquakes [4] the prevalence is not only higher than the total mean but also higher than the mean of studies up until 9 months after the events. One reason for the higher score might be, that this data here was assessed very shortly after the earthquake.
Even with the stricter cut-off, 82.2% of the sample showed a critical level of general psychiatric morbidity. This is higher than in other studies that also used the GHQ as measurement [8]. With only 45 people of the sample still being able to stay at their homes, 87.5% having lost relatives or friends and 65 having lost close family members, this high psychological burden is explainable.
While 75.9% of those who said they needed medical support received some, only 26.56% percent of those who said they needed psychological/psychiatric support, have received some 4 months after the disaster—confirming that a lot more mental health support is needed in the region.
As expected, the PC-PTSD and the GHQ scores were strongly correlated and therefore not included in the regression analysis. Some of the previously found risk factors were found in this sample as well. In contrast to other studies, we found no difference in GHQ and PC-PTSD based on gender or education level. As reported in many other studies, the loss of close family members was found as a risk factor for both PTSD and general mental health [4]. Further, a higher fear of aftershocks seems to predict traumatic stress and critical psychiatric burden. Since the region has been hit by more earthquakes in 2023 than in many other years, this fear might continue to play an important role in the maintenance of the other symptoms [24]. The continuous earthquakes might make the already difficult reconstruction process even harder and longer. Therefore, it comes with no surprise, that most people answered they needed a safe environment and housing when asked what they wish for most at the moment. Yet, these findings can also be a hint, that people might need support in dealing with their fear of aftershocks to increase their general mental health. But generally, these aftershocks are likely to destabilize the region further.
Further reasons for a higher psychological burden in the aftermath of this earthquake might be that the region was affected by other potentially destabilizing factors even before the earthquake, like the closeness to the Syrian border (refugees from Syria) with the ongoing Kurdish-conflict, the aftermaths of the pandemic and ethnic and religion conflicts.
It is perhaps necessary to mention that the city of Adiyaman, with a population of over 300.000, is located in southeastern Turkey and is home to a majority of Kurds, as well as religious groups such as Alevis and Sunnis. Due to the existing Kurdish conflict, this city was and is again and again a place of ethnic and religious clashes.
While we didn’t find any age differences in the GHQ, the younger survivors scored significantly higher in the PC-PTSD than the elders. Some previous studies found contrary results, after the Sichuan 2008 earthquake elders were found to have a higher risk for PTSD [14]. Yet, other studies did not find any age differences after natural disasters [35, 36] either, and some also found that elders had over time a significant decrease in symptoms compared to a younger group [37]. Their explanation that experiences with previous disasters might help the elderly subjects to deal with the catastrophe might be one explanation for or findings [37].
Contrary to our assumption alcohol or drug abuse has not seem to increase in the aftermath of the event, in total only 13 people said that they increased their alcohol use. Yet, a lot more reported their use of nicotine has increased since the event. Since only a few people in total said that they do drink alcohol in general, cultural, social and religious reasons might explain why there is less alcohol increase than was measured after earthquakes for other reasons [23]. Or maybe people tried to respond socially adapted. Similar findings were made for suicidal ideations, that almost did not change after the earthquake compared to before. As expected, suicidality after the earthquake is mostly explained by suicidal thoughts before the earthquake, while PTSD symptoms and general psychiatric morbidity don’t have an significant impact on the suicidal thoughts so far. These results differ from previous studies, where most report an increase [15,16,17], while others found a decrease [38]. However, it is important to continue to monitor suicidality, as it may well change if the distress continues. This was also shown by a meta-analysis where most studies, that reported an increase in suicidality, were evaluated not right after the natural disaster, but between one to three years later [16]. Further, cultural and religious reasons are likely to explain the lower suicide rates in the region, since suicide is expressly condemned in the Qu'ran, and traditionally Islamic countries have reported fewer suicides compared to Western countries in general [38]. Especially Turkey has reported lower numbers than for example the USA, China or Japan, where other studies on earthquakes and suicidality were made [39].
There were some methodological limitations to this study. Firstly, while all questions were first asked in Turkish, in some interviews the conversations around the questions were held in Kurdish, while others were in Turkish. Yet, since all interviewers are fluent in both languages, this can also be a change since the survivors were given the possibility to answer in their preferred language. This might also have decreased the hesitation of Kurdish participants who otherwise would have had to answer in Turkish. Secondly, besides the information on suicidal ideation no data on past psychiatric illnesses were collected. From the PTSD screening alone, it cannot be said for sure that the PTSD symptoms were due to the earthquake and not in consequence of previous traumatic events. Yet, since the interviewers are mental health professionals, we can assume that they would have noted if people were talking about different events. Since depression is also common in earthquake survivors, another limitation is that no validated measure of depression was used. The GHQ-12 is a general measure of mental health. Our decision to use the GHQ-12 and the PTSD Screening and no further explicit depression or anxiety screening was based on trying to keep the interviews short. Further, many other post-earthquake studies have used the GHQ, which makes our findings easily comparable.
The short time that has passed between the disaster and the interviews can be seen as a strength of this study. With the personal one-on-one interviews with mental health professionals and the open questions leaving space for their own wishes, the survivors were given a chance to use their voice.
Still, another assessment is desirable to see how the mental health of the survivors develops over time, dependent on support, time, and aftershocks. Yet, four years after the two severe earthquakes in Turkey in 1999, 25% of the survivors, who were relocated, suffered from PTSD [11], it is assumed that although the numbers might decrease somewhat over time, a large number of people will still be affected. Especially if the requests for mental health support and a safe environment, which are also evident in the responses to the open questions, are not met.
Unfortunately, we were not able to interview survivors in the Syrian regions in this survey. With war, conflict and displacement, and COVID-19, these Syrian areas have been experiencing ongoing emergencies for about 12 years and have already an overwhelmed health system. According to the WHO, just half of Syrian healthcare facilities were operational before the earthquake [2]. Due to the long-lasting burden even before the earthquake, it can be assumed that the prevalence there will be significantly higher. Therefore, a further survey there would be important.
5 Conclusion
After the catastrophic earthquake in February 2023, the present findings underscore the severe psychological impact on survivors in the affected region. The findings on the housing and work situation, as well as the wishes mentioned in the open question, show that the people affected urgently need further material support to rebuild their existential security. In addition, the interviewed colleagues report that people are still in need of necessities and that the interviewers themselves were asked for help during the interviews. Further studies in the region would be desirable to see to what extent better material support will reduce psychological stress. However, previous studies also show that despite moving to a safer region, the negative psychological effects can still be seen years later [11]. Future studies should also investigate long-term effects on survivors, focusing on coping mechanisms and resilience resources.
Data availability
The data that support the findings of this study are available and request any time by the first author via mail: jan.kizilhan@dhbw.de.
References
World Health Organization. Türkiye earthquakes: six months of resilient response and support. Geneva: World Health Organization; 2023.
World Health Organization. WHO flash appeal Earthquake response in Türkiye and Whole of Syria. Geneva: World Health Organization; 2023.
Çatal E. AFAD: Şu ana kadar 3 bin 858 artçı oldu, bu çok ciddi bir rakam. halk54.com. 15.2.2023.
Dai W, Chen L, Lai Z, Li Y, Wang J, Liu A. The incidence of post-traumatic stress disorder among survivors after earthquakes:a systematic review and meta-analysis. BMC Psychiatry. 2016;16:188. https://doi.org/10.1186/s12888-016-0891-9.
American Psychological Association. APA dictionary of psychology. 2nd ed. Washington, DC: American Psychological Association; 2015.
Casacchia M, Bianchini V, Mazza M, Pollice R, Roncone R. Acute stress reactions and associated factors in the help-seekers after the L’Aquila earthquake. Psychopathology. 2013;46:120–30. https://doi.org/10.1159/000339459.
Ozdemir O, Boysan M, Guzel Ozdemir P, Yilmaz E. Relationships between posttraumatic stress disorder (PTSD), dissociation, quality of life, hopelessness, and suicidal ideation among earthquake survivors. Psychiatry Res. 2015;228:598–605. https://doi.org/10.1016/j.psychres.2015.05.045.
Montazeri A, Baradaran H, Omidvari S, Azin SA, Ebadi M, Garmaroudi G, et al. Psychological distress among Bam earthquake survivors in Iran: a population-based study. BMC Public Health. 2005;5:4. https://doi.org/10.1186/1471-2458-5-4.
Livanou M, Kasvikis Y, Başoğlu M, Mytskidou P, Sotiropoulou V, Spanea E, et al. Earthquake-related psychological distress and associated factors 4 years after the Parnitha earthquake in Greece. Eur Psychiatry. 2005;20:137–44. https://doi.org/10.1016/j.eurpsy.2004.06.025.
Kanehara A, Ando S, Araki T, Usami S, Kuwabara H, Kano Y, Kasai K. Trends in psychological distress and alcoholism after The Great East Japan Earthquake of 2011. SSM Popul Health. 2016;2:807–12. https://doi.org/10.1016/j.ssmph.2016.10.010.
Kiliç C, Aydin I, Taşkintuna N, Ozçürümez G, Kurt G, Eren E, et al. Predictors of psychological distress in survivors of the 1999 earthquakes in Turkey: effects of relocation after the disaster. Acta Psychiatr Scand. 2006;114:194–202. https://doi.org/10.1111/j.1600-0447.2006.00786.x.
Zhang Z, Ran MS, Li YH, Ou GJ, Gong RR, Li RH, et al. Prevalence of post-traumatic stress disorder among adolescents after the Wenchuan earthquake in China. Psychol Med. 2012;42:1687–93. https://doi.org/10.1017/S0033291711002844.
Zhang Y, Ho SMY. Risk factors of posttraumatic stress disorder among survivors after the 512 Wenchuan earthquake in China. PLoS ONE. 2011;6:e22371. https://doi.org/10.1371/journal.pone.0022371.
Jia Z, Lio W, Cao Y, Yan J, Shung Z. Are the elderly more vulnerable to psychological impact of natural disaster? A population-based survey of adult survivors of the 2008 Sichuan earthquake. BMC Public Health. 2010;10:1–11.
Matsubayashi T, Sawada Y, Ueda M. Natural disasters and suicide: evidence from Japan. Soc Sci Med. 2013;82:126–33.
Jafari H, Heidari M, Heidari S, Sayfouri N. Risk factors for suicidal behaviours after natural disasters: a systematic review. Malays J Med Sci MJMS. 2020;27:20.
Lu T-H. Earthquake and suicide: bringing context back into disaster epidemiological studies. Int J Epidemiol. 2004;33:1406–9.
Orui M, Harada S, Hayashi M. Changes in suicide rates in disaster-stricken areas following the Great East Japan earthquake and their effect on economic factors: an ecological study. Environ Health Prev Med. 2014;19:459–66. https://doi.org/10.1007/s12199-014-0418-2.
Nishio A, Akazawa K, Shibuya F, Abe R, Nushida H, Ueno Y, et al. Influence on the suicide rate two years after a devastating disaster: a report from the 1995 Great Hanshin-Awaji earthquake. Psychiatry Clin Neurosci. 2009;63:247–50. https://doi.org/10.1111/j.1440-1819.2009.01942.x.
Kõlves K, Kõlves KE, de Leo D. Natural disasters and suicidal behaviours: a systematic literature review. J Affect Disord. 2013;146:1–14.
Gerstner RMF, Lara-Lara F, Vasconez E, Viscor G, Jarrin JD, Ortiz-Prado E. Earthquake-related stressors associated with suicidality, depression, anxiety and post-traumatic stress in adolescents from Muisne after the earthquake 2016 in Ecuador. BMC Psychiatry. 2020;20:347. https://doi.org/10.1186/s12888-020-02759-x.
Chilcoat HD, Breslau N. Posttraumatic stress disorder and drug disorders: testing causal pathways. Arch Gen Psychiatry. 1998;55:913–7. https://doi.org/10.1001/archpsyc.55.10.913.
Bianchini V, Roncone R, Giusti L, Casacchia M, Cifone MG, Pollice R. PTSD growth and substance abuse among a college student community: coping strategies after 2009 L’aquila Earthquake. Clin Pract Epidemiol Ment Health. 2015;11:140. https://doi.org/10.2174/1745017901511010140.
EarthquakeList.org. Adıyaman Earthquake Report. 2023. https://earthquakelist.org/turkiye/adiyaman/adiyaman/. Accessed 6 Sep 2023.
Kilic C, Rezaki M, Rezaki B, Kaplan I, Ozgen G, Sağduyu A, Oztürk MO. General Health Questionnaire (GHQ12 & GHQ28): psychometric properties and factor structure of the scales in a Turkish primary care sample. Soc Psychiatry Psychiatr Epidemiol. 1997;32:327–31. https://doi.org/10.1007/BF00805437.
Goldberg DP, Gater R, Sartorius N, Ustun TB, Piccinelli M, Gureje O, et al. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol Med. 1997;27:191–7. https://doi.org/10.1017/s0033291796004242.
Goldberg DP, Hillier VF. A scaled version of the general health questionnaire. Psychol Med. 1979;9:139–45. https://doi.org/10.1017/s0033291700021644.
Werneke U, Goldberg DP, Yalcin I, Ustün BT. The stability of the factor structure of the general health questionnaire. Psychol Med. 2000. https://doi.org/10.1017/s0033291799002287.
Kılıç C. Genel Sağlık Anketi: geçerlilik ve güvenilirlik çalışması. Turk Psikiyatri Derg. 1996;7:83–9.
Goldberg DP, Oldehinkel T, Ormel J. Why GHQ threshold varies from one place to another. Psychol Med. 1998;28:915–21. https://doi.org/10.1017/s0033291798006874.
Prins A, Bovin MJ, Kimerling R, Kaloupek DG, Marx BP, Pless Kaiser A, Schnurr pp. The primary care PTSD screen for DSM-5 (PC-PTSD-5). Washington, DC: National Center for PTSD; 2015.
Arbeitseinheit für Klinische Psychologie und Psychotherapie der Universität Bielefeld. The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5) Türkisch - Deutsch: Arbeitseinheit für Klinische Psychologie und.
Beck AT, Steer RA, Brown G. Beck depression inventory–II. Psychological assessment. 1996.
Leeies M, Pagura J, Sareen J, Bolton JM. The use of alcohol and drugs to self-medicate symptoms of posttraumatic stress disorder. Depress Anxiety. 2010;27:731–6. https://doi.org/10.1002/da.20677.
Goenjian AK, Najarian LM, Pynoos RS, Steinberg AM, Manoukian G, Tavosian A, Fairbanks LA. Posttraumatic stress disorder in elderly and younger adults after the 1988 earthquake in Armenia. Am J Psychiatry. 1994;151:895.
Kohn R, Levav I, Garcia ID, Machuca ME, Tamashiro R. Prevalence, risk factors and aging vulnerability for psychopathology following a natural disaster in a developing country. Int J Geriatr Psychiatry. 2005;20:835–41.
Kato H, Asukai N, Miyake Y, Minakawa K, Nishiyama A. Post-traumatic symptoms among younger and elderly evacuees in the early stages following the 1995 Hanshin-Awaji earthquake in Japan. Acta Psychiatr Scand. 1996;93:477–81.
Pritchard C, Amanullah S. An analysis of suicide and undetermined deaths in 17 predominantly Islamic countries contrasted with the UK. Psychol Med. 2007;37:421–30.
World Health Organization. Global Health Observatory Data Repository. 2021. https://apps.who.int/gho/data/view.main.MHSUICIDEASDRv.
Acknowledgements
I changed the number of affilation for Neuman in "2" and revised the abstract with my newest and revised abstract, which is identically with my revised manuscript. Best Jan.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
JIK and JN designed the study, JIK planned the assessment. JN analyzed the data and JN and JIK wrote the paper. SA, EA, AD, HUAM provided the Turkish translations, gave input for the design and conducted the interviews. AB helped with the data entry. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects/patients were approved by the Institute for Psychotherapy and Psychotraumatology, University of Dohuk, Ethical Committee, No.I (IPP-07-02-2023). We also received permission from the Turkish Medical Association and the local government to conduct the interviews in the city of Adiyaman.
Consent for publication
Written, informed consent was obtained from the patients for publication of this manuscript and any accompanying information or images.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kizilhan, J.I., Neumann, J., Aslan, S. et al. Psychological impact of the earthquake 2023 in Turkey. Discov Public Health 21, 71 (2024). https://doi.org/10.1186/s12982-024-00198-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12982-024-00198-7