
Abstract
Background
Despite increasing effort for treating primary central nervous system lymphoma (PCNSL), the prognosis of human immunodeficiency virus (HIV) -related PCNSL was still unsatisfactory. There is currently a lack of clinical evidence for the application of Bruton tyrosine kinase (BTK) inhibitor in HIV-related PCNSL. We reported two HIV-related PCNSL patients, who achieved sustained remission by application of BTK inhibitor based treatment. This protocol had not been previously reported for the treatment of HIV-related PCNSL.
Case presentation
The two cases were characterized by the treatment choice of Bruton tyrosine kinase (BTK) inhibitor. Rituximab was not recommended for them due to their very low CD4+ T cell counts. They both took MTX as the first-line therapy and got a relief in initial phase. For the first case, ibrutinib was kept both in the first-line therapy and in the maintenance therapy. When the second case underwent a progressive disease, we continued to use orelabrutinib as one of the salvage treatment, in combination with programmed cell death-1 (PD-1) inhibitor plus lenalidomide. They both achieved a continuous response of up to 20 months without opportunistic infection.
Conclusions
This report highlights the safety and effectiveness of BTK inhibitors, as well as lenalidomide and PD-1 inhibitor in HIV-related PCNSL patients. Both the new therapeutic approaches and a multidisciplinary team authentically contributed to improved survival outcome among HIV-positive PCNSL patients.
Similar content being viewed by others


Background
One of the most common HIV-associated lymphomas is diffuse large B-cell lymphoma (DLBCL), including primary central nervous system lymphoma (PCNSL), which generally develops in patients with severe immunosuppression and positive Epstein Barr virus (EBV) [1,2,3]. The prognosis of HIV-related PCNSL patients is inferior to that in HIV-negative patients [4, 5]. Compared to before the advent of antiretroviral therapy (ART), the overall survival post-ART has improved. Increasing evidence supports induction treatment of high-dose methotrexate (HD-MTX) combination with effective ART in most patients with HIV-related PCNSL [1, 6]. Rituximab has been used successfully in a small number of HIV-related PCNSL patients and other HIV-associated lymphomas [7]. Bruton tyrosine kinase (BTK) inhibitor is promising in PCNSL [8, 9], however its application in HIV-related PCNSL is unclear. Here, we reported two HIV-related PCNSL patients, who achieved sustained remission by application of BTK inhibitor.
Case presentation
Case 1
A 41-year-old Chinese man complained numbness at the right extremity for one month in April, 2021. He also had paroxysmal dizziness without nausea, vomiting, convulsions, and consciousness disorder. He had normal muscle strength and muscle tension without sensation dysfunction and neck stiffness. The brain magnetic resonance imaging (MRI) showed a space-occupying lesion (Fig. 1a-d). No extra-cranial lesion was found. HIV confirmatory test was positive. The CD4+T cell count was 15 cells/µL. Serum cryptococcal antigen test was negative. T-cell spot of tuberculosis test was negative. Serum EBVCA -IgG and NA -IgG antibodies were positive. EBV DNA was undetectable in peripheral blood and HIV RNA load was 5.05 × 105 copies/mL. The cerebrospinal fluid (CSF) pressure was 150 mm H2O, protein level was 936 mg/L, cell count was 12 × 106 /L, acid-fast stain and India ink stain were negative. The cryptococcus antigen, culturing of bacteria and fungus, and cytomegalovirus (CMV) -DNA using CSF samples were also all negative. EBV DNA was 2.662 × 104 copies/mL and HIV RNA loads were 2.06 × 105 copies/mL in CSF samples. No other pathogens were confirmed by the next-generation sequencing in the CSF sample. The biopsy of brain lesions indicated EBV -positive large B-cell lymphoma (not otherwise specified type) (Fig. 1e-h). The foscarnet sodium therapy and ART were initiated. The regimens and treatment course for PCNSL was showed in Fig. 1i. The SMZ/TMP (oral, 2 tablets daily), fluconazole (oral, 200 mg daily) and azithromycin (oral, 200 mg daily) were applied for the prophylactic treatment of Pneumocystis jirovecii pneumonia, fungus infection and mycobacterium infection. After taking the induction regimen of MTX/ibrutinib (a BTK inhibitor) /temozolomide (3 cycles), he experienced a partial response (PR) in August, 2021, then kept the PR though MTX (another 2 cycles) was replaced by Cytarabine (2 cycles) due to its kidney injury adverse effect. He declined the autologous stem cell transplantation. During the maintenance mono-therapy with ibrutinib, he achieved a complete response (CR) in March, 2022. In February, 2023, he still kept CR with undetectable blood HIV RNA and 336 cells/µL of CD4+ T cell count.

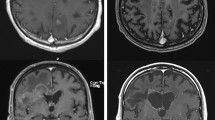
The radiological, pathologic diagnosis and treatment of case 1. Brain contrast-enhanced MRI (a-d): A space-occupying lesion about 3.9 × 2 × 1.6 cm at the corpus callosum with a ring enhancement before treatment (in Apr, 2021) (a); Having a partial response (PR) after 2 months treatment (In August, 2021) (b); Keeping a PR after 4 months treatment (In October, 2021) (c); Achieving a complete response (CR) after 8 months treatment (In March, 2022) and keeping a CR after 19 months treatment (In February, 2023) (d). Histological characteristics (e-h): Diffuse distribution of tumor cells with flaky coagulation necrosis were found. There were a large amount of lymphoid cells proliferation especially around the blood vessels and lymphocyte infiltration in blood vessel wall. The volume of some cells is medium to small, and other cells are medium to large. The nucleus is slightly irregular, and nucleolus enlargement and nuclear division were found (H&E staining, original magnification×200) (e); The diffuse expression of CD20-positive tumor cells ( immunohistochemical staining, original magnification×200) (f). The tumor cells with positive expression of Pax-5 (immunohistochemical staining, original magnification×200)(g). The positive EBV-encoded small RNA (EBER) was found (situ hybridization, original magnification×200) (h). Treatment regimen adjustment (i)
Case 2
A 39-year-old Chinese man complained headache and dizziness for two and a half months in May, 2021. He had no fever, consciousness disorder, convulsions or limbs movement disorder. Mannitol treatment could relieve the symptoms. The brain MRI showed a space-occupying lesion (Fig. 2a-d). No extra-cranial lesion was found. HIV confirmatory test was positive. The CD4+T cell count was 27 cells/µL. HIV RNA load was 1.57 × 104 copies/mL in blood. Serum Rubella IgG, CMV IgG, herpes simplex virus-1/2 IgG, EBVCA -IgG, EBNA -IgG antibodies were positive. EBV DNA load was 1.19 × 105 copies/mL in peripheral blood. Serum CMV DNA load was undetectable. T-cell spot of tuberculosis test was negative. To avoid worsening of brain herniation, lumbar puncture was not applied to this case. The biopsy of brain lesion indicated EBV -positive PCNSL of large B-cell lymphoma (non-germinal center B-cell-like type) (Fig. 2e-h). The ganciclovir therapy and ART were initiated. He also adopted the same prophylactic treatment as described in the first case. The regimens and treatment course for PCNSL was showed in Fig. 2i. After taking the induction regimen of MTX/temozolomide (3 cycles), he got a PR in August, 2021, and kept PR with MTX/temozolomide/orelabrutinib (a BTK inhibitor) (another 3 cycles). He declined the autologous stem cell transplantation. Then he had a disease progression (PD) during the regimen of Cytarabine/temozolomide/orelabrutinib (2 cycles) in December, 2021, and adopted the salvage treatment regimen of sintilimab (PD-1 inhibitor) /orelabrutinib/lenalidomide (an immunomodulatory drug) followed by another PR in March, 2022. In August, 2022, he experienced a CR during orelabrutinib/lenalidomide maintenance therapy. Then, the patient continued mono-therapy of orelabrutinib and still kept CR with undetectable blood HIV RNA and 116 cells/µL of the CD4+T cell count until the lasted follow-up in May, 2023.

The radiological, pathologic diagnosis and treatment of case 2. Brain contrast-enhanced MRI (a-d): A ring enhancement space-occupying lesion 4.7 × 4.6 × 3.4 cm in the right cerebellar hemisphere with an amygdala cerebelli herniation before treatment (In May, 2021) (a). Having a PR after 2 months treatment (In August, 2021) (b). Presenting a progressive disease after 6 months treatment (In December, 2021) (c). Achieving a CR after 13 months treatment (In August, 2022) and keeping a CR after 19 months treatment (In February, 2023) (d). Histological characteristics (e-h): Diffuse distribution of tumor cells with flaky coagulation necrosis was found. The volume of most cells is large. The nucleus is slightly irregular, and nucleolus enlargement and nuclear division were found (H&E staining, original magnification×200) (e). The diffuse expression of CD20-positive tumor cells (immunohistochemical staining, original magnification×200) (f). The tumor cells with positive expression of Pax-5 (immunohistochemical staining, original magnification×200) (g). The positive EBV-encoded small RNA (EBER) was found (situ hybridization, original magnification×200) (h). Treatment regimen adjustment (i)
Discussion
The influence of ART on HIV-related PCNSL was beneficial and ART could really prevent from opportunistic infections occurrence after virological control and immunological recovery. The efficacy of anti -EBV therapy on PCNSL was undetermined [10]. There is currently no standard treatment for HIV-related PCNSL, and national comprehensive cancer network guidelines recommend the application of HD -MTX as induction therapy [11]. These two cases took MTX as the first-line therapy and got a relief in initial phase. Rituximab was not recommended for these two cases due to their very low CD4+T cell counts. However, the first case stopped MTX during induction therapy due to its kidney injury adverse effect and the second case got a progressive disease during consolidation therapy. For relapsed or refractory PCNSL, BTK inhibitors and immunomodulatory drugs such as lenalidomide and pomalidomide can be effective [8, 9]. PD-1 inhibitors suggest better efficacy in a small sample of retrospective studies for relapsed/refractory HIV-negative PCNSL [12, 13]. However, the effectiveness of these treatments in HIV-related PCNSL is uncertain. In our first case, ibrutinib has added to first-line therapy and achieved further remission by maintenance therapy, which showed similar response for treatment -naïve HIV-negative PCNSL cases [14, 15]. The ibrutinib/MTX combination followed by ibrutinib mono-therapy maintenance achieved 64% of CR [14]. The ibrutinib/MTX /temozolomide combination achieved 88.9% of CR [15]. In the second case, orelabrutinib, PD-1 inhibitor plus lenalidomide acted as the salvage treatment and achieved another PR after disease progression and then orelabrutinib achieved sustained remission as maintenance treatment, which showed similar response for relapsed/refractory HIV-negative PCNSL cases [16, 17]. The orelabrutinib/lenalidomide -containing combination therapy achieved 73.3% of CR [16]. Although PD-1/ programmed death ligand 1 (PD-L1) over-expression in the micro-environment of PCNSL suggested a therapeutic recommendation, the therapeutic response and prognostic correlation was inconclusive [18,19,20]. The relapsed/refractory PCNSL cases with/without gene alterations (such as MYD88) of B-cell receptor signaling pathway demonstrated the clinical response to BTK inhibitors [21]. From PCNSL diagnosis until now, the overall survival of both patients were 20 months, which suggested the efficacy of BTK inhibitors, as well as lenalidomide and PD-1 inhibitors. Both patients did not have drug side effects and opportunistic infections occurrence throughout the treatment, which suggested the safety of BTK inhibitors and other target therapy. The efficacy of the BTK inhibitors monotherapy for PCNSL was limited [22, 23]. In order to avoid BTK inhibitors resistance and augment the BTK inhibitors response, it was suggested that BTK inhibitors was added into combination regimen. Last but not least, the multidisciplinary team including HIV specialist, neurosurgeon, pathologist and hematologist demonstrated the diagnostic and therapeutic advantages for HIV-positive PCNSL patients.
Data Availability
All data generated or analyzed during this study are included in this published article.
Abbreviations
- DLBCL:
-
Diffuse large B-cell lymphoma
- PCNSL:
-
Primary central nervous system lymphoma
- BTK:
-
Bruton tyrosine kinase
- PD-1:
-
Programmed cell death-1
- PD-L1:
-
Programmed death ligand 1
- HIV:
-
Human immunodeficiency virus
- MRI:
-
Magnetic resonance imaging
- ART:
-
Antiretroviral therapy
- HD -MTX:
-
High-dose methotrexate
- CSF:
-
Cerebrospinal fluid
- EBV:
-
Epstein Barr virus
- CMV:
-
Cytomegalovirus
- PR:
-
Partial response
- CR:
-
Complete response
References
Brandsma D, Bromberg JEC. Primary CNS lymphoma in HIV infection Handb Clin Neurol. 2018;152:177–86.
Kimani SM, Painschab MS, Horner MJ, Muchengeti M, Fedoriw Y, Shiels MS, et al. Epidemiology of haematological malignancies in people living with HIV. Lancet HIV. 2020;7(9):e641–51.
Ding X, Liang T, Liang B, Gao H, Wang J, Liu H, et al. Diagnostic value of EBV-DNA in CSF for PCNSL in AIDS patients with focal brain lesions: a meta-analysis of diagnostic test. Med (Baltim). 2022;101(48):e31793.
Dittus C, Grover N, Sethi T, Cohen JB, Voloschin A, Rabadey J, et al. A multicenter, real-world analysis of primary central nervous system lymphoma in those with and without human immunodeficiency virus. EJHaem. 2022;3(3):734–8.
Bayraktar S, Bayraktar UD, Ramos JC, Stefanovic A, Lossos IS. Primary CNS lymphoma in HIV positive and negative patients: comparison of clinical characteristics, outcome and prognostic factors. J Neurooncol. 2011;101(2):257–65.
Moulignier A, Lamirel C, Picard H, Lebrette MG, Amiel C, Hamidi M, et al. Long-term AIDS-related PCNSL outcomes with HD-MTX and combinedantiretroviral therapy. Neurology. 2017;89(8):796–804.
Lurain K, Uldrick TS, Ramaswami R, Polizzotto MN, Goncalves PH, Widell A, et al. Treatment of HIV-associated primary CNS lymphoma with antiretroviral therapy, rituximab, and high-dose methotrexate. Blood. 2020;136(19):2229–32.
Schaff LR, Grommes C. Update on Novel therapeutics for primary CNS lymphoma. Cancers (Basel). 2021;13(21):5372.
Ferreri AJM, Holdhoff M, Nayak L, Rubenstein JL. Evolving treatments for primary Central Nervous System Lymphoma. Am Soc Clin Oncol Educ Book. 2019;39:454–66.
Verdu-Bou M, Tapia G, Hernandez-Rodriguez A, Navarro JT. Clinical and therapeutic implications of Epstein-Barr Virus in HIV-Related Lymphomas. Cancers (Basel). 2021;13(21):5534.
González-Aguilar A, Soto-Hernández JL. The management of primary central nervous system lymphoma related to AIDS in the HAART era. Curr Opin Oncol. 2011;23(6):648–53.
Nayak L, Iwamoto FM, LaCasce A, Mukundan S, Roemer MGM, Chapuy B, et al. PD-1 blockade with nivolumab in relapsed/refractory primary central nervous system and testicular lymphoma. Blood. 2017;129:3071–3.
Ambady P, Szidonya L, Firkins J, James J, Johansson K, White T, et al. Combination immunotherapy as a non-chemotherapy alternative for refractory or recurrent CNS lymphoma. Leuk Lymphoma. 2019;60(2):515–8.
Chen FL, Pang DW, Guo HG, Ou QX, Wu X, Jiang XM. Clinical outcomes of newly diagnosed primary CNS lymphoma lymphoma treated with ibrutinib-based combination therapy: a real-world experience of off-label ibrutinib use. Cancer Med. 2020;9(22):8676–84.
Wang XX, Gao Y, Yu SS, Bai B, Ou QX, Zhu LQ, et al. Preliminary results of a phase II study of methotrexate in combination with ibrutinib and temozolomide (MIT) in newly diagnosed primary CNS lymphoma. Blood. 2021;138(S1):2481–3.
Yang C, Cui Y, Ren X, Li M, Yu K, Shen S, et al. Orelabrutinib combined with lenalidomide and immunochemotherapy for Relapsed/Refractory primary central nervous system lymphoma: a retrospective analysis of case series. Front Oncol. 2022;12:901797.
Wu JJ, Wang WH, Dong M, Ma SS, Zhang XD, Zhu LN Orelabrutinib-bruton tyrosine kinase inhibitor-based regimens in the treatment of central nervous system lymphoma: A retrospective study. Invest New Drugs. 2022;40(3):650–9.
Tsuyuki Y, Ishikawa E, Kohno K, Shimada K, Ohka F, Suzuki Y, et al. Expression of programmed cell death ligand-1 by immune cells in the microenvironment is a favorable prognostic factor for primary diffuse large B-celllymphoma of the central nervous system. Neuropathology. 2021;41(2):99–108.
Monabati A, Nematollahi P, Dehghanian A, Safaei A, Sadeghipour A, Movahedinia S, et al. Immune Checkpoint Molecules in primary diffuse large B-Cell lymphoma of the Central Nervous System. Basic Clin Neurosci. 2020;11(4):491–8.
Sugita Y, Furuta T, Ohshima K, Komaki S, Miyoshi J, Morioka M et al. The perivascular microenvironment in Epstein-Barr virus positive primary central nervous system lymphoma: the role of programmed cell death 1 and programmed cell death ligand 1.Neuropathology.2018;38(2):125–34.
Soussain C, Choquet S, Blonski M, Leclercq D, Houillier C, Rezai K, et al. Ibrutinib mono-therapy for relapse or refractory primary CNS lymphoma and primary vitreoretinal lymphoma: final analysis of the phase II ‘proof-of-concept’ iLOC study by the Lymphoma study association (LYSA) and the french oculo-cerebral lymphoma (LOC) network. Eur J Cancer. 2019;117:121–30.
Grommes C, Pastore A, Palaskas N, Tang SS, Campos C, Schartz D, et al. Ibrutinib unmasks critical role of Bruton Tyrosine kinase in primary CNS lymphoma. Cancer Discov. 2017;7(9):1018–29.
Soussain C, Choquet S, Blonski M, Leclercq D, Houillier C, Rezai K, et al. Ibrutinib monotherapy for relapse or refractory primary CNS lymphoma and primary vitreoretinal lymphoma: final analysis of the phase II ‘proof-of-concept’ iLOC study by the Lymphoma study association (LYSA) and the french oculo-cerebral lymphoma (LOC) network. Eur J Cancer. 2019;117:121–30.
Acknowledgements
We thank the patients for agreeing to submit this report. We also thank the Jinyong Wang (Department of Infectious Diseases II of the First Affiliated Hospital of China Medical University) for their professional assistance.
Funding
No research funding.
Author information
Authors and Affiliations
Contributions
Ying Wen and Xiaojing Yan had the original idea for the paper. Xiaoxue Wang, Xiaojing Yan, Ying Zhou and Ying Wen were in charge of treatment and management of the patient. Ying Zhou, Xiaojing Yan and Ying Wen wrote the paper. Xuyong Lin was responsible for pathological figure description. Jun Wang completed the brain lesion biopsy. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
The patient has provided written informed consent for the publication of this report.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhou, Y., Wang, X., Lin, X. et al. Sustained response following BTK inhibitors based treatment in HIV-related primary central nervous system lymphoma: case report. AIDS Res Ther 20, 63 (2023). https://doi.org/10.1186/s12981-023-00554-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12981-023-00554-8