
Abstract
Introduction
Intestinal parasites and HIV/AIDS co-infection become a major public health concern in Africa. The management and care of HIV/AIDS patients is being complicated by intestinal parasitic infections. Therefore, this study aimed to determine the prevalence and associated factors of intestinal parasitic infections among people living with HIV at Dessie Referral Hospital, North-east Ethiopia.
Methods
This cross sectional study was conducted from March to May 2019. Systematic simple random sampling technique was used to recruit study participants. Stool specimen was collected and examined microscopically using wet mount, formol-ether concentration technique and modified Zeihl–Neelsen methods. Socio-demographic characteristics and associated factors were collected using structured questionnaire. The recent CD4 cell count was obtained from patients ART follow-up record. Data were analysed using SPSS version 20 software. Bivariate and multivariate logistic regression was done to investigate the association between independent and dependent variables.
Results
Of the total of 223 study participants 120 (53.8%) were females and 162 (72.6%) were urban resident. The overall prevalence of intestinal parasites was 47 (21.1%). Eleven different intestinal parasites species were detected. The dominant intestinal parasite species was Entameoba histolytica 14 (6.3%) followed by Enterobius vermicularis 5 (2.2%). Multivariate logistic regression analysis showed that individuals who had a habit of hand washing after latrine were less likely to be infected with intestinal parasitic infection (AOR 0.15, 95% CI 0.05–0.412). On the other hand individuals who had CD4 cell count of < 200 cells/ml3 were 45.53 times more likely infected with intestinal parasites.
Conclusion
The prevalence of intestinal parasite was higher than previous report from the same study area almost a decade ago. There was statistical significant association between hand washing habit after latrine, habit of eating raw vegetables and CD4 cell count less than 200 cells/ml3 and intestinal parasitic infections. Health education program interrupted in Dessie referral hospital should be continued to reduce the prevalence of intestinal parasites. Utilization of water treatment, washing hand after latrine and eating cooked or appropriately washed vegetables should also be promoted. Moreover, periodic laboratory stool specimen examination and prompt treatment are necessary.
Similar content being viewed by others


Background
Intestinal parasitic infections are widely distributed throughout the world and they are a major cause of morbidity and mortality [1]. They are usually highly prevalent in sub-Saharan Africa, where HIV/AIDS cases are also concentrated [2]. The co-infection of intestinal parasites and HIV/AIDS has become a major public health concern in Africa. Human immune deficiency (HIV) infection suppress human immunity and expose individuals to opportunistic infections is responsible for high mortality rate [3]. Among the opportunistic infections, intestinal parasitic infections caused by helminths and protozoa are the most common infections in the world [4]. Intestinal parasitic infections become severe when they appear in HIV/AIDS patients. They play an important role in the progression of HIV infection to AIDS, by further disturbing the immune system [1]. The common immunopathogenetic basis for the deleterious effects that parasitic diseases may involve in preferential activation of the T helper type process. Thus combating the HIV should involve control and prevention of parasitic diseases [5].
The prevalence of both HIV/AIDS and intestinal parasites in Ethiopia is high. In Ethiopia the national adult HIV prevalence is 0.9% and an estimated 613,000 people were living with HIV, and 30% were from the Amhara region in 2017 [6]. The incidence rate of HIV in Dessie was higher than other towns of Amhara region with 5.74 per 1000 population [6]. The high occurrence of associated factors such as low coverage of insufficient water supply for drinking, low coverage of self and environmental hygiene facilities and contamination of food and drinking water that results from improper disposal of human excreta favour the high prevalence of intestinal parasitic infections [7, 8]. In Ethiopia, intestinal parasitic infections are responsible for more than half a million annual visits of the outpatient services of the health institutions [9]. This report may be underestimated due to lack of appropriate diagnostic test methods in many of the health institutions. Intestinal parasites and HIV/AIDS are widespread throughout the country [8, 9]. The management and care of HIV/AIDS patients is complicated by intestinal parasitic infections. So, detecting intestinal parasites and understanding the health complications they cause will help health workers to manage properly and treat HIV/AIDS patients. As far as we know, there was only one study conducted 9 years ago among pre-ART and on ART HIV/AIDs patient in the study area. Therefore, this study was aimed to update the information about the prevalence and associated factors of intestinal parasitic infection among people living with HIV who are on ART follow up at Dessie Referral Hospital, Dessie town, North-East Ethiopia.
Methods
Study area
This study was conducted at Dessie Referral Hospital which is found in Dessie town, North-east Ethiopia. Dessie town is found in western part of Amhara region and it is 401 km far from Addis Ababa, the capital city of Ethiopia. It is geographically located at 11°8N latitude, 39°38E longitude, and an average altitude of 2470 m above sea level. The town is generally characterized by cold weather with mean annual maximum and minimum temperature of 25 °C and 5 °C, respectively. Based on the 2007 census conducted by the Central Statistical Agency of Ethiopia, Dessie town has a total population of 151,174 of whom 72,932 are men and 78,242 women. A study in Amhara region reported that incidence rate of HIV in Dessie was higher than other towns of Amhara region with 5.74 per 1000 population [6].
Study design and period
This institution based cross sectional study was conducted from March to May 2019.
Inclusion and exclusion criteria
All HIV/AIDS patients visited ART clinic of Dessie Referral Hospital during the study period were included. Individuals who were on intestinal parasitic infection treatment during the data collection period were excluded.
Sample size and sampling technique
The sample size was determined using the single population proportion formula using a prevalence of 17.6% [8] with margin of error 5% and 95% confidence interval [Z (1− ά/2) = 1.96]. The final calculated sample size was 223 and systematic random sampling technique was used to recruit the study participants using the ART clinic registration book as a sampling frame.
Data collection
Socio-demographic and associated factors were collected using pre-tested structured questionnaire. Data collectors were trained before the start of data collection. Information about recent CD4 cell count of people living with HIV was obtained from their ART follow-up record. An estimated 5 g stool specimen was collected from each study participant using leak proof and clean plastic container for parasitological examination.
Laboratory investigation
Stool sample was examined microscopically using direct wet mount, Formol–ether concentration technique and modified Ziehl–Neelsen method for parasite detection. Direct wet mount examination was performed using normal saline and Lugol’s iodine at Dessie referral Hospital. Then the remained stool sample was preserved with 10% formalin for formol–ether concentration technique and modified Zeihl–Neelsen method procedures. For formol-ether concentration technique, an estimated 1 g (pea-size) stool sample was mixed with 4 ml of 10% formol water. Additional 4 ml of 10% v/v formol water was added and mixed by shaking. After the content sieved 4 ml of diethyl ether was added and mixed for 1 min. Then it was immediately centrifuged at 3000 revolution per minute (rpm) for 1 min. Finally, the sediment was examined under microscope. The remaining sediment was stained using Modified Ziehl–Neelsen method for the detection of intestinal coccidian parasites. Standard Operational Procedure (SOP) was strictly followed during microscopic examination of stool specimen for intestinal parasites.
Data analysis
Data were checked for completeness and were entered to SPSS version 20 software and analysed. Logistic regression were done to investigate the association between independent variables and dependent variable. In all comparisons, p-value less than 0.05 was considered statistically significant.
Ethical consideration
The willingness of the study participants were asked using written consent form. Ethical clearance was obtained from Wollo University, College of Medicine and Health Science, Department of Medical Laboratory Science. Study participants with positive intestinal parasite result were treated in Dessie Referral Hospital according to the national treatment guideline.
Result
Socio-demographic characteristics and associated factors
Of the total of 223 study participants 120 (53.8%) were females, 108 (48.4%) were between 30 and 49 age group, 162 (72.6%) were urban resident, 100 (44.8%) were single and majority of them 92 (41.3%) were at primary educational level. Majority (84.3%) of the study participants had the habit of using latrine. With regard to water source for drinking, 82.5% of study participants use pipe water. Almost all of the study participants 216 (96.9%) had no the habit of using water treatment (Table 1).
Prevalence of intestinal parasites among people living with HIV
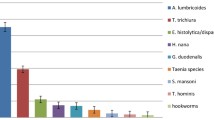
The overall prevalence of intestinal parasites was 47 (21.1%). Eleven different intestinal parasites species were detected. The dominant intestinal parasite species was Entameoba histolytica 14 (6.3%) followed by Enterobius vermicularis 5 (2.2%), Gardia lamblia 4 (1.8%), Ascaris lumbricoides 4 (1.8%) and Cryptosporidium species 4 (1.8%). The least common parasites detected in this study were Isospora belli and Schistosoma mansoni (Fig. 1).

intestinal parasites detected among individuals living with HIV attending ART clinic of Dessie Referral Hospital from March to May 2019.
Associated factors for intestinal parasites among people living with HIV
Bivariate analysis showed that hand washing habit after latrine, habit of eating raw vegetables, eating raw meat and CD4 count showed statistical significant association with intestinal parasitic infection. In multivariate logistic regression analysis only hand washing habit after latrine, CD4 cell count of less than 200cells/ml3 and habit of eating raw vegetables had statistical significant association with intestinal parasitic infection. There was statistical significant association between intestinal parasitic infections and hand washing habit. Those individuals who had hand washing habit after latrine were less likely to be infected with intestinal parasites (AOR 0.15, 95% CI 0.05–0.412). Similarly, individuals who had CD4 cell count of < 200 cells/ml3 were 45.53 times more likely infected with intestinal parasites compared to those who had > 500 CD4 cells/ml3 (Table 2).
Discussion
Intestinal parasites and HIV/AIDS are co-endemic in many regions of the world [10]. In this study, majority of the study participants (53.8%) were females. This was in agreement with a report from Kano, Nigeria [11]. The prevalence of HIV/AIDS may be relatively increased in women as receptive partner in heterosexual intercourse [11]. In the present study majority of the HIV/AIDS patients were single (44.8%). This could be one of the possible reasons for being exposed to HIV/AIDS as a result of having multiple sexual partner.
This study revealed that the prevalence of intestinal parasites among people living with HIV was 47 (21.1%). The finding was higher than previous studies reported from Ethiopia (13.9%) [12], Nigeria (11.4%) [11] and Cameroon (14.64%) [12, 13]. On the other hand the prevalence was lower than reports from Cameroon (57.48%) and Ethiopia [3, 14, 15]. The lower or higher prevalence of intestinal parasites in this study compared to previous studies might be due to variations in geographical area that affect the distribution of parasites, study period (seasonal variations), life style and culture of the society, awareness about the prevention and control of intestinal parasites, differences in socio economic status and the diagnostic methods employed for parasite detection.
The prevalence of intestinal parasites was also higher than the study conducted in Dessie Referral Hospital 9 years ago among HIV/AIDS patients (17.6%) [8]. The possible reasons might be due to the interruption of scheduled deworming program to people taking ART at the study site. The other most probable reason could be the interruption of health education programs that was given for HIV/AIDS patients at Dessie Referral Hospital about the transmission, prevention and control of intestinal parasites and other infectious diseases.
With regard to the species of intestinal parasites, the most common parasite detected in this study was E. histolytica (6.3%) and E. vermicularis (2.2%). The prevalence of E. histolytica was higher than a study conducted among HIV/AIDs patients reported from Benin City, Nigeria (3.3%) [2]. On the other hand it was consistent with studies conducted in Cameroon (7.52%) [12] and Lesotho (6.7%) [16].
In the present study there was statistically significant association between CD4 cell count and intestinal parasitic infection among HIV/AIDs patients. This was consistent with previous studies [15, 17, 18]. Similarly, hand washing habit after toilet and eating raw vegetables showed statistical significant association with intestinal parasitic infection. These factors are known to expose individuals for intestinal parasitic infections. Especially, eating raw vegetables that are not washed appropriately before eating is the major source of intestinal parasitic infections. The present study has limitations with regard to Microsoporidia, Strongyloides stercoralis and Enetrobius vermicularis diagnosis. Although the diagnosis of these parasites require specific and sensitive diagnostic methods, we could not employ special diagnostic techniques due to lack of resources. Therefore, the prevalence these parasites might be underestimated in this study.
Conclusion
The prevalence of intestinal parasite was higher than previous report from the same study area almost a decade ago. The dominant intestinal parasites detected were E. histolytica followed by E. vermicularis. The present study also revealed statistical significant association between hand washing habit after latrine, eating raw vegetables and CD4 cell count and intestinal parasitic infections. The interrupted health education program in the hospital should be continued to reduce the prevalence of intestinal parasites. Utilization of water treatment, washing hand after latrine and eating cooked or appropriately washed vegetables should also be promoted. In addition, periodic laboratory stool specimen examination, awareness creations about the prevention and control of intestinal parasites and prompt treatment are necessary.
Availability of data and materials
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the manuscript.
Abbreviations
- AIDS:
-
Acquired immunodeficiency syndrome
- ART:
-
Anti-retroviral therapy
- CD4:
-
Cluster of differentiation on T4 lymphocyte cells
- HIV:
-
Human immunodeficiency virus
References
Gebrecherkos T, Kebede H, Gelagay AA. Intestinal parasites among HIV/AIDS patients attending University of Gondar Hospital, northwest Ethiopia. Ethiop J Health Dev. 2019;33(2):65–72.
Akinbo FO, Okaka CE, Omoregie R. Prevalence of intestinal parasitic infections among HIV patients in Benin City, Nigeria. Libyan J Med. 2010. https://doi.org/10.3402/ljm.v5i0.5506.
Awole M, Gebre-Selassie S, Kassa T, Kibru G. Prevalence of intestinal parasites in HIV-infected adult patients in southwestern Ethiopia. Ethiop J Health Dev. 2003;17(1):71–8.
Brooker S, Clements AC, Bundy DA. Global epidemiology, ecology and control of soil-transmitted helminth infections. Adv Parasitol. 2006;1(62):221–61.
Kaniyarakkal V, Mundangalam N, Moorkoth AP, Mathew S. Intestinal parasite profile in the stool of HIV positive patients in relation to immune status and comparison of various diagnostic techniques with special reference to Cryptosporidium at a tertiary care hospital in South India. Adv Med. 2016;17:2016.
Worku ED, Asemahagn MA, Endalifer ML. Epidemiology of HIV infection in the Amhara region of Ethiopia, 2015 to 2018 surveillance data analysis. HIV AIDS (Auckl). 2020;12:307.
Hailemariam G, Kassu A, Abebe G, Abate E, Damte D, Mekonnen E, Ota F. Intestinal parasitic infections in HIV/AIDS and HIV seronegative individuals in a teaching hospital, Ethiopia. Japn J Infect Dis. 2004;57(2):41–3.
Missaye A, Dagnew M, Alemu A, Alemu A. Prevalence of intestinal parasites and associated risk factors among HIV/AIDS patients with pre-ART and on-ART attending dessie hospital ART clinic, Northeast Ethiopia. AIDS Res Ther. 2013;10(1):1–9.
Alemu A, Shiferaw Y, Getnet G, Yalew A, Addis Z. Opportunistic and other intestinal parasites among HIV/AIDS patients attending Gambi higher clinic in Bahir Dar City, North West Ethiopia. Asian Pac J Trop Med. 2011;4(8):661–5.
Adamu H, Petros B. Intestinal protozoan infections among HIV positive persons with and without antiretroviral treatment (ART) in selected ART centers in Adama, Afar and Dire-Dawa, Ethiopia. Ethiop J Health Dev. 2009. https://doi.org/10.4314/ejhd.v23i2.53230.
Jegede EF, Oyeyi ET, Bichi AH, Mbah HA, Torpey K. Prevalence of intestinal parasites among HIV/AIDS patients attending Infectious Disease Hospital Kano, Nigeria. Pan Afr Med J. 2014;17:295.
Gebretsadik D, Haileslasie H, Feleke DG. Intestinal parasitosis among HIV/AIDS patients who are on anti-retroviral therapy in Kombolcha, North Central, Ethiopia: a cross-sectional study. BMC Res Notes. 2018;11(1):1–5.
Nkenfou CN, Nana CT, Payne VK. Intestinal parasitic infections in HIV infected and non-infected patients in a low HIV prevalence region, West-Cameroon. PLoS ONE. 2013;8(2):e57914.
Vouking MZ, Enoka P, Tamo CV, Tadenfok CN. Prevalence of intestinal parasites among HIV patients at the Yaoundé Central Hospital, Cameroon. Pan Afr Med J. 2014;18:136.
Teklemariam Z, Abate D, Mitiku H, Dessie Y. Prevalence of intestinal parasitic infection among HIV positive persons who are naive and on antiretroviral treatment in Hiwot Fana Specialized University Hospital, Eastern Ethiopia. ISRN AIDS. 2013;2013:32429.
Oguntibeju OO. Prevalence of intestinal parasites in HIV-positive/AIDS patients. Malays J Med Sci. 2006;13(1):68.
Assefa S, Erko B, Medhin G, Assefa Z, Shimelis T. Intestinal parasitic infections in relation to HIV/AIDS status, diarrhea and CD4 T-cell count. BMC Infect Dis. 2009;9(1):1–6.
Naik R, Ravichandraprakash H, Ukey P, Vijayanath V, Shreeharsha G, Chandak V. Opportunistic intestinal parasitic infections in HIV/AIDS patients presenting with diarrhea and their correlation with CD4+ T-lymphocyte counts. Int J Pharm Bio Sci. 2012;2(4):293–9.
Acknowledgements
We would like to acknowledge Wollo University Medical Laboratory Science department technical assistants and other staffs for their cooperation during laboratory investigations. We would also like to thank all Dessie Referral Hospital staffs for their cooperation for the accomplishment of this study.
Funding
This study was fully funded by the Wollo University.
Author information
Authors and Affiliations
Contributions
DGF, AA and HB involved in proposal writing, designed the study and participated in all implementation stages of the project. DGF and AA also analysed the data and finalized the write up of the manuscript. DGF, AA and HB were responsible for critically revising the proposal and the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written consent form was used to ask patients or guardians for their willingness. Ethical clearance was obtained from the institutional review board of Wollo University, College of Medicines and Health Sciences. Individuals who were positive for intestinal parasite were treated with an appropriate anti-parasitic drugs in the study Hospital.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Feleke, D.G., Ali, A., Bisetegn, H. et al. Intestinal parasitic infections and associated factors among people living with HIV attending Dessie Referral Hospital, Dessie town, North-east Ethiopia: a cross-sectional study. AIDS Res Ther 19, 19 (2022). https://doi.org/10.1186/s12981-022-00443-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12981-022-00443-6