
Abstract
Background
Depression is considered to be an immune-related disease; however, previous studies have focused on inflammatory factors, and there is no conclusive conclusion on the relationships between immunoglobulins and depression. Therefore, the objective of this cross-sectional study was to evaluate the associations between immunoglobulins and depressive symptoms in Chinese older adults.
Results
The China Hainan Centenarian Cohort Study (CHCCS) provides a significant population-based sample of older adults in Hainan, China. A total of 1547 older adults were included in this study. A baseline survey was conducted using a structured questionnaire. Blood samples were obtained following standard procedures. The Geriatric Depression Scale (GDS-15) was used to evaluate depressive symptoms of the participants. This sample of older adults had a median age of 94.75 (range: 80–116) years, and the proportion of women was 72.07%. The prevalence of older adults with depressive symptoms was 20.36% (315 older adults). After adjusting for all covariates, we found that immunoglobulin A levels were positively associated with depression. The adjusted reliability of the association between immunoglobulin A and depression was 0.106 (beta) and 1.083 (odds ratio) (P < 0.05 for both).
Conclusions
The present study provides epidemiological evidence that depression has significant associations with immunoglobulin A levels in older adults. Further research should be conducted on the effects of regulating immunoglobulin A to improve depressive symptoms.
Similar content being viewed by others


Background
Depression is the main cause of suicide, with alterations in mood and emotion as the main clinical features [1, 2]. According to World Health Organization reports, major depression will rank as the leading cause of disease burden worldwide by 2030 [3]. Recent studies have found that the vicious cycle of "mental-nerve-immunity" is an important pathway regarding the occurrence and aggravation of depressive symptoms, which is mainly manifested by abnormal levels of immune factors [4]. Among these factors, immunoglobulin A exerts a variety of anti-inflammatory effects by interfering with the complement innate immune system and inhibiting the release of proinflammatory cytokines [5, 6]. Abnormal levels of immunoglobulin A could disrupt the balance between proinflammatory and anti-inflammatory reactions in the body, which is generally believed to be closely related to the occurrence of depression; however, there have been some differences in specific conclusions [7, 8]. Takagi and Ohira [9] found that patients with depression have higher levels of immunoglobulin A in the saliva. However, Kawano and Emori [10] reported that breast milk solute immunoglobulin A levels were negatively correlated with emotional abnormalities such as depression and anxiety in patients with postpartum depression.
Previous studies have found that old age is an independent risk factor for depression [11]. Researchers [12, 13] have realized that immunoglobulin A levels were closely associated with age in older adults. Immunoglobulin A levels were found to increase with age in a study involving 8768 participants with a median age of 62 years [14]. However, there is little evidence regarding whether immunoglobulin levels are related to depression in older adults. In previous studies, immunoglobulin A levels were lower in Caucasians and showed no significant differences across other ethnicities [12,13,14]. In addition, data on the associations between immunoglobulins and depression in Asian populations are scarce, especially for Chinese older adults. Therefore, using the database from the China Hainan Centenarian Cohort Study (CHCCS), this cross-sectional study aimed to identify the associations between immunoglobulins and depression in Chinese older adults to provide a reference for the prevention and treatment of depression.
Results
This study included 1115 women (72.07%) and 432 men (27.93%). These older adults had a median age of 94.75 (range: 80–116) years. The prevalence of depression in the total sample was 20.36% (315 older adults). The mean ± standard deviation levels of immunoglobulin A were 3.79 ± 2.29 g/dL for the depression group and 3.51 ± 1.57 g/dL for the nondepression group (P < 0.001; Fig. 1b). As Table 1 shows, the group of older adults with depression were older, had a higher percentage of women, had higher levels of immunoglobulin A, and had lower levels of RBC, hemoglobin, immunoglobulin M and complement C3 than the group without depression (P < 0.05 for all).

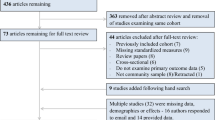
a The flowchart of participants in this study; b Immunoglobulin A, immunoglobulin M and complement C3 levels in older adults with and without depression
By multivariate linear regression analyses, we found that immunoglobulin A levels were positively associated with Geriatric Depression Scale (GDS-15) (P < 0.05 for all, Table 2). The beta value for immunoglobulin A after adjusting for all covariates was 0.106 (95% CI: 0.016–0.195, P < 0.05). Table 3 shows the results from multivariate logistic regression analyses. The participants who had higher immunoglobulin A levels tended to have higher odds of depression (P < 0.05 for all). The adjusted odds ratio between immunoglobulin A and depressive symptoms after adjusting for all covariates was 1.083 (95% CI: 1.001–1.172, P < 0.05).
Discussion
In our study, older women reported depressive symptoms more frequently than older men, and there was a significant correlation between immunoglobulin A levels and depression. After adjusting for the covariates, this association remained significant. Based on this study, we confirmed that immunoglobulin A is a good biomarker that could be used to effectively identify those with depression and, the mechanism involved in regulating immunoglobulin A levels might be responsible for the development of depression.
It is well known that immunoglobulins are closely related to the occurrence of depressive symptoms in specific populations [15, 16]. Denitsa revealed that major depression was accompanied by higher serum immunoglobulin M/A responses, and compared with controls, depressive patients showed higher immunoglobulin A responses to Citrobacter koseri, which might be related to the microbe-gut-brain axis [4]. Francois found that immunoglobulin M levels were positively correlated with girls’ anxiety scores among 1199 adolescents (636 girls) in the Netherlands [17]. Another study involving mothers with major depression and their children revealed that mothers had higher levels of solute immunoglobulin A in their saliva and showed more negative emotions, including negative influence, intrusion, and criticism; correspondingly, their children showed higher levels of solute immunoglobulin A and greater social withdrawal [18]. In this study, immunoglobulin A levels were found to be associated with depression in Chinese older adults.
The mechanism through which immunoglobulins play a negative role in mental health is not clearly understood, but some studies have shown that immunoglobulins are related to neurotransmitter abnormalities [19]. Buranee found that immunoglobulins A and M could affect the regulation of central neural and glial activity through the tryptophan catabolite pathway by increasing the expression of picolinic acid and decreasing the concentration of quinolinic acid, which leads to physiological somatic symptoms [20, 21]. In addition, an increase in solute immunoglobulin A levels is not only a triggering factor of stress but also an aggravating factor for further stress. These mechanisms are related to the gut-brain axis and hypothalamic–pituitary–adrenal axis [22, 23]. Moreover, it has been reported that the paired immunoglobulin receptor B is related to inhibition of axon regeneration [24]. Secreted protein acidic and rich in cysteine-related protein containing immunoglobulin domains 1 could bind to pro-brain derived neurotrophic factor, negatively regulate its potential maturation, and affect brain nerve function, especially learning and memory processes [25].
This study has several limitations. First, as an observational and cross-sectional study, it cannot prove causality of the association between immunoglobulins and depression. Second, effective validation with further studies is necessary to determine the external validity or generalizability of our findings.
Conclusions
The present study provides epidemiological evidence that immunoglobulin A levels have significant associations with depression in Chinese older adults. Further research should be conducted on the effects of regulating immunoglobulin A to improve depressive symptoms.
Methods
Participants
From June 2014 to December 2016, the CHCCS investigated older adults aged 80 years or older from 18 regions throughout Hainan, China. Based on a demographics list provided by the Department of Civil Affairs, the CHCCS enrolled a total of 1797 older adults [992 centenarians (55.20%) and 805 oldest-old adults (aged 80–99 years; 44.80%)]. All participants were community-dwelling older adults (Fig. 1a). The cohort profile and investigation method have been described previously [26]. The participants were assessed by neurologists who could communicate with them, and none of the participants had severe dementia or cognitive impairment, which made them unable to complete the GDS-15. After excluding 250 participants with missing GDS-15 (107 participants) or missing immunoglobulin levels (143 participants), the final analysis included data from 1547 participants [837 centenarians (54.10%) and 710 oldest-old adults (aged 80–99 years; 45.90%); Table 4]. The study protocol was approved by the Ethics Committee of Hainan Hospital of Chinese People's Liberation Army General Hospital (Sanya, China; Number: 301hn11201601). All participants gave their informed consent.
Standard procedures
A baseline survey including epidemiological questionnaires, physical examination, and laboratory tests was conducted through a household survey of face-to-face interviews by the multidisciplinary research team consisting of geriatricians, neurologists, cardiologists, endocrinologists, nephrologists and nurses. All home interview surveyors were strictly trained, and physical examination were conducted following standard procedures [27, 28]. Age and sex were registered according to the second-generation identification card information of older adults. The operator measured the systolic and diastolic blood pressure of older adults who took a sitting position by electronic sphygmomanometers (Omron Hem-7200, Japan). Each parameter was measured twice and averaged, with at least a one-minute interval between the two measurements. The GDS-15 was used to measure depressive symptoms of the participants [29]. The scale had a maximal total score of 15 points and comprised 15 dichotomous items (possible range: 0–15) [29]. Depression was diagnosed by experienced neurologists based on the GDS-15 in combination with medical records and clinical symptoms by communicating with the participants and their family members. Scales > 6 were identified as potential depression, and higher scales indicated more severe symptoms of depression.
Samples of venous blood were obtained from all fasting participants by professional nurses and transported within 4 h in cold storage (4 °C) to the central laboratory. Red blood cell (RBC), hemoglobin, mean corpuscular hemoglobin concentration (MCHC), white blood cell (WBC), and neutrophil were detected by a blood autoanalyzer (SYSMEX XS-800I). Serum levels of immunoglobulin A, immunoglobulin G, immunoglobulin M, immunoglobulin E, complement C3, complement C4, and C-reactive protein (CRP) were determined by enzyme colorimetry (Roche Products Ltd., Basel, Switzerland) on a fully automatic biochemical autoanalyzer (COBAS c702; Roche Products Ltd.).
Statistical analyses
Continuous variables are described as the mean ± standard deviation, which were compared using Student’s t tests. Categorical variables are described as percentages, which were compared using chi-square tests. Multivariate linear regression analyses were used to analyze the associations between immunoglobulins and depression. Multivariate logistic regression analyses were performed to determine independent correlates of depressive symptoms. All these were adjusted for in three models: Model 1: no adjustment; Model 2: adjusted for age, sex, and ethnicity; Model 3: age, sex, ethnicity, centenarians, systolic blood pressure (SBP), diastolic blood pressure (DBP), RBC, hemoglobin, MCHC, WBC, neutrophil, CRP, immunoglobulin A, immunoglobulin G, immunoglobulin M, immunoglobulin E, complement C3, and complement C4. Statistical analyses were performed with the SPSS 17.0 software package (Chicago, IL, USA). P values < 0.05 were considered statistically significant, and confidence intervals (CIs) were computed at the 95% level.
Availability of data and materials
The datasets used and analyzed during the present study are available from the corresponding author on reasonable request.
Abbreviations
- CHCCS:
-
China Hainan Centenarian Cohort Study
- CI:
-
Confidence interval
- CRP:
-
C-reactive protein
- DBP:
-
Diastolic blood pressure
- GDS-15:
-
Geriatric Depression Scale
- MCHC:
-
Mean corpuscular hemoglobin concentration
- OR:
-
Odds ratio
- RBC:
-
Red blood cell
- SBP:
-
Systolic blood pressure
- WBC:
-
White blood cell
References
Conejero I, Olié E, Calati R, Ducasse D, Courtet P. Psychological pain, depression, and suicide: recent evidences and future directions. Curr Psychiatry Rep. 2018;20:33.
Ribeiro JD, Huang X, Fox KR, Franklin JC. Depression and hopelessness as risk factors for suicide ideation, attempts and death: meta-analysis of longitudinal studies. Br J Psychiatry. 2018;212:279–86.
Malhi GS, Mann JJ. Depression. Lancet. 2018;392:2299–312.
Simeonova D, Stoyanov D, Leunis JC, Carvalho AF, Kubera M, Murdjeva M, et al. Increased serum immunoglobulin responses to gut commensal gram-negative bacteria in unipolar major depression and bipolar disorder type 1, especially when melancholia is present. Neurotox Res. 2020;37:338–48.
Dowlati Y, Herrmann N, Swardfager W, Liu H, Sham L, Reim EK, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry. 2010;67:446–57.
Beurel E, Toups M, Nemeroff CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. 2020;107:234–56.
Jacob CM, Pastorino AC, Fahl K, Carneiro-Sampaio M, Monteiro RC. Autoimmunity in IgA deficiency: revisiting the role of IgA as a silent housekeeper. J Clin Immunol. 2008;28(Suppl 1):S56-61.
Gold PW, Pavlatou MG, Carlson PJ, Luckenbaugh DA, Costello R, Bonne O, et al. Unmedicated, remitted patients with major depression have decreased serum immunoglobulin A. Neurosci Lett. 2012;520:1–5.
Takagi S, Ohira H. Effects of expression and inhibition of negative emotions on health, mood states, and salivary secretory immunoglobulin A in Japanese mildly depressed undergraduates. Percept Mot Skills. 2004;98:1187–98.
Kawano A, Emori Y. The relationship between maternal postpartum psychological state and breast milk secretory immunoglobulin A level. J Am Psychiatr Nurses Assoc. 2015;21:23–30.
Dao ATM, Nguyen VT, Nguyen HV, Nguyen LTK. Factors associated with depression among the elderly living in urban vietnam. Biomed Res Int. 2018;2018:2370284.
Paganelli R, Quinti I, Fagiolo U, Cossarizza A, Ortolani C, Guerra E, et al. Changes in circulating B cells and immunoglobulin classes and subclasses in a healthy aged population. Clin Exp Immunol. 1992;90:351–4.
Khan SR, van der Burgh AC, Peeters RP, van Hagen PM, Dalm V, Chaker L. Determinants of serum immunoglobulin levels: a systematic review and meta-analysis. Front Immunol. 2021;12: 664526.
Khan SR, Chaker L, Ikram MA, Peeters RP, van Hagen PM, Dalm V. Determinants and reference ranges of serum immunoglobulins in middle-aged and elderly individuals: a population-based study. J Clin Immunol. 2021;41:1902–14.
Farnam A, Majidi J, Nourazar SG, Ghojazadeh M, Movassaghpour A, Zolbanin SM. Effect of anger patterns and depression on serum IgA and NK cell frequency. Iran J Immunol. 2016;13:37–44.
Chojnowska S, Ptaszyńska-Sarosiek I, Kępka A, Knaś M, Waszkiewicz N. Salivary biomarkers of stress, anxiety and depression. J Clin Med. 2021;10:517.
François M, Schaefer JM, Bole-Feysot C, Déchelotte P, Verhulst FC, Fetissov SO. Ghrelin-reactive immunoglobulins and anxiety, depression and stress-induced cortisol response in adolescents. The TRAILS study. Prog Neuropsychopharmacol Biol Psychiatry. 2015;59:1–7.
Ulmer-Yaniv A, Djalovski A, Priel A, Zagoory-Sharon O, Feldman R. Maternal depression alters stress and immune biomarkers in mother and child. Depress Anxiety. 2018;35:1145–57.
He S, Philbrook A, McWhirter R, Gabel CV, Taub DG, Carter MH, et al. Transcriptional control of synaptic remodeling through regulated expression of an immunoglobulin superfamily protein. Curr Biol. 2015;25:2541–8.
Kanchanatawan B, Sirivichayakul S, Carvalho AF, Anderson G, Galecki P, Maes M. Depressive, anxiety and hypomanic symptoms in schizophrenia may be driven by tryptophan catabolite (TRYCAT) patterning of IgA and IgM responses directed to TRYCATs. Prog Neuropsychopharmacol Biol Psychiatry. 2018;80:205–16.
Kanchanatawan B, Sirivichayakul S, Thika S, Ruxrungtham K, Carvalho AF, Geffard M, et al. Physio-somatic symptoms in schizophrenia: association with depression, anxiety, neurocognitive deficits and the tryptophan catabolite pathway. Metab Brain Dis. 2017;32:1003–16.
Campos-Rodríguez R, Godínez-Victoria M, Abarca-Rojano E, Pacheco-Yépez J, Reyna-Garfias H, Barbosa-Cabrera RE, et al. Stress modulates intestinal secretory immunoglobulin A. Front Integr Neurosci. 2013;7:86.
Reyna-Garfias H, Miliar A, Jarillo-Luna A, Rivera-Aguilar V, Pacheco-Yepez J, Baeza I, et al. Repeated restraint stress increases IgA concentration in rat small intestine. Brain Behav Immun. 2010;24:110–8.
Liu J, Wang Y, Fu W. Axon regeneration impediment: the role of paired immunoglobulin-like receptor B. Neural Regen Res. 2015;10:1338–42.
Suzuki R, Fujikawa A, Komatsu Y, Kuboyama K, Tanga N, Noda M. Enhanced extinction of aversive memories in mice lacking SPARC-related protein containing immunoglobulin domains 1 (SPIG1/FSTL4). Neurobiol Learn Mem. 2018;152:61–70.
Fu S, Hu J, Chen X, Li B, Shun H, Deng J, et al. Mutant single nucleotide polymorphism rs189037 in ataxia-telangiectasia mutated gene is significantly associated with ventricular wall thickness and human lifespan. Front Cardiovasc Med. 2021;8:658908.
Fu S, Ping P, Li Y, Li B, Zhao Y, Yao Y, et al. Centenarian longevity had inverse relationships with nutritional status and abdominal obesity and positive relationships with sex hormones and bone turnover in the oldest females. J Transl Med. 2021;19:436.
Yao Y, Fu S, Zhang H, Li N, Zhu Q, Zhang F, et al. The prevalence of depressive symptoms in Chinese longevous persons and its correlation with vitamin D status. BMC Geriatr. 2018;18:198.
Almeida OP, Almeida SA. Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int J Geriatr Psychiatry. 1999;14:858–65.
Acknowledgements
We appreciate all those who participated in the present study for their continued cooperation.
Funding
This work was supported by grants from the National Natural Science Foundation of China (81900357, 81903392, 81941021, 81901252, 82001476, 81802804, and 81801251), the Military Medical Science and Technology Youth Incubation Program (20QNPY110 and 19QNP060), the Excellent Youth Incubation Program of Chinese People’s Liberation Army General Hospital (2020-YQPY-007), the Natural Science Foundation of Hainan Province (821QN389 and 821MS112), the Military Medicine Youth Program of Chinese People’s Liberation Army General Hospital (QNF19069 and QNF19068), the National Key R&D Program of China (2018YFC2000400), the National S&D Resource Sharing Service Platform Project of China (YCZYPT[2018]07), the Specific Research Fund of the Innovation Platform for Academicians of Hainan Province (YSPTZX202216), the Hainan Major Scientific and Technological Cooperation Project (2016KJHZ0039), the China Postdoctoral Science Foundation funded project (2019M650359, 2020M682816, and 2021T140298), Young Elite Scientists Sponsorship Program by CAST (2021QNRC001), the Medical Big Data R&D Project of Chinese People’s Liberation Army General Hospital (MBD2018030), the National Geriatric Disease Clinical Medicine Research Center Project (NCRCG-PLAGH-2017–014), the Central Health Care Scientific Research Project (W2017BJ12), the Hainan Medical and Health Research Project (16A200057), the Sanya Medical and Health Science and Technology Innovation Project (2016YW21, 2017YW22, and 2018YW11), and the Clinical Scientific Research Supporting Fund of Chinese People’s Liberation Army General Hospital (2017FC-CXYY-3009). The sponsors had no role in the design, conduct, interpretation, review, approval or control of this article.
Author information
Authors and Affiliations
Contributions
YLZ, YY and SF designed the study and performed the investigation. ZS and YJZ conducted statistical analysis and drafted the manuscript. PZ, JL, YZ, and ZH revised the manuscript. The authors declare that they have no conflicts of interest. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The present study was approved by the ethics committee of Hainan Hospital of Chinese People's Liberation Army General Hospital (301hn11201601). Informed consent was obtained from all participants and legal guardians.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sun, Z., Lin, J., Zhang, Y. et al. Association between immunoglobulin A and depression in Chinese older adults: findings from a cross-sectional study. Immun Ageing 19, 21 (2022). https://doi.org/10.1186/s12979-022-00283-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12979-022-00283-y