
Abstract
Background
Female genital fistula is a traumatic debilitating injury, frequently caused by prolonged obstructed labor, affecting between 500,000-2 million women in lower-resource settings. Vesicovaginal fistula causes urinary incontinence, and other morbidity may occur during fistula development. Women with fistula are stigmatized, limit social and economic engagement, and experience psychiatric morbidity. Improved surgical access has reduced fistula consequences yet post-repair risks impacting quality of life and well-being include fistula repair breakdown or recurrence and ongoing or changing urine leakage or incontinence. Limited evidence on risk factors contributing to adverse outcomes hinders interventions to mitigate adverse events. This study aims to quantify these adverse risks and inform clinical and counseling interventions to optimize women’s health and quality of life following fistula repair through: identifying predictors and characteristics of post-repair fistula breakdown and recurrence (Objective 1) and post-repair incontinence (Objective 2), and to identify feasible and acceptable intervention strategies (Objective 3).
Methods
This mixed-methods study incorporates a prospective cohort of women with successful vesicovaginal fistula repair at approximately 12 fistula repair centers in Uganda (Objectives 1-2) followed by qualitative inquiry among key stakeholders (Objective 3). Cohort participants will have a baseline visit at the time of surgery followed by data collection at 2 weeks, 6 weeks, 3 months and quarterly thereafter for 3 years. Primary predictors to be evaluated include patient-related factors, fistula-related factors, fistula repair-related factors, and post-repair behaviors and exposures, collected via structured questionnaire at all data collection points. Clinical exams will be conducted at baseline, 2 weeks post-surgery, and for outcome confirmation at symptom development. Primary outcomes are fistula repair breakdown or fistula recurrence and post-repair incontinence. In-depth interviews will be conducted with cohort participants (n ~ 40) and other key stakeholders (~ 40 including family, peers, community members and clinical/social service providers) to inform feasibility and acceptability of recommendations.
Discussion
Participant recruitment is underway. This study is expected to identify key predictors that can directly improve fistula repair and post-repair programs and women’s outcomes, optimizing health and quality of life. Furthermore, our study will create a comprehensive longitudinal dataset capable of supporting broad inquiry into post-fistula repair health.
Trial Registration ClinicalTrials.gov Identifier: NCT05437939.
Plain english summary
Female genital fistula is a traumatic birth injury which occurs where access to emergency childbirth care is poor. It causes uncontrollable urine leakage and is associated with other physical and psychological symptoms. Due to the urine leakage and its odor, women with fistula are stigmatized which has mental health and economic consequences. Ensuring women’s access to fistula surgery and ongoing wellbeing is important for limiting the impact of fistula. After fistula surgery, health risks such as fistula repair breakdown or recurrence or changes to urine leakage can happen, but studies during this time are limited. Our study seeks to measure these health risks and factors influencing these risks quantitatively, and work with patients, community members, and fistula care providers to come up with solutions. We will recruit up to 1000 participants into our study at the time of fistula surgery and follow them for three years. We will collect data on patient sociodemographic characteristics, clinical history, and behavior after fistula repair through patient survey and medical record review. If participants have changes in urine leakage, they will be asked to return to the fistula repair hospital for exam. We will interview about 80 individuals to obtain their ideas for feasible and acceptable intervention options. We expect that this study will help to understand risk factors for poor health following fistula repair and, eventually, improve women’s health and quality of life after fistula.
Similar content being viewed by others


Background
Female genital fistula is a traumatic debilitating injury affecting somewhere between 500,000 to 2 million women, mostly in sub-Saharan Africa, with up to 100,000 annual incident cases [1, 2]. Most often caused by prolonged obstructed labor in lower-resource settings, other etiologies are iatrogenic or traumatic. Many fistula-causing births result in stillbirth [3]. Women with fistula experience uncontrollable urinary and/or fecal leakage through the vagina [3,4,5]. Other consequences of obstructed labor injury complex include neurologic, gynecologic, and orthopedic injury, resulting in pain, weakness, difficulty walking and secondary infertility [6]. Women with fistula are stigmatized, which restricts their participation in social and economic activities [3, 6], and report substantial psychiatric morbidity [7].
Improved global surgical access has reduced the significant physical, psychosocial, and economic consequences of fistula, although women with successful surgery may continue to face adverse post-repair outcomes. Surgical repair breakdown or fistula recurrence rates range from 2.1–18.4%, largely occurring within the first 12 months following surgery [8,9,10]. Incontinence continues post-repair among about one-third of women despite fistula closure [11, 12], and some develop incident incontinence despite initial post-surgical resolution [9, 10]. From the patient perspective, fistula closure and persistent incontinence present similarly and perpetuate the physical, psychosocial, and economic consequences of fistula [6, 13,14,15].
Neither incidence of adverse post-repair outcomes nor their risk factors are well established, which constrains the development and implementation of evidence-based clinical and counseling interventions to mitigate harmful processes. Most prospective research focuses on repair failure during hospitalization or early clinical-follow up, with sparse data on predictors of later fistula repair breakdown and recurrence. Existing literature points to fistula severity, strenuous activity, sexual intercourse, and pregnancy or childbirth as potential risk factors [8,9,10, 16, 17]. Fistula recurrence can be mechanistically characterized as surgical breakdown or re-injury, thus investigating both biological and social factors important to each potential pathway is key. The enhanced recovery after surgery literature has identified patient counseling, physical conditioning, avoidance of alcohol and smoking, and good nutrition as protective [18]. Surgical site infection, an intermediate factor associated with late breakdown, is more common among patients with co-morbidities, advanced age, risk indices, and lengthier surgery [19]. Factors responsible for re-injury may include the biological and social structures that resulted in development of the first fistula, including limited access to emergency obstetric care. A woman’s risk of fistula recurrence following surgery is likely to be influenced by the biological alterations occurring from both the fistula and the fistula surgery itself.
Urinary incontinence following fistula repair is complex due to the variety of anatomic and functional factors at play which often remain uncharacterized, particularly over time [20]. Research on potential intervention points for reducing persistent and incident post-repair incontinence is limited by the breadth of factors assessed, lack of differentiation between incontinence types, and lack of longitudinal follow-up. Predictors of immediate post-repair incontinence include fistula severity, including size and location, presence of vaginal scarring, and shorter urethral length [11, 21, 22]. Less is known about incident incontinence following successful surgical resolution.
Our research aims to understand adverse risks and inform clinical and counseling interventions to optimize women’s health and quality of life following fistula repair. We have developed a mixed-methods research study incorporating a longitudinal cohort to robustly identify predictors of fistula repair breakdown and recurrence (Objective 1), identify predictors and characteristics of post-repair incontinence (Objective 2), supplemented by qualitative work among key stakeholders to identify feasible and acceptable strategies for modifying key risk factors of adverse outcomes (Objective 3). These three objectives are expected to tangibly inform the development of clinical and counseling interventions to mitigate complications, improve post-surgical outcomes and quality of life. We employ a mixed-methods approach to enhance our understanding of the quantitative findings and ensure that intervention recommendations resulting from this study are informed by feasibility and acceptability considerations from women with fistula, families, and health and social providers. Our investigative approach seeks to elucidate factors essential for determining risk of post-surgical adverse outcome, thereby leading to appropriately targeted and contextually-adapted interventions, and will identify priority research areas needed for women with continued poor outcomes. Our research is situated in Uganda which has one of the highest lifetime fistula symptom prevalences globally of 19.2 per 1,000 reproductive aged women and annual incidence of ~ 5,000 [23, 24], despite this, no research on fistula recurrence and risk factors has been conducted to date in Uganda.
Methods
This sequential explanatory mixed-methods study is guided by a conceptual framework (Fig. 1) highlighting factors to be explored including both invariable and potentially mutable factors to develop the evidence base that will allow women undergoing fistula repair to maintain their reproductive and overall health over time. The ClinicalTrials.gov identifier is NCT05437939.

Summarized conceptual framework between predictors and adverse fistula outcomes
Study setting and sites
Uganda’s National Fistula Technical Working Group (est. 2002) has focused on increasing fistula surgery availability [25]. Fistula surgery is available at 20 centers of excellence in Uganda, with 25 trained surgeons within national and regional referral hospitals. Regional literature suggests fistula repair is successful among ~ 80% of affected women. [26, 27]
Research sites are approximately 12 fistula repair facilities across Uganda (Fig. 2). Some sites conduct routine surgeries within ongoing urogynecological services only, others conduct fistula repair camps only, and others combine both routine care and camp models. Patients under the care of study providers and research assistants at alternative care locations will be eligible for study participation if they meet study eligibility criteria.

Partnering fistula repair study sites across Uganda
Longitudinal cohort study
Our study will recruit a longitudinal cohort of 1,000 women with successful (closed) vesicovaginal fistula repair (~ 48 h after surgery). Participants will be followed for 3 years in total, with data collected via questionnaire at baseline (surgery), 2 weeks (hospital discharge), 6 weeks, 3 months and quarterly thereafter (Fig. 3).

Overview of study data collection and timeline
Inclusion and exclusion criteria
Inclusion criteria are vesicovaginal fistula, completed fistula surgery with confirmed closure, age 15 or above (where individuals 15–17 meet Ugandan legal criteria for emancipation), and capable and willing to provide informed consent. Exclusion criteria are do not live within a feasible location for follow-up, operationalized by return travel back to fistula repair facility and cellular telephone network. Potential participants with prior fistula repair will not be excluded.
In the case of fresh fistula limited in size (< 2cm) and time since occurrence (< 3 months), catheterization alone may successfully heal ~ 10% [28]. If a potential participant’s fistula is eligible for and undergoes catheterization instead of surgery and the fistula is confirmed to be closed, they will be eligible for study enrollment if they meet all other study eligibility criteria.
Study procedures
Study researchers will recruit participants into the cohort following confirmation of successful fistula repair. Potentially eligible women will be identified through review of urogynecology department surgical logbooks, patient medical records, and communication with fistula providers. After fistula repair, women stay at the repair facility for 14 days minimum for post-repair catheterization. The study researcher will approach women who meet inclusion criteria in-person ~ 48 h after surgery to screen for eligibility; explain the study procedures, risks and benefits, and participant rights; invite those eligible to participate; and formally enroll those who agree. The study researcher will then collect participant contact information and administer the baseline questionnaire.
Two-week data collection will occur prior to hospital discharge. Other follow-up data collection (6 weeks and quarterly, starting at 3 months) will occur over mobile phone. Participants with no phone will be provided with a study phone and airtime. Clinical exams will be conducted at baseline and 2 weeks post-surgery for fistula and repair characterization, and data from routine post-surgical follow-up appointments at 6 weeks and 3 months post-repair will inform outcome assessment. Women reporting symptoms on interviewer-administered questionnaire or through other study or clinical communication will return to the fistula repair facility for outcome assessment and clinical care following standard clinical procedures. Transportation costs will be reimbursed for all follow-up data collection required.
Participants will be followed through 36 months post-repair, regardless of outcome and subsequent care. Some participants may undergo multiple fistula surgeries during their study participation. If this occurs, participant follow-up will be adjusted to incorporate data collection at 6 weeks and 3 months following the subsequent surgery, after which regular quarterly data collection will continue through 36 months after the participant’s enrollment.
Measures
Primary predictors to be investigated include patient-related factors, fistula-related factors, fistula repair-related factors, and post-repair behaviors and exposures, collected via structured questionnaire at all follow-up data collection points and from medical records and clinical forms when examinations are performed (Table 1). Supplementary data to characterize incontinence among women with persistent incontinence without fistula breakdown/recurrence and to assess pregnancy-related exposures and outcomes among women reporting pregnancy.
Data analysis
To identify predictors of post-repair fistula breakdown and recurrence (Objective 1), we will first calculate the incidence of post-repair fistula breakdown and recurrence and its 95% confidence interval (CIs) overall by dividing the number of events identified by the total person-time observed. The probability of event-free survival at defined time points will be calculated using the Kaplan–Meier estimate. We will then estimate the individual and joint-effects of the patient, fistula, fistula repair, and post-repair characteristics on time to post-repair fistula breakdown and recurrence in order to identify significant factors in time to post-repair fistula breakdown and recurrence. We will fit proportional hazards frailty survival models to jointly analyze times to post-repair fistula breakdown and recurrence [29]. These models will include a shared frailty at the subject level to accommodate within-subject correlation of times to breakdown and recurrence events and interactions of predictors with event type to accommodate potential differences in the association of predictors with times to the events. These models will also include a shared frailty at the provider level since patients will be clustered within providers within facilities. We will fit the frailty survival models using routines in Stata statistical analysis software (StataCorp, College Station, TX, USA). [30]
Prior to fitting multivariable models, we will calculate the estimated correlation of all potential predictors to identify any highly correlated groups of predictors. We will not include such groups of predictors in any multivariable models. We will assess the adequacy of the proportional hazards assumption through inspection of Schoenfield residuals as a function of time. In the event our data violate the proportional hazards assumption, we will modify our modelling approach to accommodate interactions or stratification, as is most appropriate for the data. We will subsequently fit one multivariable proportional hazards regression model to document the comparative relationship between patient, fistula, fistula repair, and post-repair characteristics and the hazard rate of post-repair fistula breakdown and recurrence integrating all independent variables that were associated with the outcome in bivariable analyses at a conservative p threshold of p < 0.1. Final model selection will be determined via Akaike’s Information Criteria [52]. Secondary analyses will assess time to post-repair fistula breakdown (< 3 months post-repair) and time to fistula recurrence (≥ 3 months post-repair) separately, and by fistula etiology (obstetric versus iatrogenic), although our study is not powered for secondary outcomes.
Other methods will be used to better understand the contribution of risk factors of fistula repair breakdown and recurrence. To overcome the biases inherent to observational research in understanding causal effects [31], we will conduct secondary analyses employing propensity score methods to account for systematic differences between exposed and unexposed participants, allowing effects to be interpreted as causal, similar to a randomized experiment [32,33,34]. For these analyses, we will estimate a series of models for each key modifiable factor of interest, first predicting the probability of exposure using key baseline and other measures deemed to be relevant for developing the treatment weight, followed by analyses of the exposure and outcome incorporating the treatment weight, as described above. Finally, we will seek to construct a classification rule based on predictors using techniques such as recursive partitioning and random forests using routines in R (R Foundation for Statistical Computing, Vienna, Austria) to identify groups of women defined by the exposure characteristics with high probability of adverse outcome. [35]
To identify predictors and characteristics of post-repair incontinence (Objective 2), we will first estimate the proportion of women who experience post-repair incontinence and associated 95% confidence interval at multiple time points (e.g., 6m, 12m, 2y and 3y). Our primary analysis of predictors of persistent post-repair incontinence will focus on incontinence at 3 months, the time point by which incontinence resolvable through surgery will have resolved per expert opinion. We will first estimate bivariable relationships between each predictor and post-repair incontinence using multi-level mixed effects logistic regression modeling procedures in Stata to accommodate our clustered data [36]. Subsequently, we will estimate one multivariable model to understand the independent and joint effects of patient, fistula, fistula repair, and post-repair characteristics on post-repair incontinence at 3m, integrating all independent variables that were associated (p < 0.1) with the outcome in bivariable analyses, addressing correlation as described for Objective 1. To identify predictors of incident post-repair incontinence, we will assess incident post-repair incontinence and factors associated with time to incident post-repair incontinence using the survival analysis methods described for Objective 1. Finally, we will conduct analyses of binary predictors of interest employing propensity scores and seek to develop classification rules following the methods described for Objective 1.
Sample size
The longitudinal cohort study sample size for (up to n = 1000 women) was calculated to provide adequate power to detect a minimum difference in effect by exposures on risk of fistula repair breakdown or recurrence and incontinence of 20% (Objectives 1 and 2) using the log-rank test for two-sample comparison of survivor functions (Objective 1) and the Pearson’s chi-squared two-sample proportions test (Objective 2). These effect differences were determined to be clinically significant based on expert opinion. Power calculations were developed using Stata’s power procedure, with values α = 0.05 and 1−β = 0.80 [36]. Prior research on fistula recurrence risk suggests that factors of interest for our survival analyses (Objective 1) may have hazard ratios ranging from 1.0 to 3.4 [9]. Fig. 4 illustrates the minimum sample size required for estimation of effect estimates ranging from 1.1 to 2.0 with parameters α = 0.05 and 1−β = 0.80, demonstrating adequate power for two-sample comparison of survivor functions (i.e., time to fistula repair breakdown, time to fistula recurrence) with a sample size of 1000 for effect estimates (hazard ratios) of 1.2 or higher, illustrating a 20% or higher risk difference, accommodating some loss to follow-up. Other research has reported repair breakdown or recurrence rates of approximately 15%. With our target sample size of 1000, we anticipate being able to estimate this incidence with precision range 2.5% (i.e., between 12.8 and 17.4%).

Sample size calculations for robust estimation of fistula breakdown or recurrence and persistent incontinence outcomes
Sample size calculations for comparisons between risk factors of post-repair urinary incontinence at 6 and 12 months were estimated using the Pearson’s chi-squared two-sample proportions test with parameters α = 0.05 and 1-β = 0.80. We have estimated risk differences of approximately 10 percentage points, across a range of possibilities, given the lack of informative estimates from the literature. For a potential comparison of 9 percentage points (e.g., from 1 to 10%) we achieve power of 0.80 at approximately 200 study participants (Fig. 4). On the other end of the range (e.g., a comparison between 50 and 60%; Fig. 4), statistical power of 0.80 is achieved with a minimum sample size of 800 participants.
Qualitative component
Qualitative research with key stakeholders will be conducted to expand inform the development of feasible and acceptable intervention concepts targeting risk factors identified from our longitudinal cohort findings (Objectives 1–2).
Study participants
We will enroll approximately 80 individuals in total, including women with fistula, family members, community members, clinical and social service providers, and government. We will purposively sample ~ 40 longitudinal cohort participants to reflect study variability in region and adverse outcome experience. Other key stakeholders (~ 40) will be identified through discussion with study investigators, site leads and research assistants, and other clinical and social service providers for fistula in Uganda, to maximize variability in respondent region and clinical and patient support roles. Identified individuals will be invited to participate over the phone, email, or in-person and those who are interested and are willing to provide informed consent will be scheduled for an in-depth interview with a trained qualitative interviewer at a convenient time and private location. Informed consent for all respondents will be conducted in person, with written or thumbprint confirmation obtained, as appropriate. To respect the privacy and confidentiality of longitudinal cohort participants, permission will first be sought from the research participant before recruiting potential family member or peer qualitative participants.
Study procedures
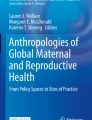
Based on our quantitative findings (Objectives 1 and 2), literature, and expert clinical and contextual experience, the research team will develop a semi-structured and open-ended in-depth interview guide for key stakeholder interviews to obtain a nuanced understanding of their perspectives on feasible and acceptable potential intervention opportunities for addressing key risk and causal factors associated with adverse outcomes. Exploration of intervention possibilities with stakeholders may employ constructs from health behavior theories COM-B (‘capability’, ‘opportunity’, ‘motivation’, and ‘behavior’) model (Fig. 5) and the theoretical domains framework (TDF) for understanding individual and contextual issues, and the Consolidated Framework for Implementation Research (CFIR) for pre-implementation assessment of factors important to successful implementation (i.e., intervention characteristics, inner setting (characteristics of implementing organization), outer setting (features of the external context or environment), and implementation process (strategies or tactics for implementation setup or delivery) [37, 38]. Interviews will be conducted in a private setting by an experienced qualitative interviewer and are anticipated to take 1–2 h. Participants may be asked to respond iteratively as new data arises during the qualitative process. Interviews will be audio recorded and translated into English and transcribed.

COM-B (‘capability’, ‘opportunity’, ‘motivation’, and ‘behavior’) model to inform intervention exploration for qualitative objective. [39]
Data analysis
During the iterative interview and analysis process, we will combine COM-B [39], CFIR [37], and TDF analyses to identify a series of behavioral and implementation targets for each risk factor identified within our quantitative analysis, and for each of these we will 1) classify using the COM-B [39], 2) detail potentially modifiable determinants of behavior (e.g., barriers or facilitators) across CFIR [37] domains, 3), list the theoretical domain and techniques for behavior change using the TDF, and 4) develop and assess potential implementation strategies across multiple actors to achieve the desired change.
Further qualitative data analysis will follow a 2-stage systematic process [40]. The first stage will involve data coding and classification by reviewing the transcripts for potential conceptual categories, using the in-depth interview guide. Two types of codes will be employed: deductive and inductive/emergent. First, deductive codes that represent expected influences will be applied to the data; these will be taken from the existing literature and the theoretical orientation of the interview guide (i.e., COM-B, TFR and CFIR construct list). Next, inductive codes that emerge organically from the data will represent themes that were not expected by the researchers. Emergent themes will be identified based on recurrence rate and on similarities and differences noted across the texts. A codebook will be developed from the themes that will include a detailed description of each code, code inclusion and exclusion criteria, and examples of the code in use. Coded data will be analyzed to describe the different dimensions and commonalities of each theme, their distribution across socio-demographic variables, and the patterns and linkages between themes. Comparisons will be made to detect divergent views among participants and to contrast observations by sample population characteristics and type of key stakeholder.
Sample size
The qualitative sample size was selected on the basis of our prior experience with thematic saturation from our research among women with fistula in the Ugandan context; however, final sample size will be determined through iterative assessment of thematic saturation as data are collected across different participant types. [41]
Ethical approval
The study protocol was approved by the Makerere University School of Medicine Research and Ethics Committee (Ref#: 2021–277), the Uganda National Council for Science and Technology (REF#: HS2033ES), and the University of California, San Francisco Human Research Protection Program, Committee on Human Research (IRB# 21–33559). All individuals eligible for participation will undergo an informed consent process prior to enrollment; individuals unable to provide signatures for informed consent will provide thumbprint confirmation. All study procedures will be performed in accordance with the relevant guidelines and regulations.
Discussion
This study activities described in this protocol seek to estimate the contribution of a broad range of potential risk factors of key adverse outcomes following genital fistula repair: fistula repair breakdown or recurrence, persistent urinary incontinence, and incident urinary incontinence. We hope to overcome several key limitations to the current evidence base through recruiting a sample size capable of robust assessment, employing a longitudinal design to enable evaluation of time-varying contributors and a longer time frame through extending participant follow-up. We will focus on a broad range of patient, clinical, and behavioral characteristics to best inform the development of relevant clinical care interventions, paying particular attention to those that are modifiable without excluding those currently considered unmodifiable, which will guide us to identifying subgroups at highest risk for ensuring care engagement and influence subsequent research priorities.
The results of this study are expected to inform key intervention targets for integration into clinical and counseling interventions to mitigate these risks and ensure women’s high quality of life following genital fistula repair. We will engage key stakeholders (e.g., women with fistula, family members, community members, clinical and social service providers, government) in the interpretation of our findings and strategy development activities to improve the translation of our quantitative findings into feasible and acceptable intervention possibilities. Study progress and findings will be shared with national and global fistula and maternal health stakeholders through dissemination meetings, reports, presentations, and papers.
The next steps of this research program include intervention development, employing the strategies arising from the proposed research, assessment of acceptability and feasibility, and testing for effectiveness. This broader program is likely to result in tangible recommendations and intervention strategies for improving women’s health and wellbeing following genital fistula repair in the short and long term, allowing them to move on to healthy and productive lives. This work is an important corollary to existing efforts to increase access to genital fistula surgery among the estimated 500,000–2 million women currently living with this condition. [1, 2]
In addition to informing an important evidence gap, establishing a large longitudinal cohort such as this represents an important opportunity to develop a resource for investigating other important research questions on the period following genital fistula repair, including those focused on other physical concerns and psychosocial trajectories and outcomes, and we will encourage and support investigation in these areas through professional development among research team members, collaborating with other researchers, and developing capacity through the involvement of trainees in our project.
Study enrollment activities began in May 2022 and are currently ongoing. A total of 441 longitudinal cohort participants have been enrolled through November 2023.
Availability of data and materials
The datasets to be generated during and analyzed during the current study will be de-identified and made publicly available after the study is complete and all planned analyses are achieved.
Abbreviations
- COM-B:
-
Capability, opportunity, motivation, and behavior framework
- CFIR:
-
Consolidated framework for implementation research
- M:
-
Month
- NGO:
-
Non-governmental organization
- TDF:
-
Theoretical domains framework
- Y:
-
Year
References
de Bernis L. Obstetric fistula: guiding principles for clinical management and programme development, a new WHO guideline. Int J Gynaecol Obstet. 2007;99(Suppl 1):S117–21.
United Nations General Assembly. Intensifying efforts to end obstetric fistula within a decade. Report of the Secretary-General. A/75/264. New York, NY: United Nations, 2020.
Wall LL, Arrowsmith SD, Briggs ND, Browning A, Lassey A. The obstetric vesicovaginal fistula in the developing world. Obstet Gynecol Surv. 2005;60(7 Suppl 1):S3–51.
Hilton P. Vesico-vaginal fistulas in developing countries. Int J Gynaecol Obstet. 2003;82(3):285–95.
Hilton P, Ward A. Epidemiological and surgical aspects of urogenital fistulae: a review of 25 years’ experience in southeast Nigeria. Int Urogynecol J Pelvic Floor Dysfunct. 1998;9(4):189–94.
Arrowsmith S, Hamlin EC, Wall LL. Obstructed labor injury complex: obstetric fistula formation and the multifaceted morbidity of maternal birth trauma in the developing world. Obstet Gynecol Surv. 1996;51(9):568–74.
Duko B, Wolka S, Seyoum M, Tantu T. Prevalence of depression among women with obstetric fistula in low-income African countries: a systematic review and meta-analysis. Arch Womens Ment Health. 2021;24(1):1–9.
Nielsen HS, Lindberg L, Nygaard U, et al. A community-based long-term follow up of women undergoing obstetric fistula repair in rural Ethiopia. BJOG. 2009;116(9):1258–64.
Delamou A, Delvaux T, El Ayadi AM, et al. Fistula recurrence, pregnancy, and childbirth following successful closure of female genital fistula in Guinea: a longitudinal study. Lancet Glob Health. 2017;5(11):e1152–60.
Browning A, Menber B. Women with obstetric fistula in Ethiopia: a 6-month follow-up after surgical treatment. BJOG. 2008;115:1564–9.
Frajzyngier V, Ruminjo J, Barone MA. Factors influencing urinary fistula repair outcomes in developing countries: a systematic review. Am J Obstet Gynecol. 2012;207(4):248–58.
El Ayadi AM, Barageine J, Korn A, et al. Trajectories of women’s physical and psychosocial health following obstetric fistula repair in Uganda: a longitudinal study. Trop Med Int Health. 2019;24(1):53–64.
Khisa AM, Nyamongo IK. Still living with fistula: an exploratory study of the experience of women with obstetric fistula following corrective surgery in West Pokot. Kenya Reprod Health Matters. 2012;20(40):59–66.
Nardos R, Phoutrides EK, Jacobson L, et al. Characteristics of persistent urinary incontinence after successful fistula closure in Ethiopian women. Int Urogynecol J. 2020. https://doi.org/10.1007/s00192-020-04265-w.
El Ayadi AM, Barageine JK, Miller S, et al. Women’s experiences of fistula-related stigma in Uganda: a conceptual framework to inform stigma-reduction interventions. Culture Health Sex. 2020;22(3):352–67.
Wilson AL, Chipeta E, Kalilani-Phiri L, Taulo F, Tsui AO. Fertility and pregnancy outcomes among women with obstetric fistula in rural Malawi. Int J Gynaecol Obstet. 2011;113(3):196–8.
Akpak YK, Yenidede I, Kilicci C. Evaluation of etiology, characteristics, and treatment of patients with vesicovaginal fistula observed in rural Africa. J Gynecol Obstet Hum Reprod. 2021;50(6): 101879.
Azhar RA, Bochner B, Catto J, et al. Enhanced recovery after urological surgery: a contemporary systematic review of outcomes, key elements, and research needs. Eur Urol. 2016;70(1):176–87.
Korol E, Johnston K, Waser N, et al. A systematic review of risk factors associated with surgical site infections among surgical patients. PloS One. 2013;8(12):e83743.
Goh JT, Krause H, Tessema AB, Abraha G. Urinary symptoms and urodynamics following obstetric genitourinary fistula repair. Int Urogynecol J. 2013;24(6):947–51.
Bengtson AM, Kopp D, Tang JH, Chipungu E, Moyo M, Wilkinson J. Identifying patients with vesicovaginal fistula at high risk of urinary incontinence after surgery. Obstet Gynecol. 2016;128(5):945–53.
Browning A. Risk factors for developing residual urinary incontinence after obstetric fistula repair. BJOG. 2006;113(4):482–5.
Uganda Bureau of Statistics ICF. Uganda demographic and health survey 2016. Kampala, Uganda: UBOS and ICF; 2018.
Uganda Ministry of Health. National Obstetric Fistula Strategy 2011/2012–2015/2016. Kampala: Uganda Ministry of Health; 2011.
Direct Relief. Global Fistula Map. 2013. http://www.globalfistulamap.org/. Accessed Nov 1 2015.
Kayondo M, Wasswa S, Kabakyenga J, et al. Predictors and outcome of surgical repair of obstetric fistula at a regional referral hospital, Mbarara, western Uganda. BMC Urol. 2011;11(1):23.
McCurdie FK, Moffatt J, Jones K. Vesicovaginal fistula in Uganda. J Obstet Gynaecol. 2018;38(6):822–7.
Waaldijk K. The immediate management of fresh obstetric fistulas. Am J Obstet Gynecol. 2004;191(3):795–9.
Kalbfleisch JD, Prentice RL. The statistical analysis of failure time data. 2nd ed. New York: Wiley; 2002.
Gutierrez R. Parametric frailty and shared frailty survival models. Stata J. 2002;2:22–44.
Hernan MA, Robins JM. Estimating causal effects from epidemiological data. J Epidemiol Commun Health. 2006;60(7):578–86.
Rosenbaum PR. Model-based direct adjustment. J Am Stat Assoc. 1987;82(398):387–94.
Hirano K, Imbens GW. The propensity score with continuous treatments. In: Gelman A, Meng XL, editors. Applied Bayesian modeling and causal inference from incomplete-data perspectives. West Sussex, England: Wiley; 2004.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Statistics Med. 2015;34(28):3661–79.
Strobl C, Malley J Fau - Tutz G, Tutz G. An introduction to recursive partitioning: rationale, application, and characteristics of classification and regression trees, bagging, and random forests. (1939–1463 (Electronic)).
Lp S. Stata 16 base reference manual. College Station, TX: Stata Press; 2019.
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4:50.
Keith RE, Crosson JC, O’Malley AS, Cromp D, Taylor EF. Using the consolidated framework for implementation research (CFIR) to produce actionable findings: a rapid-cycle evaluation approach to improving implementation. Implement Sci. 2017;12(1):15.
Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42.
Bernard HR, Ryan GW. Analyzing qualitative data: systematic approaches. Thousand Oaks, CA: SAGE Publication, Inc.; 2010.
Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. 2018;52(4):1893–907.
Coates J, Swindale A, Bilinksy P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access: Indicator Guide. Washington, D.C.:: FHI 360/FANTA, 2007.
Üstün TB, Kostanjsek N, Chatterji S, Rehm J. Measuring health and disability: Manual for WHO disability assessment schedule WHODAS 2.0: World Health Organization; 2010.
Klovning A, Avery K, Sandvik H, Hunskaar S. Comparison of two questionnaires for assessing the severity of urinary incontinence: the ICIQ-UI SF versus the incontinence severity index. Neurourol Urodyn. 2009;28(5):411–5.
Jackson S, Donovan J, Brookes S, Eckford S, Swithinbank L, Abrams P. The bristol female lower urinary tract symptoms questionnaire: development and psychometric testing. Br J Urol. 1996;77(6):805–12.
Lee PH, Macfarlane DJ, Lam TH, Stewart SM. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review.
García-Moreno C, Organization WH. WHO multi-country study on women’s health and domestic violence against women initial results on prevalence, health outcomes and women’s responses. Geneva: World Health Organization; 2005.
International Center for Research on Women. Estimating the costs and impacts of intimate partner violence in developing countries: a methodological resource guide. Washington, DC: International Center for Research on Women; 2016.
Rogers GR, Villarreal A, Kammerer-Doak D, Qualls C. Sexual function in women with and without urinary incontinence and/or pelvic organ prolapse. Int Urogynecol J Pelvic Floor Dysfunct. 2001;12(6):361–5.
Butchart A. Couple founctionality assessment took (CFAT). Baltimore, MD: Catholic Relief Services; 2016.
Conroy AA, Ruark A, Neilands TB, et al. Development and validation of the couple sexual satisfaction scale for HIV and sexual health research. Arch Sex Behav. 2021;50(7):3297–311.
Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption–II. Addiction. 1993;88(6):791–804.
Group GATSC. Global adult tobaccy survey (GATS): core questionnaire with optional questions. Atlanta, GA: Centers for Disease Control and Prevention; 2020.
Landrum R. College students’ use of caffeine and its relationship to personality. Coll Stud J. 1992;26(2):151–5.
Ayadi El A, Nalubwama H, Barageine J, et al. Development and preliminary validation of a post-fistula repair reintegration instrument among Ugandan women. Reprod Health. 2017;14(1):109.
Webster J, Nicholas C, Velacott C, Cridland N, Fawcett L. Validation of the WHOQOL-BREF among women following childbirth. Aust N Z J Obstet Gynaecol. 2010;50(2):132–7.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13.
Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–7.
Robins RW, Hendin HM, Trzesniewski KH. Measuring global self-esteem: construct validation of a single-item measure and the rosenberg self-esteem scale. Pers Soc Psychol Bull. 2001;27(2):151–61.
El Ayadi AM, Barageine JK, Neilands TB, et al. Validation of an adapted instrument to measure female genital fistula-related stigma. Glob Public Health. 2021;16(7):1057–67.
Nakigudde J, Musisi S, Ehnvall A, Airaksinen E, Agren H. Adaptation of the multidimensional scale of perceived social support in a Ugandan setting. Afr Health Sci. 2009;9(Suppl 1):S35-41.
Osman A, Lamis DA, Freedenthal S, Gutierrez PM, McNaughton-Cassill M. The multidimensional scale of perceived social support: analyses of internal reliability, measurement invariance, and correlates across gender. J Pers Assess. 2014;96(1):103–12.
Sherbourne CD, Stewart AL. The MOS social support survey. Social Sci Med. 1991;32(6):705–14.
Cox CM, Hindin MJ, Otupiri E, Larsen-Reindorf R. Understanding couples’ relationship quality and contraceptive use in Kumasi, Ghana. Int Perspect Sex Reprod Health. 2013;39(4):185–94.
Steinberg R. The triangle of love: intimacy, passion, commitment. New York: Basic; 1987.
Funk JL, Rogge RD. Testing the ruler with item response theory: increasing precision of measurement for relationship satisfaction with the couples satisfaction index. J Fam Psychol. 2007;21(4):572–83.
Larzelere RE, Huston TL. The dyadic trust scale: toward understanding interpersonal trust in close relationships. J Marriage Fam. 1980;42:595–604.
Aron A, Aron EN, Smollan D. Inclusion of other in the self scale and the structure of interpersonal closeness. J Pers Soc Psychol. 1992;63:596–612.
Christensen A, Shenk JL. Communication, conflict, and psychological distance in nondistressed, clinic, and divorcing couples. J Consult Clin Psychol. 1991;59:458–63.
Ayers S, Wright DB, Thornton A. Development of a measure of postpartum PTSD: the city birth trauma scale. Front Psychiatry. 2018;9:409.
Flynn KE, Lin L, Cyranowski JM, et al. Development of the NIH PROMIS ® sexual function and satisfaction measures in patients with cancer. J Sexual Med. 2013;10(01):43–52.
Martínez-Restrepo S, Ramos-Jaimes L, Espino A, Valdivia M, Cueva JY. Measuring Women’s Economic Empowerment: Critical Lessons from South America, 2017.
Acknowledgements
The authors would like to thank our collaborating research sites and team members for their commitments to our research study and study participants, our study participants for sharing their time and experiences with the research team and greater scientific community, and Ashley Mitchell and Susan Awor for supporting research implementation activities.
Funding
This study is funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the US National Institutes of Health (NICHD R01HD101570; PI: El Ayadi). The funders held no role in study design, data collection, analysis and interpretation of data, nor in writing the manuscript.
Author information
Authors and Affiliations
Contributions
AME: conceptualization, methodology, formal analysis, writing—original draft, writing—review and editing, supervision, project administration, funding acquisition. SO: conceptualization, project administration, writing—review and editing. FK: conceptualization, project administration, writing—review and editing. SM: conceptualization, writing—review and editing. AK: conceptualization, writing – review and editing. HN: conceptualization, project administration, writing—review and editing. JN: methodology, writing—review and editing. MG: project administration, writing—review and editing. PE: project administration, writing—review and editing. RT: project administration, writing—review and editing. EA: methodology, writing—review and editing. JB: conceptualization, methodology, writing—original draft, writing—review and editing, supervision, project administration, funding acquisition.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Makerere University School of Medicine Research and Ethics Committee (Ref#: 2021-277), the Uganda National Council for Science and Technology (REF#: HS2033ES), and the University of California, San Francisco Human Research Protection Program, Committee on Human Research (IRB# 21-33559). All individuals eligible for participation will undergo an informed consent process prior to enrollment; individuals unable to provide signatures for informed consent provided thumbprint confirmation. All study methods are performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
El Ayadi, A.M., Obore, S., Kirya, F. et al. Identifying opportunities for prevention of adverse outcomes following female genital fistula repair: protocol for a mixed-methods study in Uganda. Reprod Health 21, 2 (2024). https://doi.org/10.1186/s12978-023-01732-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12978-023-01732-7