
Abstract
Evidence suggests that COVID-19 may impair access to sexual and reproductive health services and safe abortion. The purpose of this systematic review was investigating the changes of abortion services in the COVID-19 pandemic era. We searched PubMed, Web of Science and Scopus for relevant studies published as of August 2021, using relevant keywords. RCT and non-original studies were excluded from the analysis and 17 studies of 151 included in our review. Requests to access medication abortion by telemedicine and demand for self-managed abortion were the main findings of identified studies. Women requested an abortion earlier in their pregnancy, and were satisfied with tele-abortion care due to its flexibility, and ongoing telephone support. Presenting telemedicine services without ultrasound has also been reported. Visits to clinics were reduced based on the severity of the restrictions, and abortion clinics had less revenue, more costs, and more changes in the work style of their healthcare providers. Telemedicine was reported safe, effective, acceptable, and empowering for women. Reasons for using tele-abortion were privacy, secrecy, comfort, using modern contraception, employing of women, distance from clinics, travel restrictions, lockdowns, fear of COVID-19, and political reasons (abortion prohibition). Complications of women using tele-abortion were pain, lack of psychological support, bleeding, and need to blood transfusions. The results of this study showed that using telemedicine and teleconsultations for medical abortion in the pandemic conditions may be extended after pandemic. Findings can be used by reproductive healthcare providers and policy makers to address the complications of abortion services.
Trail registration This study is registered in PROSPERO with number CRD42021279042
Plain English summary
COVID-19 pandemic shocks the international community, especially health policymakers around the world. The most important consequence of this outbreak has been direct and indirect impacts on health service provisions in all parts of the health system, including sexual and reproductive health services. We reviewed numerous studies investigating healthcare related to abortion in the pandemic era that showed women had more requests to access medical abortion, more than surgical. They preferred self-managed abortion process by telemedicine. Presenting telemedicine services without ultrasound has also been reported. Visits to clinics were reduced, and this decrease was reported based on the severity of the restrictions. Abortion clinics had reduced revenue, increased costs, and changed work style of their healthcare providers. Reasons for using telemedicine were fear of COVID-19, travel restrictions, lockdowns, more privacy, secrecy, and comfort. Telemedicine was reported safe, effective, acceptable, satisfying, and empowering for women. Maternal complications using tele-abortion were pain, bleeding, and need to blood transfusions. These findings can be used by policy makers and reproductive healthcare providers to address the complications of abortion management.
Similar content being viewed by others

Background
COVID-19 pandemic has put a lot of pressure on the health systems of countries around the world [1, 2]. The burden of infection and the high mortality and morbidity rates have led health systems to do their utmost to combat it. The national health services of the affected countries faced lack of funding, inadequate finance, deprivation of human and technical resources, and rigid and fragmented health policy-making [1, 3].
The coronavirus pandemic, directly and indirectly, has affected health service provisions in all parts of the health system, including reproductive health services such as maternity care, family planning, and sexual health [4, 5]. Coronavirus infection and its complications in mothers increased the need for special care in the obstetrics ward. Fear, stigma, misinformation, and socioeconomic factors including restrictions, lack of financial resources, reduced economic activity, and reduced government revenues indirectly affected the access to essential reproductive health services [4,5,6].
Reduction in access to and utilization of essential reproductive health services during the coronavirus pandemic increased the number of women who suffer from complications or die during pregnancy [7, 8]. An abortion, or termination of pregnancy, is a procedure to end a pregnancy. Abortion services include ending pregnancy either by taking medicines or having a surgical procedure. In addition, abortion services and stock-out of contraceptives to prevent unintended pregnancies are disrupted [7,8,9]. A 10% reduction in service coverage during reproductive age could result in the death of an additional 28,000 mothers, over 3.3 million unsafe abortions, and 15.4 million unintended pregnancies as family planning services face disruptions [8, 10]. Access to sexual health services and safe abortion reduced in many countries in COVID-19 pandemic lockdowns. This issue can increase the mortality of adolescent women and girls who are more vulnerable to unintended pregnancies than others [9].
Unsafe abortion is one of the most critical problems of reproductive health services, which is more common in middle and low-income countries. That is due to the lack of access to legal abortion services and financial resources [11, 12]. About 7 million women are admitted to hospitals in these countries every year due to the complications of unsafe abortion. Annually, about 4.7 to 13.2% of maternal deaths occur due to unsafe abortion, and the cost of management of the complications of unsafe abortion is estimated at US$ 553 million [12, 13].
Concerning the morbidities and high burden of unsafe abortions, in cases where safe abortion services are limited or are not available, people resort to using herbs or drugs or surgical procedures from unknown and often unsafe sources to terminate their pregnancies [14]. Some countries have recognized this risk during the COVID-19 pandemic and have allowed people with remote counseling or telemedicine to take some medications at home to avoid abortion with mentioned methods [14]. Therefore, some studies suggest that in these situations, health systems can use telemedicine, virtual and social networks to provide education and counselling on contraceptive methods or safe drugs for induced abortion to prevent the risk of unsafe abortion [15].
Global efforts were made in a crucial circumstance like this to quickly create safe and effective vaccinations. The first COVID-19 vaccination was ultimately authorized by the American Food and Drug Administration in August 2021 [16]. After immunization with this vaccine, fertility doesn’t appear to be impaired [16]. In these situations, it seems necessary to provide education and counselling about safe sexual health to prevent coronavirus infection, care before and after using contraceptive or abortion methods in the current pandemic. Despite numerous studies, some questions remain unanswered, including the impact of pandemic on the services for abortion and post-abortion and the strategies should the health systems adapt to manage abortions in the current pandemic. So far, no study has integrated all the strategies and practical approaches to administering this issue. Therefore, in this study, we intend to systematically review the studies investigating management of health services to abortions during the COVID-19 pandemic.
Methods
This study is a systematic review of abortion services during the COVID-19 pandemic. With the intention of reliability and authenticity of the results, this report adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. Also, this study is registered in PROSPERO with number CRD42021279042.
Data sources
We searched comprehensively the online databases of PubMed, Web of Science, and Scopus for relevant studies which were published in English from December 2019 to August 2021 (see Additional file 1).
Search strategy
The search strategy of the present study was organized in collaboration with two members of the research team. An electronic search was performed in each database based on the following keywords: abortion, miscarriage, feticide, SARS-CoV-2, Coronavirus, COVID-19. The complete search strategy is as follows:
Strategy search:
-
A.
COVID-19 OR SARS-CoV-2 OR Corona virus
-
B.
Abortion OR miscarriage OR abort OR feticide OR “pregnant termination”
-
C.
[A] AND [B]
Eligibility criteria
Retrieved studies should meet the following criteria to be included in this study.
-
The original studies investigated abortion services during the COVID-19 pandemic
-
The studies published from the beginning of the COVID-19 to August 2021
The articles which had at least one of the following criteria were excluded:
-
− Non-original articles, including reviews, case reports, clinical trial protocol, and editorials
-
− Articles without obtainable full texts, abstract papers, and conference abstracts
-
− Non-English language
Data retrieval
The EndNote software was used to organize articles of the systematic review. Search results from reviewed databases composed in a single EndNote library and duplicate records removed.
Data screening
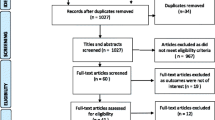
Two research team members independently screen titles and abstracts of retrieved studies to determine if they meet inclusion and exclusion criteria. The process of study selection is shown in Fig. 1.

Prisma flowchart
Data extraction
This study extracted variables included the first author, year, type of evidence/ study, country, participants (number), age, abortion services, satisfaction, factors related to abortion services, maternal outcome, and other findings. Three authors independently extracted outcome data using the standardized table. Two members of the research team designed these specifications on the table. In order to exclude any duplications, the selected articles were surveyed by other researchers once again.
Quality assessment
Two independent members of the research team assessed the quality of the cross-sectional and cohort studies by New Castle-Ottawa Scale (NOS), any disagreement was resolved by a third author, and the consensus was achieved.
Results
Selection and characteristics of included studies
The study selection process is shown in Fig. 1. One hundred fifty-one records were identified through the database and reference lists of articles. After removing duplicated records, 112 records remained; finally, 25 full-text articles were assessed for eligibility and seventeen articles have been included: Cross-sectional [17,18,19, 32, 33], prospective [20, 23, 34], retrospective [23, 24] cohort, qualitative [20, 25], mixed-method [21, 22], descriptive [26,27,28,29,30] studies and a newspaper [29]. Included studies have been conducted in USA, France, Belgium, UK, Scotland, Mexico, Columbia, Nepal, and eight European countries, as showed in Table 1.
COVID-19 and abortion
The results showed that during the COVID -19 pandemic, requests for access to medication abortion by telemedicine and demand for self-managed medication abortion had been increased [20,21,22,23,24, 26, 28, 29, 34,35,36]. In contrast, the number of abortion requests and procedures in the abortion centers were generally dropped [31]. It was more significant in the most severe and longest-lasting lockdowns [28]. In another report, the number of visits to abortion clinics has been reduced by 32%, with an additional 23% reduction in areas where abortion is prohibited [18]. Travel restrictions [32], lockdowns [22, 27, 28], and fear of COVID-19 [17] were among reasons to choose telemedicine abortion. Request for telemedicine abortion was reported based on location and distance from the hospital [32].
Satisfaction in telemedicine service
Numerous studies described tele-abortion safe, effective [20, 29, 32], very acceptable [20, 32, 34], and satisfying for women [23, 26, 29]. More individuals preferred medical abortion to surgical abortion [17]. In one study, the most frequent reasons to choose telemedicine abortion were privacy (38.3%), secrecy (46.2%), and comfort (34.9%) [22].
According to the results of a qualitative research, the quality of abortion care was improved in telemedicine services due to access, comfort, flexibility, and ongoing telephone support [20, 32]. It also reported that self-sourced medication abortion was safe, effective, and empowering for women [32, 33]. Another report showed no significant difference in satisfaction of services during and after lockdown (p = 0.690) [17].
Complications and challenges of tele-abortion
The most reported complications of mothers were bleeding [24, 34], pain [24, 34], and need to blood transfusions (0.4%) [26]. The COVID-19 pandemic had created many challenges in abortion clinics, including changes in the work style of healthcare providers, increased costs, and reduced revenue, but care activities continued [37, 38]. Using medication abortion and present telemedicine services without ultrasound has also been reported [20, 23, 33].
Discussion
Our results may indicate two different aspects. First, Increased rates of miscarriage throughout the pandemic may be due to the risk of COVID 19 during pregnancy, decreased access to prenatal care, or the financial downturn associated with the pandemic [39, 40]. Second, Decrease the rate of clinics appointments for abortion and increase the number of self-managed abortions, which can be due to fear of infection during the on-site visit or inability to go to the clinic due to disruption of the transportation system or childcare. We recognized higher stay-at-home behaviour levels with significant increases in requests in support of these probabilities. Studies have found that barriers to accessing the clinic, especially the cost of abortion, are reasons that individuals often cite. These barriers were reflected at the individual level at the state level, where the highest rates of applications were related to the residence in states with more restrictive abortion policies. There was also a correlation between the increase in the rate of requests in the counties, where the mean distance between nearest abortion clinics was longer, and the high proportion of the population living below the FPL [27], for example Texas, the state with the most prohibitive criteria, showed the greatest rise in requests, notwithstanding an almost low burden of COVID-19 [28]. International human rights law explicitly accredits the rights to sexual and reproductive health and autonomy of the body. These rights create a positive commitment by the government to provide information and services related to abortion and remove unnecessary medical barriers that eliminate practical access [41]. In times of crisis like pandemics, the international human rights commitments of states to respect, protect, and achieve the rights to health, life, and indiscrimination, among other rights, are not suspended. Steps to limit unsafe abortions and assure access to essential sexual and reproductive health services, such as abortion services, are key responsibilities of governments, even in emergencies. Achieving this main obligation demands the repeal of laws and procedures that criminalize, impede, or impair access to sexual and reproductive services, ensure public access to services, and limit unsafe abortions [42, 43]. Reaching these main obligations is vital and necessary in the time of COVID-19. Government responses that have promoted access to self-managed abortion are necessary steps to improve agreement with human rights obligations. Governments must fulfill similar proof-based and transformative solutions to guarantee abortion access for those who need a surgical abortion or those who do not have independence or basic support to offer self-managed abortion. States must more anticipate and deal with medical deficiencies due to interrupted supply chains. Other critical measures such as guaranteeing that telemedicine and other abortion services are possible to marginalized groups for free or at a low price. The results of a qualitative study showed that one of the common and positive experiences of maternal health care providers during the COVID-19 pandemic was the use of telemedicine capacity to care pregnant women that was beneficial in relieving their anxiety and breaking the chain of COVID-19 transmission [44]. However, telemedicine does not apply to all women and in all areas. Lack of adequate internet connection in some places prevents the widespread use of telemedicine [45].
Limitations
This study has several limitations. First, even more than a year after the beginning of the COVID-19 epidemic, many aspects of reproductive health and abortion services are still unknown due to the lack of related articles. Second, existing studies sometimes report disparate material that cannot be discussed in the desired detail (because both our knowledge of the epidemic and its effects is rapidly increasing, and the results of the studies presented from different communities based on social and indigenous situations. Last, the present study was supposed to be done as a meta-analysis, but due to factors such as: the scarcity and heterogeneity of existing articles, the unknown nature of the disease, and its effects on reproductive health (including abortion), it was practically not possible.
Suggestions
Based on the results and limitations of the study, in order to achieve more and better results, the following items are suggested:
-
1.
Conducting studies with a wider range and more diverse variables regarding reproductive health and pregnancy.
-
2.
Investigating and comparing the effects and complications of COVID-19 on reproductive health in different communities.
-
3.
Investigating the effect of vaccination on the consequences of pregnancy and abortion (when we did this study, vaccination of pregnant women had not been done and we could not investigate the consequences of vaccination on pregnancy and abortion).
Overall, this study presents new findings on the impact of COVID-19 on aspects of abortion that can be used by reproductive health care providers to manage the complications of abortion.
Conclusion
COVID-19 is a pandemic, which implies that global values need to be considered. It appears that countries with strict rules must revise their abortion laws throughout pandemics to decrease the unsafe abortions rate and their complications. The COVID-19 emergency is urging states to extend their healthcare systems and review their health laws. Women could suffer urgent harm if the restricted law is not repealed. Evidence suggests that COVID-19 may impair reproductive health, directly or indirectly. Given the effects of the COVID-19 epidemic on reproductive health, the results of this study provide detailed information on the various aspects of abortion and how to manage it in pandemic conditions. The findings of this study can be used by reproductive health care providers and policy makers to address the complications of abortion management.
Availability of data and materials
The authors expressed that all information provided in this article can be shared.
Abbreviations
- FPL:
-
Federal poverty level
References
World Health Organization. COVID-19 related mortality and morbidity among healthcare providers—based on information as at 14 February 2021. Brazzaville: Regional Office for Africa; 2021.
World Health Organization. WHO Coronavirus dashboard. 2021. https://covid19.who.int/. Accessed 13 Jan 2022.
Armocida B, et al. The Italian health system and the COVID-19 challenge. Lancet Public health. 2020;5(5):e253–e253.
Krubiner CB, Keller JM, Kaufman J. Balancing the COVID-19 response with wider health needs: key decision-making considerations for low-and middle-income countries. CGDev. 2020;8.
McDonnell S, et al. The impact of the Covid-19 pandemic on maternity services: a review of maternal and neonatal outcomes before, during and after the pandemic. Eur J Obstet Gynecol Reprod Biol. 2020;255:172–6.
Townsend R, et al. Global changes in maternity care provision during the COVID-19 pandemic: a systematic review and meta-analysis. E Clin Med. 2021;37:100947.
Roberton T, et al. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: a modelling study. Lancet Glob Health. 2020;8(7):e901–8.
Riley T, et al. Estimates of the potential impact of the COVID-19 pandemic on sexual and reproductive health in low- and middle-income countries. Int Perspect Sex Reprod Health. 2020;46:73–6.
Adelekan B, et al. Effect of COVID-19 pandemic on provision of sexual and reproductive health services in primary health facilities in Nigeria: a cross-sectional study. Reprod Health. 2021;18(1):166.
Krishna UR. Reproductive health during the COVID-19 pandemic. J Obstet Gynaecol India. 2021. https://doi.org/10.1007/s13224-021-01546-2.
Say L, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323–33.
Singh S, Maddow-Zimet I. Facility-based treatment for medical complications resulting from unsafe pregnancy termination in the developing world, 2012: a review of evidence from 26 countries. BJOG. 2016;123(9):1489–98.
Vlassoff M, Shearer J, Walker D, Lucas H, et al. Economic impact of unsafe abortion-related morbidity and mortality: evidence and estimation challenges. Brighton: Institute of Development Studies; 2008. p. 94.
Todd-Gher J, Shah PK. Abortion in the context of COVID-19: a human rights imperative. Sex Reprod Health Matters. 2020;28(1):1758394.
Wang Y, Yang Q. Post abortion care and management after induced abortion during the COVID-19 pandemic: a Chinese expert consensus. Adv Ther. 2021;38(2):1011–23.
Foschi N, et al. Urological safety and COVID-19 vaccinations. Vaccines. 2022;10(11):1887.
Aryal S, Nepal S, Ballav Pant S. Safe abortion services during the COVID -19 pandemic: a cross-sectional study from a tertiary center in Nepal. F1000Research. 2021;10:112.
Andersen M, Bryan S, Slusky D. COVID-19 surgical abortion restriction did not reduce visits to abortion clinics. SSRN J. 2020. https://doi.org/10.2139/ssrn.3726434.
Marquez-Padilla F, Saavedra B. The unintended effects of the COVID-19 pandemic and stay-at-home orders on abortions. J Popul Econ. 2022;35(1):269–305.
Boydell N, et al. Women’s experiences of a telemedicine abortion service (up to 12 weeks) implemented during the coronavirus (COVID-19) pandemic: a qualitative evaluation. BJOG. 2021. https://doi.org/10.1111/1471-0528.16813.
LaRoche KJ, et al. Attitudes of US adults toward using telemedicine to prescribe medication abortion during COVID-19: a mixed methods study. Contraception. 2021;104(1):104–10.
Atay H, et al. Why women choose at-home abortion via teleconsultation in France: drivers of telemedicine abortion during and beyond the COVID-19 pandemic. BMJ Sex Reprod Health. 2021. https://doi.org/10.1136/bmjsrh-2021-201176.
Kerestes C, et al. Provision of medication abortion in Hawai’i during COVID-19: practical experience with multiple care delivery models. Contraception. 2021;104(1):49–53.
Gibelin K, et al. COVID-19 impact in abortions’ practice, a regional French evaluation. J Gynecol Obstet Human Reprod. 2021;50(5):102038.
De Kort L, Wouters E, van de Velde S. Obstacles and opportunities: a qualitative study of the experiences of abortion centre staff with abortion care during the first COVID-19 lockdown in Flanders, Belgium. Sex Reprod Health Matters. 2021;29(1):180.
Chong ER, et al. Expansion of a direct-to-patient telemedicine abortion service in the United States and experience during the COVID-19 pandemic. Contraception. 2021;104(1):43–8.
Aiken AR, Starling JE, Gomperts R. Factors associated with use of an online telemedicine service to access self-managed medical abortion in the US. JAMA Netw Open. 2021;4(5):e2111852–e2111852.
Aiken AR, et al. Demand for self-managed online telemedicine abortion in the United States during the coronavirus disease 2019 (COVID-19) pandemic. Obstet Gynecol. 2020;136(4):835.
Romanis EC, Parsons JA. Legal and policy responses to the delivery of abortion care during COVID-19. Int J Gynecol Obstet. 2020;151(3):479–86.
Aiken AR, et al. Demand for self-managed online telemedicine abortion in eight European countries during the COVID-19 pandemic: a regression discontinuity analysis. BMJ Sex Reprod Health. 2021. https://doi.org/10.1136/bmjsrh-2020-200880.
De Kort L, et al. Abortion care in a pandemic: an analysis of the number and social profile of people requesting and receiving abortion care during the first COVID-19 lockdown (March 16 to June 14, 2020) in Flanders, Belgium. Arch Public Health. 2021;79(1):140.
Godfrey EM, et al. Family medicine provision of online medication abortion in three US states during COVID-19. Contraception. 2021;104(1):54–60.
Karlin J, et al. Greasing the wheels: the impact of COVID-19 on US physician attitudes and practices regarding medication abortion. Contraception. 2021;104(3):289–95.
Reynolds-Wright JJ, et al. Telemedicine medical abortion at home under 12 weeks’ gestation: a prospective observational cohort study during the COVID-19 pandemic. BMJ Sex Reprod Health. 2021. https://doi.org/10.1136/bmjsrh-2020-200976.
Kaller S, et al. Abortion service availability during the COVID-19 pandemic: results from a national census of abortion facilities in the U.S. Contraception X. 2021;3:100067.
Porter Erlank C, Lord J, Church K. Acceptability of no-test medical abortion provided via telemedicine during Covid-19: analysis of patient-reported outcomes. BMJ Sex Reprod Health. 2021. https://doi.org/10.1136/bmjsrh-2020-200954.
Roberts SCM, Schroeder R, Joffe C. COVID-19 and independent abortion providers: findings from a rapid-response survey. Perspect Sex Reprod Health. 2020;52(4):217–25.
Roberts SCM, et al. Disruptions to abortion care in Louisiana during early months of the COVID-19 pandemic. Am J Public Health. 2021. https://doi.org/10.2105/AJPH.2021.306284.
Bayefsky MJ, Bartz D, Watson KL. Abortion during the Covid-19 pandemic—ensuring access to an essential health service. N Engl J Med. 2020;382(19): e47.
Turret E et al. COVID-19 does not change the right to abortion. Health Aff. 2020; 17.
Center for reproductive rights. Breaking ground 2018: treaty monitoring bodies on reproductive rights. New York: Center for Reproductive Rights; 2018.
CESCR U. General Comment No. 22, para. 49 (a)(c)(e). UN Doc. E/C.12/GC/22. 2016. https://www.escr-net.org/resources/general-comment-no-22-2016-right-sexual-and-reproductive-health.
CESCR, U. General comment No. 14, para. 44. UN Doc. E/C.12/2000/4. 2000. https://www.escr-net.org/resources/general-comment-14.
Hantoushzadeh S, et al. Experiences of health care providers on pregnancy and childbirth care during the COVID-19 pandemic in Iran: a phenomenological study. BMC Pregnancy Childbirth. 2021;21(1):1–9.
Semaan A, et al. Voices from the frontline: findings from a thematic analysis of a rapid online global survey of maternal and newborn health professionals facing the COVID-19 pandemic. BMJ Glob Health. 2020;5(6): e002967.
Funding
This study received a grant from Kermanshah University of Medical Sciences with this ID: IR.KUMS.REC.1401.587.
Author information
Authors and Affiliations
Contributions
KQ, and ASH designed the study. KQ conducted the interviews. Data extraction conducted by MH, MD, and MI. RKH, ZK interpreted the data. MK, MF, EM, MM, and BMB drafted the article and the final approval of the version to be submitted was done by all authors. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This article is based on published data, and hence ethical approval is not required.
Consent for publication
Not applicable.
Competing interests
The all authors declare that there is no conflict of interest regarding the publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search details.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Qaderi, K., Khodavirdilou, R., Kalhor, M. et al. Abortion services during the COVID-19 pandemic: a systematic review. Reprod Health 20, 61 (2023). https://doi.org/10.1186/s12978-023-01582-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12978-023-01582-3