
Abstract
Background
Sexual and reproductive health (SRH) is referring to physical and emotional wellbeing and includes the ability to be free from unwanted pregnancy, unsafe abortion, sexually transmitted infections including HIV/AIDS, and all forms of sexual violence and coercion. SRH is the main services packages that prevent and reduce adolescent reproductive health risks and problems. While the government of Ethiopia has undertaken several measures to improve SRH services, there was limited data on utilization among adolescents and associated factors.
Objective
To assess utilization of SRH services and associated factors among adolescents attending secondary schools in Haramaya District, Eastern Ethiopia.
Methods
A school-based cross-sectional study was conducted among adolescent students aged 15–19 years. A total of 692 adolescents were selected using a multi-stage sampling from two randomly selected secondary schools, each from rural and urban settings, in Haramaya district where 642 provided complete data and included in the analysis. A structured, pretested, and self-administered questionnaire was used to collect data. Data entry was conducted using Epi Data version 3.1 and exported to STATA version 16 for analysis. Bivariable and multivariable binary logistic regression were used to identify factors associated with school adolescents’ utilization of SRH. Statistically significant associations are declared at P-value < 0.05.
Result
A total of 642 completed the survey questionnaire, constituting a response rate of 92.7% (642/692). Male adolescents accounted 63.7% and the mean age of respondents was 17.71 years. Among those who completed the survey, 23.5% (95% CI: 20–26.8) utilized SRH services. Adolescents who were exposed to SRH information (adjusted odds ratio (AOR) = 2.11, 95% CI: 1.22–3.6), aware of SRH service providing facility (AOR = 1.83, 95% CI: 1.12–3.0) and SRH service components (AOR = 2.76, 95%, CI: 1.53–4.97), and distance from SRH facilities (AOR = 2.28, 95%, CI: 1.13–4.62) were significantly associated with the utilization of SRH services.
Conclusion
Nearly one-in-four secondary school adolescents (23.5%) utilized SRH services. Targeted promotion of SRH providing facilities and SRH service components aimed at awareness creation could improve adolescents’ utilization of SRH services. Improved SRH services utilization among adolescents who were far from SRH services providing facilities needs further investigation.
Plain language summary
Sexual and reproductive health (SRH) refers to physical and emotional wellbeing and includes the ability to be free from unwanted pregnancy, unsafe abortion, sexually transmitted infections including HIV/AIDS, and all forms of sexual violence and coercion. Components of the SRH services are important to reduce adolescent reproductive health risks and problems. This paper reports on the frequency of in-school adolescents who utilized SRH services and the factors that determined it.
AbstractSection Methodswe collected data from 642 in-school secondary school adolescents, aged 15–19 years, in Haramaya district, East Ethiopia. The data were collected from two schools, one from rural and the other from urban areas, using lottery method from the available schools in the district. A face-to-face interview was conducted to obtain data from the adolescents in the selected secondary schools.
AbstractSection ResultOut of 642 in-school adolescents, 23.5% utilized SRH services in Haramaya District. Adolescents who previously received SRH information, who knew SRH services providing facility, aware of SRH service components, and those who live not close to the SRH facilities were utilized the SRH services more often compared to their friends.
AbstractSection ConclusionNearly one-in-four secondary school adolescents (23.5%) utilized SRH services. Targeted promotion of SRH providing facilities and SRH service components aimed at awareness creation could improve adolescents’ utilization of SRH services.
Similar content being viewed by others


Introduction
Sexual and reproductive health (SRH) refers to physical and emotional wellbeing and includes the ability free from unwanted pregnancy, unsafe abortion, STIs including HIV, and all forms of sexual violence and coercion. The majority of people become sexually active during the adolescence period putting people in this age group at higher risks of SRH problems [1]. The World Health Organization (WHO) defines an adolescent as an individual aged from 10 to 19 years [2]. Adolescence is a transitional phase of growth and development during which of the most rapid and complex life stages characterized by a significant physical, cognitive, behavioural, social, and psychological change occurs [3]. This development was characterized by suboptimal decisions and actions that put them to unintentional injury and risk-taking [4].
Globally about 1.2 billion of the total population are adolescents and more than half of this population lives in developing countries [5]. Sub-Saharan Africa (SSA) is the region where 23% of its total population (1.06 billion) were adolescents [6]. In Ethiopia, one of a country in the SSA with a rapidly growing population of adolescents and youths, adolescents account for 33.8% of the estimated total population of 90 million [7].
Pregnancy, abortion, and STIs (including HIV) are the major SRH risks that result in adverse reproductive health outcomes in adolescents than adults. According to the 2018 Inter-Agency Working Group on Reproductive Health (IAWG) report, AIDS-related death among adolescents are nearly tripled from 21,000 in 2000 to 60,000 in 2014, one-in-four women give birth during adolescence or before they reach their 18th birthday, and 3.9 million females aged 15–19 years undergo unsafe abortion every year [5]. A national-level report of the Ethiopia Demographic Health Survey in 2016 indicated that the adolescent fertility rate was 80 births per 1000 [7]. Female adolescents aged 15–19 years were seven times more likely to be HIV positive than male adolescents [8]. Research evidence reveal that early pregnancy, abortion, and STIs (including HIV infection) rates are high among adolescents, and hence adolescent and youth reproductive health is a public health concern [9].
Sexual and reproductive health services include access to information and services on prevention, diagnosis, counselling, treatment, and care, and require that all people can safely reach services without traveling for a long time or distance [10].
A study conducted in higher education institutions in Ethiopia revealed that one-third of university students have already been sexually experienced. Of these, nearly two-thirds were found to have sexual experience already before joining higher education institutions evidencing that SRH problems manifest early on and calls for interventions at early adolescence [11]. A range of social norms and practices that prevent sexually active adolescents from accessing contraceptives, maternity care, and other services due to their age and gender is challenging for effective service delivery [9, 12]. A qualitative study by Munea et al. in Northwest Ethiopia reported that the community was intolerant to adolescent premarital sex and did not approve neither SRH use nor SRH communication with unmarried adolescents[13]. Consequently, the main barriers preventing adolescents to access SRH services was related to cognitive accessibility (a lack of sexual knowledge and a lack of awareness of services) and psychosocial accessibility (feelings of shyness and shame, fear of parents finding out service use, and lack of confidentiality) as noted by Thongmixay et al. [14]. Low service uptake due to these challenges were affecting adolescent health and it compromise the educational attainment of adolescents, increases dependency, and reduce the economic potential of the country [15].
The International Conference on Population and Development (ICPD) in 1994 held in Cairo established a comprehensive SRH service that needs to address and solve the SRH problem for adolescents and youth [16]. National strategy for adolescent and young sexual and reproductive (AYSR) health aims to increase access to information, education and to promote health service uptakes by adolescents and youth [8].
Despite that utilization of ASRH are not well explored in Ethiopia, previous studies focused on youth and adult people. A few studies that assessed ASRH services, in turn, are limited to selected service components[17]. Therefore, this study aimed to assess the utilization of SRH services among secondary school adolescent students in Haramaya District, Eastern Ethiopia.
Materials and methods
Study design and settings
We conducted a school-based cross-sectional study in Haramaya District which is located at 500 km away from Addis Ababa, the capital of Ethiopia. When this study was conducted, the district has a total population of 313,152 (50.9% were males). Only 16.9% of the total population were urban residents with the significant majority residing in the rural parts of the district. There are eight health centers and one general hospital in the study area. The district has 6 secondary schools (3 in urban and 3 in rural areas) and enrolled a total of 6972 students in the 2019/2020 academic year (where 73.0% were males).
This study was conducted from March 1 to 15, 2020 in secondary schools at Haramaya District, East Hararge Zone, Oromia Regional State, Ethiopia.
Sample size and sampling procedure
The sample size was calculated using a single proportion formula with the assumption of 95% confidence interval, 21.2% proportion of SRH service utilization [18] from the study conducted in Nekemte town, Western Ethiopia, 4% margin of error, 1.5 of design effect, and 15% of non-response rate was added the sample size resulting in a minimum sample size of 692. The final sample size considered for analysis was 642 due to consideration of completeness of data.
A multi-stage sampling method was applied to select representative sample of adolescent students. In the first stage, secondary schools in the Haramaya district were clustered into two groups (urban and rural), then from each cluster one school was selected by a simple random sampling method, making a total of two schools. Secondly, school adolescents were stratified by their grade level of attendance. Sample size was then allocated proportionally after obtaining list of students from the respective school administration. Finally, the study participants were selected from each grade by using simple random sampling from the sampling frame of student roster.
Outcome variable
The dependent variable of interest in this study was adolescent SRH service utilization. The definition of the utilization of the SRH services was ever utilization of any one of the following SRH services:
-
SRH information Education and counselling
-
Contraceptive service
-
Pregnancy test & care
-
Voluntary counselling and testing (VCT)
-
Sexually transmitted infections (STI) screening, diagnosis, and management services
-
Safe abortion care
The outcome variable was measured based on self-report using a “yes or no” response to a single question on whether participants have ever utilized any one or many of the specific SRH service components in private and government health facilities.
Data collection tool and procedure
Data were collected using a pre-tested, self-administered questionnaire adapted from the John Cleland’s illustrative questioner for interviewing young people and reviewing works of literature. The tool consisted of three sections: socio-demographic, individual, and health facility characteristics. The original questionnaire was developed in English and then translated into the local Afan-Oromo language. The translated version was then translated back to the original English version for consistency. Six data collectors who were diploma graduates and two supervisors (BSc degree) conducted the data collection following orientation on study objectives, benefits of the study, research ethics and informed consent, and data collection techniques. Before the actual data collection, a pre-test was conducted to identify problems with the assessment tool in a small sample of students, 35(5%), outside the selected study setting. During the data collection, the principal investigator and the supervisors made daily checks to assess completeness of each returned questionnaire and questionnaires with several missing values for important variables have been discarded.
Operational definition
SRH service utilization
Refers to ever utilization of one or more of SRH service components in private and government health facilities [18]. Positive response to SRH service utilization was further validated by at least one type of services mentioned by respondents and those who received one or more service components were considered to have utilized SRH services. SRH information, education and counselling, contraceptive, pregnancy test & care, VCT, and HIV test, STI diagnosis and management, and Safe abortion care were the service components assessed in this study.
Accessibility of RHS facility (geographical accessibility)
In this study, accessibility was measured based on adolescent’s self-report of distance they had to travel to health facilities providing SRH services.
Data processing and analysis
Data were entered into Epidat version 3.1 and then exported to STATA version 14 for statistical analysis. Descriptive results were presented in tables, figures, and using numerical summary measures for continuous variable. To explore relationship between variables, cross-tabulation was conducted for variables of interest against the outcome variable. SRH services utilization was measured using a dichotomous response (Yes = 1 and No = 0). The positive response was further validated with questions on the type of SRH services utilized. The proportion of SRH service utilization was computed with specific service components. Family wealth index was computed using principal component analysis (PCA) by considering locally available household assets and categorized in to five (very poor, poor, medium, rich and very rich). Bivariable binary logistic analysis was conducted to select candidate variables for the multivariable binary logistic regression. Variables with P-value less than 0.25 in bivariable binary logistic regression model proceeded into the multivariable binary logistic regression model. Moreover, model fitness was checked by the Hosmer–lemeshow test and multi-collinearity of variables in the final model was also checked using the variance inflation factor (VIF). Variables in the final model with P-value < 0.05 were considered as statistically significant predictor of SRH service utilization. Effect estimates were reported using odd ratio with a corresponding 95% confidence interval.
Result
Socio-demographic characteristics of participants
A total of 642 adolescent students have participated in the study which makes a response rate of 92.7%. From the total respondents, 63.7% respondents were male students with the mean age of 17.71 years SD (± 1.19) and more than half, 57.6%, were grade 9 and 10. From the total participants 75.1% were single and 86.1% were Muslims. Regarding the living arrangement of students, most of them, 81.5%, were living with their families (Table 1).
Secondary school adolescents’ characteristics
Of the total adolescents participated in the study 39% ever had a boy or girlfriend and 20% of were sexually active. 68.5% of participating adolescents reported that had been exposed to SRH information with 52% mentioned peers as the main source of information. Regarding discussion of SRH issues 62.2% respondents ever discussed at least two SRH issues: 42.6% discussed with peers followed by 19.8% discussed with healthcare providers (Table 2).
From all respondents, more than half of 56.1% knew health facilities that provide SRH services and 66.7% knew SRH service types. Out of these respondents, 90.9% knew VCT services, 73.1% knew contraceptive services and 29.0% knew safe abortion services (Table 3).
Utilization of SRH services
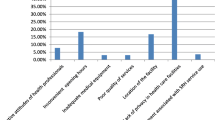
Overall, 23.5% (95% CI: 20, 26.8) of in-school adolescents utilized SRH services (64.2% male and 35.8% female students) in Haramaya district. The most frequently used SRH services components were counseling, information, and education, followed by VCT & HIV testing (Fig. 1). Of 132 sexually experienced adolescents, 42.4% used SRH services, of which 46.2% were married. Among adolescents who utilized SRH services, 41% did not want to return to the health facility. The main reasons for not wanting to return to health facilities were: not having enough privacy 28(45%), too embracing 13(21%), and no healthcare provider of same sex (14.5%) (Fig. 2).

Utilization of SRH service components among in-school adolescents in 2020, Haramaya District, Ethiopia

Main reasons for in-school adolescents not returning to Sexual and Reproductive Health facility in 2020, Haramaya District, Ethiopia
Factors associated with utilization of SRH
A binary logistic regression model was used to identify factors associated with utilization of SRH services. Based on the estimates from the bivariable binary logistic regression model, the factors significantly associated with utilization of SRH were age, marital status, living arrangement, having own income, ever had sexual intercourse, ever exposed to SRH information, discussion of SRH issues, perceived SRH risks, know of RH facility, aware of RH services, and being far at distant from the facility. All variables that showed association in the bivariable model are entered into the multivariable binary logistic regression model. Controlling for the effect of other variables in the model, adolescents with the following characteristics were over two-fold more likely to use SRH services: exposure for information (AOR = 2.11, 95% CI: 1.22–3.66), awareness of SRH services(AOR = 2.76 95%, CI: 1.53–4.97), identifying SRH facility whereabouts (AOR = 1.83 95% CI: 1.12–3.0), and far from SRH clinics (AOR = 2.28 95%, CI: (1.13–4.62) showed statistically significant association at p-value < 0.05 (Table 4).
Discussion
This cross sectional study assessed level of in-school adolescents’ SRH services utilization in Harmaya district, east Ethiopia, and identified factors associated with service utilization. The level of SRH services utilization was estimated at 23.5% (95% CI: 20.4, 27.0). Factors significantly associated with the in-school adolescents’ utilization of SRH services include exposure to SRH information, awareness of SRH services providing facility and service components, and distance from service providing facilities.
The level of SRH services utilization among in-school adolescents in the study setting was 23.5%. This finding was consistent with similar studies among in-school adolescents in Ethiopia and elsewhere where SRH services utilization reports ranged from 21.2 to 24.6% [18,19,20,21]. However, compared to other similar studies in Ethiopia, magnitude of the SRH services utilization observed in the study setting was low. For example, a study in southern Ethiopia reported an SRH services utilization of 33.8% among high school adolescents in youth friendly service implemented areas [22]. Similarly, a study in Debre Tabor town among high-school- and preparatory-students reported an SRH service utilization of 28.8% [23]. The SRH services utilization in the study setting, however, was high compared to adolescents in the general population (8.6%) [24] and those who reside in areas where youth friendly services are not implemented (9.9%) [22]. Part of the variation could be explained by differences in terms of factors related to service delivery like friendliness, negative attitude from service providers and feasibility of service hours; factors related adolescents’ perception (fear of being seen while using SRH services); and socio-cultural barriers [21, 25].
The most utilized SRH services components include information, education, and counseling (80.1%) where previous studies also reported a similar services utilization pattern that was largely limited to information seeking and counseling services [26]. The percentage of utilization of other services including contraception (28.5%), STI treatment (13.9%), pregnancy testing (13.2%), and safe abortion care (7%) were also comparable with previous studies [26]. However, this study did not assess adolescent’s unmet need of important services which might have shed light on the potential gaps to be addressed pointing to the services that adolescents seek but did not use.
Adolescents who previously had exposure to SRH information were significantly associated with current service utilization. Previous studies also reported consistent reports that adolescents who had multiple sources of SRH information including discussion with family members, friends, healthcare providers, and schools were more likely to use SRH services [22, 27, 28] as these may improve adolescents’ awareness on SRH related issues.
Adolescents who were aware of the specific SRH service components were more likely to utilize the services than those who did not know. Due to the nature of the study, however, it was not possible to state whether awareness of the specific SRH services components had led to service utilization or the reported awareness was secondary to the service utilization itself. Previous similar studies elsewhere emphasized the importance of adolescents’ awareness of SRH services providing facilities, particularly for rural adolescents [29]. It was further emphasized that lack of awareness of SRH service components and knowledge about youth friendly services among adolescents and where to go to use those services were the main reason for the low uptake of adolescent SRH services [29, 30].
Interestingly, in this study, adolescents who were far from health facilities that provide SRH services were two times more likely to utilize SRH services than those who lived close to SRH services providing facilities. This finding was against the reports in previous studies that indicated availability of service providing facilities in close by facilitated SRH services utilization [17, 19]. A systematic review by Nisiima et al. reported that facilitators of utilization of SRH services were mostly structural in nature including the quality of health services and clinics for adolescents to fit their needs and preferences [30]. Due to reasons related to confidentiality, availability of needed service, attitude of service providers, and shyness [17, 21], adolescents may prefer to use services from facilities where they could not be easily identified and find services of their preference. Poor understanding of the adolescents’ reproductive health needs in the community due to socio-cultural norms (not approving sexuality discussion during adolescents and hence utilization of services) and fear of adolescents to be seen by community members are big challenges impeding SRH use that need critical attention. In this study, for 58.9% of adolescents, their parents lived in rural areas and 18.5% of the adolescents lived alone in order to attend their high school study in the town of the Haramaya district. Consequently, the perceived freedom of living alone and confidentiality may have contributed to the observed association of distance and SRH services utilization.
Our study was not without limitation. Pertaining to sensitive nature of the topic studied, respondents may not give honest responses as required. This might underestimate the prevalence of SRH service utilization. We have tried to reduce issues related to confidentiality by making the data collection anonymous and using a self-administered structured questionnaire in the local language for data collection obtain information. This study cannot indicate the direction of the causal relationship.
Conclusion
The level of in-school adolescents SRH services utilization was not satisfactory to prevent potentially amenable problems related to and associated impacts of sexual activity and pregnancy related outcomes of adolescents. Targeted promotion of SRH providing facilities and SRH service components aimed at awareness creation could improve adolescents’ utilization of SRH services. Improved SRH services utilization among adolescents who were far from SRH services providing facilities needs further investigation.
Availability of data and materials
All data pertaining to the findings are presented in this paper. However, the data can be obtained from the corresponding author any time on reasonable request.
Abbreviations
- AIDS:
-
Acquired Immune Deficiency Syndromes
- ASRH:
-
Adolescent sexual and reproductive health
- AOR:
-
Adjusted odd ratio
- CSA:
-
Central statistic authority
- EDHS:
-
Ethiopian Demographic and Health Survey
- FMOH:
-
Federal Ministry of Health
- FP:
-
Family planning
- HIV:
-
Human immune virus
- HTTP:
-
Harmful traditional practice
- IAWG:
-
Inter-agency working groups
- SRH:
-
Sexual and reproductive health
- SSA:
-
Sub-Saharan Africa
- STI:
-
Sexual transmitted infection
- UNFPA:
-
United Nation Fund for Population Activities
- UNICEF:
-
United Nation International Children Emergency Fund
- VCT:
-
Voluntary counselling and testing
References
Wakasa BF, Oljira L, Demena M, Regassa LD, Daga WB. Risky sexual behavior and associated factors among sexually experienced secondary school students in Guduru, Ethiopia. Prev Med Rep. 2021;16(23):101398 https://doi.org/10.1016/j.pmedr.2021.101398.
African Health Organization. Adolescents Health Risks and Solutions. Available from: https://aho.org/fact-sheets/adolescents-health-risks-and-solutions. Accessed 23 Nov 2021.
Sivagurunathan C, Umadevi R, Rama R, Gopalakrishnan S. Adolescent health: present status and its related programmes in India. Are we in the right direction? JCDR. 2015;9(3):LE01-6. https://doi.org/10.7860/JCDR/2015/11199.5649.
Casey BJ, Getz S, Galvan A. The adolescent brain. Dev Rev. 2008;28(1):62–77.
UNICEF. Unicef Data: Monitoring the Situation of Children and Women. Available from: https://data.unicef.org/resources/adolescent-health-dashboard-regional-profiles/. Accessed 12 Dec 2021.
The World Bank Group. Data: Population, total-Sub-Saharan Africa. Available from: https://data.worldbank.org/indicator/SP.POP.TOTL?locations=ZG. Accessed 20 Mar 2022.
Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF, 2016. Available from: https://dhsprogram.com/pubs/pdf/FR328/FR328.pdf. Accessed 15 April 2021.
Federal Democratic Republic of Ethiopia Ministry of Health. National Reproductive Health Strategy: 2016-2020. Addis Ababa, October 2016. Available from: https://www.prb.org/wp-content/uploads/2020/06/Ethiopia-National-Reproductive-Health-Strategy-2016-2020.pdf. Accessed 13 Dec 2021.
Abebe M, Awoke W. Utilization of youth reproductive health services and associated factors among high school students in Bahir Dar, Amhara regional state, Ethiopia. Open J Epidemiol. 2014;4(02):69.
Denno DM, Hoopes AJ, Chandra-Mouli V. Effective strategies to provide adolescent sexual and reproductive health services and to increase demand and community support. J Adolesc Health. 2015;56(1):S22–41.
Mengistu TS, Melku AT. Sexual and reproductive health problems and service needs of university students in south east Ethiopia: Exploratory qualitative study. J Publ Health. 2013;1(4):184–8.
Coast E, Jones N, Francoise UM, Yadeta W, Isimbi R, Gezahegne K, et al. Adolescent sexual and reproductive health in Ethiopia and Rwanda: a qualitative exploration of the role of social norms. SAGE Open. 2019. https://doi.org/10.1177/2158244019833587.
Munea AM, Alene GD, Debelew GT, Sibhat KA. Socio-cultural context of adolescent sexuality and youth friendly service intervention in West Gojjam Zone, Northwest Ethiopia: a qualitative study. BMC Public Health. 2022;22(1):281. https://doi.org/10.1186/s12889-022-12699-8.
Thongmixay S, Essink DR, Greeuw T, Vongxay V, Sychareun V, Broerse JEW. Perceived barriers in accessing sexual and reproductive health services for youth in Lao People’s Democratic Republic. PLoS ONE. 2019;14(10):e0218296. https://doi.org/10.1371/journal.pone.0218296.
Morris JL, Rushwan H. Adolescent sexual and reproductive health: the global challenges. Int J Gynecol Obstet. 2015;131:S40–2.
UNECA/UNFPA/AUC. International Conference on Population and Development (ICPD/15): African Regional Review Report. Addis Ababa, October 2009. Available from: https://www.unfpa.org/sites/default/files/event-pdf/ICPD%2015%20Report.pdf. Accessed 15 Apr 2021.
Ansha MG, Bosho CJ, Jaleta FT. Reproductive Health services utilization and associated factors among adolescents in Anchar District, East Ethiopia. J Family Reprod Health. 2017;11(2):110.
Binu W, Marama T, Gebaba M, Sinaga M. Sexual and reproductive health services utilization and associated factors among secondary school students in Nekemte town, Ethiopia. Reprod Health. 2018;15(1):64. https://doi.org/10.1186/s12978-018-0501-z.
Abate AT, Ayisa AA, W/Mariam TG. Reproductive health services utilization and its associated factors among secondary school youths in Woreta town, South Gondar, North West Ethiopia: a cross sectional study. BMC Res Notes. 2019;12:90. https://doi.org/10.1186/s13104-019-4129-z.
Bilal SM, Spigt M, Dinant GJ, Blanco R. Utilization of sexual and reproductive health services in Ethiopia-Does it affect sexual activity among high school students? Sex Reprod Healthc. 2015;6(1):14–8. https://doi.org/10.1016/j.srhc.2014.09.009.
Napit K, Shrestha KB, Magar SA, Paudel R, Thapa B, Dhakal BR, et al. Factors associated with utilization of adolescent-friendly services in Bhaktapur district, Nepal. J Health Popul Nutr. 2020;39(1):2. https://doi.org/10.1186/s41043-020-0212-2.
Haile B, Shegaze M, Feleke T, Glagn M, Andarge E. Disparities in utilization of sexual and reproductive health services among high school adolescents from youth friendly service implemented and non-implemented areas of Southern Ethiopia. Arch Public Health. 2020;78(1):126. https://doi.org/10.1186/s13690-020-00508-w.
Simegn A, Azale T, Addis A, Dile M, Ayalew Y, Minuye B. Youth friendly sexual and reproductive health service utilization among high and preparatory school students in Debre Tabor town, Northwest Ethiopia: a cross sectional study. PLoS ONE. 2020;15(9):e0240033. https://doi.org/10.1371/journal.pone.0240033.
Tilahun T, Bekuma TT, Getachew M, Seme A. Assessment of access and utilization of adolescent and youth sexual and reproductive health services in western Ethiopia. Reprod Health. 2021;18(1):85. https://doi.org/10.1186/s12978-021-01136-5.
Abraham G, Yitbarek K, Morankar SN. Determinants of adolescents reproductive health service utilization in Ethiopia: a systematic review of quantitative evidence. Adolesc Health Med Ther. 2019;10:10.
Ayehu A, Kassaw T, Hailu G. Level of young people sexual and reproductive health service utilization and its associated factors among young people in Awabel District, Northwest Ethiopia. PLoS ONE. 2016;11(3):e0151613.
Motuma A, Syre T, Egata G, Kenay A. Utilization of youth friendly services and associated factors among youth in Harar town, east Ethiopia: a mixed method study. BMC Health Serv Res. 2016;16(1):272. https://doi.org/10.1186/s12913-016-1513-4.
Feleke SA, Koye DN, Demssie AF, Mengesha ZB. Reproductive health service utilization and associated factors among adolescents (15–19 years old) in Gondar town, Northwest Ethiopia. BMC Health Serv Res. 2013;13(1):294. https://doi.org/10.1186/1472-6963-13-294.
Ilori OR, Awodutire PO, Ilori OS. Awareness and utilization of adolescent reproductive health services among in-school adolescents in urban and rural communities in Oyo state. Niger Med J. 2020;61(2):67–72.
Ninsiima LR, Chiumia IK, Ndejjo R. Factors influencing access to and utilisation of youth-friendly sexual and reproductive health services in sub-Saharan Africa: a systematic review. Reprod Health. 2021;18(1):135.
Acknowledgements
We would like to thank Haramaya University, College of Health and Medical Science, School of Graduate Studies for giving this chance to conduct this study and Zonal and Haramaya education office and school heads for their support and respective contribution. We are also grateful to our study participants and data collectors for their cooperation.
Funding
The first author (CA) received fund for data collection from Haramaya University.
Author information
Authors and Affiliations
Contributions
CA: conceived the study, carried out the overall design and execution, performed data collection, statistical analysis, and drafted the manuscript. LO: conceived the study, critically contributed on the design and execution of the study, and data collection techniques and statistical analysis. SH: contributed in the statistical analysis and drafting the manuscript. MM: conceived the study, critically contributed on the design and execution of the study, data collection techniques, statistical analysis, drafting the original draft and interpretation of the results. All authors read and approved the final manuscript..
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was also conducted following the declaration of Helsinki where ethical approval was obtained from the Haramaya University College of Health and Medical Sciences Institutional Health Research Ethics Review Committee (IHRERC) and data were collected anonymously without personal identifiers. Data were collected following after obtaining an informed voluntary written and signed consent from each participants aged 18 years and above. For minors (< 18 years of age) selected in this study, consent was first obtained from their parents or guardians by sending them a sealed consent form through their selected child.
Consent for publication
Study participants/guardians agreed publication of aggregate data.
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Abdurahman, C., Oljira, L., Hailu, S. et al. Sexual and reproductive health services utilization and associated factors among adolescents attending secondary schools. Reprod Health 19, 161 (2022). https://doi.org/10.1186/s12978-022-01468-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12978-022-01468-w