
Abstract
Background
Literature shows that women’s sexual autonomy, which refers to women’s capacity to refuse sex and ask a partner to use condom, has significant implications on the sexual and reproductive health outcomes and sexual-and-gender based violence. Nevertheless, there is scarcity of empirical evidence to support the association between women’s sexual autonomy and intimate partner violence (IPV) in sub-Saharan Africa.
Methods
Data for the study were extracted from the recent Demographic and Health Surveys in 24 countries in sub-Saharan Africa between 2010 and 2019. Bivariable and multivariable binary logistic regression analyses were performed to examine the association between sexual autonomy and IPV in all the studied countries. Statistical significance was set at p < 0.05.
Results
The pooled prevalence of IPV and sexual autonomy in the 24 countries were 38.5% and 73.0% respectively. Overall, the odds of exposure to IPV were higher among women with sexual autonomy, compared to those without sexual autonomy even after controlling for covariates (age, level of education, marital status, current working status, place of residence, wealth quintile and media exposure). At the country-level, women from Angola, Cameroon, Chad, Gabon, Cote d’lvoire, Gambia, Mali, Nigeria, Kenya, Comoros, Zambia, and South Africa who had sexual autonomy were more likely to experience IPV whilst those in Burundi were less likely to experience IPV. The study showed that sexual autonomy increases women’s exposure to IPV and this occurred in many countries except Burundi where women with sexual autonomy were less likely to experience IPV.
Conclusion
The findings highlight the need for serious programs and policies to fight against IPV in the sub-region. Additionally, laws need to be passed and implemented, with law enforcement agencies provided with the necessary resources to reduce intimate partner violence among women with sexual autonomy.
Plain language summary
Globally, intimate partner violence is regarded as a public health concern due to its devastating effects on the physical, emotional, and reproductive health of women. This study sought to determine how women’s capacity to refuse sex, negotiate for safe sex practices such as insisting on partner to use condom, and feeling justified in asking a partner to use condom is associated with the potential of experiencing violence from an intimate partner. Using data from the demographic and health survey conducted between 2010 and 2019, we found that women who had more capacity to refuse sex, negotiate for safe sex practices such as insisting on partner to use condom, and feeling justified in asking a partner to use condom were more likely to experience violence from their intimate partners after controlling for other factors such as the age of the woman, level of education, marital status, place of residence, economic status, and media exposure. The results highlight the need for sub-Saharan African countries to step up programs that ease up intimate partner violence reporting and access to legal support for those who experience it. Additionally, laws need to be passed and implemented, with law enforcement agencies provided with the necessary resources to reduce intimate partner violence among women with sexual autonomy.
Similar content being viewed by others

Introduction
Intimate partner violence (IPV) is a public health concern and increasingly gaining global attention [1]. Any violence (physical, psychological, and sexual harm) that occurs in an intimate relationship can be considered or referred to as IPV [2,3,4]. However, in this study, IPV is conceptualized as physical violence (i.e., throwing something at a woman, slapping, punching, threatening with a weapon, kicking or dragging, strangling and pulling of hair), emotional violence (i.e., insults, humiliation and threats to harm) and sexual violence (physically forced into unwanted sex, being forced into other unwanted sexual acts, and physically forced to perform sexual acts that one doesn’t want to). The pervasiveness of IPV worldwide cannot be downplayed as one out of every three females would have ever experienced some form of IPV at some point in their lives [2]. The phenomenon is endemic in sub-Saharan Africa (SSA), with most women being at risk of experiencing IPV [5].
There is the need for more pragmatic and evidence-based approaches towards combating IPV in SSA due to the concomitant harmful consequences of IPV on the health and psychosocial wellbeing of women. IPV infringes on the rights of women and subsequently lowers their confidence and self-efficacy [6, 7]. Moreover, IPV is associated with many negative mental health outcomes including depression, heightened anxiety, and post-traumatic stress [8]. Women who experience IPV are most likely to have poor maternal and child health outcomes as they would not be able to seek early health care due to fear of being abused by their partners [9]. Considering the critical nature of IPV, the United Nations (UN) in its 17 Sustainable Development Goals [SDGs] re-emphasized the need to reduce and possibly eliminate IPV by 2030.
Also, given the relevance and timeliness of the need for evidence-based approach towards the fight against IPV, different researchers have investigated widely this phenomenon to aid policy and intervention development, and implementation [6,7,8, 10,11,12,13,14]. Most of these studies have investigated how socio-demographic characteristics such age, marital status, educational attainment, and employment status of women predict the likelihood of experiencing IPV as a woman [8, 15, 16]. However, in the context of SSA, studies investigating the influence of other critical factors, such as autonomy on the women’s probability of experiencing IPV have been sparse.
Sexual autonomy describes the independent decision-making related to issues of sex and its related activities. Our study’s conceptualization of women’s sexual autonomy is premised on Budu et al. [17] definition which holds that women’s sexual autonomy refers to a woman’s capacity to refuse sex, negotiate for safe sex practices such as insisting on partner to use condom, and feeling justified in asking a partner to use condom. Literature is replete with evidence that women with high sexual autonomy have significantly lower risk of adverse SRH outcomes including unwanted pregnancy [18] and non-use of modern contraceptives [19]. Amidst the preponderance of evidence establishing association between sexual autonomy and adverse SRH outcomes, there is paucity of information about the association between sexual autonomy and women’s likelihood of experiencing IPV. However, a study conducted in Nigeria [20] reported that women's sexual autonomy, which encompasses women’s ability to ask for condom during sex and refuse sex, has been associated with higher likelihood of women experiencing IPV. However, the findings of the study could not be generalized to the entire sub-Saharan African countries given the contextual differences. We, therefore, sought to fill the gap in literature and contribute to the use of empirical evidence in the fight against IPV by examining the association between sexual autonomy and IPV against married and cohabiting women in SSA. We hypothesize that women’s sexual autonomy is inversely associated with exposure to IPV. Findings from our study will inform policies and interventions aimed at eliminating IPV among married and cohabiting women through women empowerment initiatives.
Methods
Data source and study design
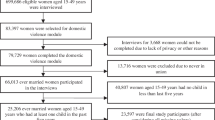
This study pooled data from the demographic and health survey (DHS) of 24 countries in SSA, which adopted a cross-sectional study design. DHS is a nationally representative survey that collects data on several health indicators including IPV and sexual autonomy across low- and middle-income countries. DHSs are mostly carried out every five years. However, the period can be extended in some countries due to certain conditions that exist in such countries. Data for each survey is collected from both men and women, which are sampled by a two-stage sampling technique [21]. The first stage involves the selection of clusters usually called enumeration areas (EAs). The second stage includes choosing of households for the survey. Sampling methodology and data collection procedure used by the DHS are found in a previous study [21]. Data collection was done by survey staff who were trained and instructed in standard DHS procedures. These procedures include general interviewing techniques, conducting interviews at the household level, measuring blood pressures and review of each question and mock interviews between participants. The DHS in SSA is usually conducted in English, French and Portuguese, depending on the official language of the country. For this study, the inclusion criteria were countries whose datasets were published between 2010 and 2019 and had information on the DHS domestic violence modules and sexual autonomy. Using the inclusion criteria, the DHS of 26 countries were initially identified. However, only the DHS of 24 countries had data on IPV and sexual autonomy. The two countries excluded in the study were Benin and Tanzania. Based on eligible respondents for the domestic violence modules [22], only ever married, currently married and cohabiting women were included. In all, 99,769 ever married, currently married and cohabiting women who completed information on IPV and sexual autonomy were included in this study. Table 1 shows the countries that were included in this study. The dataset is freely accessible via this link: https://dhsprogram.com/data/available-datasets.cfm. This paper was prepared in line with Strengthening Reporting of Observational studies in Epidemiology (STROBE) reporting guidelines (Additional file 1: Table S1) [23].
Study variables
Outcome variable
IPV was the dependent variable in this study. It was derived from three key variables namely, physical, emotional and sexual violence. These variables focused on a number of questions in the domestic violence module (DVM). However, questions in the DVM were derived from a modified version of the conflict tactics scale [24, 25]. On physical violence (PV), each respondent was asked whether her last partner ever pushed her; shook or threw something at her; slapped her; punched her with his fist or something harmful; kicked or dragged her; strangled or burnt her; threatened her with a knife, gun, or other weapons; and twisted her arm or pulled her hair. For emotional violence (EV), respondents were asked whether their last partner ever: humiliated her; threatened to harm her; and insulted or made her feel bad. Lastly, on sexual violence (SV), respondents were asked whether their partner ever physically forced the respondent into unwanted sex; whether the partner ever forced her into other unwanted sexual acts; and whether the respondent has been physically forced to perform sexual acts which she did not want to. For these questions, the responses were ‘yes’ and ‘no’. A respondent who had experienced at least one of the violent acts was considered as ever experienced physical, emotional or sexual violence. Ever had IPV was generated from all the questions asked on physical, emotional and sexual violence, and respondents who had encountered experienced at least one of these violent acts regarded as ever had IPV and otherwise. Similar coding has been used in previous studies that used DHS dataset [9, 26].
Key explanatory variable
The main explanatory variable for this study was sexual autonomy. This variable was created as an index of two questions consisting of “whether married/cohabiting women can refuse sex” and “whether married/cohabiting women can ask their partners to use condoms.” 1 = No; 2 = Yes; and 3 = don't know/not sure/depends were the answer choices in both questions. For this study, the respondents who responded “Don't know/not sure/depends” were dropped. Therefore, the final response options used in the analysis were 1 = No; and 2 = Yes. To create the variable “sexual autonomy” respondents who answered “Yes” to at least one of the questions was considered as having sexual autonomy while those who answered “No” to the two questions were considered as not having sexual autonomy. The selection of the variables and their recoding were informed by literature and availability in the dataset [27,28,29].
Covariates
Seven variables (age, level of education, marital status, current working status, place of residence, wealth quintile and media exposure) were considered in this study as covariates. We utilised the existing coding for age, educational level, current working status, place of residence, and wealth quintile as found in the DHS dataset. In the DHS, age was coded as ‘15–19’, ‘20–24’, ‘25–29’, ‘30–34’, ‘35–39’, ‘40–44’, and ‘45–49’. The level of education was coded as ‘no education’, ‘primary’, ‘secondary’, and ‘higher’. Using Principal Component Analysis (PCA), the wealth quintile in the DHS was analysed as an index of household assets and utilities and classified as “poorest,” “poorer,” “middle,” “richer,” and “richest.” The original wealth quintile categorization employed in the DHS was used in this study. Place of residence was coded as ‘urban’ and ‘rural’. Current working status was coded as ‘no’ and ‘yes’. Media exposure was generated from three variables on the frequency of watching television, reading newspaper/magazine, and listening to radio. Each of these variables were categorized into “not at all, less than once a week, at least once a week, and almost every day”, which were re-categorized into ‘No’ (not at all) and “Yes” (less than once a week, at least once a week, and almost every day). An index variable called mass media exposure was created using the recoded responses from the three variables. Any woman whose response option was “Yes” in any of the variables after the recoding was said to have been exposed to mass media whilst those that responded “No” in all the three were said to have no exposure to mass media.
Data analyses
Different data analyses were carried out using Stata version 16.0. For the first analysis, the prevalence of IPV and the proportion of women who had sexual autonomy were calculated from frequencies and percentages and were presented by bar charts. Second, Pearson’s chi-square test of independence was used to examine the independent associations between sexual autonomy and IPV (involving physical violence, emotional violence, and sexual violence) in each of the 24 countries included in this study. Finally, the association between sexual autonomy on IPV in each of the 24 countries was assessed through bivariable and multivariable binary logistic regression models. Two models (Model I and II) were built to examine the association between sexual autonomy and IPV. The first model (bivariable) consisted of only the sexual autonomy and IPV. In the second model (multivariable), we included all the covariates together with sexual autonomy and IPV. The results were presented as crude odds ratios (ORs) and adjusted odds ratios (AORs), at 95% confidence intervals (CIs). The women’s sample weights for the domestic violence module (d005/1,000,000) were applied to get unbiased estimates, according to the DHS guidelines. Also, the survey command (svy) in Stata was used to adjust for the complex sampling structure of the data in the regression analyses.
Ethical consideration
Ethical approval was not sought for thestudy since the analysis was done using publicly available data. Details about data and ethical standards are available at: http://goo.gl/ny8T6X.
Results
Background characteristics of the women in sub-Saharan Africa
Out of the 99,769 women, majority (21.4%) were aged 25–29 years. Most of the women had no education (37.1%), were married (78.2%), and exposed to mass media (66.8%). More than half (66.8%) of the women were currently working. Most (20.3%) of the women belonged to the poorer wealth quintile. Majority (64.2%) of the women were residing in rural areas (see Table 2).
Prevalence of IPV and sexual autonomy among women in sub-Saharan Africa
In the 24 sub-Saharan African countries studied, the prevalence of IPV was 38.5%. On the country level, the highest prevalence of IPV was 60.6% in Sierra Leone with the lowest in Comoros (9.8%) (Fig. 1). In terms of sexual autonomy among married and cohabiting women, the overall prevalence was 73.0%. Married and cohabiting women in Namibia had the highest prevalence of sexual autonomy with 97.8% and the lowest recorded in Mali (38.1%) (see Fig. 2).

Prevalence (%) of IPV among married and cohabiting women in SSA

Prevalence (%) of sexual autonomy among married and cohabiting women in SSA
Distribution of sexual autonomy among married and cohabiting women and IPV in Sub-Saharan Africa
Table 3 shows the distribution of sexual autonomy among married and cohabiting women across PV, EV, SV and IPV by countries in Central, West, East and Southern Africa. Sexual autonomy showed a significant association with PV, EV, SV, and overall IPV in SSA. In terms of specific violence, Sierra Leone recorded the highest PV (50.8%) and EV (44.1%) among those with sexual autonomy. Congo DR recorded the highest SV (24.0%) among women with sexual autonomy. Sexual autonomy had significant association with IPV in 13 countries (Angola, Cameroon, Chad, Gabon, Cote d’lvoire, Gambia, Nigeria, Burundi, Kenya, Uganda, Namibia, South Africa, and Zambia) out of the 24. Thus, in these countries, IPV was higher among married and cohabiting women who had sexual autonomy.
Association between sexual autonomy among married and cohabiting women and IPV in sub-Saharan Africa
The logistic regression analysis also showed significant association between sexual autonomy and IPV among women in sub-Saharan Africa. This, however, does not support our hypothesis that women’s sexual autonomy is inversely associated with risk of experiencing IPV. The odds of having IPV were higher among women with sexual autonomy [OR = 1.38, 95% CI = 1.31–1.44] but this reduced slightly after controlling for the confounders [aOR = 1.28, 95% CI = 1.21–1.35]. In the adjusted model, sexual autonomy had significant association with IPV among women in Angola, Cameroon, Chad, and Gabon in Central Africa. In West Africa, the odds of IPV were higher among women with sexual autonomy in Cote d’lvoire, Gambia, Mali, and Nigeria. In East Africa, sexual autonomy had significant association with IPV among women in Burundi, Comoros, and Kenya. Finally, in Southern Africa, sexual autonomy had significant association with IPV among women in South Africa, and Zambia (see Model II of Table 4).
Discussion
This study sought to determine the association between sexual autonomy and IPV among women in sexual unions in SSA. We found the pooled prevalence of sexual autonomy and IPV to be 73.0% and 38.5% respectively. Women who had sexual autonomy were more likely to experience IPV using the pooled data.
The pooled prevalence of IPV among the women in our study is comparable with the findings of previous studies [26, 30]. At the country level, the highest prevalence of IPV was 60.6% in Sierra Leone. This finding is not surprising since conflict and post-conflict situations increase the susceptibility of women to violence due to the deterioration of social protection measures during such times [8, 31, 32]. Another possible reason for the high prevalence of IPV in Sierra Leone could be explained by some socio-cultural factors. For instance, Horn et al. [33] revealed that culture and religion in Sierra Leone encourages women to remain in violent relationships. The idea is that women must remain in such relationships, to avoid leaving the children in the care of “wicked” stepmothers. Additionally, the use of IPV as a proxy punishment for women’s refusal to perform their conjugal duty, which is only excusable in a case of sickness could have accounted for the high prevalence of IPV [34]. Our study also recorded the lowest prevalence of IPV in Comoros, and this agrees with the finding of Izugbara et al. [8] that women in Comoros were the safest when it comes to IPV in SSA.
For sexual autonomy among married and cohabiting women, the overall prevalence was 73.0%. While this figure is relatively high, there exists cross-country differences that suggest that many countries in the sub-region still have lower rates of sexual autonomy among women. For example, while married and cohabiting women in Namibia recorded as high as 97.8% sexual autonomy, those in Mali recorded 38.1%. In effect, it is important for policies aimed at improving women’s sexual autonomy in the sub-region to pay critical attention to cross-country variations. Countries with low sexual autonomy among women deserve greater attention.
In this study, we found a significant association between sexual autonomy and IPV among women in SSA. This, however, did not support the hypothesis that women’s sexual autonomy is inversely associated with risk of experiencing IPV. Interestingly, the odds of IPV among women in sexual unions were higher among those with sexual autonomy compared to those without sexual autonomy. This finding is consistent with report from other study [26]. A study by Sunmola et al. [20] found that women with the ability to negotiate safer sex with their partners were more likely to experience more forms of violence in Nigeria. This could be that women with sexual autonomy would have the capacity to fight for their rights, which their husbands will interpret as a challenge to their authority, making them act violently towards their wives. Also, women with sexual autonomy would tend go against the cultural norms that preach subordination of women in intimate relationships, which may result in IPV. In most African settings, women cannot refuse or deny their partners sex unless they are menstruating, pregnant, breastfeeding, or are in their betrothal period. Hence, any attempt by a woman to deny or refuse sex is likely to be subjected to violence [35]. Deep-rooted cultural norms could have accounted for significant finding in our study. For example, cultural norms demand that women should conform and submit to their husbands’ sexual desires and demands without hesitation could have perpetrated IPV in situations where women refuse or try to negotiate for a safer sex [20].
Another important aspect of IPV that needs to be noted in terms of sexual violence and sexual autonomy is that women, who do not feel they have the right or are empowered to ask their partners to use condoms or refuse sex, have the tendency not to disclose sexual violence to people for legal action. This is due to the fact that in many African communities, sexual violence remains a sensitive topic to be discussed which is seen as a taboo for women to talk about it with their husband in some cultures. This, however, makes victims of sexual violence feel uncomfortable to report it in studies [36]. Therefore, studies on association between sexual autonomy and IPV need to be interpreted with caution.
Strengths and limitation
The study has some strengths and limitations. The main strength of the study lies in its use of nationally representative datasets of many countries in SSA. This notwithstanding, the study adopted a cross-sectional design, which prevents us from making causal inferences between the studied variables. Also, given the retrospective nature of reporting, which characterizes DHS data, this study is not immune to recall biases. Also, given the socio-cultural norms that surround issues of IPV in some countries, the data may be subject to social desirability biases. Furthermore, because the data was collected at different times, there could have been changes within and across countries that muddled the findings of this study. Hence, the generalization of the findings to all women in the respective countries should be done with caution.
Conclusion
This study found a significant association between sexual autonomy and IPV among women in SSA. This, however, did not support our hypothesis that women’s sexual autonomy is inversely associated with risk of experiencing IPV. The overall prevalence of IPV among women in 24 sub-Saharan African countries was 38.5% and that of sexual autonomy among married and cohabiting women was 73.0%. Moreover, sexual autonomy had significant association with IPV in 13 countries (Angola, Cameroon, Chad, Gabon, Cote d’lvoire, Gambia, Nigeria, Burundi, Kenya, Comoros, Uganda, South Africa, and Zambia). We suggest that social interventions aimed at empowering women in SSA must pay particular attention to countries with high rates of IPV. Based on our findings, there is the need for sub-Saharan African countries to step up programs that will improve IPV reporting and access to legal support for those who experience IPV. Despite the relevance of the study’s findings, we recommend that caution must be taken when interpreting the results on the association between the sexual autonomy and IPV since there is reporting bias concerning sexual violence.
Availability of data and materials
The dataset is freely accessible via this link: https://dhsprogram.com/data/available-datasets.cfm.
Abbreviations
- AOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
- COR:
-
Crude odds ratio
- DHS:
-
Demographic and Health Survey
- IPV:
-
Intimate partner violence
- SDGs:
-
Sustainable Development Goals
- SSA:
-
Sub-Saharan Africa
References
Potter LC, Morris R, Hegarty K, García-Moreno C, Feder G. Categories and health impacts of intimate partner violence in the World Health Organization multi-country study on women’s health and domestic violence. Int J Epidemiol. 2021;50(2):652–62.
Kabir R, Rahman S, Monte-Serrat DM, Arafat SY. Exploring the decision-making power of Bangladeshi women of reproductive age: results from a national survey. South East Asia J Med Sci. 2017;1(1):4–8.
Upadhyay UD, Gipson JD, Withers M, Lewis S, Ciaraldi EJ, Fraser A, Huchko MJ, Prata N. Women’s empowerment and fertility: a review of the literature. Soc Sci Med. 2014;115:111–20.
World Health Organization. Understanding and addressing violence against women: intimate partner violence (No. WHO/RHR/12.36). Geneva: World Health Organization; 2012.
World Health Organization. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violence. Geneva: World Health Organization; 2013.
Mukamana JI, Machakanja P, Adjei NK. Trends in prevalence and correlates of intimate partner violence against women in Zimbabwe, 2005–2015. BMC Int Health Hum Rights. 2020;20(1):1–11.
Spangenberg K, Wobil P, Betts CL, Wiesner TF, Gold KJ. Intimate partner violence among mothers of sick newborns in Ghana. Health Care Women Int. 2016;37(5):583–94.
Izugbara CO, Obiyan MO, Degfie TT, Bhatti A. Correlates of intimate partner violence among urban women in sub-Saharan Africa. PLoS ONE. 2020;15(3): e0230508.
Ahinkorah BO. Intimate partner violence against adolescent girls and young women and its association with miscarriages, stillbirths and induced abortions in sub-Saharan Africa: evidence from demographic and health surveys. SSM-Popul Health. 2021;13: 100730.
Durevall D, Lindskog A. Intimate partner violence and HIV in ten sub-Saharan African countries: what do the demographic and health surveys tell us? Lancet Glob Health. 2015;3(1):e34–43.
Lee-Rife SM. Women’s empowerment and reproductive experiences over the lifecourse. Soc Sci Med. 2010;71(3):634–42.
Meiksin R, Meekers D, Thompson S, Hagopian A, Mercer MA. Domestic violence, marital control, and family planning, maternal, and birth outcomes in Timor-Leste. Matern Child Health J. 2015;19(6):1338–47.
Roesch E, Amin A, Gupta J, García-Moreno C. Violence against women during covid-19 pandemic restrictions. BMJ. 2020;369: m1712.
Sabarwal S, Santhya KG, Jejeebhoy SJ. Women’s autonomy and experience of physical violence within marriage in rural India: evidence from a prospective study. J Interpers Violence. 2014;29(2):332–47.
Kwagala B, Wandera SO, Ndugga P, Kabagenyi A. Empowerment, partner’s behaviours and intimate partner physical violence among married women in Uganda. BMC Public Health. 2013;13(1):1–10.
Okenwa LE, Lawoko S, Jansson B. Exposure to intimate partner violence amongst women of reproductive age in Lagos, Nigeria: prevalence and predictors. J Fam Violence. 2009;24(7):517–30.
Budu E, Ahinkorah BO, Seidu AA, Hagan JE, Agbemavi W, Frimpong JB, Adu C, Dickson KS, Yaya S. Child marriage and sexual autonomy among women in Sub-Saharan Africa: evidence from 31 demographic and health surveys. Int J Environ Res Public Health. 2021;18(7):3754.
Abada T, Tenkorang EY. Women’s autonomy and unintended pregnancies in the Philippines. J Biosoc Sci. 2012;44(6):703–18.
Crissman HP, Adanu RM, Harlow SD. Women’s sexual empowerment and contraceptive use in Ghana. Stud Fam Plan. 2012;43(3):201–12.
Sunmola AM, Mayungbo OA, Fayehun OA, Opayemi RS, Morakinyo LA. Is women’s tendency to negotiate safer sex another opportunity for intimate partner violence in Nigeria? J Interpers Violence. 2021;36(7–8):NP3624–45.
Corsi DJ, Neuman M, Finlay JE, Subramanian SV. Demographic and health surveys: a profile. Int J Epidemiol. 2012;41(6):1602–13.
Hindin MJ, Kishor S, Ansara DL. Intimate partner violence among couples in 10 DHS countries: predictors and health outcomes. Macro International Incorporated; 2008.
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, Strobe Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–149.
Kishor S. Domestic violence measurement in the demographic and health surveys: the history and the challenges. Division for the Advancement of Women. 2005. p. 1–10.
Straus MA. Measuring intrafamily conflict and violence: the conflict tactics (CT) scales. London: Routledge; 2017.
Ahinkorah BO, Dickson KS, Seidu AA. Women decision-making capacity and intimate partner violence among women in sub-Saharan Africa. Arch Public Health. 2018;76(1):1.
Putra IG, Dendup T, Januraga PP. The roles of women empowerment on attitude for safer sex negotiation among Indonesian married women. Women Health. 2021;61(1):95–108.
Sano Y, Sedziafa AP, Vercillo S, Antabe R, Luginaah I. Women’s household decision-making autonomy and safer sex negotiation in Nigeria: an analysis of the Nigeria demographic and health survey. AIDS Care. 2018;30(2):240–5.
Tenkorang EY. Negotiating safer sex among married women in Ghana. Arch Sex Behav. 2012;41(6):1353–62.
Devries KM, Mak JY, Garcia-Moreno C, Petzold M, Child JC, Falder G, Lim S, Bacchus LJ, Engell RE, Rosenfeld L, Pallitto C. The global prevalence of intimate partner violence against women. Science. 2013;340(6140):1527–8.
Black E, Worth H, Clarke S, Obol JH, Akera P, Awor A, Shabiti MS, Fry H, Richmond R. Prevalence and correlates of intimate partner violence against women in conflict affected northern Uganda: a cross-sectional study. Confl Health. 2019;13(1):1.
Wako E, Elliott L, De Jesus S, Zotti ME, Swahn MH, Beltrami J. Conflict, displacement, and IPV: findings from two Congolese refugee camps in Rwanda. Violence Against Women. 2015;21(9):1087–101.
Horn R, Puffer ES, Roesch E, Lehmann H. ‘I don’t need an eye for an eye’: Women’s responses to intimate partner violence in Sierra Leone and Liberia. Glob Public Health. 2016;11(1–2):108–21.
Schneider LT. Partners as possession: a qualitative exploration of intimate partner sexual violence in Freetown, Sierra Leone. J Aggress Maltreat Trauma. 2019;28(2):127–45.
Amoakohene MI. Violence against women in Ghana: a look at women’s perceptions and review of policy and social responses. Soc Sci Med. 2004;59(11):2373–85.
Moletsane R, Mitchell C. Researching sexual violence with girls in rural South Africa. In: The Wiley handbook on violence in education: forms, factors, and preventions. Hoboken: Wiley; 2018. p. 433.
Acknowledgements
The authors thank the MEASURE DHS project for their support and for free access to the original data.
Funding
The study did not receive any funding.
Author information
Authors and Affiliations
Contributions
RGA, BOA, AS, LKD, JO, EA, and FAH conceived the study. RGA, LKD, FAH, BOA, and AS wrote the methods section and performed the data analysis. RGA, BOA, AS, LKD, JO, EA, and FAH were responsible for the initial draft of the manuscript. All the authors reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was not sought for the current study since the analysis was done using publicly available. Since, the dataset is already available in the public domain, no ethical approval was required for this study. Details about data and ethical standards are available at: http://goo.gl/ny8T6X.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
STROBE 2007 (v4) Statement—Checklist of items that should be included in reports of cross-sectional studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Aboagye, R.G., Dadzie, L.K., Arthur-Holmes, F. et al. Intimate partner violence against married and cohabiting women in sub-Saharan Africa: does sexual autonomy matter?. Reprod Health 19, 79 (2022). https://doi.org/10.1186/s12978-022-01382-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12978-022-01382-1