
Abstract
Background
The Mediterranean fever (MEFV) gene codes for protein pyrin, one of the regulators of inflammasome activity in innate immune cells. Mutations in this gene are considered the primary cause of Familial Mediterranean fever, but are also found in other monogenic and multifactorial autoinflammatory diseases. The aim of the study was to determine if healthy carriers of MEFV gene mutations and R202Q polymorphism have clinical manifestations of inflammation and impaired oxidative stress parameters.
Methods
One hundred DNA samples from healthy volunteers (13.3 ± 8.87 years of age (mean ± SD); range 2–35) were sequenced by ABI PRISM 310 automated sequencer (PE Applied Biosystems, Norwalk, USA). The Eurofever questionnaire was used to collect retrospectively medical history data. Oxidative stress was determined by measuring spectrophotometrically thiobarbituric acid reactive substances (TBARS) in plasma and erythrocytes, as well as advanced oxidation protein products in plasma. Superoxide dismutase (SOD) activity was determined by McCord and Fridovich method in plasma and erythrocytes, while the catalase erythrocyte activity was assessed using a catalase ELISA kit.
Results
We found heterozygous carriers of K695R/N mutations in 5 %, E148Q/N mutations in 6 %, R202Q homozygous polymorphism in 10 % and heterozygous R202Q alterations in 45 % of healthy volunteers. The MEFV mutation carriers and R202Q polymorphism homozygotes reported significantly more often recurrent febrile episodes (p = 0.009), diffuse abdominal pain (p = 0.025), and malaise (p = 0.012) compared to non-carriers. Erythrocyte TBARS levels and plasma SOD activity were higher in persons with MEFV mutations and R202Q/R202Q (p = 0.03 and p = 0.049, respectively).
Conclusions
Healthy individuals may bear E148Q and K695R MEFV gene mutations, as well as R202Q polymorphism in homozygous state. The determined gene alterations contribute to a subtle oxidative stress and may be associated with more frequent episodes of fever and unspecific inflammatory manifestations. An incomplete penetrance or variable expressivity of R202Q in populations of different ethnicity could influence the expression of autoinflammatory diseases phenotype.
Similar content being viewed by others

Background
The Mediterranean fever (MEFV) gene codes for the protein pyrin that is expressed in the cells of the innate immune system, especially granulocytes, monocytes, synovial fibroblasts and dendritic cells. Although the precise role of pyrin has not yet been clearly determined, it is one of the specific modulators of inflammasome, caspase-1 activation with interleukin-1β (IL-1β) production, activation of nuclear factor-kB and leukocyte apoptosis [1–4].
Clinical consequences of altered inflammasome regulation result from interleukin-1β effects and massive influx of activated leukocytes into tissues. Activated neutrophils and monocytes release proinflammatory cytokines, initiate acute-phase inflammatory response and undergo oxidative burst with an intense generation of reactive oxygen and nitrogen species via the NADPH oxidase complex and myeloperoxidase system [1–6].
The MEFV gene mutations are considered the primary cause of familial Mediterranean fever (FMF), the most common periodic fever syndrome and the prototype of monogenic autoinflammatory disease (AID). However, MEFV gene mutations are also frequently found in other AIDs, including Behcet’s disease, Henoch-Schönlein purpura, polyarteritis nodosa, ulcerative colitis, multiple sclerosis, etc. The knowladge about its role in the pathogenesis of these diseases is still obscure, but it is hypothesized that MEFV mutations could predispose to proinflammatory states [7–11].
Familial Mediterranean fever predominantly affects the populations of eastern Mediterranean origin, such as Turks, Jews, Arabs and Armenians. There is no official registry of FMF prevalence in Serbia, and its clinical diagnosis is very rare. The most frequent clinical manifestations of FMF are self-limited recurrent attacks of high fever (>38 °C) and sterile serositis (mostly peritonitis), synovitis and erysipeloid rash [1–3]. In the attack period, there are high levels of acute-phase reactants, leukocytosis and increased oxidative stress, evidenced by defective antioxidant defenses and enhanced oxidation products. The parameters usually return to normal in the remission period. However, in some patients, subclinical inflammation and oxidative stress are reported during the disease-free period as well [12–15].
In a large percentage of FMF patients, these five MEFV mutations are most frequently found: M680I, M694V, M694I and V726A in exon 10, and E148Q in exon 2. M694V homozygotes have a severe form of the disease, while mutations, such as E148Q and V726A, have a reduced penetrance and rarely cause any symptoms [2, 4, 16, 17].
The precise influence of R202Q alteration, in exon 2 of the MEFV gene, on inflammasome activity has been analysed additionaly. A high frequency of R202Q heterozygosity is detected in various populations and does not seem to cause any autoinflammatory effect in its carriers. Since this high carrier rate could not be explained by inbreeding or genetic drift, it is proposed to represent a selective advantage, a type of balancing selection, possibly toward increased innate immune response to a yet unidentified pathogen [3, [18–21]. In contrast, the frequency of R202Q homozygosity is very low and has been found to be associated with autoinflammatory manifestations in FMF patients that do not have any MEFV mutation or when R202Q is in compound heterozygous state with a mutation. This shows that despite its low frequency, the R202Q homozygosity has a high penetrance rate and suggests a potent dosage-dependent pro-inflammatory effect [15, 21–23].
The aim of the study was to determine if healthy carriers of MEFV gene mutations and R202Q polymorphism have clinical manifestations of inflammation and impaired oxidative stress parameters.
Methods
The study was conducted in compliance with the Declaration of Helsinki and Good Clinical Practice (GCP) Guidelines. The relevant study documents were approved by an independent Ethics Committee and the informed consent forms were obtained from the participants.
This cross-sectional study was performed as an addition to the recently published study by Debeljak M. et al. [24] intended to evaluate the distribution of MEFV gene mutations in healthy populations of South-East Europe. One hundered healthy subjects (age > 2 years) or their parents have signed informed consent for blood samples to be collected for genetics and oxidative stress parameters analysis, as well as medical history data. The Eurofever project questionnaire [25, 26] was used to collect retrospectivelly the data about occurrence of inflammatory clinical manifestations during their life. The questionnaire is designed to recognize autoinflammatory syndromes and to collect information about clinical presentations in patients with a genetically confirmed diagnosis of AID or suspected cases on the basis of positivity of diagnostic criteria. A part of the questionnaire about clinical manifestations describes the characteristics of disease episodes for a recurrent disease course, with detailed analysis of fevers (frequency, duration, triggers, etc.), muco-cutaneous manifestations, musculoskeletal system, lymphoid organs and other organ systems, constitutional symptoms (fatigue, malaise, weight loss, insomnia, etc.), surgical procedures, family history, laboratory findings (routine and specific blood examinations), imaging and drug therapy. Recurrent fever was defined as 3 or more episodes of fever (≥38.0 °C) in a 6 months interval, that lasted for a few days without any identified cause after thorough examination, followed by a fever-free interval (with a sense of well-being) of at least 2 weeks. Clinical manifestations were compared between the persons with determined MEFV mutations and R202Q polymorphism and the control group that comprised all the persons without MEFV mutations.
Healthy volunteers can be considered as representative of Serbian population since questionnaire and blood samples were obtained when subjects were performing routine blood tests for health check up. Inclusion criteria were absence of acute and chronic illnesses, fever free period of at least 2 weeks prior to the blood samples collection, and a signed informed consent. Blood samples with EDTA were collected at the Department of Pediatric Rheumatology, Clinical Center in Nis, Serbia. 200 μl of the whole blood was used for DNA isolation by DNeasy Blood & Tissue Kit (QIAGEN Inc., Valencia, CA, USA). The DNA samples were tested for the presence of MEFV gene mutations within the multinational Eurofever Project (EAHC, Project No2007332) [24–26]. The MEFV gene exons 2 and 10 were amplified individualy by PCR. The exon 2 (360 bp) was amplified using the forward 5′-AAAACGGCACAGATGATTCCG-3′ and reverse 5′-AAGGGCCTGCACTCCTTC-3′ primers, and exon 10 (400 bp) by the following primers: forward 5′-AGCAGGAAGAGAGATGCAGTG-3′ and reverse 5′-TTGGAGACAAGACAGCATGG-3′. The exon 10 amplicons were primarily screened using Denaturing high performance liquid chromatography (dHPLC), for separation of those with normal nucleotide sequences (WAVE®Systems 4500 Series, Transgenomic, Inc., Omaha: NE, USA). Thereafter, sequencing was carried out using the Big Dye Terminator cycle sequencing kit and ABI PRISM 310 automated sequencer (PE Applied Biosystems, Norwalk, USA). The exon 2 amplicons were directly sequenced using the same method. The sequencing was performed at the Center for Medical Genetics, University Children’s Hospital Ljubljana, Slovenia. Obtained nucleotide sequences were compared with MEFV gene sequences at the [GenBank:NM_000243.2].
Complete blood count parameters were assessed using COULTER® AcT Diff Analyzer (Beckman Coulter Corporation, Hialeah, FL, USA). For C-reactive protein (CRP) and albumins concentration measurement we used fully automated Erba Mannheim XL600 analyzer (ERBA Diagnostics Mannheim Gmbh, Baden-Wurttemberg, Germany). Erythrocyte sedimentation rate (ESR) was assessed using the Westergren ESR method [27].
Lipid peroxidation was evaluated measuring thiobarbituric acid reactive substances (TBARS) in plasma and washed erythrocytes. TBARS in erythrocytes were assessed spectrophotometrically using the method by Jain et al. [28]. Trichloroacetic acid and tertiary butyl alcohol were added to erythrocytes in phosphate buffer (pH-7.4) forming the chromogen. The absorption was measured at 532 nm wavelength. TBARS concentration was expressed as nmol/g of hemoglobin. TBARS concentration in plasma was determined spectrophotometrically using the method by Andreeva et al. [29]. This method is based on the reaction of malondialdehyde (MDA) with thiobarbituric acid, at a high temperature and low pH. Measurement of MDA-TBA2 chromogen was than assessed at 532 nm wavelength.
Protein oxidation was measured spectrophotometrically by determination of advanced oxidation protein products (AOPP) in plasma, according to chloramine T solution, which in the presence of potassium iodide have absorbance at 340 nm [30].
Total superoxide dismutase (SOD) activity was measured in plasma and erythrocytes. The activities of both SODs were determined by measuring the inhibition of pyrogallol autoxidation [31]. This is a “negative” type of reaction, as we measure the decrease of nitroblue tetrazolium oxidation at the expense of pyrogallol autoxidation under alkaline conditions. One unit of SOD was defined as the amount of enzyme that causes 50 % inhibition of the pyrogallol autooxidation rate at 420 nm.
The catalase activity was determined in erythrocyte lysates using a catalase ELISA kit (Enzo Life Sciences, Inc., Farmingdale, NY 11735, USA), according to the manufacturer’s instructions.
The results were expressed as means ± standard deviations (SD) or medians ± interquartile range (IQR), as required. Statistical analysis was conducted using Chi-squared test for association (with Phi and Cramer’s V test for the strength of association (Phi)), with statistical significance at p < 0.05, and Fisher’s exact test when necessary. The Hardy-Weinberg principle was applied to test for R202Q polymorphism. Conditional logistic regression analysis for matched data was used to estimate an interaction between genotype and clinical manifestations (outcome). Statistical analysis of oxidative stress parameters was conducted using the Mann-Whitney U-test. For correlation between the parameters we used Spearman’s rank order correlation. Statistical analyses were performed using SPSS 17.0 (SPSS, Chicago, IL, USA) statistical program.
Results
Out of 100 healthy volonteeers enrolled, 47 were males and 53 females, with average age of 13.3 ± 8.87 years (mean ± SD) (range 2–35). All study subjests were Caucasians of the Serbian ethnicity, without family history of FMF or other autoinflammatory disease and no consanguinity. No demographic differences were determined between persons with different MEFV genotype.
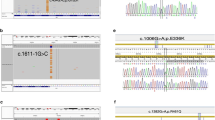
The DNA samples sequencing has found that 11 % (n = 11) of subjects have MEFV gene mutations. No homozygous mutation for MEFV gene was determined. We have only found heterozygous MEFV gene mutation K695R/N (c.2084A > G) in exon 10 in 5 % (n = 5) of subjects, and E148Q/N (c.442G > C) mutation in exon 2 in 6 % (n = 6) of subjects. These subjects comprised the group we named “MEFV mutation carriers”.
The R202Q (c.605G > A) homozygous polymorphism was found in 10 % (n = 10) of subjects, and we named this group “R202Q homozygotes”. Only one subject had heterozygous K695R/N mutation in combination with R202Q homozygous state why we used his data for analysis in two groups (“MEFV mutation carriers” and “R202Q homozygotes”). Data for the groups MEFV mutation carriers and R202Q homozygotes were pulled together in larger group for more precise statistical analysis, and we named this group “MEFV/R202Qhomo”.
Heterozygous R202Q polymorphism was fond in 45 % (n = 45) of subjects, and they together with subjects with no MEFV mutations nor R202Q polymorphism (N/N) made the group named “control group” (n = 80) (N/N plus R202Q/N) (average age of 15.3 ± 11.6 years). No demographic differences were determined between subjects in different groups.
The allele and genotype frequencies for R202Q polymorphism were in Hardy-Weinberg equilibrium. However, the expected frequency of R202Q recessive phenotype (aa) was quite low: 10.6 % (f(a) = 0.325).
Erythrocyte TBARS levels were higher in MEFV/R202Qhomo group compared to the control group (p = 0.03, U = 84) (Fig. 1a). There was no difference in TBARS concentrations in plasma (p = 0.946, U = 161), nor AOPP levels (p = 0.322, U = 121), between the groups. There was positive corelation between AOPP and erythrocyte TBARS levels, but not statistically significant (rs = 0.643, p = 0.086). Plasma SOD levels were higher in MEFV/R202Qhomo group than in the control group (p = 0.049, U = 58.5) (Fig. 1b). Although the activities of erythrocyte SOD and catalase were lower in MEFV/R202Qhomo group, the difference was not statistically significant (for both groups p = 0.439). The R202Q homozygotes had significantly higher values of SOD plasma levels compared to the control group (p = 0.001) (Table 1). All the examined oxidative stress parameters did not show any important differences among subjects who were heterozygous for R202Q polymorphism and those without R202Q (N/N).

The significant difference of oxidative stress parameters in study subjects according to MEFV genotype group. a The TBARS concentrations in erythrocytes (median ± IQR) according to the MEFV genotype. *p = 0.03, compared to others. b Total SOD activity in plasma (mean ± SD) according to the MEFV genotype. *p = 0.001 and **p = 0.049, compared to others. MEFV/R202Qhomo - MEFV mutation carrier plus R202Q homozygotes group, Control group - N/N and R202Q/N
None of the subjects met clinical diagnostic criteria for FMF or other autoinflammatory diseases. In order to evaluate clinical manifestations in our subjects according to the MEFV genotype, we compared clinical manifestations frequency between defined groups (Table 2). Data was missing for 4 subjects in control group (N/N plus R202Q/N), for different manifestations and their data were excluded.
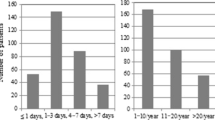
The subjects in MEFV/R202Qhomo group reported significantly more often: recurrent febrile episodes of unknown cause (p = 0.002, Phi = 0.319), diffuse abdominal pain (p = 0.007, Phi = 0.277), peritonitis (p = 0.004, Phi = 0.321), and malaise/fatigue (p = 0.002, Phi = 0.349) compared to control group (Fig. 2). The results revealed a medium strong correlation between the occurrence of recurrent fever and determined heterozygous MEFV mutations and R202Q homozygosity. Average duration of fever episodes were 3.64 ± 1.26 days, and they reoccurred after 3.1 ± 1.2 months on the average.

The clinical manifestations between mutation carriers with R202Q homozygotes and persons without MEFV gene changes. *p < 0.026. MEFV/R202Qhomo - MEFV mutation carrier plus R202Q homozygotes group, Control group - N/N and R202Q/N
The subjects in MEFV mutation carriers group experienced more often: recurrent febrile episodes of unknown cause (p = 0.048, Phi = 0.213), diffuse abdominal pain (p = 0.023, Phi = 0.256), peritonitis (p = 0.01, Phi = 0.326), and malaise/fatigue (p = 0.006, Phi = 0.336), compared to control group (n = 76). Subjects in R202Q homozygotes group, compared to control group, had significantly higher rates of recurrent fever (p = 0.022, Phi = 0.252), diffuse abdominal pain (p = 0.047, Phi = 0.224), and lymphadenopathy (p = 0.049, Phi = 0.216).
According to the conditional logistic regression analysis, no mutation nor R202Q alteration could significantly predict the development of most common clinical manifestations in our study group.
Complete blood count parameters and basic biochemical analyses (albumins, hemoglobin, CRP and ESR) were not different between the groups. There was a positive correlation between erythrocyte TBARS and leukocyte count (rs = 0.838, p = 0.009), as well as between plasma SOD levels and ESR (rs = 0.798, p = 0.031) in MEFV/R202Qhomo group.
Discussion
The observed MEFV heterozygote mutation carrier rate of 11 % is relatively high for the Serbian healthy population. The clinical diagnosis of FMF, by applying Tel Hashomer criteria, is very rare in Serbia. It is possible that absence of FMF cases in Serbia is maybe due to the lack of the most commonly found mutations (M694V, V726A, M680I and M694I) and genotypes that are found in other populations in Mediterranean area. The mutations determined in our study were predominantly heterozygous E148Q and K695R. The E148Q mutation is frequently found in different populations and is usualy associated with milder clinical features with reduced penetrance. It is suggested to predispose to an inflammatory phenotype when in combination with other pro-inflammatory factors [32, 33]. In contrast to E148Q, K695R is considered a rare MEFV gene mutation. Generally, K695R has been found both as the sole mutation in FMF patients and in asymptomatic individuals. Because of its weak phenotypic presentation it has been supposed to predispose to subtle inflammatory changes [17, 20, 33–35]. We did not determine M694V mutation in our subjects and thus cannot say that there is linkage disequilibrium with the R202Q variant. The p.Ser52Asn of MVK and p.Gln703Lys of NLRP3 are not been analyzed and it would be interesting for further studies to investigate association of these changes [36].
It is interesting that in different persons the same MEFV mutation can be asymptomatic, it may present with inflammatory symptoms, or even be considered responsible for autoinflammatory disease [4, 16, 17]. Recognition of an inflammatory phenotype in single-mutation cases suggests that mutations lead to a gain-of-function with gene-dosage effect, rather than a simple loss-of-function recessive model, which has been considered their primary result [2, 18–20].
We observed a very high R202Q heterozygous carrier rate (45 %), as well as R202Q homozygosity in healthy individuals (10 %) compared to other studies, but without any clear influence on the phenotype. On the contrary, R202Q homozygosity was found in 9.2 % of Greek FMF patients [20] and in 43 % of Turkish FMF patients [22] in whom the phenotype corresponded to the characteristic autoinflammatory phenotype, with fever, serositis and monoarthritis occurring most frequently. Karakus et al. [37] showed that homozygous R202Q genotype was significantly higher in fibromyalgia patients than in healthy controls, and that morning fatique and irritable bowel syndrome had significant associations with this polymorphism.
In addition to the inflammatory symptoms, increased oxidative stress has been reported in AID patients during attacks, as well as in remission periods [14, 15]. It has been reported that neutrophils harboring MEFV gene mutations produce high levels of superoxide anion without any stimulation [6].
Since erythrocytes effectively scavenge reactive oxygen species, their membranes are simultaneously influenced by free radicals, intracellular antioxidative systems and plasma antioxidants. They are therefore regarded as a good indicator of lipid peroxidation [38]. The subjects in MEFV/R202Qhomo group in this study had significantly higher concentrations of erythrocytes TBARS, which might partly be the result of insufficient or depleted cellular antioxidant protection. The erythrocyte SOD and catalase activity were decreased in these persons but not statisticaly significant, and this should be reanalysed in a larger study group. It has been reported that FMF patients have significantly decreased activities of these enzymes in the attack period [13, 14]. Advanced oxidation protein products are novel oxidative stress and inflammation markers. Activated neutrophils are shown to participate directly in their formation [39]. There are no many studies evaluating the AOPP levels in FMF patients with MEFV mutations. Sahin et al. [40] determined lower AOPP levels in FMF patients with attack-free period than in controls. They studied AOPP levels according to the paraoxonase phenotype and found that FMF patients with a QQ phenotype exhibited lower AOPP levels than the controls, while there was not significant difference if the patients had QR + RR paraoxonase phenotype. However, comparably, free thiol levels and protein carbonyl groups are changed in the attack periods, decreased and increased respectively [13, 14]. Although not statistically significant, AOPP levels were increased in MEFV/R202Qhomo group subjects and positively correlated with TBARS erythrocyte levels. This all implies on a complex oxidative regulation depending on various factors.
The major SOD isoenzyme in plasma is CuZn-extracellular SOD (EC-SOD), mostly secreted by endothelial cells [41, 42]. Leukocytes produce high levels of superoxide anion after activation and EC-SOD is the main enzymatic scavenger in the extracellular matrix. Compared to other antioxidative enzymes, induction and regulation of EC-SOD is governed by cytokines and not its substrate O2 − or other oxidants [43, 44]. Elevated plasma SOD levels were reported to reflect a response to increased oxidative stress in cancer patients and were implicated as a sensitive marker of inflammatory processes [45, 46]. Moreover, increased plasma SOD activity was observed in severe forms of acute appendicitis, indicating increased neutrophil infiltration and inflammation [47]. Considering inflammasome dysfunction in leukocytes with mutated pyrin, the increased plasma SOD activity in our study was perhaps an adaptive response to enhanced leukocyte activation and IL-1β release, since the leukocyte count was not significantly changed.
Most prevalent clinical manifestations in a FMF attack are fever and abdominal pain due to peritonitis [2, 3]. These symptoms are seen not only in homozygotes for the most common MEFV mutations, but also in compound heterozygote carriers [20, 34]. Healthy volunteers in our study could not be diagnosed as FMF or any other AID, but the mutation carriers and R202Q homozygotes reported recurrent fever and diffuse abdominal pain significantly more often than non-carriers. This could indicate that persons with heterozygous mutations and R202Q/R202Q changes had an impaired innate immunity response. Additionally, this might imply an increased risk of developing inflammatory conditions during life. Unfortunately, due to the cross-sectional design of our study, this can be only speculated about, and prospective (life time) clinical follow-up studies are therefore warranted.
However, neither mutation nor R202Q/R202Q could predict an inflammatory outcome in our study. The persons affected had occasional health problems that could not be significantly associated with the presence of detected gene changes. Additionally, there were no signs of subclinical inflammation. Types and frequency of clinical manifestations in R202Q homozygotes group were not different in comparison to the E148Q and K695R heterozygotes, pointing to the similar effect of this MEFV gene change. An influence of gene-dosage effect could be proposed, as R202Q heterozygosity was quite frequent but was not associated with a particular health problem.
Although R202Q homozygosity was found in patients with typical FMF presentation in other studies [21, 22] the symptoms reported by our R202Q homozygotes were mild, atypical and often without accompanying fever. This is perhaps the consequence of an incomplete penetrance or variable expressivity of R202Q in the Serbian population caused by the influence of additional genetic or environmental factors characteristic for this region.
Conclusion
Healthy individuals may bear E148Q or K695R mutations of the MEFV gene, as well as R202Q alteration in the homozygous state in Serbia. An incomplete penetrance or variable expressivity of R202Q in populations of different ethnicity could influence the expression of autoinflammatory disease phenotypes. These gene changes may influence innate immunity and oxidative stress regulation. MEFV gene changes do not necessarily induce an autoinflammatory disease in the Serbian population, but may be responsible for more frequent occurrence of fever episodes and unspecific inflammatory manifestations in carriers.
Abbreviations
AID, autoinflammatory diseases; AOPP, advanced oxidation protein products; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; FMF, familial Mediterranean fever; GCP, good clinical practice; IL-1β, interleukin-1β; IQR, interquartile range; MEFV, Mediterranean fever; SD, standard deviation; SOD, superoxide dismutase; TBARS, thiobarbituric acid reactive substances
References
Diaz A, Hu C, Kastner DL, Schaner P, Reginato AM, Richards N, et al. Lipopolysaccharide-induced expression of multiple alternatively spliced MEFV transcripts in human synovial fibroblasts: a prominent splice isoform lacks the C-terminal domain that is highly mutated in familial Mediterranean fever. Arthritis Rheum. 2004;50:3679–89.
Chae JJ, Aksentijevich I, Kastner DL. Advances in the understanding of familial Mediterranean fever and possibilities for targeted therapy. Br J Haematol. 2009;146(5):467–78.
Papadopoulos VP, Giaglis S, Mitroulis I, Ritis K. The population genetics of familial Mediterranean fever: a meta-analysis study. Ann Hum Genet. 2008;72(Pt 6):752–61.
Chae JJ, Cho YH, Lee GS, Cheng J, Liu PP, Feigenbaum L, et al. Gain-of-function Pyrin mutations induce NLRP3 protein-independent interleukin-1β activation and severe autoinflammation in mice. Immunity. 2011;34(5):755–68.
Witko-Sarsat V, Gausson V, Descamps-Latscha B. Are advanced oxidation protein products potential uremic toxins? Kidney Int Suppl. 2003;84:S11–4.
Sarkisian T, Emerit I, Arutyunyan R, Levy A, Cernjavski L, Filipe P. Familial Mediterranean fever: clastogenic plasma factors correlated with increased O2(−) – production by neutrophils. Hum Genet. 1997;101:238–42.
Yazici A, Cefle A, Savli H. The frequency of MEFV gene mutations in Behcet’s disease and their relation with clinical findings. Rheumatol Int. 2012;32(10):3025–30.
Yalçinkaya F, Ozçakar ZB, Kasapçopur O, Oztürk A, Akar N, Bakkaloğlu A, et al. Prevalence of the MEFV gene mutations in childhood polyarteritis nodosa. J Pediatr. 2007;151(6):675–8.
Gershoni-Baruch R, Broza Y, Brik R. Prevalence and significance of mutations in the familial Mediterranean fever gene in Henoch-Schönlein purpura. J Pediatr. 2003;143(5):658–61.
Yıldırım B, Tuncer C, Kan D, Tunc B, Demirag MD, Ferda Percın E, et al. MEFV gene mutations and its impact on the clinical course in ulcerative colitis patients. Rheumatol Int. 2011;31(7):859–64.
Kümpfel T, Gerdes LA, Wacker T, Blaschek A, Havla J, Krumbholz M, et al. Familial Mediterranean fever-associated mutation pyrin E148Q as a potential risk factor for multiple sclerosis. Mult Scler. 2012;18(9):1229–38.
Sahin M, Uğuz AC, Demirkan H, Nazıroğlu M. Colchicine modulates oxidative stress in serum and leucocytes from remission patients with Family Mediterranean Fever through regulation of Ca2+ release and the antioxidant system. J Membr Biol. 2011;240(1):55–62.
Ediz L, Ozkol H, Tekeoglu I, Tuluce Y, Gulcu E, Koyuncu I. Increased oxidative stress in patients with familial Mediterranean fever during attack period. Afr Health Sci. 2011;11 Suppl 1:S6–S13.
Guzel S, Andican G, Seven A, Aslan M, Bolayirli M, Celik Guzel E, et al. Acute phase response and oxidative stress status in familial Mediterranean fever (FMF). Mod Rheumatol. 2012;22:431–7.
Korkmaz C, Ozdogan H, Kasapcopur O, Yazici H. Acute phase response in familial Mediterranean fever. Ann Rheum Dis. 2002;61:79–81.
Gershoni-Baruch R, Shinawi M, Leah K, Badarnah K, Brik R. Familial Mediterranean fever: prevalence, penetrance and genetic drift. Eur J Hum Genet. 2001;9(8):634–7.
Aksentijevich I, Torosyan Y, Samuels J, Centola M, Pras E, Chae JJ. Mutation and haplotype studies of familial Mediterranean fever reveal new ancestral relationships and evidence for a high carrier frequency with reduced penetrance in the Ashkenazi Jewish population. Am J Hum Genet. 1999;64(4):949–62.
Booty MG, Chae JJ, Masters SL, Remmers EF, Barham B, Le JM, et al. Familial Mediterranean fever with a single MEFV mutation: where is the second hit? Arthritis Rheum. 2009;60:1851–61.
Yagel D, Berkun Y, Padeh S, Abu A, Reznik-Wolf H, Livneh A, et al. Clinical disease among patients heterozygous for familial Mediterranean fever. Arthritis Rheum. 2009;60:1862–6.
Giaglis S, Papadopoulos V, Kambas K, Doumas M, Tsironidou V, Rafail S, et al. MEFV alterations and population genetics analysis in a large cohort of Greek patients with familial Mediterranean fever. Clin Genet. 2007;71(5):458–67.
Ritis K, Giaglis S, Spathari N, Micheli A, Zonios D, Tzoanopoulos D, et al. Non-isotopic RNase cleavage assay for mutation detection in MEFV, the gene responsible for familial Mediterranean fever, in a cohort of Greek patients. Ann Rheum Dis. 2004;63(4):438–43.
Ozturk A, Ozcakar B, Ekim M, Akar N. Is MEFV gene Arg202Gln (605G > A) A disease-causing mutation? Turk J Med Sci. 2008;38(3):205–8.
Şahin A, Erten Ş, Altunoğlu A, Işıkoğlu S, Neşelioğlu S, Ergin M, et al. Comparison of serum oxidant and antioxidant parameters in familial Mediterranean fever patients (FMF) with attack free period. Acta Reumatol Port. 2014;39(4):316–21.
Debeljak M, Toplak N, Abazi N, Szabados B, Mulaosmanović V, Radović J, et al. The carrier rate and spectrum of MEFV gene mutations in central and southeastern European populations. Clin Exp Rheumatol. 2015;33(6 Suppl 94):S19–23.
The Autoinflammatory Diseases’ Working Group of the Paediatric Rheumatology European Society (PRES) and the Executive Agency for Health and Consumers (EAHC, Project No2007332): Eurofever project: Eurotraps. 2009. http://fmf.igh.cnrs.fr/ISSAID/EUROTRAPS/intranet/doc/D2.1_appendix1.pdf. Accessed 20 Feb 2014.
The Autoinflammatory Diseases’ Working Group of the Paediatric Rheumatology European Society (PRES) and the Executive Agency for Health and Consumers (EAHC, Project No2007332): Eurofever project: Eurotraps. 2009. http://fmf.igh.cnrs.fr/ISSAID/EUROTRAPS/intranet/doc/D2.1_appendix2.pdf. Accessed 20 Feb 2014.
Thomas RD, Westengard JC, Hay KL, Bull BS. Calibration and validation for erythrocyte sedimentation tests: role of the International Committee on Standardization in Hematology reference procedure. Arch Pathol Lab Med. 1993;117:719–23.
Jain SK, McVie R, Duett J, Herbst JJ. Erythrocyte membrane lipid peroxidation and glycosylated hemoglobin in diabetes. Diabetes. 1989;38:1539–43.
Andreeva JL, Kozjemakin AL, Kiskun AA. Modifikacija metoda opredelnija perekisej lipidov testes tiobarbiturovoj kisloti. Lab Delo. 1988;11:41–3.
Witko-Sarsat V, Friedlander M, Capeillère-Blandin C, Nguyen-Khoa T, Nguyen AT, Zingraff J, et al. Advanced oxidation protein products as a novel marker of oxidative stress in uremia. Kidney Int. 1996;49(5):1304–13.
McCord JM, Fridovich I. Superoxide dismutase: an enzymic function for erythrocuprein (hemocuprein). J Biol Chem. 1969;244:6049–55.
Gökçe I, Gökçe S, Kılıç A, Bozlar U, Kocaoğlu M, Ongürü O, et al. Familial Mediteranean fever with protein-losing enteropathy due to constrictive pericarditis. World J Pediatr. 2011;7(4):365–7.
Topaloglu R, Ozaltin F, Yilmaz E, Ozen S, Balci B, Besbas N, et al. E148Q is a disease-causing MEFV mutation: a phenotypic evaluation in patients with familial Mediterranean fever. Ann Rheum Dis. 2005;64:750–2.
Caglayan AO, Demiryilmaz F, Ozyazgan I, Gumus H. MEFV gene compound heterozygous mutations in familial Mediterranean fever phenotype: a retrospective clinical and molecular study. Nephrol Dial Transplant. 2010;25(8):2520–3.
Akin H, Onay H, Turker E, Cogulu O, Ozkinay F. MEFV mutations in patients with Familial Mediterranean Fever from the Aegean region of Turkey. Mol Biol Rep. 2010;37(1):93–8.
Shinar Y, Obici L, Aksentijevich I, Bennetts B, Austrup F, Ceccherini I, et al. Guidelines for the genetic diagnosis of hereditary recurrent fevers. Ann Rheum Dis. 2012;71(10):1599–605.
Karakus N, Yigit S, Inanir A, Inanir S, Toprak H, Okan S. Association between sequence variations of the Mediterranean fever gene and fibromyalgia syndrome in a cohort of Turkish patients. Clin Chim Acta. 2012;414:36–40.
Kolanjiappana K, Manoharana S, Kayalvizhi M. Measurement of erythrocyte lipids, lipid peroxidation, antioxidants and osmotic fragility in cervical cancer patients. Clin Chim Acta. 2002;326:143–9.
Piwowar A. Advanced oxidation protein products. Part I. Mechanism of the formation, characteristics and property. Pol Merkur Lekarski. 2010;28(164):166–9.
Sayın Kocakap DB, Günel-Özcan A, Çabuk F, Ensari C. The frequency of Familial Mediterranean fever gene mutations and genotypes at Kirikkale and comparison with the mean of regional MEFV mutation frequency of Turkey. Mol Biol Rep. 2014;41(3):1419–26.
Sandström J, Karlsson K, Edlund T, Marklund SL. Heparin-affinity patterns and composition of extracellular superoxide dismutase in human plasma and tissues. Biochem J. 1993;294(Pt 3):853–7.
Adachi T, Ohta H, Yamada H, Futenma A, Kato K, Hirano K. Quantitative analysis of extracellular-superoxide dismutase in serum and urine by ELISA with monoclonal antibody. Clin Chim Acta. 1992;212:89–102.
Mates JM, Perez-Gomez C, De Castro IN. Antioxidant enzymes and human diseases. Clin Biochem. 1999;32(8):595–603.
Nozik-Grayck E, Suliman HB, Piantadosi CA. Extracellular superoxide dismutase. Int J Biochem Cell Biol. 2005;37(12):2466–71.
Hasan HR, Mathkor TH, Al-Habal MH. Superoxide dismutase isoenzyme activities in plasma and tissues of Iraqi patients with breast cancer. Asian Pac J Cancer Prev. 2012;13(6):2571–6.
Andrade BB, Reis-Filho A, Souza-Neto SM, Raffaele-Netto I, Camargo LM, Barral A, et al. Plasma superoxide dismutase-1 as a surrogate marker of vivax malaria severity. PLoS Negl Trop Dis. 2010;4(4):e650.
Koltuksuz U, Uz E, Ozen S, Aydinç M, Karaman A, Akyol O. Plasma superoxide dismutase activity and malondialdehyde level correlate with the extent of acute appendicitis. Pediatr Surg Int. 2000;16(8):559–61.
Acknowledgements
This work was partly supported by the Eurofever Project (EAHC, Project No2007332) and by the Project No. 41018 and 31060 of Ministry of Education and Science in Serbia.
Funding
The work was partly supported by the Eurofever Project (EAHC, Project No2007332) in the part of DNA samples analysis in Slovenia. Also, it was partly funded by the Projects No. 41018 and 31060 of Ministry of Education, Science and Technological Development of Republic of Serbia, through covering funds of materials for biochemical analysis.
Availability of data and materials
The dataset supporting the conclusions of this article is available in the GenBank (National Center for Biotechnology Information) repository, RRID:nif-0000-02873 and hyperlink: http://www.ncbi.nlm.nih.gov/genbank/.
The datasets of clinical and biochemical reuslts supporting the conclusions of this article are included within the article.
Authors’ contributions
JM participated in the design of the study and acquisition of data, carried out the molecular genetic studies and biochemical analyses, performed the statistical analysis, analysis and interpretation of data, involved in drafting the manuscript. JV have made substantial contributions to the conception and design, acquisition of data, analysis and interpretation of data, involved in drafting the manuscript and its revision. MD, NT, DL and TA have made substantial contributions to the conception and design, acquisition of data, carried out the molecular genetic studies, and analysis and interpretation of data. TJS and DP substantial contributions to the analysis and interpretation of data, participated in performing biochemical analyses. VB and MM participated in the study design and coordination, and helped to draft and revise the manuscript. GK and AV substantial contributions to the analysis and interpretation of data, participated in performing biochemical analyses. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Milenković, J., Vojinović, J., Debeljak, M. et al. Distribution of MEFV gene mutations and R202Q polymorphism in the Serbian population and their influence on oxidative stress and clinical manifestations of inflammation. Pediatr Rheumatol 14, 39 (2016). https://doi.org/10.1186/s12969-016-0097-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12969-016-0097-1