
Abstract
Maintenance of internal homeostasis is a sophisticated process, during which almost all organs get involved. Liver plays a central role in metabolism and involves in endocrine, immunity, detoxification and storage, and therefore it communicates with distant organs through such mechanisms to regulate pathophysiological processes. Dysfunctional liver is often accompanied by pathological phenotypes of distant organs, including the eyes. Many reviews have focused on crosstalk between the liver and gut, the liver and brain, the liver and heart, the liver and kidney, but with no attention paid to the liver and eyes. In this review, we summarized intimate connections between the liver and the eyes from three aspects. Epidemiologically, we suggest liver-related, potential, protective and risk factors for typical eye disease as well as eye indicators connected with liver status. For molecular mechanism aspect, we elaborate their inter-organ crosstalk from metabolism (glucose, lipid, proteins, vitamin, and mineral), detoxification (ammonia and bilirubin), and immunity (complement and inflammation regulation) aspect. In clinical application part, we emphasize the latest advances in utilizing the liver-eye axis in disease diagnosis and therapy, involving artificial intelligence-deep learning-based novel diagnostic tools for detecting liver disease and adeno-associated viral vector-based gene therapy method for curing blinding eye disease. We aim to focus on and provide novel insights into liver and eyes communications and help resolve existed clinically significant issues.
Similar content being viewed by others


Introduction
Over the last decades, more and more researches have raised human understanding of interorgan connections to an unprecedented level, particularly in the fields of epidemiology, molecular biology, diagnostics, and therapeutics.
As the largest solid organ, the liver performs a number of essential bioactivities related to metabolism, immunity, endocrine, storage, and detoxification, implying its central role in systemic regulation. Meanwhile, this could become a double-edged sword, as liver dysfunction would disrupt homeostasis and significantly influence extrahepatic tissues, including the eyes [1]. From an ocular perspective, its unique anatomical structures have been utilized as a window to directly witness disease-related neurovascular changes, and the latest study further expands this application to detecting asymptomatic liver disease like fatty liver disease, viral hepatitis, and slight cirrhosis even at the initial stages [2]. Such timely identification plus interventions can significantly improve the disease prognosis [3]. However, currently published reviews about the liver or eye rarely focus on interorgan connections, which is far behind the increasing number of basic medical studies and clinical practices.
Therefore, finding out the underlying molecular pathways between the liver and the eyes, as well as their change rules, embodiment in the epidemiological/clinical relationship could help to deepen our insights into the occurrence/progression of liver-eye diseases, and subsequently into their diagnosis/treatment.
Epidemiological evidence and public health significance
An increasing number of epidemiological works indicate that eye disease has liver-related protective factors or risk factors and vice versa [4,5,6,7]. A timely identification of such factors would help health care workers better evaluate patients’ status and better identify high-risk groups of liver/eye disease patients that require a transfer to receive complete ophthalmic/hepatic examination, which is certainly beneficial to individual outcomes [8]. Besides, an early alert as well as intervention could significantly reduce disease burden for society [9], particularly in an era with an aging and growing population when blinding ophthalmic conditions and all types of liver diseases are becoming prevalent [9, 10].
Ophthalmopathy-related hepatic factors
Glaucoma is the main reason for irreversible blindness worldwide and is estimated to afflict more than 76 million people [11]. Elevated intraocular pressure (EIOP) is the only modifiable risk factor identified to date during the whole course [12]. Retrospective studies have indicated that mean IOP levels in Asian adults are positively and linearly increased with the nonalcoholic-fatty liver disease (NAFLD) grades [5], and therefore liver steatosis patients have elevated odds ratios (ORs) for high IOP (≥ 22 mmHg), which shows a linear dose-response relationship with the severity of fatty liver, including in patients with alcoholic liver disease [13, 14]. The cubic spline curve from another cross-sectional study indicates that there is an inverse dose-dependent relationship between ORs for EIOP and serum 25-hydroxyvitamin D3(25(OH)D) content, especially in subgroups < 20 ng/ml [15]. Given that more than 37% of the global population might suffer from NAFLD [16], up to 24% and 40% of the people, respectively, in the US and Europe are estimated to suffer from vitamin D deficiency [17], and nearly 9.5% of untreated EIOP patients would deteriorate into primary glaucoma over the next 5-year follow-up [18], physicians may well raise their alertness. In addition to EIOP, circumpapillary retinal nerve fiber layer thickness (cpRNFLT) thinning has been identified as one of the well-performed initial signs of glaucoma [19, 20]. The LIFE-Adult study also suggests categorizing adverse lipid profiles (e.g., high apolipoprotein B (ApoB), high non-HDL cholesterol, high total cholesterol, high low-density lipoprotein (LDL) cholesterol, low high-density lipoprotein (HDL) cholesterol) as independent covariates of thicker cpRNFLT, thus helping conceal nerve fiber decay in glaucoma, of which per 1 mmol/l increase in non-HDL cholesterol brings about 0.5 μm elevation in cpRNFLT [20]. Quantifying the impacts of adverse liver-lipid metabolism profiles matters to refining cpRNFLT-based early diagnosis of glaucoma. (Fig. 1).

Gluacoma-related hepatic factors. A The restricted cubic spline curve shows a linear dose-response relationship between ORs for EIOP and the severity of fatty liver. The red line indicates the estimated OR, and the dotted lines indicate the 95% CI. The purple areas indicate population density. ORs odds ratios, EIOP elevated intraocular pressure, CI confidence interval. p < 0.05 implies statistically significant. This graph is cited from the “Graphic abstract” in [11] without any adaptation, Lee, Jun-Hyuk et al., Fatty Liver Is an Independent Risk Factor for Elevated Intraocular Pressure. Nutrients. 2022; 14(21):4455, with the permission from the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/). B This cubic spline curve illustrates an inverse dose-response relationship between the plasma 25(OH)D levels and ORs of EIOP. 25(OH)D 25-hydroxyvitamin D3, ORs, odds ratios. This illustration is cited from Fig. 3 in [12] without any adaptation, Lee, Jun-Hyuk et al., Inverse Relationship between Serum 25-Hydroxyvitamin D and Elevated Intraocular Pressure. Nutrients. 20–23; 15(2):423, with permission from the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/). C A standardized β coefficients heatmap for multiple biomarkers with global and sectoral cpRNFLT. Multivariable linear regression analysis is carried out for each biomarker (independent variable) with corresponding global and sectoral cpRNFLT (dependent variable) with age, sex, and scanning circle radius adjustment. White (empty) squares are depicted for sectors that do not come to a valid corrected p value by the false-positive discovery rate method, while positive associations (red colored), and negative associations (blue colored) are shaded based on respective standardized β coefficients for those significant sectors. GGT, γ-glutamyl transferase, WHR, waist-to-hip ratio, HDL, high-density lipoprotein, ApoB, apolipoprotein B, Optic nerve head sectors: LDL, low-density lipoprotein, N, nasal sector, NI, infero-nasal sector, NS, supero-nasal sector, TI, infero-temporal sector, T, temporal sector, TS, supero-temporal sector, G, global sector. This heatmap is cited from Fig. 1 in [17] without any adaptation, Rauscher, F.G., Wang, M., Francke, M. et al. Renal function and lipid metabolism are major predictors of circumpapillary retinal nerve fiber layer thickness—the LIFE-Adult Study. BMC Med 19, 202 (2021), with permission under the Creative Commons International licence 4.0. (http://creativecommons.org/licenses/by/4.0/)
Age-related macular degeneration (AMD) is another leading cause of blindness in elderly people and shows a prominent genetic basis [21]. AMD patient cohort studies have demonstrated the positive correlation between high levels of serum Complement Factor H-related protein 4 (FHR-4) and the risk of AMD [4]. Such an increase in FHR-4 is related with locus variants, such as rs10922109 of Factor H (CFH), that can upregulate its liver expression level [22]. The Genome-Wide Association Study (GWAS) further indicates that hepatic lipase (LIPC) locus variants, especially rs10468017 of the promoter, are related to late AMD [23] (Fig. 2).

AMD-associated liver factor FHR-4. A Box plots show serum FHR-4 levels from two independent cohorts: Cambridge (214 controls and 304 advanced AMD cases) and EUGENDA (308 controls with 180 advanced cases). The geometric mean FHR-4 levels are: in Cambridge, 5.5 µg ml/l in controls and 6.6 µg ml/l in AMD cases; in EUGENDA, 6.0 µg ml/l in controls and 7.2 µg ml/l in cases. AMD patients have statistically increased FHR-4 levels compared to controls, and these differences still remain significant after sex, age, batch effects, and the first two genetic principal components adjustment (p = 0.018 and 8.4 × 10−5, for Cambridge and EUGENDA, respectively; Wald test). AMD age-related macular degeneration, FHR-4 Factor H-related protein 4. B A two-stage, fixed-effects meta-analysis of individual participants’ data from the Cambridge and EUGENDA study shows a significant association between FHR-4 levels and late AMD. Panel A shows forest plots of ORs with 95% CI of late AMD per SD change in natural logarithmically transformed FHR-4 levels using logistic regression models after sex, age, batch effects, and the first two genetic principal components adjustment. The overall OR estimate is obtained from a two-stage, fixed-effects, meta-analysis of the two study-specific estimates. I2 statistics is used to assess heterogeneity across studies. OR odds ratios, CI confidence intervals, SD standard deviation. A and B are respectively adapted from Fig. 1 and Fig. S1 in [16], Cipriani, V., Lorés-Motta, L., He, F. et al. Increased circulating levels of Factor H-Related Protein 4 are strongly associated with age-related macular degeneration. Nat Commun 11, 778 (2020), with authorization from the Creative Commons International licence 4.0 (http://creativecommons.org/licenses/by/4.0/)
Diabetic retinopathy (DR) is a very common and blinding complication of diabetes mellitus affecting more than 100 million individuals worldwide, which is accompanied by dyslipidemia normally [24, 25]. A cross-sectional research has validated that, for patients with type II diabetic mellitus (T2DM), those having a higher cholinesterase (CHE) level (> 10,500 U/L) are at a lower OR of DR at 0.498, while those with a lower total proteins level (< 60 g/L) have a higher OR at 1.624 [26]. Another 10-year prospective cohort study further indicates that plasma ApoA-I level (≥ 7.4 μmol/L) is correlated with a decreased hazard ratio (HR) of DR at 0.86, while serum ApoC-III (≥ 6.3 μmol/L) and ApoE levels (≥ 1.1 μmol/L) are correlated with a higher HR at about 1.2 [24]. Besides, serum lipoprotein(a) (≥ 30.5 mg/dL) is related with an adjusted incidence OR of DR at 3.46, while increased levels of ApoB (≥ 77.5 g/L) and fetuin-A (a major liver-derived glycoprotein) present a positive correlation with DR degree at an adjusted OR = 1.02 [27, 28]. Liver derived peptide adropin shows the opposite trend [1, 29]. NAFLD is related with proliferative/laser-treated DR at an adjusted OR = 1.75 [30]. Given that apolipoproteins could reflect liver functions and are not influenced by dietary status [24], taking fundus examination in T2DM patients who have the above-mentioned changes could help DR monitoring.
Patients with dry eye disease (DED) present with ocular surface inflammation and tear film homeostatic imbalance [31], at a prevalence rate ranging from 5% to 50% within different populations [32]. The Lifelines Cohort study demonstrates that liver cirrhosis and gallstone are independent risk factors of DED, with respective OR at 3.38 and 1.22 [33].
Ocular motor cranial nerve palsies (CNP) paralyze extra-ocular muscles and cause diplopia [34]. Data from National Health Insurance Service-National Sample Cohort (NSC) shows that adults with low HDL cholesterol, elevated triglyceride, and elevated alanine aminotransferase (ALT) contents have a higher hazard ratio (HR) for ocular motor CNP at 1.24, 1.18, and 1.141, respectively [6, 34]. Besides, an increase in the morbidity of ocular motor CNP is observed as the plasma level of liver γ-glutamyl transferase (GGT) increases, with the highest HR at 1.245 [6]. It is worth noting that palsies of the 3rd, 4th, and 6th cranial nerve are rather common in neuro-ophthalmology practice, and GGT is one of the most sensitive indicators for liver function changes [6]. Moreover, it has been found that hepatic cirrhosis patients are prone to smooth pursuit eye movements (SPEM) disruption [35].
Furthermore, NAFLD is identified as a risk factor (OR = 2.378) of vascular lesions, like arteriovenous compression and arterial narrowing in the retina [36]. AFP and CA-125 cut-off values at 957.2 ng/ml and 114.25 U/ml could serve as independent risk factors for predicting ocular metastasis of liver cancer with the separate value of area under the curve (AUC) at 0.739 and 0.810 [37]. However, the two indices may have limited reference value as they are also elevated upon liver carcinogenesis or systemic cancer metastasis [38, 39]. Recently, a Mendelian randomization case-control study reports that genetic variants within the CYP2R1 locus would reduce liver 25-hydroxylase activities and the resultant low blood levels of 25(OH)D are linked with increased non-infectious uveitis/scleritis risk at an OR = 6.42 [40]. Interestingly, excessive blood unbound bilirubin is suggested to be a protective factor in specific conditions, including in neonates to reduce the severity of retinopathy of prematurity (ROP) [41], and in patients with diabetic mellitus or impaired glucose tolerance to protect against DR [42].
Eye indicators connected with liver status
Similarly, some ocular examination indices can also alert or monitor liver diseases development, which matters to those asymptomatic or rapidly-progressing in the course.
Acute liver failure (ALF) refers to a rare but lethal condition that normally impacts individuals without preexisting liver diseases [8], accompanied by the rapid development of coagulopathy and hepatic encephalopathy secondary to the liver injuries [8]. Complex infectious (i.e., reactivation of chronic hepatitis B virus infection), pharmacological (i.e., acetaminophen), immunological (i.e., autoimmune hepatitis), along with genetic factors (i.e., acute presentations of Wilson disease) could lead to this condition [8]. The prognosis of ALF is correlated with the management of intracranial hypertension [(ICH), referring to constant intracranial pressure > 20 mm Hg] that may well rapidly progress to cerebral herniation and death [8, 43]. Conventional monitoring techniques for ICH, such as CT scan and intracranial catheter insertion, present great false-negative, bleeding and infectious risks [44, 45]. Continuous efforts have been made to develop novel non-invasive techniques for monitoring changes in intracranial pressure and identifying an elevation of it during therapy, timely and accurately [8]. Due to connected subarachnoid space around the optic nerve and the brain, elevated intracranial pressure could be transmitted to the perineural space through cerebrospinal fluid circulation [46], leading to an enlargement in optic nerve sheath diameter (ONSD) [44, 47]. Prior studies of traumatic brain injury-caused intracranial hypertension showed the credibility of measuring ONSD [48]. For its performance in ALF patients, a meta-analysis including 31 studies indicated a higher sensitivity (0.92 versus 0.70; p < 0.01) with an equal specificity in diagnosing elevated intracranial pressure by measuring ONSD using ocular ultrasonography (US) than magnetic resonance imaging (MRI) [49]. Recently, a prospective study performed in adult cohort with ALF reported an increase in median ONSD with hepatic encephalopathy grade [44]. A children ALF cohort also showed a similar trend and further defined thresholds for different stages of hepatic encephalopathy grade [47] (Table 1). These results demonstrated the potential of ONSD in predicting ALF-related prognosis; however, its performance in such small-scale cohorts requires further validation by more large-scale prospective studies [50].
Infection of hepatitis virus would lead to chronic hepatitis, cirrhosis, and even liver carcinoma, in which the hepatitis C virus (HCV) affects 2.2% of the global population [51], with DED being a common comorbidity. Studies have found that, compared to hepatitis C patients at initial 0–3 stages of cirrhosis, patients at more advanced 4–6 stages tend to have worse ocular surface indices, such as higher Ocular Surface Disease Index (OSDI), decreased Schirmer test I, lower tear-film breakup time, and worse conjunctival/corneal vital dye staining scores [52, 53]. In addition, chorioretinal structures of the eyes could serve as a noninvasive proxy of hepatic microvasculature due to correlations between reduced retinal thickness/macular volumes and increased cirrhosis severity irrelevant to primary etiologies [54]. Particularly, there is an inverse correlation between increased ganglion cell complex (GCC) thickness and Fibrosis-4 scores (a liver fibrosis risk index) when above the minimum cut-off value (score ≥ 2.67) in elderly people (defined as > 65 years old) [55].
NAFLD is estimated to take the place of the hepatitis B and C viruses as the driving cause of hepatocellular carcinoma (HCC) [7]. Data from a case-control work indicates that DR is an independent risk factor for HCC development (OR = 8.654) in patients having NAFLD, and these high-risk groups should therefore have regular HCC screening [7]. For children with NAFLD, liver fibrosis degrees and retinopathy sign severity (pathological grading for retinal arterial tortuosity) display a positive correlation (r = 0.31) [56].
The mutual epidemiological correlations between the liver and eyes were depicted in Fig. 3.

Created with Biorender.com
The liver-eye epidemiological correlation network. Common liver diseases listed (left) are linked with their epidemiologically correlated ocular pathologies (right). NAFLD is associated with glaucoma, diabetic retinopathy, and dry eye disease, whereas viral hepatitis and cirrhosis are linked with dry eye disease. In turn, diabetic retinopathy could elevate hepatocarcinoma risk in T2DM patients. NAFLD nonalcoholic fatty liver disease, EIOP elevated intraocular pressure, T2DM type II diabetic mellitus, OR odds ratio.
Molecular pathways and pathophysiological regulation
Substantial laboratory findings have revealed and supported an intimate biological connection between the liver and eyes under physiological and pathological conditions, despite their great anatomical distance. We summarized consistent molecular regulatory mechanisms and cross-talking pathways between the two organs (Figs. 4, 5).

Created with Biorender.com
The molecular liver-eye regulatory pathways under physiological settings. (Taken normal liver as an example.). LUT lutein, ZEA zeaxanthin, βc β-carotene, αc α-carotene, CFHR4 Factor H-related protein 4, 25(OH)D, 25-hydroxyvitamin D3, FA fatty acid, HDL high density lipoprotein, LDL low-density lipoprotein, EET epoxyeicosatrienoic acid, PEDF epithelium-derived factor, RE retinyl esters.

Created with Biorender.com
Underlying interorgan molecular pathways changes in pathological conditions. (Taken liver cirrhosis as an example.) RPE retinal pigment epithelium, TUDCA tauroursodeoxycholic acid, UDCA ursodeoxycholic acid, HGF hepatocyte growth factor, IGF insulin-like growth factor 1, LPS lipopolysaccharide, ER endoplasmic reticulum.
Consistent biological regulatory patterns of the liver and eyes
Normal retinal pigment epithelium (RPE) consists of a monolayer of melanin-rich epithelial cells located between choroids and photoreceptor (PR) outer segments, which works with PR to sustain visual cycles [57]. Epithelial-mesenchymal transformation (EMT) transforms RPE cells to de-differentiated mesenchymal phenotypes (loss of apical-basal cell polarity, dysregulated cell proliferation and migration, and blindness correlation) [58]. In vitro, RPE cells originated from human induced pluripotent stem cells (hiPSC-RPE) show the enrichment of liver tumor/carcinoma/carcer tox functions-related proteins and phosphosites alterations as well as sharing commonality with hepatocyte proliferation-initial stages of liver malignancy-related pathways [57,58,59]. Overall, the highest enrichment of hepatocyte growth factor-cellular-mesenchymal to epithelial transition factor (HGF-MET) signaling pathway has been detected, which could regulate EMT transcriptional profiles [57].
Besides, the retina is as metabolically active as the liver parenchyma in the protein synthesis and such an anabolic pattern can be attributed to constant insulin receptor and Akt-1 kinase activities comparable to those of the postprandial liver [60]. In addition, RPE cells have been found to express as high levels of ketogenesis and fatty acid oxidation-related mitochondrial HMG-CoA synthase 2 (Hmgcs2) to generate β-hydroxybutyrate through fatty acid oxidation for energy supply as hepatocytes do [57, 61, 62].
Glucose metabolism
Liver plays a central role in blood glucose homeostasis, as it involves in regulating multiple pathways of glucose metabolism, including glycogenolysis, gluconeogenesis, glycogenesis, and glycolysis [63]. Besides, the liver could regulate insulin efficacy through removing 50% of secreted insulin in peripheral circulation, inhibiting hyperinsulinemia induced insulin resistance in adipose/muscle tissues [64, 65]. Liver glucose supply matches whole-body glucose demand (80–90% of endogenous glucose production derived from the liver under postabsorptive condition) [66], and a relatively stable level of blood glucose is the major energy source for normal retina metabolism [67].
In acute or chronic liver disease, hepatocytes could not respond to insulin signaling in a physiological way and resultant dysregulated glycogenolysis, gluconeogenesis, and lipogenesis promote hyperglycemia, systemic insulin resistance and eventually causing elevated risk of T2DM, of which NAFLD is the most prevalent type and lead to a nearly two-fold increased risk [68, 69]. Lipid intermediates accumulation in liver impairs its ability of insulin clearance and induces hepatic insulin resistance as well as gluconeogenesis [69].
Blood glucose in the hyperglycemic condition enters the polyol pathway and is reduced to sorbitol by aldose reductase in the eye lens, causing apoptosis and eventually cataract [70, 71]. Besides, hyperglycemia can result in abnormal metabolism in vascular endothelial cells of the eyes to impair them, and an activated pro-inflammatory phenotype of retinal microglia, Müller cells, and migrated circulating leukocytes in retinal microcirculation,
which collectively cause vascular bed dysfunction and chronic regional inflammation [72, 73]. Recently, it has also been found that high levels of blood glucose could cause injuries directly on neuronal cells (neuroretina), even prior to the breakdown of the blood-retinal barrier (BRB), to promote neurodegeneration, neuronal cell death, and eventually DR [74].
Furthermore, insulin resistance and hyperglycemia stimulate sympathetic nerve activity as well as trabecular meshwork cell excessive synthesis of extracellular matrix to cause increased IOP [75, 76]. Apart from hyperglycemia-related toxicity, some secreted molecules might also play a role in communications between the liver and the eyes. In infants with ROP, increased incidence and severity of this illness may be due to subdued endogenous insulin signaling-induced liver insulin-like growth factor 1 (IGF1) reduction and use of IGF1 exerts significant inhibition on pathological neovascularization and improvement of physiologic retinal revascularization [77]. Likewise, fibroblast growth factor-21 (FGF-21) is another regulatory factor primarily excreted by hepatocytes, of which the level is decreased in T2DM patients [78]. Supplementation of FGF-21 has shown inhibitive effects on retinal neovascularization in mice mimicking hypoxia-caused neovascularization in DR [79,80,81].
Amino acid and protein metabolism
Liver metabolized amino acids and proteins impose impacts on the eyes under both physiologic and pathologic scenarios. Taurine is a sulfur-containing amino acid residing and functioning throughout the retinal layers particularly in the RPE and PR cells [82], and its deficiency leads to PR degeneration and retinal ganglion cell loss [83]. It has been found that taurine in the retina is primarily synthesized from liver glycolysis-derived 1-carbon than from that of retinal glycolysis, under the control of liver HIF-1α stabilization [84, 85].
Ornithine aminotransferase (OAT) is an enzyme predominantly expressed by liver cells, and involves in the catabolism of ornithine to proline precursors [86]. Its deficiency causes hyperornithinemia at 10–20 folds of the normal levels, and the cytotoxicity of excessive free ornithine would cause gyrate atrophy of the choroid and retina [87].
Besides, newly synthesized retinol-binding protein 4 (RBP4) could bind with and then transfer retinol in serum, while the deficiency causes immobilized liver storage, reduced serum levels of retinol, and a disrupted visual cycle [88, 89], its excess could also impair retina via microglia and IL-18-mediated inflammation in mice models [90, 91]. RBPR2 is a liver-specific receptor for the RBP4-retinol complex, which mediates the liver and systemic circulation retinol cycle [92]. The RBPR2−/− mice model exhibits reduced liver storage and ocular supplies of retinoids, as well as a significant loss of visual ability [92]. Liver Kupffer cells are the main source of HGF, and this cytokine could bind with its receptors to sustain the structural and functional integrity of corneal/lens epithelial cells, ganglion cells, and RPE cells [93, 94], as well as hyperactivate the MET receptors overexpressed by uveal melanoma (UM) cells to facilitate metastasis and therapy resistance [95]. Furthermore, ABCC6 is an organic substrate transporter expressed exclusively by hepatocytes, while its pathogenic mutation might alter liver secretion of anti-mineralization/anti-calcification proteins, like fetuin-A and Gla proteins, and cause eye mineralization in pseudoxanthoma elasticum (PXE) [96]. Reduced albumin generation by the liver results in low intravenous oncotic pressure that induces retinal soft exudates extravasation [97].
In turn, retinal pigment epithelium-derived factors (PEDF) excreted by RPE could act on the liver [98]. It has shown systemic impacts on inhibiting the Wnt coreceptors, low-density lipoprotein receptor-related protein 6 (LRP6) and steatohepatitis severity [99, 100].
Fatty acid, cholesterol, and bile acid metabolism
The liver participates in systemic metabolism and circulation of lipids to modulate ocular pathophysiological bioactivities. As long ago as in 1980s, the liver was found to convert 18:3 omega-3 fatty acid to 22:6 omega-3 fatty acid, and then this docosahexaenoic acid was transported in secreted lipoproteins to the developing retina to synthesize membrane phospholipids [101, 102]. Also, the liver cytochrome P450 epoxygenase-derived epoxyeicosatrienoic acid (EET) exerts an inhibitive effect on eye inflammation [103]. As to cholesterol, RPE contains an HDL-based active reverse transport system that could return excessive peripheral cholesterol to the liver [104]. The primary bile acids (BAs) are liver metabolites of cholesterol, which contribute to the absorption of vitamin A and dietary fat, and they undergo deconjugation and dehydroxylation to secondary BAs (i.e., deoxycholic acid [DCA] and lithocholic acid [LCA]) in the distal part of small intestine and colon [105]. This conversion is partially mediated by the modification of gut bacteria [106].
In NAFLD patients, however, the abundance of the bacteria responsible for conversion is decreased, which leads to decreased stimulation of BAs receptors by secondary BAs and further intestinal microbial disturbance [107]. Reshaping intestinal microbiome is accompanied by altered levels of secondary BAs [108]. The ursodeoxycholic acid (UDCA) and tauroursodeoxycholic acid (TUDCA) of the secondary BAs exert neuroprotective impacts on retinopathies mainly via activating the TGR5-mediated pathway [109].
Provitamins, vitamins, and their derivatives metabolism
Carotenoids refer to a group of natural, orange/yellow/red color, lipophilic, natural pigments, in which the Provitamin A subtype (β-carotene, α-carotene), and retinyl esters (RE) are absorbed and transported to the liver, where they are partially stored in liver stellate cells as RE (retinyl palmitate and retinyl stearate) or converted to all-trans retinol which binds with RBP4 to be secreted into the bloodstream [110]. Meanwhile, the rest of the unprocessed carotenoids (lutein, zeaxanthin, and β-carotene) are integrated into LDL and HDL to be returned into the circulation [111]. In RPE cells, retinol is transformed to 11-cis retinol, the precursor of 11-cis retinaldehyde by RPE65, which constitutes rhodopsin with opsin to retain the photosensitivity of rod cells [111]. Meanwhile, circulated zeaxanthin and lutein are utilized by the retinal macula to filter harmful blue light as well as to repress singlet oxygen species-caused oxidative stress [112], in which HDL (specifically ApoA-I) answers for such courier [113]. Furthermore, vitamin A is transformed to its active derivative retinoic acid on ocular surface, which activates the retinoic acid receptor (RAR) and retinoid X receptor (RXR) to ensure normal differentiation and mucus secretion of corneal and conjunctival epithelial cells [114, 115]. Interestingly, misfolded rhodopsin can cause retinal oxidative stress that in turn undermines hepatic antioxidative defense in P23H transgenic rats mimicking retinitis pigmentosa (RP), potentially through damaging the melanopsin system that causes circadian desynchronization or certain retina-derived, liver-directed molecules [116].
Besides, the liver is an important organ for synthesizing B vitamins, including folic acid [117], which could protect retinal ganglion cells from death in glaucoma and prevent retinal microvascular endothelial cell from DNA methylation/hydroxy-methylation impairment in DR [118,119,120].
In addition, vitamin D activation undergoes two rounds of hydroxylation, of which the first step of hydroxylation to 25(OH)D is catalyzed by CYP2R1 in the liver [121, 122]. Patients with hepatic diseases are largely accompanied by reduced liver CYP2R1 activities and thus lower blood vitamin D levels [1, 123], so does those with genetical variants within the CYP2R1 locus [40].
Mineral metabolism
The systemic homeostasis of human-required minerals, like iron, copper, and zinc, highly depends on the normal liver function, while liver disease can impair such balance and impose great impacts on eye functions [124]. Iron is abundant in the retina and indispensable for essential biochemical activities, while an excessive intracellular load of it could cause oxidative stress and ferroptosis [125]. Hepcidin (Hepc) is the key hormone for reducing the blood concentration of iron, which is primarily synthesized by the liver and functions through antagonizing the only known. iron exporter ferroportin (Fpn) in human to inhibit intestinal absorption and liver release of the iron [126]. Although the retina has a regional regulatory mechanism by synthesizing Hepc just like hepatocytes do, transgenic mice model indicates that liver-specific rather than retina-specific absence of Hepc leads to increased blood and retinal free iron levels that enable subsequent hypertrophy of RPE and degeneration of PR cells [127]. Zinc is the second most prevalent essential trace element in vivo [128], with its content being particularly high in ocular tissues (with the highest level in the retina-choroid) [129]. Zinc is indispensable for many essential physiological processes of the retina, including regulating rhodopsin stabilization and retinol metabolism, while its systemic deficiency may lead to retinitis pigmentosa as well as abnormal visual dark adaptation [129, 130]. It has been reported that alcoholic/viral liver disease could result in zinc deficiency in patients along with corresponding ocular manifestations [128].
Hepatolenticular degeneration is an inborn defect of copper metabolism caused by pathological mutation of the transmembrane copper-transporter ATPase gene ATP7B [131]. The generated dysfunctional ATP7B copper transporters could result in impaired biliary copper excretion, and the resultant excessive deposition of copper in ocular tissues leads to corneal pigment ring (the Kayser-Fleischer ring), nystagmus, or sunflower cataract [132].
Detoxification of ammonia and bilirubin
Cell metabolism bioactivities in vivo, like amino acid deamination/transamination, purine/pyrimidine decomposition, and urea degradation by gut microbiota, can produce nearly 1000 mmol of ammonia per day, of which the majority is converted by the liver. to urea and then removed in the form of urine to sustain a normal plasma level (in adult, < 50 μm; in neonate, < 150 μm) [133]. Besides, liver converting glutamate into glutamine by glutamine synthetase and amino may well represent another equally important pathway of removing ammonia [134]. Liver disease could disrupt these processes and then resultant. high plasma ammonia (0.2-1 mM) could obstacle the citric acid cycle and mitochondrial respiratory chain, causing great toxicities to retinal Müller cells (vacuolization, swelling, and even necrosis) as well as to optic nerves [135,136,137]. The nitrogen metabolism patterns of retina that primarily rely on glutamine synthesis to remove ammonia make it vulnerable to ammonia toxicity [133].
Similarly, liver disease undermines the clearance ability of hepatocytes of unbound bilirubin from the blood and the resultant high plasma levels of such a potent neurotoxin could bind with and yellow the conjunctiva (one of the most visible manifestations) and cause retinopathy [138], potentially by affecting transporters of the blood-retina barrier [139,140,141]. In addition to the cytotoxicity to eye tissues, hyperbilirubinemia could cause injuries to visual cortex and impair visual acuity (called hepatic cortical blindness) [142]. However, the negative effect of unbound bilirubin on eye health is not always definite, as its potent antioxidative property may exert protective effects upon specific conditions mentioned before [42, 143].
Immunity regulation
Liver is the major production pool of complements [144], and its synthesized complement factor H (CFH) prevents the alternative pathway of complement activation, and membrane attack complex formation/deposition in choroidal neovascularization [145].
Besides, the RNA sequencing has indicated that in vivo the only source of FHR-4 is the liver and that FHR-4 accumulation in the choriocapillaris can stimulate the complement system and recruit circulating immune cells to exacerbate inflammation [146] (Fig. 6).

FHR-4 accumulated in the choriocapillaris could inhibit C3b breakdown. A The diagram illustrates the anatomical structures of the macula, including the RPE, the underlying BrM, and the intercapillary septa within the choriocapillaris. Basement membranes are shown in black lines. Drusen is the hallmark lesion of early AMD that forms in the BrM underneath the RPE basement membrane. RPE retinal pigment epithelium, BrM Bruch’s membrane, AMD age-related macular degeneration. B FHR-4 prevents FHL-1 from acting as a cofactor for factor I and results in C3 convertase formation and subsequent activation of the amplification loop of complement and inflammation. FHR-4, Factor H related protein 4, FHL-1, FH-like 1. A and B are adapted from Fig. 2a and Fig. 2j in [16], Cipriani, V., Lorés-Motta, L., He, F. et al., Increased circulating levels of Factor H-Related Protein 4 are strongly associated with age-related macular degeneration. Nat Commun 11, 778 (2020), with authorization from the Creative Commons International licence 4.0. (http://creativecommons.org/licenses/by/4.0/)
Besides, liver dysfunction leads to increased intestinal permeability, gut bacterial translocation, as well as serum LPS and various pathogen-associated pattern molecules (PAMPs) levels, which promotes the secretion of pro-inflammatory cytokines TNF-α and IL-6 by adipose tissues [147]. Such elevated release of pathogenic mediators has been linked with retinopathy by activating microglia infiltration through pattern recognition receptors (PRRs) [30, 148]. Likewise, fetuin-A is a glycoprotein predominantly synthesized and secreted from the liver that enhances the secretion of proinflammatory cytokines in adipose tissue as well, while NAFLD patients have elevated serum levels of it [149].
Other modulatory pathways
Melanocyte-derived exosomes obtained from hepatic circulation of UM patients with liver metastases contained microRNAs (miRNAs), of which the upregulated miR-454, let-7b, and miR-21 are involved in regulating liver stellate cell activation [150,151,152].
Excessive estrogen due to liver dysfunction might protect the eyes by alleviating PR cell apoptosis in RP mice through the classic estrogen receptors (ERs)-mediated N-myc Downstream Regulated Gene 2 expression routine [153], by protecting retinal astrocytes along with ganglion cells from endoplasmic reticulum stress via activating G-protein-coupled ER in ROP [154, 155], by inhibiting Caspase-3 activation and tau protein dephosphorylation to protect astrocytes from oxidative stress [156], and by modulating the mitochondrial pathway to reduce high-glucose caused retinal ganglion cell damages [157].
In addition, the gut (including intestinal microbiota and their products) could be mediators of liver-eye communication, as liver diseases regulate their homeostasis, which is intimately correlated with ocular pathogenesis [158]. It has been found that valeric acid, a gut microbiota metabolite, could penetrate to the eyes and sustain homeostasis of IOP, while NAFLD patients were less abundant in valerate [159, 160]. Besides, decreased butyrate production is found in NAFLD [161], while butyrate has shown protective effects on ocular surface inflammation [162], DR [163], and intraocular bacterial infection [164]. Moreover, activating the aryl hydrocarbon receptor (AHR) and its involved signals is associated with the protection of RPE cells and the retina, as well as the inhibition of choroidal neovascularization, uveitis, and AMD [165]. NAFLD-related dysbiosis has been proven to cause decreased indole and its derivatives production, while these factors are endogenous ligands of AHR [165, 166].
Clinical links and practical applications
Diagnostic techniques
Visible alterations in eye manifestations can help clinicians to timely diagnose and deal with liver-related health issues, like Kayser-Fleischer ring implying Wilson disease, sclera icterus reflecting jaundice, xanthelasma palpebra indicating hepatic steatosis, and spontaneous subconjunctival/vitreous/retinal hemorrhage referring to hepatic failure [1, 2].
Besides, clinical statistics could provide clues for relatively hidden illnesses, for nearly 50% of cases of gram-negative endogenous endophthalmitis (EBE) originate from liver abscesses [167], and patients with orthotopic liver transplants are susceptible to Aspergillus endophthalmitis with eyes being the second most common site of infection only to lung [168]. In addition, nearly half of UM patients develop metastases, with the liver being the most preferential site [95, 169]. Nevertheless, the non-specificity and non-sensitivity of such summarized clinical features undermine their value as independent diagnosis index [2, 170].
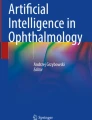
In recent years, the video electro-oculography (VOG) technique designed for early detection of dysfunctional cognitive/motor abilities in Parkinson’s, Alzheimer’s disease or multiple sclerosis has also been tested in diagnosing minimal hepatic encephalopathy (MHE), the earliest form of hepatic encephalopathy commonly found in liver cirrhosis patients [35, 171,172,173]. The results showed that MHE patients have longer latencies and worse performance in most eye movement tests, of which the latency of reflexive saccades in vertical antisaccades test and the vertical version of the memory-guided saccades test [35]. The underlying mechanism relates to impaired mental processing speed and attention [35]. In addition, artificial intelligence (AI)-based deep-learning (DL) algorithm has evolved rapidly in medical imaging-processing by automatically analyzing input graphs and coming to diagnosis data [174, 175]. This technology has been validated in image-centered ophthalmology to detect glaucoma, multiple retinopathies (including ROP, AMD, DR, and diabetic macular edema) [176,177,178,179,180]. The latest study adopts the ResNet-101 deep neural network to establish both slit-lamp and fundus images-trained DL models, in which the slit-lamp model performs well in detecting liver cirrhosis and cancer, while both models work relatively weaker in predicting cholelithiasis, NAFLD, viral hepatitis, and hepatic cysts [2]. Interpretation of working principles indicates that the structure of the iris, conjunctiva, sclera, and fundus contains diagnostic information identifiable to AI-DL models (Fig. 7) [2].

The schemes for constructing the AI-DL-based liver disease diagnosis models. A Collection of liver disease examination results, slit-lamp, and retinal fundus images. B Slit-lamp images and retinal fundus images are categorized to train DL algorithm-based models for identifying liver disease separately C Competitions between human clinicians and AI-DL models, involving three ophthalmologists, and three hepatobiliary surgeons. AI artificial intelligence, DL deep learning. Reprinted from [2], Xiao W, Huang X, Wang JH, et al. Screening and identifying hepatobiliary diseases through deep learning using ocular images: a prospective, multicentre study. Lancet Digit Health. 2021; 3(2): e88–e97 without any adaption, Copyright (2021), with permission from Elsevier under the Creative Commons (CC-BY-NC-ND 4.0) license (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Therapeutic strategies
In addition to diagnosis, hepatic and eye diseases also exhibit intimate associations in therapy, indicating that targeting at the liver could help treat ocular abnormalities and vice versa (Fig. 8).

All pictures are created with BioRender.com
Intimately correlated therapeutic pathways. A The schemes of using eye-directed bright-light therapy against pruritus via restoring circadian arrhythmia-related endogenous opioid dysregulation. The light density is 10,000 LUX, with the frequency at 60 min each time, bid. B Long-acting FGF-21 could counteract increased VEGF-induced retinal vascular leakages in DR via increasing inter-endothelial tight junction protein Claudin-1 expression levels. FGF-21 can inhibit retinal neovascularization and inflammation via an adiponectin-dependent way in AMD murine models. FGF-21 fibroblast growth factor-21, VEGF vascular endothelial growth factor, AMD age-related macular degeneration, DR diabetic retinopathy. C OAT-carrying AAV8 vectors are administered through intravenous retro-orbital plexus injections to restore liver OAT levels. Restored liver OAT activity can reduce serum ornithine levels to treat choroidal and retinal gyrate atrophy. AAV8 adeno-associated virus serotype 8, OAT ornithine aminotransferase.
Pruritus is an agonizing complaint frequently from patients with cholestatic liver diseases, such as primary biliary cirrhosis and primary sclerosing cholangitis. A clinical trial has validated the amelioration effects of bright-light therapy (BLT) on hepatogenic pruritus, potentially via restoring circadian rhythms through retino-thalamic pathway [181, 182]. For liver abscess-induced EBE treatment, early surgical resection of primary lesions and administration of antibiotics are essential for recurrent patients [183]. In addition, liver transplantation could restore disrupted electroretinogram and blue-yellow defects in the eyesight of patients with grievous liver failure [115]. The administration of FGF-21 could prevent retinal or choroidal neovascularization and regional TNF-α expression through upregulating adiponectin in circulation as well as retina in neovascular AMD models [80].
Also, the use of IGF1 holds potential for preventing ROP, as previously referred [77]. In recent years, emerging gene therapy has given hope of potential cure for various diseases, of which the eye is a prime target [184]. In current studies, adeno-associated viral vectors (AAVs) have been the priority vectors of choice and their common hepatotropic properties enable effective gene transfer towards hepatocytes to restore their generation of deficient proteins [184, 185]. For OAT (EC 2.6.1.13) deficiency, current therapy strategies of reducing plasma ornithine levels by arginine-restricted and vitamin B6-enriched diet merely slow but not prevent gyrate atrophy of the choroid and retina [86]. Using serotype 8 AAV (AAV8) vector, a preclinical work suggested that restoration of a minimum 10% of liver specific OAT activity could reach a persistent decrease in serum ornithine levels as well as a significant inhibition of retinal degeneration [87, 186]. Likewise, using antisense targeting at liver CFHR4 synthesis might become promising for AMD treatment [187]. In addition to the gene transfer technology, herbal medicinal components show therapeutic potentials as well [188]. The Traditional Chinese Medicine (TCM) adopts principles: “clear liver heat to enhance eyesight”, “liver blood deficiency inducing myopia”, and “nourish liver-yin to improve visual function” to guide eye disease therapy, and TCM physicians therefore prescribe black or brown bear bile (containing the major effective component TUDCA), medicinal herbs like wolfberry (containing lycium barbarum polysaccharide), aloe vera (containing aloin), acupuncture, or compound preparations (Qiming granules) to ease eye discomforts complicated with “liver depression” [135, 189,190,191,192]. Nevertheless, a prospective study of T2DM patients using glucagon-like receptor-I agonists calls for more attention paid on potential side effects of therapeutic strategies, as a protective effect on liver steatosis of NASH was found with aggravated retinopathy simultaneously [71]. Current and future treatments for liver diseases should guarantee that they would not worsen ophthalmopathy (if existed) and vice versa [193].
Conclusions
This review tries to preliminarily link two anatomically and functionally irrelevant organs together individually from the epidemiological, mechanical, and clinical aspects.
Particularly, it is worth noting that various pathways might cooperate with or counteract each other, like hepatic saturation of free fatty acid could elevate iron stores, which then amplifies T2DM-related retinal pericyte loss [64]. Also, the COVID-19 pandemic-caused mandatory lockdown further stressed the necessity of combining AI-DL-based models with 5G-based Cloudy medicine to remotely screen for disease in a noninvasive as well as convenient manner [2, 194].
Regarding liver-eye interactions, there are still certain unsolved problems worth further exploration. In terms of the epidemiological aspect, current work tends to simply show changes in disease severity or prevalence rates rather than calculate the precise thresholds of liver disease indices alterations enabling to predict the occurrence or stages of ophthalmopathy or those of ocular indices enabling to judge hepatic status. Therefore, further research may well adopt larger patient-cohorts to confirm potential correlations and provide references for public health policymaking. As to the molecular mechanisms field, functions of liver/eyes-specific molecules on targets, along with their space–time regulatory/transporting mechanisms under both pathological/physiological situations, remain to be clarified, particularly for those with regional regulatory systems in the eyes or those with ectopic expression, such as leucine-rich α-2 glycoprotein 1 (LRG-1), a constitutive liver protein that is also strongly expressed by eyes in pathological situations [195]. Besides, feedback signals from target organs and their reciprocation with primary organs/signals are still unknown, like how the eye signals to the liver to modulate its vitamin A store release when concentrations of retinoid are low. In clinics, TCM theories and therapies-entailed scientific foundation could help researchers focus on the liver-eye axis from a holistic view and should receive more attention, but the liver toxicity of ethnomedicine requires extra attention [196]. Meanwhile, current AI-DL models are still suboptimal in milder liver disease detection and clinical utility, but their relatively-high sensitivity in identifying early-stage liver pathologies still holds promise for becoming a diagnostic tool. All in all, more studies focusing on liver-eye interorgan communications would enhance our understanding of their underlying molecular regulatory pathways and help us to develop rational early detective/therapeutic methods to reduce disease burden and improve clinical prognosis.
Availability of data and materials
All data/graphs adopted are available from corresponding authors upon proper request.
References
Wang F, So KF, Xiao J, et al. Organ–organ communication: the liver’s perspective. Theranostics. 2021;11:3317–30.
Xiao W, Huang X, Wang JH, et al. Screening and identifying hepatobiliary diseases through deep learning using ocular images: a prospective, multicentre study. Lancet Digit Health. 2021;3:e88–97.
Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, Harrison SA, Brunt EM, Sanyal AJ. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American association for the study of liver diseases. Clin Liver Dis. 2018;11:81.
Cipriani V, Lorés-Motta L, He F, et al. Increased circulating levels of Factor H-Related Protein 4 are strongly associated with age-related macular degeneration. Nat Commun. 2020;11:778.
Kwon YJ, Kim JH, Jung DH. Association between nonalcoholic fatty liver disease and intraocular pressure in Korean adults. J Glaucoma. 2018;27:1099–104.
Kim J, Han K, Yoo J, et al. Liver enzymes and risk of ocular motor cranial nerve palsy: a nationwide population-based study. Neurol Sci. 2022;43:3395–405.
Azuma S, Asahina Y, Kakinuma S, et al. Diabetic retinopathy as a risk factor associated with the development of hepatocellular carcinoma in nonalcoholic fatty liver disease. Dig Dis. 2019;37:247–54.
Vasques F, Cavazza A, Bernal W. Acute liver failure. Curr Opin Crit Care. 2022;28:198–207.
Bourne R, Steinmetz JD, Flaxman S, Briant PS, Taylor HR, Resnikoff S, Casson RJ, Abdoli A, Abu-Gharbieh E, Afshin A, Ahmadieh H. Trends in prevalence of blindness and distance and near vision impairment over 30 years: an analysis for the global burden of disease study. Lancet Glob Health. 2021;9:e130–43.
Pimpin L, Cortez-Pinto H, Negro F, et al. Burden of liver disease in Europe: epidemiology and analysis of risk factors to identify prevention policies. J Hepatol. 2018;69:718–35.
Tham YC, Li X, Wong TY, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121:2081–90.
Stein JD, Khawaja AP, Weizer JS. Glaucoma in adults-screening, diagnosis, and management: a review. JAMA. 2021;325:164–74.
Chen YJ, Chen JT, Tai MC, et al. Examining the associations among intraocular pressure, hepatic steatosis, and anthropometric parameters. Medicine. 2019;98:e17598.
Lee JH, Kwon YJ, Lee HS, et al. Fatty liver is an independent risk factor for elevated intraocular pressure. Nutrients. 2022;14(21):4455.
Lee JH, Kwon YJ, Lee HS, et al. Inverse Relationship between serum 25-hydroxyvitamin D and elevated intraocular pressure. Nutrients. 2023;15(2):423.
Le MH, Yeo YH, Li X, et al. 2019 Global NAFLD prevalence: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2022;20:2809-2817.e28.
Amrein K, Scherkl M, Hoffmann M, et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. 2020;74:1498–513.
Gordon MO, Kass MA. What we have learned from the ocular hypertension treatment study. Am J Ophthalmol. 2018;189:xxiv–xxvii.
Zangalli CS, Jammal AA, Reis ASC, et al. Minimum rim width and peripapillary retinal nerve fiber layer thickness for diagnosing early to moderate glaucoma. J Glaucoma. 2022;32(6):526–32.
Rauscher FG, Wang M, Francke M, et al. Renal function and lipid metabolism are major predictors of circumpapillary retinal nerve fiber layer thickness-the LIFE-adult study. BMC Med. 2021;19:202.
Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2:e106–16.
Strunz T, Grassmann F, Gayán J, et al. A mega-analysis of expression quantitative trait loci (eQTL) provides insight into the regulatory architecture of gene expression variation in liver. Sci Rep. 2018;8:5865.
Neale BM, Fagerness J, Reynolds R, et al. Genome-wide association study of advanced age-related macular degeneration identifies a role of the hepatic lipase gene (LIPC). Proc Natl Acad Sci U S A. 2010;107:7395–400.
Zhang Q, Hu J, Hu Y, et al. Relationship between serum apolipoproteins levels and retinopathy risk in subjects with type 2 diabetes mellitus. Acta Diabetol. 2018;55:681–9.
Tan TE, Wong TY. Diabetic retinopathy: looking forward to 2030. Front Endocrinol. 2022;13:1077669.
Yao X, Pei X, Fan S, et al. Relationship between renal and liver function with diabetic retinopathy in patients with type 2 diabetes mellitus: a study based on cross-sectional data. Sci Rep. 2022;12:9363.
Moosaie F, Davatgari RM, Firouzabadi FD, et al. Lipoprotein(a) and apolipoproteins as predictors for diabetic retinopathy and its severity in adults with type 2 diabetes: a case-cohort study. Can J Diabetes. 2020;44:414–21.
Yilmaz A, Yilmaz T, Gunay M. Elevated serum fetuin-A levels are associated with grades of retinopathy in type 2 diabetic patients. Int Ophthalmol. 2018;38:2445–50.
Li S, Sun J, Hu W, et al. The association of serum and vitreous adropin concentrations with diabetic retinopathy. Ann Clin Biochem. 2019;56:253–8.
Targher G, Bertolini L, Rodella S, et al. Non-alcoholic fatty liver disease is independently associated with an increased prevalence of chronic kidney disease and proliferative/laser-treated retinopathy in type 2 diabetic patients. Diabetologia. 2008;51:444–50.
Sheppard J, Shen Lee B, Periman LM. Dry eye disease: identification and therapeutic strategies for primary care clinicians and clinical specialists. Ann Med. 2023;55:241–52.
Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocul Surf. 2017;15:334–65.
Vehof J, Snieder H, Jansonius N, et al. Prevalence and risk factors of dry eye in 79,866 participants of the population-based Lifelines cohort study in the Netherlands. Ocul Surf. 2021;19:83–93.
Choi DD, Han K, Oh SY, et al. Association between metabolic syndrome and incidence of ocular motor nerve palsy. Sci Rep. 2021;11:23033.
Casanova-Ferrer F, García-Cena CE, Gallego JJ, et al. Minimal hepatic encephalopathy is associated to alterations in eye movements. Sci Rep. 2022;12:16837.
Yang W, Xu H, Yu X, et al. Association between retinal artery lesions and nonalcoholic fatty liver disease. Hepatol Int. 2015;9:278–82.
Tang J, Zhang LJ, Kang M, et al. AFP and CA-125 as an accurate risk factor to predict eye metastasis in hypertension patients with liver carcinoma: a STROBE-compliant article. Front Genet. 2022;13:1010903.
Hu X, Chen R, Wei Q, et al. The landscape of alpha fetoprotein in hepatocellular carcinoma: Where are we? Int J Biol Sci. 2022;18:536–51.
Lopez JB, Balasegaram M, Thambyrajah V. Serum CA 125 as a marker of hepatocellular carcinoma. Int J Biol Markers. 1996;11:178–82.
Susarla G, Chan W, Li A, et al. Mendelian randomization shows a causal effect of low Vitamin D on non-infectious uveitis and scleritis risk. Am J Ophthalmol. 2022;244:11–8.
Boskabadi H, Shoeibi N, Bagheri F, et al. Potential role of bilirubin in preventing retinopathy of prematurity. Curr Pediatr Rev. 2023;19:197–202.
Yasuda M, Kiyohara Y, Wang JJ, et al. High serum bilirubin levels and diabetic retinopathy: the Hisayama Study. Ophthalmology. 2011;118:1423–8.
Sheikh MF, Unni N, Agarwal B. Neurological monitoring in acute liver failure. J Clin Exp Hepatol. 2018;8:441–7.
Cardoso FS, Pereira R, Moreno R, et al. Optic nerve sheath diameter in acute liver failure: a prospective cohort study. GE Port J Gastroenterol. 2021;28:170–8.
Karvellas CJ, Fix OK, Battenhouse H, et al. Outcomes and complications of intracranial pressure monitoring in acute liver failure: a retrospective cohort study. Crit Care Med. 2014;42:1157–67.
Hansen HC, Helmke K. Validation of the optic nerve sheath response to changing cerebrospinal fluid pressure: ultrasound findings during intrathecal infusion tests. J Neurosurg. 1997;87:34–40.
Das MC, Srivastava A, Yadav RK, et al. Optic nerve sheath diameter in children with acute liver failure: a prospective observational pilot study. Liver Int. 2020;40:428–36.
del Saz-Saucedo P, Redondo-González O, Mateu-Mateu Á, et al. Sonographic assessment of the optic nerve sheath diameter in the diagnosis of idiopathic intracranial hypertension. J Neurol Sci. 2016;361:122–7.
Xu N, Zhu Q. Optic nerve sheath diameter measured by ultrasonography versus Magnetic Resonance Imaging for diagnosing increased intracranial pressure: a systematic review and meta-analysis. Med Ultrason. 2023. https://doi.org/10.11152/mu-4037.
Rajajee V, Williamson CA, Fontana RJ, et al. Noninvasive intracranial pressure assessment in acute liver failure. Neurocrit Care. 2018;29:280–90.
Kim S, Han KH, Ahn SH. Hepatitis C virus and antiviral drug resistance. Gut Liver. 2016;10:890–5.
Karaman Erdur S, Kulac Karadeniz D, Kocabora MS, et al. Ocular surface and tear parameters in patients with chronic hepatitis C at initial stages of hepatic fibrosis. Eye Contact Lens. 2015;41:117–20.
Gumus K, Yurci A, Mirza E, et al. Evaluation of ocular surface damage and dry eye status in chronic hepatitis C at different stages of hepatic fibrosis. Cornea. 2009;28:997–1002.
Gifford FJ, Moroni F, Farrah TE, et al. The eye as a non-invasive window to the microcirculation in liver cirrhosis: a prospective pilot study. J Clin Med. 2020;9(10):3332.
Lampignano L, Niro A, Castellana F, et al. Liver fibrosis and retinal features in an older Mediterranean population: results from the Salus in Apulia study. Front Neurosci. 2022;16:1048375.
Liccardo D, Mosca A, Petroni S, et al. The association between retinal microvascular changes, metabolic risk factors, and liver histology in pediatric patients with non-alcoholic fatty liver disease (NAFLD). J Gastroenterol. 2015;50:903–12.
Mertz JL, Sripathi SR, Yang X, et al. Proteomic and phosphoproteomic analyses identify liver-related signaling in retinal pigment epithelial cells during EMT. Cell Rep. 2021;37:109866.
Zhou M, Geathers JS, Grillo SL, et al. Role of Epithelial-Mesenchymal Transition in Retinal Pigment Epithelium Dysfunction. Front Cell Dev Biol. 2020;8:501.
Jiang Y, Sun A, Zhao Y, et al. Proteomics identifies new therapeutic targets of early-stage hepatocellular carcinoma. Nature. 2019;567:257–61.
Reiter CE, Sandirasegarane L, Wolpert EB, et al. Characterization of insulin signaling in rat retina in vivo and ex vivo. Am J Physiol Endocrinol Metab. 2003;285:E763–74.
Adijanto J, Du J, Moffat C, et al. The retinal pigment epithelium utilizes fatty acids for ketogenesis. J Biol Chem. 2014;289:20570–82.
Reyes-Reveles J, Dhingra A, Alexander D, et al. Phagocytosis-dependent ketogenesis in retinal pigment epithelium. J Biol Chem. 2017;292:8038–47.
Han HS, Kang G, Kim JS, et al. Regulation of glucose metabolism from a liver-centric perspective. Exp Mol Med. 2016;48:e218.
Altamura S, Müdder K, Schlotterer A, et al. Iron aggravates hepatic insulin resistance in the absence of inflammation in a novel db/db mouse model with iron overload. Mol Metab. 2021;51:101235.
Gastaldelli A, Abdul Ghani M, DeFronzo RA. Adaptation of insulin clearance to metabolic demand is a key determinant of glucose tolerance. Diabetes. 2021;70:377–85.
Norton L, Shannon C, Gastaldelli A, et al. Insulin: the master regulator of glucose metabolism. Metabolism. 2022;129:155142.
Hernández C, Garcia-Ramírez M, García-Rocha M, et al. Glycogen storage in the human retinal pigment epithelium: a comparative study of diabetic and non-diabetic donors. Acta Diabetol. 2014;51:543–52.
Ballestri S, Zona S, Targher G, et al. Nonalcoholic fatty liver disease is associated with an almost twofold increased risk of incident type 2 diabetes and metabolic syndrome. Evidence from a systematic review and meta-analysis. J Gastroenterol Hepatol. 2016;31:936–44.
Hamed AE, Elsahar M, Elwan NM, et al. Managing diabetes and liver disease association. Arab J Gastroenterol. 2018;19:166–79.
Hashim Z, Zarina S. Osmotic stress induced oxidative damage: possible mechanism of cataract formation in diabetes. J Diabetes Complications. 2012;26:275–9.
Thakur S, Gupta SK, Ali V, et al. Aldose Reductase: a cause and a potential target for the treatment of diabetic complications. Arch Pharm Res. 2021;44:655–67.
Li X, Yu ZW, Li HY, et al. Retinal microglia polarization in diabetic retinopathy. Vis Neurosci. 2021;38:E006.
Forrester JV, Kuffova L, Delibegovic M. The Role of Inflammation in Diabetic Retinopathy. Front Immunol. 2020;11:583687.
Rübsam A, Parikh S, Fort PE. Role of inflammation in diabetic retinopathy. Int J Mol Sci. 2018;19(4):942.
Song BJ, Aiello LP, Pasquale LR. Presence and risk factors for glaucoma in patients with diabetes. Curr Diab Rep. 2016;16:124.
Yu AL, Fuchshofer R, Kampik A, et al. Effects of oxidative stress in trabecular meshwork cells are reduced by prostaglandin analogues. Invest Ophthalmol Vis Sci. 2008;49:4872–80.
Cakir B, Hellström W, Tomita Y, et al. IGF1, serum glucose, and retinopathy of prematurity in extremely preterm infants. JCI Insight. 2020;5(19):e140363.
Zibar K, Blaslov K, Bulum T, et al. Basal and postprandial change in serum fibroblast growth factor-21 concentration in type 1 diabetic mellitus and in healthy controls. Endocrine. 2015;48:848–55.
Lai AK, Lo AC. Animal models of diabetic retinopathy: summary and comparison. J Diabetes Res. 2013;2013:106594.
Fu Z, Gong Y, Liegl R, et al. FGF21 administration suppresses retinal and choroidal neovascularization in mice. Cell Rep. 2017;18:1606–13.
Badman MK, Pissios P, Kennedy AR, et al. Hepatic fibroblast growth factor 21 is regulated by PPARalpha and is a key mediator of hepatic lipid metabolism in ketotic states. Cell Metab. 2007;5:426–37.
Tao Y, He M, Yang Q, et al. Systemic taurine treatment provides neuroprotection against retinal photoreceptor degeneration and visual function impairments. Drug Des Devel Ther. 2019;13:2689–702.
Gaucher D, Arnault E, Husson Z, et al. Taurine deficiency damages retinal neurones: cone photoreceptors and retinal ganglion cells. Amino Acids. 2012;43:1979–93.
Singh C, Hoppe G, Tran V, et al. Serine and 1-carbon metabolism are required for HIF-mediated protection against retinopathy of prematurity. JCI Insight. 2019;4(14):e129398.
Hoppe G, Lee TJ, Yoon S, et al. Inducing a visceral organ to protect a peripheral capillary bed: stabilizing hepatic HIF-1α prevents oxygen-induced retinopathy. Am J Pathol. 2014;184:1890–9.
Montioli R, Bellezza I, Desbats MA, et al. Deficit of human ornithine aminotransferase in gyrate atrophy: molecular, cellular, and clinical aspects. Biochim Biophys Acta Proteins Proteom. 2021;1869:140555.
Seker Yilmaz B, Gissen P. Targeting the liver to treat the eye. EMBO Mol Med. 2023;15(4):e17285.
Montenegro D, Zhao J, Kim HJ, et al. Products of the visual cycle are detected in mice lacking retinol binding protein 4, the only known vitamin A carrier in plasma. J Biol Chem. 2022;298: 102722.
Shen J, Shi D, Suzuki T, et al. Severe ocular phenotypes in Rbp4-deficient mice in the C57BL/6 genetic background. Lab Invest. 2016;96:680–91.
Du M, Otalora L, Martin AA, et al. Transgenic mice overexpressing serum retinol-binding protein develop progressive retinal degeneration through a retinoid-independent mechanism. Mol Cell Biol. 2015;35:2771–89.
Du M, Phelps E, Balangue MJ, et al. Transgenic mice over-expressing RBP4 have RBP4-dependent and light-independent retinal degeneration. Invest Ophthalmol Vis Sci. 2017;58:4375–83.
Radhakrishnan R, Leung M, Roehrich H, et al. Mice lacking the systemic vitamin a receptor rbpr2 show decreased ocular retinoids and loss of visual function. Nutrients. 2022;14(12):2371.
Elbasiony E, Cho W, Mittal SK, et al. Suppression of lipopolysaccharide-induced corneal opacity by hepatocyte growth factor. Sci Rep. 2022;12:494.
Wong WK, Cheung AW, Yu SW, et al. Hepatocyte growth factor promotes long-term survival and axonal regeneration of retinal ganglion cells after optic nerve injury: comparison with CNTF and BDNF. CNS Neurosci Ther. 2014;20:916–29.
Machiraju D, Hassel JC. Targeting the cMET pathway to enhance immunotherapeutic approaches for mUM patients. Front Oncol. 2022;12:1068029.
Rasmussen MR, Sommerlund M, Moestrup SK. Is classical pseudoxanthoma elasticum a consequence of hepatic ‘intoxication’ due to ABCC6 substrate accumulation in the liver? Expert Rev Endocrinol Metab. 2013;8:37–46.
Onder C, Bengur T, Selcuk D, et al. Relationship between retinopathy and cirrhosis. World J Gastroenterol. 2005;11:2193–6.
Uhlén M, Fagerberg L, Hallström BM, et al. Proteomics. Tissue-based map of the human proteome. Science. 2015;347:1260419.
Protiva P, Gong J, Sreekumar B, et al. Pigment epithelium-derived factor (PEDF) Inhibits Wnt/β-catenin signaling in the liver. Cell Mol Gastroenterol Hepatol. 2015;1:535-549.e14.
Chen CC, Lee TY, Leu YL, et al. Pigment epithelium-derived factor inhibits adipogenesis in 3T3-L1 adipocytes and protects against high-fat diet-induced obesity and metabolic disorders in mice. Transl Res. 2019;210:26–42.
Scott BL, Bazan NG. Membrane docosahexaenoate is supplied to the developing brain and retina by the liver. Proc Natl Acad Sci U S A. 1989;86:2903–7.
Li J, Pora BLR, Dong K, et al. Health benefits of docosahexaenoic acid and its bioavailability: a review. Food Sci Nutr. 2021;9:5229–43.
McLellan GJ, Aktas Z, Hennes-Beean E, et al. Effect of a soluble epoxide hydrolase inhibitor, UC1728, on LPS-induced uveitis in the rabbit. J Ocul Biol. 2016;4(1):2334–838.
Jun S, Datta S, Wang L, et al. The impact of lipids, lipid oxidation, and inflammation on AMD, and the potential role of miRNAs on lipid metabolism in the RPE. Exp Eye Res. 2019;181:346–55.
Arab JP, Karpen SJ, Dawson PA, et al. Bile acids and nonalcoholic fatty liver disease: Molecular insights and therapeutic perspectives. Hepatology. 2017;65:350–62.
Win A, Delgado A, Jadeja RN, et al. Pharmacological and metabolic significance of bile acids in retinal diseases. Biomolecules. 2021;11(2):292.
Chen J, Thomsen M, Vitetta L. Interaction of gut microbiota with dysregulation of bile acids in the pathogenesis of nonalcoholic fatty liver disease and potential therapeutic implications of probiotics. J Cell Biochem. 2019;120:2713–20.
Beli E, Yan Y, Moldovan L, et al. Restructuring of the gut microbiome by intermittent fasting prevents retinopathy and prolongs survival in db/db Mice. Diabetes. 2018;67:1867–79.
Daruich A, Picard E, Boatright JH, et al. Review: the bile acids urso- and tauroursodeoxycholic acid as neuroprotective therapies in retinal disease. Mol Vis. 2019;25:610–24.
Tanumihardjo SA, Russell RM, Stephensen CB, et al. Biomarkers of nutrition for development (BOND)-vitamin A review. J Nutr. 2016;146:1816s-s1848.
Harrison EH. Mechanisms of transport and delivery of vitamin A and carotenoids to the retinal pigment epithelium. Mol Nutr Food Res. 2019;63: e1801046.
Kim JE, Clark RM, Park Y, et al. Lutein decreases oxidative stress and inflammation in liver and eyes of guinea pigs fed a hypercholesterolemic diet. Nutr Res Pract. 2012;6:113–9.
Li B, Vachali P, Chang FY, et al. HDL is the primary transporter for carotenoids from liver to retinal pigment epithelium in transgenic ApoA-I(−/−)/Bco2(−/−) mice. Arch Biochem Biophys. 2022;716:109111.
Nezzar H, Chiambaretta F, Marceau G, et al. Molecular and metabolic retinoid pathways in the human ocular surface. Mol Vis. 2007;13:1641–50.
Samarawickrama C, Chew S, Watson S. Retinoic acid and the ocular surface. Surv Ophthalmol. 2015;60:183–95.
Perdices L, Fuentes-Broto L, Segura F, et al. Hepatic oxidative stress in pigmented P23H rhodopsin transgenic rats with progressive retinal degeneration. Free Radic Biol Med. 2018;124:550–7.
Sijilmassi O, Del Río SA, Maldonado Bautista E, et al. Gestational folic acid deficiency alters embryonic eye development: Possible role of basement membrane proteins in eye malformations. Nutrition. 2021;90:111250.
Enz TJ, Tribble JR, Williams PA. Comparison of glaucoma-relevant transcriptomic datasets identifies novel drug targets for retinal ganglion cell neuroprotection. J Clin Med. 2021;10(17):3938.
Liu X, Cui H. The palliative effects of folic acid on retinal microvessels in diabetic retinopathy via regulating the metabolism of DNA methylation and hydroxymethylation. Bioengineered. 2021;12:10766–74.
Yang S, Ye Z, Liu M, et al. Associations of different serum folate forms with indices of nonalcoholic fatty liver disease and advanced fibrosis. Obes Res Clin Pract. 2023;17:58–65.
Caban M, Lewandowska U. Vitamin D, the vitamin D receptor, calcitriol analogues and their link with ocular diseases. Nutrients. 2022;14(11):2353.
Rhyu J, Yu R. Newly discovered endocrine functions of the liver. World J Hepatol. 2021;13:1611–28.
Lin SH, Wang CC, Huang KT, et al. Liver graft pathology and low serum 25-hydroxyvitamin D after living donor liver transplantation. Metabolites. 2022;12(5):388.
Ma C, Han L, Zhu Z, et al. Mineral metabolism and ferroptosis in non-alcoholic fatty liver diseases. Biochem Pharmacol. 2022;205:115242.
Shahandeh A, Bui BV, Finkelstein DI, et al. Effects of excess iron on the retina: insights from clinical cases and animal models of iron disorders. Front Neurosci. 2021;15:794809.
Guo CH, Chen PC, Ko WS. Status of essential trace minerals and oxidative stress in viral hepatitis C patients with nonalcoholic fatty liver disease. Int J Med Sci. 2013;10:730–7.
Baumann BH, Shu W, Song Y, et al. Liver-specific, but not retina-specific, hepcidin knockout causes retinal iron accumulation and degeneration. Am J Pathol. 2019;189:1814–30.
Mohammad MK, Zhou Z, Cave M, et al. Zinc and liver disease. Nutr Clin Pract. 2012;27:8–20.
Gilbert R, Peto T, Lengyel I, et al. Zinc Nutrition and Inflammation in the Aging Retina. Mol Nutr Food Res. 2019;63:e1801049.
Rodríguez-Menéndez S, Fernández B, García M, et al. Quantitative study of zinc and metallothioneins in the human retina and RPE cells by mass spectrometry-based methodologies. Talanta. 2018;178:222–30.
Charbonnier P, Chovelon B, Ravelet C, et al. ATP7B-deficient hepatocytes reveal the importance of protein misfolding induced at low copper concentration. Cells. 2022;11(21):3400.
Annamalai AK, Prajna VN, Chowdhury G, et al. Wilson disease: never too late. Am J Med. 2022;135:e370–1.
Xu R, Ritz BK, Wang Y, et al. The retina and retinal pigment epithelium differ in nitrogen metabolism and are metabolically connected. J Biol Chem. 2020;295:2324–35.
Hakvoort TB, He Y, Kulik W, et al. Pivotal role of glutamine synthetase in ammonia detoxification. Hepatology. 2017;65:281–93.
Jung E, Kim J. Aloin inhibits Müller cells swelling in a rat model of thioacetamide-induced hepatic retinopathy. Molecules. 2018;23(11):2806.
Kroupina K, Bémeur C, Rose CF. Amino acids, ammonia, and hepatic encephalopathy. Anal Biochem. 2022;649:114696.
Xu J, Hao J, Gao Y, et al. Hepatic cortical blindness. Am J Med Sci. 2022;364:492–8.
Kahán A, Málnási S, Szalai L, et al. Bilirubin retinopathy. Br J Ophthalmol. 1968;52:808–17.
Carroll WJ, Peck T, Jenkins TL, et al. Periocular, periorbital, and orbital pathology in liver disease. Surv Ophthalmol. 2017;62:134–49.
Li P, Yang Y, Lin Z, et al. Bile duct ligation impairs function and expression of Mrp1 at rat blood-retinal barrier via bilirubin-induced P38 MAPK pathway activations. Int J Mol Sci. 2022;23(14):7666.
Albanna W, Lüke JN, Schubert GA, et al. Modulation of Ca(v)2.3 channels by unconjugated bilirubin (UCB)—Candidate mechanism for UCB-induced neuromodulation and neurotoxicity. Mol Cell Neurosci. 2019;96:35–46.
Good WV, Wong RJ, Norcia AM, et al. Bilirubin-induced neurotoxicity and visuocortical dysfunction. J Perinatol. 2023;43:240–1.
Ishibashi F, Kawasaki A, Kojima R, et al. Association between serum total bilirubin levels and the morphology of corneal nerve fibers in Japanese patients with uncontrolled type 2 diabetes. Diabetes Care. 2014;37:e131–2.
Dreismann AK, Hallam TM, Tam LC, et al. Gene targeting as a therapeutic avenue in diseases mediated by the complement alternative pathway. Immunol Rev. 2023;313:402–19.
Lyzogubov VV, Tytarenko RG, Jha P, et al. Role of ocular complement factor H in a murine model of choroidal neovascularization. Am J Pathol. 2010;177:1870–80.
Kim EJ, Grant GR, Bowman AS, et al. Complete transcriptome profiling of normal and age-related macular degeneration eye tissues reveals dysregulation of anti-sense transcription. Sci Rep. 2018;8:3040.
Mohammad S, Thiemermann C. Role of metabolic endotoxemia in systemic inflammation and potential interventions. Front Immunol. 2020;11:594150.
Andriessen EM, Wilson AM, Mawambo G, et al. Gut microbiota influences pathological angiogenesis in obesity-driven choroidal neovascularization. EMBO Mol Med. 2016;8:1366–79.
Jensen-Cody SO, Potthoff MJ. Hepatokines and metabolism: Deciphering communication from the liver. Mol Metab. 2021;44:101138.
Eldh M, Olofsson Bagge R, Lässer C, et al. MicroRNA in exosomes isolated directly from the liver circulation in patients with metastatic uveal melanoma. BMC Cancer. 2014;14:962.
Aughton K, Kalirai H, Coupland SE. MicroRNAs and uveal melanoma: understanding the diverse role of these small molecular regulators. Int J Mol Sci. 2020;21(16):5648.
Zhu D, He X, Duan Y, et al. Expression of microRNA-454 in TGF-β1-stimulated hepatic stellate cells and in mouse livers infected with Schistosoma japonicum. Parasit Vectors. 2014;7:148.
Xiong YC, Chen T, Yang XB, et al. 17β-oestradiol attenuates the photoreceptor apoptosis in mice with retinitis pigmentosa by regulating N-myc downstream regulated gene 2 Expression. Neuroscience. 2021;452:280–94.
Li R, Wang Y, Chen P, et al. G-protein-coupled estrogen receptor protects retinal ganglion cells via inhibiting endoplasmic reticulum stress under hyperoxia. J Cell Physiol. 2021;236:3780–8.
Li R, Wang Y, Chen P, et al. Inhibiting endoplasmic reticulum stress by activation of G-protein-coupled estrogen receptor to protect retinal astrocytes under hyperoxia. J Biochem Mol Toxicol. 2021;35:e22641.
Means JC, Lopez AA, Koulen P. Estrogen protects optic nerve head astrocytes against oxidative stress by preventing caspase-3 activation, Tau dephosphorylation at Ser(422) and the formation of tau protein aggregates. Cell Mol Neurobiol. 2021;41:449–58.
Hao M, Li Y, Lin W, et al. Estrogen prevents high-glucose-induced damage of retinal ganglion cells via mitochondrial pathway. Graefes Arch Clin Exp Ophthalmol. 2015;253:83–90.
Nadeem U, Boachie-Mensah M, Zhang J, et al. Gut microbiome and retinal diseases: an updated review. Curr Opin Ophthalmol. 2022;33:195–201.
Skrzypecki J, Niewęgłowska K, Samborowska E. Valeric Acid, a Gut Microbiota Product, Penetrates to the Eye and Lowers Intraocular Pressure in Rats. Nutrients. 2020;12(2):387.
Loomba R, Seguritan V, Li W, et al. Gut microbiome-based metagenomic signature for non-invasive detection of advanced fibrosis in human nonalcoholic fatty liver disease. Cell Metab. 2017;25:1054-1062.e5.
Su X, Gao Y, Yang R. Gut microbiota derived bile acid metabolites maintain the homeostasis of gut and systemic immunity. Front Immunol. 2023;14:1127743.
Schaefer L, Hernandez H, Coats RA, et al. Gut-derived butyrate suppresses ocular surface inflammation. Sci Rep. 2022;12:4512.
Huang Y, Wang Z, Ye B, et al. Sodium butyrate ameliorates diabetic retinopathy in mice via the regulation of gut microbiota and related short-chain fatty acids. J Transl Med. 2023;21:451.
Singh S, Singh PK, Kumar A. Butyrate ameliorates intraocular bacterial infection by promoting autophagy and attenuating the inflammatory response. Infect Immun. 2023;91:e0025222.
Choudhary M, Malek G. The aryl hydrocarbon receptor: a mediator and potential therapeutic target for ocular and non-ocular neurodegenerative diseases. Int J Mol Sci. 2020;21(18):6777.
Chen J, Vitetta L, Henson JD, et al. Intestinal dysbiosis, the tryptophan pathway and nonalcoholic steatohepatitis. Int J Tryptophan Res. 2022;15:11786469211070532.
Tiecco G, Laurenda D, Mulè A, et al. Gram-negative endogenous endophthalmitis: a systematic review. Microorganisms. 2022;11(1):80.
Hunt KE, Glasgow BJ. Aspergillus endophthalmitis. An unrecognized endemic disease in orthotopic liver transplantation. Ophthalmology. 1996;103:757–67.
Jager MJ, Shields CL, Cebulla CM, et al. Uveal melanoma. Nat Rev Dis Primers. 2020;6:24.
Rim TH, Lee G, Kim Y, et al. Prediction of systemic biomarkers from retinal photographs: development and validation of deep-learning algorithms. Lancet Digit Health. 2020;2:e526–36.
Ouerfelli-Ethier J, Elsaeid B, Desgroseilliers J, et al. Anti-saccades predict cognitive functions in older adults and patients with Parkinson’s disease. PLoS ONE. 2018;13:e0207589.
Chehrehnegar N, Nejati V, Shati M, et al. Behavioral and cognitive markers of mild cognitive impairment: diagnostic value of saccadic eye movements and Simon task. Aging Clin Exp Res. 2019;31:1591–600.
Montagnese S, Gordon HM, Jackson C, et al. Disruption of smooth pursuit eye movements in cirrhosis: relationship to hepatic encephalopathy and its treatment. Hepatology. 2005;42:772–81.
Ting DSW, Peng L, Varadarajan AV, et al. Deep learning in ophthalmology: The technical and clinical considerations. Prog Retin Eye Res. 2019;72:100759.
Balyen L, Peto T. Promising artificial intelligence-machine learning-deep learning algorithms in ophthalmology. Asia Pac J Ophthalmol. 2019;8:264–72.
Peeters F, Rommes S, Elen B, et al. Artificial intelligence software for diabetic eye screening: diagnostic performance and impact of stratification. J Clin Med. 2023;12(4):1408.
Pandey PU, Ballios BG, Christakis PG, et al. An ensemble of deep convolutional neural networks is more accurate and reliable than board-certified ophthalmologists at detecting multiple diseases in retinal fundus photographs. Br J Ophthalmol. 2023. https://doi.org/10.1136/bjo-2022-322183.
Rasheed HA, Davis T, Morales E, et al. DDLSNet: a novel deep learning-based system for grading funduscopic images for glaucomatous damage. Ophthalmol Sci. 2023;3:100255.
Attallah O. GabROP: gabor wavelets-based cad for retinopathy of prematurity diagnosis via convolutional neural networks. Diagnostics (Basel). 2023;13(2):171.
Han J, Choi S, Park JI, et al. Detecting macular disease based on optical coherence tomography using a deep convolutional network. J Clin Med. 2023;12(3):1005.
Bergasa NV, Link MJ, Keogh M, et al. Pilot study of bright-light therapy reflected toward the eyes for the pruritus of chronic liver disease. Am J Gastroenterol. 2001;96:1563–70.
Beuers U, Wolters F, Oude Elferink RPJ. Mechanisms of pruritus in cholestasis: understanding and treating the itch. Nat Rev Gastroenterol Hepatol. 2023;20:26–36.
Wang Y, Wang X, Di Y. Surgery combined with antibiotics for the treatment of endogenous endophthalmitis caused by liver abscess. BMC Infect Dis. 2020;20:661.
Seker Yilmaz B, Gissen P. Targeting the liver to treat the eye. EMBO Mol Med. 2023;15:e17285.
Kuzmin DA, Shutova MV, Johnston NR, et al. The clinical landscape for AAV gene therapies. Nat Rev Drug Discov. 2021;20:173–4.
Boffa I, Polishchuk E, De Stefano L, et al. Liver-directed gene therapy for ornithine aminotransferase deficiency. EMBO Mol Med. 2023;15:e17033.
Khanani AM, Thomas MJ, Aziz AA, et al. Review of gene therapies for age-related macular degeneration. Eye (Lond). 2022;36:303–11.
Saika S, Yamanaka O, Sumioka T, et al. Fibrotic disorders in the eye: targets of gene therapy. Prog Retin Eye Res. 2008;27:177–96.
Huang Y, Wang J, Wang Y, et al. Pharmacological mechanism and clinical study of Qiming granules in treating diabetic retinopathy based on network pharmacology and literature review. J Ethnopharmacol. 2023;302:115861.
Li XY, Su FF, Jiang C, et al. Development history and prospect of Fel Ursi. Zhongguo Zhong Yao Za Zhi. 2022;47:4284–91.
Gao LL, Ma JM, Fan YN, et al. Lycium barbarum polysaccharide combined with aerobic exercise ameliorated nonalcoholic fatty liver disease through restoring gut microbiota, intestinal barrier and inhibiting hepatic inflammation. Int J Biol Macromol. 2021;183:1379–92.
Xi X, Han L, Ding M, et al. Exploring the relationship between intestinal flora and the pathological mechanism of myopia in adolescents from the perspective of Chinese and Western medicine: a review. Medicine. 2023;102:e33393.
Hermans MP, Bouenizabila E, Daniel Amoussou-Guenou K, et al. Fatty liver and atherogenic dyslipidemia have opposite effects on diabetic micro- and macrovascular disease. Diabetes Metab Syndr. 2022;16:102613.
Galiero R, Pafundi PC, Nevola R, et al. The importance of telemedicine during COVID-19 pandemic: a focus on diabetic retinopathy. J Diabetes Res. 2020;2020:9036847.
De Rossi G, Da Vitoria Lobo ME, Greenwood J, et al. LRG1 as a novel therapeutic target in eye disease. Eye. 2022;36:328–40.
Pan X, Zhou J, Chen Y, et al. Classification, hepatotoxic mechanisms, and targets of the risk ingredients in traditional Chinese medicine-induced liver injury. Toxicol Lett. 2020;323:48–56.
Acknowledgements
We acknowledged all authors corresponding to our references and BioRender.com.
Funding
This work was funded by the National Natural Science Foundation of China, Grant number: 82170570.
Author information
Authors and Affiliations
Contributions
JHW and YFY conceived the study idea, and C.H.D to the study design. The literature collection and analysis were performed by JHW, YFY, CHD, ZW, CT, LZH. This manuscript was revised by CQH, XHH.
Corresponding authors
Ethics declarations
Consent for publication
All authors have read and approved the final version of the manuscript.
Competing interests
All authors declared that the study was performed without any competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, J., Duan, C., Yang, Y. et al. Insights into the liver-eyes connections, from epidemiological, mechanical studies to clinical translation. J Transl Med 21, 712 (2023). https://doi.org/10.1186/s12967-023-04543-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-023-04543-3