
Abstract
Background
The global prevalence of insufficient physical activity (PA) was reported to be 27.5% in 2016, and there were stable levels of insufficient PA worldwide between 2001 and 2016. The global target of a 10% reduction in insufficient PA by 2025 will not be met if the trends remain. The relevant data for trends in China were still scarce. This study aimed to determine nationwide temporal trends in insufficient PA among adults in China from 2010 to 2018.
Methods
645 903 adults aged 18 years or older were randomly selected from four nationally representative cross-sectional surveys of the China Chronic Disease and Risk Factor Surveillance conducted in 2010, 2013, 2015, and 2018. PA was measured using the Global Physical Activity Questionnaire. Temporal changes in insufficient PA prevalence and participation of domain-specific moderate- to vigorous-intensity PA (MVPA) were analyzed using logistic regression.
Results
From 2010 to 2018, the age-adjusted prevalence of insufficient PA in China increased from 17.9% (95% confidence interval 16.3% to 19.5%) in 2010 to 22.3% (20.9% to 23.8%) in 2018 (P for trend < 0.001). By age group, with a significant increase in insufficient PA in adults aged 18–34 years (P for trend < 0.001), which rose more rapidly than in adults aged ≥ 35 years (P for interaction < 0.001). Insufficient PA has increased significantly among adults engaged in agriculture-related work, non-manual work, and other manual work (all P for trend < 0.05). And among the occupational groups, those engaged in agriculture-related work had the fastest increase (P for interaction = 0.01). The percentage of adults participating in work-related MVPA decreased from 79.6% (77.8% to 81.5%) to 66.8% (64.9% to 68.7%) along with a decrease in time spent on work-related MVPA, while percentages of adults participating in recreation-related MVPA increased from 14.2% (12.5% to 15.9%) to 17.2% (16.0% to 18.4%) (all P for trend < 0.05).
Conclusions
Among Chinese adults, an increasing trend was found in insufficient PA from 2010 to 2018, with more than one-fifth of adults failing to achieve the recommendation of adequate PA. More targeted PA promotion strategies should be developed to improve population health.
Similar content being viewed by others

Introduction
Insufficient physical activity (PA), defined as less than 150 min of moderate-intensity aerobic PA or 75 min of vigorous-intensity aerobic PA per week, or equivalent [1, 2], is an important risk factor for non-communicable diseases (NCDs), including hypertension, type 2 diabetes, breast cancer, colorectal cancer, and chronic pain [3,4,5,6,7,8,9]. Insufficient PA also has been estimated as the fourth leading risk factor for global mortality [10] and is estimated to cost global healthcare systems $50 billion annually [11]. It has been a prominent and increasingly prevalent global public health problem [11, 12]. Since the end of the twentieth century, PA related recommendations highlighted moderate- to vigorous-intensity PA (MVPA), including walking, cycling, running, and gardening, mainly for adults [13]. MVPA can effectively weaken the link between sedentary time and the risk of cardiovascular disease mortality [14]. MVPA also improves mental health, such as depression and anxiety [15].
So far, many studies have explored the prevalence of insufficient PA and its trend over time, especially in developed countries. A global study of insufficient PA pooled data from 358 surveys across 168 countries and estimated global and regional trends in insufficient PA from 2001 to 2016. The results showed that in 2016, the prevalence of age-standardized insufficient PA was 27.5% globally, higher for women than men [16]. Another worldwide study found that insufficient PA is higher in high-income countries than in low-income [12]. Further, insufficient PA exists in several domains in life: at work, transport, or recreation, and different domains-specific PA may affect health differently [17]. Tessa et al. reported that work-related PA was the highest contributor, and recreation-related PA was the lowest contributor in PA of 81 countries, including China [18]. Otherwise, a previous study found that the odds of engaging in recreation-related PA among the elderly in China were higher than that of the younger [19]. Higher levels of all domain-specific PA were associated with a lower risk of all-cause mortality [17]. Recreation-related PA has a stronger relationship with mental health than work-related PA and transport-related PA [20]. It is essential to study domain-specific PA trends and propose appropriate policies. The Outline of the “Healthy China 2030” Plan, issued on October 25, 2016, has initiated a nationwide fitness campaign, stipulating that more than 40% of urban and rural residents should regularly participate in the exercise by 2030 [21, 22]. However, a long period is required to achieve the goal. To the best of our knowledge, no studies or reports provided temporal trends and detailed demographics, the location-specific prevalence of insufficient PA, and the PA patterns in China's total or subpopulation.
To further understand the changes in the prevalence of insufficient PA in the Chinese mainland in recent years, supplement the gaps in relevant domestic research fields, and provide a basis for future policy formulation and further research, our study used data from the China Chronic Disease and Risk Factor Surveillance (CCDRFS). It aimed to examine trends in insufficient PA among Chinese adults aged 18 years or older according to age, gender, geographical location, ethnicity, education, occupation, income, body mass index (BMI), and different domain-specific PA from 2010 to 2018.
Methods
Study design and population
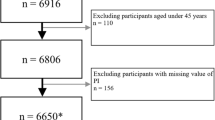
The China Chronic Disease and Risk Factor Surveillance (CCDRFS), established by the Chinese Center for Disease Control and Prevention (China CDC) and incorporated into the National Disease Surveillance Points (DSPs) system, is a series of periodical cross-sectional nationwide surveys that collected data on PA and other health-related risk factors (e.g., smoking, harmful drinking, and unbalanced diet) [23]. DSPs system comprised 161 districts/counties in all 31 provinces (autonomous and municipalities) from 2004 to 2012 and expanded to 605 districts/counties since 2013 [24, 25]. Within the DSPs scheme, the CCDRFS has also been designed to represent mainland China's entire population. In 2010, all 161 DSPs conducted the CCDRFS survey. Since 2013, with the expansion of the DSPs system, the CCDRFS was further expanded to 298 DSPs and represented the national and provincial levels (Appendix 1). Appendix Fig. 1 shows the maps of surveillance districts/counties before and after expansion in 2013. Within the DSPs, the participants were selected using a multi-stage stratified clustering random sampling method. First, the townships or subdistricts were chosen using the proportional to population size (PPS) sampling (2010 and 2013) or the systematic random sampling (SRS, 2015 and 2018) [26]. Second, the villages or residential areas were selected using the PPS (2010 and 2013) method or SRS (2015 and 2018) method in each chosen township/subdistrict. Third, each village or residential area was divided into several residential quarters, with 50–60 households. Finally, 50 families from one residential quarter were selected to be the target households in 2010 and 2013, and 45 families from one residential quarter were selected to be the target households in 2015 and 2018 (Fig. 1). For the CCDRFS 2010 and CCDRFS 2013, the Kish method was used to choose one participant within every household [27, 28]. Since 2015, all eligible participants were invited to participate in the field survey. The participants who met the following inclusion criteria were included in the CCDRFS: 1) aged 18 years or older; 2) having lived in the address for more than six months in the past 12 months; 3) not pregnant; 4) with no serious health condition or illness which could be the inability to complete the interviews or potentially interfere with PA, including intellectual disability or language disorder. Figure 1 shows the details of the sampling frame of four CCDRFS surveys. The Ethical Committee of the Chinese Center for Disease Control and Prevention (China CDC) approved the 2015 survey (No.201519-B). All other CCDRFS surveys (No.201010, No.201307, No.201819) were approved by the Ethical Committee of the National Center for Chronic and Noncommunicable Disease Control and Prevention (NCNCD), except the 2015 survey. Every participant provided written informed consent. The Ethical Committee of the NCNCD approved this study to analyze all CCDRFS data (202019).

Flow diagram of study design and sampling procedure of China Chronic Disease and Risk Factors Surveillance 2010-18. DSPs: Disease Surveillance Points; PPS: probability to size sampling; SRS: systematic random sampling. †All DSPs were selected. ‡half of all DSPs (605) were selected using stratified sampling
Of the 681 236 individuals initially invited, 650 270 completed the surveys (95.5%), including 98 174 in 2010, 177 466 in 2013, 189 754 in 2015, and 184 876 in 2018. The corresponding survey response rates from 2010 to 2018 were 90.5%, 96.9%, 97.4%, and 94.9%, respectively. After excluding 1564 participants with missing basic information data (e.g., age, gender, educational attainment, etc.) and 2803 participants with missing or unreasonable values for PA, 645 903 adults were included in this study.
Physical activity measures
Trained interviewers from the local Centers for Disease Control and Prevention conducted the face-to-face questionnaire interview, physical measurement, and biochemical sample collection. The householder or an adult well acquainted with the household was interviewed using a household questionnaire. The economic and environmental information of the household, as well as the basic information of all family members (e.g., birth date, gender), was collected. The participants meeting the inclusion criteria were interviewed by investigators using an individual questionnaire (paper-and-pencil based in 2010 and 2013, tablet-assisted in 2015 and 2018) to obtain information on demographic characteristics, lifestyle factors, and history of chronic diseases (Appendix 2). All data collected by paper–pencil interviews were entered in customized entry software promptly by interviewees and were delivered to the NCNCD by the internet. Once outliers or missing data are found during the entry process, the interviewees were required to correct or supplement them in time. No significant difference in the number of outliers or missing values was found between the data collected by the paper-and-pencil interviewing and tablet-assisted interviewing.
The Global Physical Activity Questionnaire (GPAQ) released by World Health Organization (WHO) was used to collect data on PA in the CCDRFS since 2010 (Appendix 4&5)[29, 30]. The GPAQ is a global tool for measuring PA and has been validated among adults in more than 20 countries. Short-term (that is, every one to two weeks) and long-term (that is, two to three months apart) test–retest reliability was good to very good [31]. Therefore, we used the data from 2010 to 2018 in the present study to ensure the comparability of the results. The GPAQ measures PA in duration, frequency, intensity, and context (work, transport, and leisure time) [32]. According to the GPAQ, PA is categorized into three modules: work-related (including household chores), transport-related, and recreation-related. Work-related and recreation-related PA were further divided into two subtypes with different intensities: vigorous and moderate. Transport-related PA was moderate-intensity. Participants were also asked to provide PA information, including the days engaged in a subtype of PA (e.g., vigorous work-related, moderate work-related, transport-related, vigorous recreation-related, and moderated recreation-related) in a typical week and time spent on a typical day. In 2010, the WHO recommended that all adults should do at least 150 min of moderate-intensity aerobic PA, at least 75 min of vigorous-intensity aerobic PA, or an equivalent combination of moderate- and vigorous-intensity activity throughout the week for substantial health benefits[33]. In 2013, insufficient PA was included in 25 indicators for NCDs comprehensive global monitoring framework and defined as less than 150 min of moderate-intensity activity per week, or equivalent[2]. The WHO released updated global guidelines on PA and sedentary behavior in 2020 [10]. In general, the minimum recommended amount of sufficient PA remains 150 min of moderate-intensity activity per week or equivalent. In this study, the participants who did not meet the minimum recommended amount of PA by WHO (< 150 min/week) were considered individuals with insufficient PA. When calculating the total time of MVPA, the time of vigorous PA should be multiplied by 2. We also reported the trends in the percentages of adults with MVPA more than 150 min/week and less than 300 min/week. The adults participating in domain-specific or intensity-specific PA were defined as having a ‘Yes’ response to the participation of PA subtypes. Age was classified as 18–34 years, 35–49 years, 50–64 years, and 65 years and above. According to the Compilation Rules of Statistical Zoning Code and Urban–Rural Division Code formulated by the National Bureau of Statistics, we used the urban and rural division codes to confirm whether the region where the participants live is urban or rural areas. Urban and rural classification codes beginning with a 1 indicate an urban community and beginning with a 2 indicate a rural village. Educational attainment was classified as secondary school or less, high school, and college or above. The occupations of the participants were classified into five groups: agriculture-related work, other manual work, non-manual work, unemployed (including students), and retired. BMI was categorized as underweight (BMI < 18.5 kg/m2), normal weight (18.5 kg/m2 ≤ BMI < 25 kg/m2), overweight (25 kg/m2 ≤ BMI < 30 kg/m2), and obese (BMI ≥ 30 kg/m2) according to WHO classification [34].
Statistical analyses
We accounted for the complex sample design using Taylor's series method with finite population correction for primary sampling units while estimating the sampling error [35]. All estimates, including the prevalence and means, were age-adjusted to the 2010 China standard population. The trends in prevalence or percentages over the four survey cycles by gender, age, geographical location, education, ethnicity, occupation, income, and BMI group were tested using logistic regression models; the survey cycle was treated as a continuous (ordered categorical) and independent variable. The homogeneity of the prevalence of insufficient PA across strata in each survey cycle was tested by using logistic regression models including survey cycle × strata interaction terms, with strata-specific survey cycle effect models also fitted. To test linear trends of mean minutes per week of MVPA over time, we performed linear regression models with the survey year included as an independent variable. Statistical significance was determined as a two-sided P < 0.05. All statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc, Cary, North Carolina, U.S.).
Results
Table 1 shows the essential characteristics of the samples for each survey. Between 2010 and 2018, the number of participants included in each CCDRFS survey increased from 97 837 to 183 813. From 2010 to 2018, adults living in urban areas (51.7%) and those with college or above education (17.7%) showed a higher proportion in 2018 compared to those in 2010, whereas the inverse result was showed for adults with secondary school or less education (71.8% to 64.7%). From 2010 to 2018, a lower proportion of adults performed agriculture-related work (44.0% to 33.8%). Nevertheless, adults performed non-manual work (38.1% to 47.1%), and the unemployed adults/students (6.9% to 8.9%) were observed as a higher proportion. The proportion of adults with BMI ≥ 25 kg/m2 increased steadily.
Insufficient PA prevalence
The overall prevalence of age-adjusted insufficient PA among Chinese adults aged 18 years or older increased from 17.9% (95% confidence interval 16.3 to 19.5) in 2010 to 22.3% (20.9 to 23.8) in 2018, with a slight decrease in 2013 (P for trend < 0.001). By gender, the prevalence of MVPA < 150 min/w increased from 20.1% (18.5 to 21.8) to 24.4% (23.0 to 25.9) among men, while an increase from 15.7% (13.9 to 17.4) to 20.2 (18.5 to 21.9) was observed among women (all P for trend < 0.001). By age group, with a significant increase of 6.1% in insufficient PA in younger adults aged 18–34 years (P for change < 0.001), which rose more rapidly than in adults aged ≥ 35 years (P for interaction < 0.001), but no statistically significant change was observed in the elderly (P for change = 0.13). The prevalence of insufficient PA in rural adults rose from 17.1% to 22.6%, while that rose from 18.8% to 22.0% in urban adults (all P for trend < 0.001). From 2010 to 2018, the prevalence of insufficient PA increased in both Han (from 18.1 to 22.5, P for trend < 0.001) and other ethnic groups (from 15.9 to 20.3, P for trend < 0.001). From 2010 to 2018, insufficient PA increased significantly among adults with lower educational qualifications (high school or less), those engaged in agriculture-related work, non-manual work, and other manual work (all P for trend < 0.05). In addition, among the occupational groups, those engaged in agriculture-related work had the fastest increase in the prevalence of insufficient PA (P for interaction = 0.01). Our results suggest that the prevalence of insufficient PA is on the rise across all income groups (all P for trend < 0.05). Since 2010, the prevalence of insufficient PA has increased among all BMI groups, especially among adults with a BMI < 18.5 kg/m2 (all P for trend < 0.05) (Table 2).
The prevalence of insufficient PA increased in both rural (5.8 of the relative increase, P for trend < 0.001) and urban (2.6% of the relative increase, P for trend = 0.005) men in 2018 compared to 2010. A similar change was also observed in urban and rural women (P for trend < 0.001) (Fig. 2A). The increase in insufficient PA was observed among young adults aged 18–34 years in both rural (8.8% of the relative increase, P for change < 0.001) and urban (3.6% of the relative increase, P for change < 0.001). In addition, no significant change in insufficient PA was found except in the older age group of 65 years, however, all other age groups showed an upward trend (Appendix Table 1). Overall, no changes were observed in the percentages of adults undertaking 150–299 min/w of MVPA from 2010 to 2018 (P for trend = 0.23) (Appendix Table 2).

Trends in insufficient PA (<150 min/w) and percentages of adults undertaking 150-299 min/w of MVPA in China, 2010-18
Change in domain-specific no MVPA
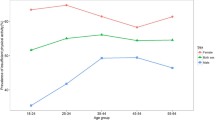
Regarding the change in participating in domain-specific MVPA, during the 8 years, the percentages of adults participating in work-related MVPA decreased most significantly, from 79.6% (77.8% to 81.5%) to 66.8% (64.9% to 68.7%) (P for trend < 0.001) (Fig. 3A), while the percentages of adults participating in recreation-related MVPA increased from 14.2% (12.5% to 15.9%) to 17.2% (16.0% to 18.4%) (P for trend = 0.014) (Fig. 3C). Participating in work-related MVPA was more prevalent among rural adults (70.7% [68.2% to 73.1%]) and women (70.6% [68.6% to 72.7%]) in 2018 (Fig. 3A). In contrast, the percentages of participating in recreation-related MVPA was higher among adults from urban areas (21.2% [19.5% to 23.0%]) and men (18.6% [17.0% to 20.2%] in 2018 (Fig. 3C). No change was observed in the percentages of adults participating in transport-related MVPA (Fig. 3B).

Trends in percentages of adults participating domain-specific MVPA in China, 2010-18
Appendix Table 4 shows the mean minutes of domain-specific MVPA per week. From 2010 to 2018, the mean minutes of work-related MVPA declined significantly in women from 922.5 min/wk (1276.7) to 817.1 min/wk (1385.6) (P for trend = 0.014) and in the youngest adults from 858.0 min/wk (1353.5) to 672.1 min/wk (1382.5) (P for trend < 0.001). A slight but significant increase was observed for minutes of transport-related MVPA overall and by characteristics (all P for trend < 0.001). For mean minutes of recreation-related MVPA, a significant increase was observed in men, women, adults aged less than 50 years, and those living in rural areas (all P for trend < 0.001). In addition, the relative contributions of domain-specific activity to total MVPA are shown in the appendix. (Appendix Table 5). There are similar research results in no intensity-specific MVPA among Chinese adults in our study. (Appendix Table 6).
Discussion
Our study was the first large nationwide study assessing the long-term trend of insufficient PA in China. Data from four large consecutive and nationally representative surveys between 2010 to 2018 showed that insufficient PA among Chinese adults (both men and women) had increased since 2010. In urban, the prevalence of insufficient PA was still climbing between men and women, and there was also a rising trend in rural. Regarding the change in domain-specific MVPA, the prevalence of work-related and transport-related MVPA decreased most significantly, while recreation-related MVPA increased. In the stratified analysis, the percentage of work-related MVPA decreased significantly in both urban and rural areas, while the downward trend of transport-related MVPA and the upward trend of recreation-related MVPA were only significant in rural areas.
WHO has set a specific insufficient PA control goal, a 10% relative reduction in the prevalence of insufficient PA by 2025[2]. However, due to the lack of historical data, the Chinese government has not set a similar goal. This study showed that from 2010 to 2018, the overall insufficient PA prevalence in Chinese adults increased by 24.6%, slightly decreasing from 2010 to 2013. Guthold’s study showed that the global prevalence of insufficient PA was stable between 2001 (28.5%) and 2016 (27.5%), as well as divergent trends, were observed in different areas or countries [16]. This study showed that the overall increasing trend in China was consistent with western high-income countries, and both were in a relatively stable state. However, there was a certain rise in insufficient PA in our research. China’s current insufficient PA was lower than the global average and neighboring developed countries like Japan and South Korea, but higher than other East and Southeast Asia countries [16]. Such a position was comparable to China's economic development level globally. As for the decrease from 2010 to 2013, we considered the survey season as one of the possible reasons. In CCDRFS 2010, 2015, and 2018, more than 85% of participants were interviewed in late autumn and winter (e.g., November, December, and January). However, in CCDRFS 2013, this proportion was less than 30%. The previous study showed a seasonal effect as PA appeared to be highest in spring and summer [36]. In addition, a cohort study in Hong Kong, China, showed an inverted U-shaped association between temperature and outdoor PA, with both very low and very high temperatures associated with lower outdoor PA, and very low temperatures leading to greater PA reduction[37]. Cold weather might also be considered a barrier to PA in an American study [38, 39]. In our surveys, most participants were interviewed during late autumn and winter (from October to December) in 2010, 2015, and 2018. However, because of the expansion of CCDRFS completed in autumn of 2013, nearly 50% of participants were interviewed in early autumn (from August to October) in 2013 and about 35% of participants from new DSPs were interviewed in spring or early summer (from March to June) in 2014.
Insufficient PA levels varied considerably according to gender, age, geographical location, education, occupation, and BMI in China. We found that insufficient PA was higher for men than for women across all survey years and higher for those aged 65 or older and 18–34 than those aged 35–64. Previous studies showed a general increase in insufficient PA with advancing age in both men and women [40]. From 2010 to 2015, insufficient PA of Chinese people aged 65 or older still was higher than those aged 18–64, according to our study. However, it was worth noting that the prevalence of insufficient PA in adults aged 18–34 surpassed that of those aged 65 or older in 2018. About 50% of adults over 65 in the “Aging in Chianti” study experienced no change in average PA, and about 13% reported an increase in PA over a 3-year follow-up [41]. Therefore, the trend of insufficient PA in the elderly still needs further research. Additionally, we found that the prevalence of insufficient PA among urban residents was higher than that of rural residents, but the upward trend was more pronounced in rural areas, which had surpassed urban areas by 2018. Likewise, a previous research report also showed that insufficient PA was higher in urban residents than among men and women rural residents [42]. The difference in low MVPA also exists among people with different levels of education in our study. Similarly, a Japanese study found that men with high educational qualifications had significantly lower PA than those with lower educational qualifications [43]. In occupational groups, our study observed that unemployed people and students had the highest prevalence of insufficient PA. An Armenia study also found that unemployed people were less engaged in PA and less likely to meet WHO recommendations on PA [44]. Interestingly, the present study found that Chinese adults with a BMI < 18.5 kg/m2 had a less prevalence of PA, and others showed increased PA as their BMI increased. In accordance with the present results, previous studies have reported the lowest PA in underweight Korean adults [45]. The recent study also showed that the prevalence of insufficient PA in normal-weight people was lower than the obese individuals, and the prevalence of insufficient PA was increasing in all BMI categories [45]. Insufficient PA increases the prevalence of chronic diseases such as obesity, hypertension, and diabetes, affecting the balance of energy metabolism, muscle function, and peripheral insulin resistance [46, 47]. According to our research results, the current situation of insufficient PA in China is not optimistic and will seriously endanger the health of residents.
Besides the decline in total PA, the study also showed that fewer adults participated in work-related MVPA and that the amount of time spent on work-related MVPA decreased. Between 2004 and 2011, a study also suggested that for both adult men and women in China, work and domestic PA levels fell by nearly half, and the decline was more pronounced for women from 2004 to 2011 [48]. A study covering 104 countries in the world reported that China also has such a trend, but work-related PA was higher in low-income countries [18]. Therefore, socio-economic factors also have an important impact on PA. In the past decades, China's industrial structure has undergone significant changes. The contribution rate of the Tertiary Industry (mainly the service industry) to Gross Domestic Product (GDP) has continued to increase since the early 1980s and has surpassed both Primary (agricultural, 8.9%) and Secondary (manufacturing, 44.2%) industries since 2013 and accelerated in the following years. Meanwhile, the employed persons in primary and secondary industries continued to decline with a significant increase in the tertiary industry [49]. This may be an essential factor leading to the decline in work-related PA among Chinese residents. Moreover, the current study has shown that the mean contribution of work-related MVPA was the most in total MVPA. These results agreed with those obtained by a global study about levels of domain-specific PA [18]. We also found that the mean contribution of work-related MVPA was declining from 2010 to 2018, while the mean contribution of recreation-related was rising. This phenomenon may be a primary factor in changing domain-specific PA in China. Furthermore, a Brazilian study showed that work-related PA has a higher contribution to poorer groups [50]. In our analysis, work-related PA was significantly higher among individuals living in rural residences than those living in urban residences, confirming the conclusion from the side. Additionally, research suggested that more work-related PA was associated with poorer physical health and a greater risk of early death [51]. As such, work-related PA might not have the same benefits to health and well-being as other domain-specific, particularly recreation. Despite this, global PA guidelines encourage adults to be active during any life domain, including leisure time, transport, occupational, and household chores PA [52]. After all, sedentary behaviors at work can also lead to health risks [53]. An increasing trend in recreation-related MVPA was found in our research, which means more adults participated in the leisure time PA. Andreas et al. found higher recreation-related PA associated with reduced cardiovascular disease and all-cause mortality risk, while higher work-related PA was associated with increased risks, independent of each other [53]. Thus, the current trend of recreation-related PA in China is beneficial to the health of residents.
The world and nations have already formulated some PA policies. For example, the “Global Recommendations on Physical Activity for Health” published by WHO was to guide decision-makers at the national and regional levels [54]. Whereafter, China also published “Several Opinions on Accelerating the Development of the Sports Industry and Promoting Sports Consumption” in 2014 [55] and the Outline of the “Healthy China 2030” Plan in 2016 [56], to make fitness for all people a national strategy, and improve people's physical fitness. Our study found that the trend of recreation-related PA was relatively optimistic, which may be attributed to the above policies. However, it is worth noting that the total insufficient PA was increasing in China, especially with the obvious decline in work-related PA.
Our study reported the trend of insufficient PA from 2010 to 2018, which could not reflect the change caused by the global pandemic in 2019. The global pandemic occurred and disrupted daily behavior patterns possibly. Results of a meta-analysis showed that a downward trend in PA was observed in adults from Italy, the United States, China, Japan, Spain, Singapore, and South Korea during the global pandemic[57]. A study of New Zealand during the pandemic also showed a significant reduction in participation in PA during the lockdown from June 2020 to April 2021, which may have an impact on subsequent health outcomes and related intervention programs[58]. Until now, no studies addressing the impact of the pandemic on PA among adults nationwide in China have been reported. We look forward to the next round of CCDRFS and future analysis of changes in insufficient PA after the global pandemic.
Strengths and limitations
Our study used multiple large nationally representative health survey data, and a total of 645 903 adults were included from 2010 to 2018, measured using the GPAQ, to describe PA trends in China. Also, the response rates in all four surveys were high, and the sampling ensured that the samples were representative of the general population in China. However, our study also has limitations. First, the PA in this study was self-reported, which was not as accurate as measured by objective instruments. When comparing the GPAQ with accelerometers and pedometers, it was found that the GPAQ data had poor concurrent validity[31]. In our research, the GPAQ was conducted in face-to-face interviews, which have excellent reliability and validity and have been widely used worldwide [25, 59], and the interviewers have received professional training. The phenotypic agreement was generally good between subjective and objective measures of insufficient PA [54, 55]. Also, it is hard to use accelerometers and other instruments to measure attitude activities in large-scale epidemiological investigations. Second, we adopted a replacement method to obtain a sufficient sample size. This sampling method was reasonable, considering that selecting replacement households when sampling was common in epidemiology studies. It was also applied in previous studies in China [60, 61] and other countries [62, 63]. The characteristics of the participants without replacement and after replacement in each CCDRFS survey were generally comparable. Therefore, the impact of replacement on the research results might be ignored. Finally, this study only described the trend of insufficient PA from 2010 to 2018 and did not explore the relationship between insufficient PA and chronic diseases. In the future, we will further conduct in-depth research on the relationship between insufficient PA and chronic non-communicable diseases.
Conclusions
In conclusion, although the situation of recreation-related MVPA had gradually improved in the past nine years, work-related and transport-related MVPA continued to decline, resulting in an increase in overall insufficient PA among Chinese adults from 2010 to 2018. Our research provides strong new evidence for the evolving insufficient PA epidemic among adults in China. PA is needed to be integrated into different areas of people's daily work, transport, and recreation. Moreover, the implementation of increasing PA will lower the incidence of chronic non-communicable diseases (NCDs), cancer, and other diseases, thus reducing mortality. Policies that support decreasing insufficient PA can also provide benefits for health, wealth, employment, and environmental sustainability. China will have a hopeful future only if the country implements strong actions against insufficient PA.
Availability of data and materials
Individual participant data in our study will not be made available publicly. For further detailed data access policy and procedure, please contact jianceshi@ncncd.chinacdc.cn.
Abbreviations
- PA:
-
Physical activity
- NCDs:
-
Non-communicable diseases
- MVPA:
-
Moderate- to vigorous-intensity physical activity
- CCDRFS:
-
China Chronic Disease and Risk Factor Surveillance
- BMI:
-
Body mass index
- China CDC:
-
Chinese Center for Disease Control and Prevention
- DSPs:
-
Disease Surveillance Points
- PPS:
-
Proportional to population size
- SRS:
-
Systematic random sampling
- NCNCD:
-
National Center for Chronic and Noncommunicable Disease Control and Prevention
- GPAQ:
-
Global Physical Activity Questionnaire
- WHO:
-
World Health Organization
- GDP:
-
Gross Domestic Product
References
Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, Carty C, Chaput JP, Chastin S, Chou R, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451–62.
WHO. Global Action Plan for the Prevention and Control of NCDs 2013-2020. 2013. https://www.who.int/publications/i/item/9789241506236. Accessed 28 Jun 2021.
Borjesson M, Onerup A, Lundqvist S, Dahlof B. Physical activity and exercise lower blood pressure in individuals with hypertension: narrative review of 27 RCTs. Br J Sports Med. 2016;50(6):356–61.
Hills AP, Arena R, Khunti K, Yajnik CS, Jayawardena R, Henry CJ, Street SJ, Soares MJ, Misra A. Epidemiology and determinants of type 2 diabetes in south Asia. Lancet Diabetes Endocrinol. 2018;6(12):966–78.
Kerr J, Anderson C, Lippman SM. Physical activity, sedentary behaviour, diet, and cancer: an update and emerging new evidence. Lancet Oncol. 2017;18(8):e457–71.
Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Lancet Physical Activity Series Working G: Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219–29.
Shiri R, Lallukka T, Rahkonen O, Leino-Arjas P. Excess Body mass and leisure time physical activity in the incidence and persistence of chronic pain. Pain Med. 2020;21(11):3094–101.
Simoes EJ, Mariotti S, Rossi A, Heim A, Lobello F, Mokdad AH, Scafato E. The Italian health surveillance (SiVeAS) prioritization approach to reduce chronic disease risk factors. Int J Public Health. 2012;57(4):719–33.
Van Blarigan EL, Meyerhardt JA. Role of physical activity and diet after colorectal cancer diagnosis. J Clin Oncol. 2015;33(16):1825–34.
Organization GWH: WHO guidelines on physical activity and sedentary behaviour. https://www.who.int/publications/i/item/9789240015128. Accessed 28 Jun 2021.
Ding D, Lawson KD, Kolbe-Alexander TL, Finkelstein EA, Katzmarzyk PT, van Mechelen W, Pratt M. The economic burden of physical inactivity: a global analysis of major non-communicable diseases. Lancet. 2016;388(10051):1311–24.
Althoff T, Sosič R, Hicks JL, King AC, Delp SL, Leskovec J. Large-scale physical activity data reveal worldwide activity inequality. Nature. 2017;547(7663):336–9.
Oja P, Titze S. Physical activity recommendations for public health: development and policy context. EPMA J. 2011;2(3):253–9.
Stamatakis E, Gale J, Bauman A, Ekelund U, Hamer M, Ding D. Sitting time, physical activity, and risk of mortality in adults. J Am Coll Cardiol. 2019;73(16):2062–72.
Dillon CB, McMahon E, O’Regan G, Perry IJ. Associations between physical behaviour patterns and levels of depressive symptoms, anxiety and well-being in middle-aged adults: a cross-sectional study using isotemporal substitution models. BMJ Open. 2018;8(1): e018978.
Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. 2018;6(10):e1077–86.
Samitz G, Egger M, Zwahlen M. Domains of physical activity and all-cause mortality: systematic review and dose-response meta-analysis of cohort studies. Int J Epidemiol. 2011;40(5):1382–400.
Strain T, Wijndaele K, Garcia L, Cowan M, Guthold R, Brage S, Bull FC. Levels of domain-specific physical activity at work, in the household, for travel and for leisure among 327 789 adults from 104 countries. Br J Sports Med. 2020;54(24):1488–97.
Bauman A, Ma G, Cuevas F, Omar Z, Waqanivalu T, Phongsavan P, Keke K, Bhushan A. Cross-national comparisons of socioeconomic differences in the prevalence of leisure-time and occupational physical activity, and active commuting in six Asia-Pacific countries. J Epidemiol Community Health. 2011;65(1):35–43.
White RL, Babic MJ, Parker PD, Lubans DR, Astell-Burt T, Lonsdale C. Domain-specific physical activity and mental health: a meta-analysis. Am J Prev Med. 2017;52(5):653–66.
Tan X, Liu X, Shao H. Healthy China 2030: a vision for health care. Value Health Reg Issues. 2017;12:112–4.
Li B. Tutorial for Outline of the Healthy China 2030 plan. Beijing: People's Medical Publishing House; 2020.
Zhang M, Wang L, Wu J, Huang Z, Zhao Z, Zhang X, Li C, Zhou M, Wang L. Data Resource Profile: China Chronic Disease and Risk Factor Surveillance (CCDRFS). Int J Epidemiol. 2022;51(2):e1–8.
Liu S, Wu X, Lopez AD, Wang L, Cai Y, Page A, Yin P, Liu Y, Li Y, Liu J, et al. An integrated national mortality surveillance system for death registration and mortality surveillance China. Bull World Health Organ. 2016;94(1):46–57.
Yang G, Hu J, Rao KQ, Ma J, Rao C, Lopez AD. Mortality registration and surveillance in China: History, current situation and challenges. Popul Health Metr. 2005;3(1):3.
Skinner CJ: Probability Proportional to Size (PPS) Sampling. In: Wiley StatsRef: Statistics Reference Online. edn.: 1–5. Accessed 28 Dec 2020.
Kish L, Frankel MR. Inference from Complex Samples. J Roy Stat Soc: Ser B (Methodol). 1974;36(1):1–22.
Korostovtseva L, Alieva A, Rotar O, Bochkarev M, Boyarinova M, Sviryaev Y, et al. Sleep Duration, Lipid Profile and Insulin Resistance: Potential Role of Lipoprotein(a). Int J Mol Sci. 2020;21(13):4680.
Armstrong T, Bull F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J Public Health. 2006;14(2):66–70.
WHO. Global physical activity questionnaire (GPAQ). 2021. [https://www.who.int/publications/m/item/global-physical-activity-questionnaire] Accessed 28 Dec 2020.
Keating XD, Zhou K, Liu X, Hodges M, Liu J, Guan J, et al. Reliability and Concurrent Validity of Global Physical Activity Questionnaire (GPAQ): A Systematic Review. Int J Environ Res Public Health. 2019;16(21):4128.
Yao P-L, Laurencelle L, Trudeau F. Former athletes’ lifestyle and self-definition changes after retirement from sports. J Sport Health Sci. 2020;9(4):376–83.
Organization WH. Global recommendations on physical activity for health. 2010.
Obesity. preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i-xii, 1-253.
Qian J. Variance Estimation With Complex Data and Finite Population Correction—A Paradigm for Comparing Jackknife and Formula〣ased Methods for Variance Estimation. ETS Res Rep Ser. 2020;(1):1–16.
Tucker P, Gilliland J. The effect of season and weather on physical activity: a systematic review. Public Health. 2007;121(12):909–22.
Ho JY, Lam HYC, Huang Z, Liu S, Goggins WB, Mo PKH, Chan EYY. Factors affecting outdoor physical activity in extreme temperatures in a sub-tropical Chinese urban population: an exploratory telephone survey. BMC Public Health. 2023;23(1):101.
King AC, Castro C, Wilcox S, Eyler AA, Sallis JF, Brownson RC. Personal and environmental factors associated with physical inactivity among different racial-ethnic groups of U.S. middle-aged and older-aged women. Health Psychol. 2000;19(4):354–64.
Wilcox S, Castro C, King AC, Housemann R, Brownson RC. Determinants of leisure time physical activity in rural compared with urban older and ethnically diverse women in the United States. J Epidemiol Community Health. 2000;54(9):667–72.
Granic A, Davies K, Dodds RM, Duncan R, Uwimpuhwe G, Pakpahan E, Robinson S, Sayer AA. Factors associated with change in self-reported physical activity in the very old: the Newcastle 85+ study. PLoS One. 2019;14(7): e0218881.
Martinez-Gomez D, Bandinelli S, Del-Panta V, Patel KV, Guralnik JM, Ferrucci L. Three-year changes in physical activity and decline in physical performance over 9 years of follow-up in older adults: The Invecchiare in Chianti Study. J Am Geriatr Soc. 2017;65(6):1176–82.
Ding L, Liang Y, Tan ECK, Hu Y, Zhang C, Liu Y, Xue F, Wang R. Smoking, heavy drinking, physical inactivity, and obesity among middle-aged and older adults in China: cross-sectional findings from the baseline survey of CHARLS 2011–2012. BMC Public Health. 2020;20(1):1062.
Matsushita M, Harada K, Arao T. Socioeconomic position and work, travel, and recreation-related physical activity in Japanese adults: a cross-sectional study. BMC Public Health. 2015;15:916.
Tcymbal A, Andreasyan D, Whiting S, Mikkelsen B, Rakovac I, Breda J. Prevalence of physical inactivity and sedentary behavior among adults in Armenia. Front Public Health. 2020;8:157.
Sung H, Kim G, Ma X, Choe H, Han Y, Yoon J, et al. Physical Activity Trends in Korean Adults from Korea National Health and Nutritional Examination Survey from 2014 to 2019. Int J Environ Res Public Health. 2022;19(9):5213.
Andersen E, Kjellså I, Hjellset VT, Henjum S. Insufficient physical activity level among Sahrawi adults living in a protracted refugee setting. BMC Public Health. 2021;21(1):166.
Xiao Q, Moore SC, Keadle SK, Xiang Y-B, Zheng W, Peters TM, Leitzmann MF, Ji B-T, Sampson JN, Shu X-O, et al. Objectively measured physical activity and plasma metabolomics in the Shanghai Physical Activity Study. Int J Epidemiol. 2016;45(5):1433–44.
Zang J, Ng SW. Age, period and cohort effects on adult physical activity levels from 1991 to 2011 in China. Int J Behav Nutr Phys Act. 2016;13:40.
National Data. [https://data.stats.gov.cn/english/easyquery.htm?cn=C01] Accessed 28 Jun 2021.
da Silva ICM, Mielke GI, Bertoldi AD, Arrais PSD, Luiza VL, Mengue SS, Hallal PC. Overall and Leisure-Time Physical Activity Among Brazilian Adults: National Survey Based on the Global Physical Activity Questionnaire. J Phys Act Health. 2018;15(3):212–8.
Coenen P, Huysmans MA, Holtermann A, Krause N, van Mechelen W, Straker LM, van der Beek AJ. Do highly physically active workers die early? A systematic review with meta-analysis of data from 193 696 participants. Br J Sports Med. 2018;52(20):1320–6.
WHO Guidelines Approved by the Guidelines Review Committee. In: Global Recommendations on Physical Activity for Health. edn. Geneva: World Health Organization Copyright © World Health Organization 2010.; 2010.
Huang Y, Benford S, Blake H. Digital Interventions to Reduce Sedentary Behaviors of Office Workers: Scoping Review. J Med Internet Res. 2019;21(2): e11079.
WHO. Global recommendations on physical activity for health [https://www.who.int/publications/i/item/9789241599979] Accessed 25 Jan 2021.
State Council Gazette Issue No. 30 Serial No. 1497 (October 30, 2014) [http://english.www.gov.cn/archive/publications/2014/11/02/content_281475004473784.htm] Accessed 28 Jun 2021.
State Council Gazette Issue No. 32 Serial No. 1571 (Nov 20, 2016) [http://english.www.gov.cn/archive/state_council_gazette/2016/11/20/content_281475495544980.htm] Accessed 28 Jun 2021.
Wunsch K, Kienberger K, Niessner C. Changes in Physical Activity Patterns Due to the Covid-19 Pandemic: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2022;19(4):2250.
Wilson OWA, McEwen H, Kelly P, Richards J. Declines in Physical Activity among New Zealand Adults during the COVID-19 Pandemic: Longitudinal Analyses of Five Data Waves from Pre-Pandemic through April 2021. Int J Environ Res Public Health. 2022;19(7):4041.
Frankel KMR. Inference from Complex Samples (with Discussion). J Roy Stat Soc. 1974;36(1):1–37.
Qian J, Cai M, Gao J, Tang S, Xu L, Critchley JA. Trends in smoking and quitting in China from 1993 to 2003: National Health Service Survey data. Bull World Health Organ. 2010;88(10):769–76.
Wang L, Gao P, Zhang M, Huang Z, Zhang D, Deng Q, Li Y, Zhao Z, Qin X, Jin D, et al. Prevalence and Ethnic Pattern of Diabetes and Prediabetes in China in 2013. JAMA. 2017;317(24):2515–23.
Nguyen TT, Nguyen XX, Ronse M, Nguyen QT, Ho PQ, Tran DT, Gerrets R, Thriemer K, Ley B, Marfurt J et al. Diagnostic practices and treatment for in the interethnic therapeutic encounter of South-Central Vietnam: a mixedmethods study. Pathogens. 2020;10(1):26.
Obi E, Okoh F, Blaufuss S, Olapeju B, Akilah J, Okoko OO, Okechukwu A, Maire M, Popoola K, Yahaya MA, et al. Monitoring the physical and insecticidal durability of the long-lasting insecticidal net DawaPlus 2.0 in three States in Nigeria. Malar J. 2020;19(1):124.
Acknowledgements
This work was supported by the National Key R&D Program of China (grant numbers 2018YFC1311702, 2018YFC131170), the grant from the Central to Local Fiscal Transfer Payment Program of China (CCDRFS 2010), and the National Major Public Health Service Project (CCDRFS 2013/15/2018). The sponsors had no role in the study's design, collection, analysis, interpretation of data, or writing the manuscript.
We thank all staff from 31 provincial Centers for Disease Control and Prevention and local Centers for Disease Control and Prevention involved in every survey to collect data and their efforts in quality control. We are also indebted to all the study participants for their participation and contribution.
Funding
This work was partly supported by a research grant from the National Key R&D Program (2018YFC1311702 and 2018YFC1311706). The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
MeiZ did the statistical analysis, supervised by LimW. YM and MeiZ wrote the manuscript, supervised by LimW and DW. All authors contributed to the data interpretation, revised each draft for important intellectual content, and read and approved the final manuscript. MeiZ and YM contributed equally as first co-authors. MaiZ, DW, and LimW contributed equally as corresponding co-authors.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The CCDRFS 2015 (No.201519-B) has been approved by the Ethical Committee of the Chinese Center for Disease Control and Prevention (China CDC). All other CCDRFS surveys (No.201010, No.201307, No.201819) were approved by the Ethical Committee of the National Center for Chronic and Noncommunicable Disease Control and Prevention (NCNCD), China CDC. The Ethical Committee of the NCNCD approved this study to analyze all CCDRFS data (202019). All participants have signed informed consent to participate.
Consent for publication
Not applicable.
Competing interests
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix2.
Data collection of CCDRFS 2010-18. Appendix 3. Analysis plan. Appendix 4.Global Physical Activity Questionnaire. Appendix 5. List of the typical physical activities. Appendix figure 1. Map of China Chronic Disease and Risk Factor Surveillance (CCDRFS) Sites. Appendix figure 2. Percentages of participants interviewed by month and survey. Appendix table 1. Trends in insufficient physical activity in urban and rural adults in China, 2010-18.Appendix table 2. Trends in adults undertaking 150-299 min/week of MVPA in China, 2010 -18. Appendix table 3. Trends in percentages of adults participating in domain-specific MVPA in China, 2010-18.Appendix table 4. Trends in mean min/week of domain-specific MVPA among adults in China, 2010-18. Appendix table 5. Mean domain-specific relative contribution to total MVPA among adults in China, 2010-18. Appendix table 6. Trends in percentages of adults without intensity-specific MVPA in China, 2010-18.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, M., Ma, Y., Xie, X. et al. Trends in insufficient physical activity among adults in China 2010–18: a population-based study. Int J Behav Nutr Phys Act 20, 87 (2023). https://doi.org/10.1186/s12966-023-01470-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12966-023-01470-w