
Abstract
All-trans retinoic acid (ATRA) is the most relevant and functionally active metabolite of Vitamin-A. From a therapeutic standpoint, ATRA is the first example of pharmacological agent exerting its anti-tumor activity via a cell differentiating action. In the clinics, ATRA is used in the treatment of Acute Promyelocytic Leukemia, a rare form of myeloid leukemia with unprecedented therapeutic results. The extraordinary effectiveness of ATRA in the treatment of Acute Promyelocytic Leukemia patients has raised interest in evaluating the potential of this natural retinoid in the treatment of other types of neoplasias, with particular reference to solid tumors.
The present article provides an overview of the available pre-clinical and clinical studies focussing on ATRA as a therapeutic agent in the context of breast cancer from a holistic point of view. In detail, we focus on the direct effects of ATRA in breast cancer cells as well as the underlying molecular mechanisms of action. In addition, we summarize the available information on the action exerted by ATRA on the breast cancer micro-environment, an emerging determinant of the progression and invasive behaviour of solid tumors. In particular we discuss the recent evidences of ATRA activity on the immune system. Finally, we analyse and discuss the results obtained with the few ATRA-based clinical trials conducted in the context of breast cancer.
Graphical Abstract

Similar content being viewed by others


Background
Vitamin-A consists of a group of organic compounds that includes retinol, retinal (also known as retinaldehyde), retinoic acid and several carotenoids [1, 2]. In humans, Vitamin-A is an essential nutrient and a fundamental component of standard diets. Vitamin-A is involved in numerous homeostatic functions, including the regulation of embryonic development as well as the maintenance of the immune system and vision in the adult [3, 4]. All-trans retinoic acid (ATRA) is considered to be the most relevant and functionally active metabolite of Vitamin-A [5]. In APL (Acute Promyelocytic Leukemia), ATRA is a standard component of the therapeutic regimen(s) which is used in the treatment of this rare type of myeloid leukemia. In this pathological context, therapeutic doses of ATRA restore the granulocytic differentiation program which is blocked in the leukemic blast, via an incompletely defined mechanism, which involves the degradation of the oncogenic fusion product deriving from a translocation involving chromosomes 15/17 and is known as PML-RARα [6]. As RARα (Retinoic Acid Receptor alpha) is one of the nuclear receptors mediating the transcriptomic effects exerted by ATRA, the retinoid represents the first example of targeted anti-tumor agent showing therapeutic efficacy. The exceptional results obtained in APL has spurred interest in the evaluation of ATRA potential as a therapeutic agent in neoplastic diseases other than this myeloid leukemia, with particular reference to solid tumors such as breast cancer. In the present review article, we provide a brief summary of the pre-clinical and clinical data available in the literature on various issues relating to the anti-tumor activity of ATRA in mammary tumors. It is expected that the present review article may be of use in filling the gap between the available evidence on the therapeutic potential of ATRA in breast cancer as well as other solid tumors and the design of ATRA-based therapeutic strategies of clinical relevance.
ATRA metabolism and signaling
The current section of the review provides information on the metabolism and signaling of ATRA that is of relevance to understand the molecular mechanisms underlying the anti-tumor action of the retinoid.
ATRA up-take and metabolism in the normal and neoplastic cell
Even if nanomolar concentrations of ATRA have been detected in the bloodstream, the main source of intra-cellular ATRA is represented by serum retinol [7]. Circulating retinol is present in the bloodstream under the form of a complex with RBP4 (Retinol Binding Protein 4) and TTR (Transthyretin). The concentration of retinol which can be determined in the circulating blood is in the low μM range [2]. Given the lipophilic nature of retinol and retinoid derivatives, the uptake of most of Vitamin-A metabolites occurs via diffusion through the plasma membrane. In some tissues, including breast cancer, the retinol/RBP4 complex can be internalized into the cell via a plasma membrane protein known as STRA6 (Signaling Receptor And Transporter of Retinol STRA6) [8].
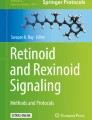
RBP4- and TTR-bound retinol are uptaken by the normal and the neoplastic cell (Fig. 1). Once inside the cell, retinol is converted into ATRA by a two step-reaction. In the first step, RDHs (Retinol Dehydrogenases) or ADHs (Alcohol Dehydrogenases) metabolize retinol into retinaldehyde and these enzymatic reactions are reversible. This is followed by the irreversible oxidation of retinaldehyde into ATRA which is carried out by RALDHs (Retinaldehyde Dehydrogenases) [1]. Since all retinol derivatives are lipophilic, as mentioned above, these molecules are present in the cytosol under the form of complexes with specific binding proteins. Indeed, eukaryotic cells contain different intracellular proteins capable of binding ATRA, retinol and/or retinaldehyde. Newly synthetized ATRA interacts with CRABPI or CRABPII (Cytosolic Retinoic Acid Binding Protein I and II), two well-known cytosolic proteins. In general, CRABPI is considered to promote ATRA degradation, while CRABPII is believed to translocate ATRA into the nucleus where it binds RARs and RXRs (Retinoid X Receptors), which are ligand-dependent transcription factors belonging to the family of SNRs (Steroid Nuclear Receptors). ATRA degradation is carried out by a few Cytochrome P-450 Hydrolases (CYP26A1, CYP26B1 and CYP26C1) and the process plays a major role in the control of the intracellular levels of the retinoid. The homeostatic concentrations of intracellular ATRA fall within the low nanomolar range [2]. In physiological conditions, the presence of such endogenous concentrations of ATRA is of fundamental importance for the maintenance of Vitamin-A dependent gene-expression and signaling. In terms of activity on target cells, ATRA can exert its physiological action in both an autocrine and a paracrine manner [9].

ATRA uptake inside the cell and intra-cellular mechanism of action. Dietary Vitamin-A is released into the blood as retinol which is complexed to RBP4 (Retinol Binding Protein 4). The cellular uptake of retinol is mediated by STRA6 (Stimulated by Retinoic Acid 6). Intracellular retinol is either stored as an ester or further oxidized into retinaldehyde by ADHs (Alcohol Dehydrogenases) or RDHs (Retinol Dehydrogenases). Retinaldehyde is further transformed into ATRA by RALDHs (Retinaldehyde Dehydrogenases). In the cytosol, ATRA can be transported to the nucleus by CRABP2 (Cellular Retinoic Acid Binding Protein 2) or by FABP5 (Fatty Acid Binding Protein 5). By converse, ATRA is targeted to degradation by CRABP1 (Cellular Retinoic Acid Binding Protein 2). In the nucleus, ATRA binds to one of the indicated SNRs (Steroid Nuclear Receptors) generating an active transcriptional complex which interacts with the DNA regulatory regions of target genes containing RAREs (Retinoic Acid Responsive Elements) or PPREs (Peroxisome Proliferator Responsive Elements). In breast cancer cells, ATRA binding to the SNR heterodimers RAR/RXR (Retinoic Acid Receptor/Retinoic X receptor) triggers growth inhibitory/differentiating effects while ATRA binding to PPAR/RXR heterodimers (Peroxisome Proliferator Activated Receptor) sustains proliferation. ATRA exerts non-genomic effects via interactions with membrane bound RARs. These interactions activate MAP-kinase cascades which concur to the activation of RARE dependent target genes. Retinol bound RBP4 can also trigger intra-cellular signals by activating the STAT3/STAT5 transcription factors
ATRA intracellular signaling
ATRA intracellular signaling occurs via genomic and non-genomic pathways. In the classical genomic pathway, ATRA acts as a ligand for transcription factors complexes that activate/repress a plethora of target genes [5]. ATRA exerts also many non-genomic effects, which include the activation of various kinase signaling pathways [10] (Fig. 1).
In the classical genomic pathway, the six SNRs, RARα, RARβ, RARγ, RXRα, RXRβ and RXRγ are believed to mediate the vast majority of ATRA-dependent transcriptional effects. The transcriptionally active forms of these SNRs consist of different RAR/RXR heterodimers in which RAR acts as the ATRA ligand-binding moiety. The ligand bound RAR/RXR heterodimers interact with RARE (Retinoic Acid Responsive Element) DNA sequences, which are generally located in the promoter region of retinoid target genes. ATRA binding to RARs generates a conformational change of the RAR/RXR complexes. This altered conformation modulates the association of the RAR/RXR heterodimers with the corresponding co-repressors/co-activators and it drives the epigenetic modifications which govern target gene transcription [10, 11]. The fundamental role of RARs in ATRA signaling is supported by a recent study based on the use of the CRISPR/CAS9 strategy and aimed at silencing RARs in murine embryonic stem cells [12]. The results obtained demonstrate that RARs are essential for the regulation of all the transcripts whose expression is controlled by ATRA. Besides RARs, ATRA is known to bind and modulate the transcriptional activities of other members of the NR family, including PPARβ-δ (Peroxisome Proliferator-Activator Receptor β/δ [13], RORβ/NR1F2 (RAR-related Orphan Receptor Beta or Nuclear Receptor 1F2 [14], COUP-TFII/NR2F2 (Chicken Ovalbumin Upstream Promoter-Transcription Factor II or Nuclear Receptor 2F2 [15] and TR4/NR2C2 (Testicular Receptor 4 or Nuclear Receptor 2C2 [16]. In breast cancer, ATRA-liganded RAR/RXR heterodimers are purported to mediate growth inhibition, whereas the PPARβ-δ/RXR heterodimer is believed to induce proliferation [13, 17]. ATRA is transported to the nucleus by the above mentioned CRABP2 and the FABP5 (Fatty Acid Binding Protein 5) cytosolic receptors. While CRABP2 delivers ATRA to the RAR/RXR heterodimers, the retinoid is delivered to the PPARβ-δ/RXR heterodimer by FABP5 [13]. The relative intracellular levels of CRABP2 and FABP5 determine the net effect of ATRA on cell proliferation.
The non-genomic signaling pathway of ATRA involves the activation of two complex intracellular processes. The first process involves the activation of specific protein kinases which lead to a cascade of post-transcriptional modifications of RARs as well as the corresponding co-repressors, co-activators and chromatin remodeling targets [18]. This results in fine-tuning of the transcriptional effects exerted by ATRA on retinoid target genes. Interestingly, a proportion of the various RAR proteins associates with the membrane lipid rafts and it is supposed to activate different types of kinases depending upon the cellular context. For instance, in some epithelial cells, including breast cancer cells and tumor associated fibroblasts, ATRA binding of plasma membrane RARα activates the p38MAPK (p38 Membrane Associated Protein Kinase). In this situation, ATRA bound RARα has been shown to interact with the G-protein αq subunit, which supports MAPK activation resulting from the engagement of upstream signaling cascades, such as those triggered by Rho GTPases [19]. In neuronal cells, ATRA stimulation of plasma membrane associated RAR(s) activates the p42/p44 MAPK [18]. In this cellular context, ATRA stimulated MAPKs trigger MSK1 (Mitogen and Stress-activated Protein Kinase-1) phosphorylation and translocation into the nucleus, where the protein is recruited to the promoters of retinoid target genes and it modulates transcription. Another ATRA-dependent non-genomic process involves the activation of the JNK2 (Janus Kinase 2)/STAT3-STAT5 (Signal Transducer and Activator of Transcription 3 and 5) signaling pathway via the STRA6 (Signaling Receptor And Transporter of Retinol) transporter. Indeed, STRA6 is not only a retinol transporter, but it is also a signaling receptor, which can be activated by retinol-bound RBP4. In this context, RBP4 mediated retinol transport induces the phosphorylation of STRA6, which results in the activation of the JAK2/STAT3–5 signaling cascade causing the induction of STAT target genes [20]. STRA6-mediated retinol transport and cell signaling are inter-dependent and they both rely on intracellular retinol trafficking and metabolism. Hence, STRA6 associates Vitamin-A homeostasis and metabolism to cell signaling, which results in the control of important biological functions such as insulin responsiveness [21].
Direct effects of ATRA on breast cancer cells
The present chapter of the review aims at providing a brief summary of what is known in terms of the direct effects exerted by ATRA on the neoplastic cell, taking into consideration the results obtained in breast cancer.
Anti-proliferative action of ATRA
Many studies describe the effects of ATRA on breast cancer cell lines and breast cancer mouse models [5]. In general, ATRA is reported to exert an inhibitory effect on the growth of the mammary tumor cell. In cell lines, ATRA triggers a growth arrest which is not associated with massive cytotoxic effects [22, 23]. Indeed, in the majority of the cell lines considered, apoptosis is only a late and secondary effect induced by ATRA [24]. Significantly, a considerable reduction in the growth of tumor cells is also observed in mice bearing xenografts of breast cancer cells [22, 23]. As to the RAR/RXR isoforms mediating the anti-proliferative action of ATRA, the data available are in line with a major involvement of RARα. In fact, in culture of different breast cancer cell lines, RARα silencing impairs the anti-proliferative activity of ATRA [22, 25]. In addition, transgenic mice characterized by the MMTV (Mouse Mammary Tumor Virus) dependent expression of a dominant-negative RARα mutant, which is characterized by a defective ligand binding domain (RARαG303E), develop metastatic mammary adenocarcinomas [26]. Finally, the role played by RARα in mediating the anti-proliferative action of ATRA in breast cancer is supported by studies performed with RARα specific agonists. Indeed, in both cell cultures and mouse models of mammary tumors, ATRA-induced growth inhibition is recapitulated only by the RARα agonist AM580, as RARβ and RARγ agonists are generally ineffective in terms of anti-proliferative effects [22, 27,28,29,30].
In breast cancer, the anti-proliferative activity of ATRA is observed predominantly in tumors characterized by a luminal and ER+ (Estrogen Receptor positive) phenotype, while the basal and HER2+ (Human Epidermal Growth Factor Receptor 2 positive) subtypes of this neoplastic disease are generally resistant to the retinoid [22, 31, 32]. The observation is supported by ATRA-sensitivity studies performed on ER+ breast cancer cell lines and it is consistent with the demonstrated crosstalk between ERα (Estrogen Receptor alpha) and RARα. Indeed, RARα is known to be a direct ERα target gene, which is induced upon estrogen treatment of breast cancer cells [33, 34]. In this cellular context, chip-seq studies indicate that the DNA binding of RAR and ERα throughout the genome is highly coincident and this coincidence is at the basis of a widespread crosstalk between ATRA and estrogen signaling, which results in an antagonistic regulation of breast cancer-associated genes [25, 35]. In its unliganded form, RARα is part of the ERα transcriptional complex and it contributes to the proliferative activity of estrogens in ER+ breast cancer cells. Upon ligand binding, RARα acquires an opposite function and it acts as an inhibitor of estrogen target genes transcription. As already mentioned, basal and HER2 enriched ERα− negative cancer cell lines tend to be resistant to ATRA, although some exceptions to the rule are observed. For instance, ATRA exerts a significant anti-tumor action on TNBC (Triple Negative Breast Cancer) cells characterized by constitutive activation of the NOTCH1 (Neurogenic locus NOTCH Homolog protein 1) cell membrane receptor. In this cellular context, RARβ-silencing studies provide evidence that the RARα-dependent induction of RARβ contributes to ATRA sensitivity [27]. In addition, 23–32% of the human breast cancers characterized by amplification of the ERBB2 gene (the locus encoding the HER2 protein) show co-amplification of the RARα gene (RARA). Interestingly, this subtype of breast cancer shows a remarkable sensitivity to ATRA and RARα agonists, regardless of ER-positivity [23].
Among the genes known to play a relevant role in mammary tumors, BRCA1 (BReast CAncer gene 1) and PALB2 (Partner And Localizer of BRCA2), two breast cancer susceptibility genes whose mutations result in familial cases of the disease, seem to be required for RARα signaling [36]. ATRA recruits BRCA1 and PALB2 to the promoters of retinoid-responsive genes where the two proteins play an important role in the transcriptional responses to the retinoid. In the breast cancer cell line MCF-7, ATRA signaling requires BRCA1 and PALB2 for the modulation of all the retinoid regulated transcriptome including the classical retinoid-responsive HOXs (Homeobox genes) genes. In breast cancer cells, depletion of BRCA1 or PALB2 diminishes the anti-proliferative effect exerted by ATRA.
As to genes other than BRCA1 and PALB2 that may be involved in the anti-proliferative action exerted by ATRA in mammary tumors, important clues come from gene-expression and DNA-methylation studies. The gene expression studies that we performed in a large panel of breast cancer cell lines and we validated in tissue slices from breast cancer patients [37] led to the identification of numerous transcripts which are induced by ATRA. In addition, the data generated indicate that the anti-proliferative action exerted by the retinoid is proportional to the amount of induced transcriptome perturbations [37]. Transcriptomic analyses performed on these data indicate that ATRA activates signaling pathways related to: 1) cell-cycle control, such as chromatin organization and DNA repair; 2) antigen presentation; 3) interferon responses. The results obtained allowed us to develop a gene-expression signature which predicts the anti-proliferative response of breast cancer to ATRA [32]. Similar types of studies aimed at assessing the DNA methylation status of TNBC cells led to the identification of over 1400 sites, which are differentially methylated in ATRA-resistant relative to ATRA-sensitive cell lines. The methylation profile generated from these data is proposed as a predictor of ATRA anti-proliferative activity in TNBC [38].
Cell-differentiating action of ATRA
ATRA is the first example of therapeutically useful differentiating agent and it stimulates the expression of differentiation markers in various types of cancer cells. With respect to this, ATRA has been shown to reverse the process of EMT (Epithelial-to-Mesenchymal Transition) in different cell lines originating from solid tumors. ATRA seems to reverse EMT by restoring the expression of E-cadherin, by downregulating the expression of Vimentin and by increasing cell-to-cell interactions [39,40,41]. In addition, ATRA has been reported to inhibit cancer cell invasion and metastasis in a variety of tumor types [42].
In breast cancer, the subpopulations of LEP (Luminal EPithelial) and MEP (MyoEPhitelial) mammary cells respond to ATRA in a different manner, as indicated by the results obtained in the model represented by the bi-cellular LM38-LP murine mammary adenocarcinoma cell line. Indeed, the LEP subpopulation responds with an increase in cell-cycle arrest and apoptosis. By converse, the MEP subpopulation responds with an induction of the senescence and adhesion processes, which results in a decrease of the cell invasive capacity [42]. In agreement with this last finding, a screening of organic molecules based on the immortalized breast mesenchymal cell line, NAMEC, led to the identification of ATRA and its synthetic analog, TTNPB (a potent and selective pan-RAR agonist), as pharmacological inducers of the MET (Mesenchymal to Epithelial Transition) process [43]. Indeed, the authors demonstrate that the two retinoids switch breast cancer cells from a mesenchymal state to an epithelial/luminal like state, causing a reduction of the metastatic potential. In this situation, no effect of ATRA or TTNPB on cell proliferation is observed.
In the in vitro model of tumor progression represented by the MCF10F cell line, ATRA re-differentiates early-stage transformed cells (restoring the branching phenotype in 3D cultures), while the retinoid is ineffective, when cells characterized by a more malignant state are considered. In this model, ATRA inhibits the expression of breast cancer-associated genes [44]. In immortalized mammary tumor cells, it is interesting to notice that ATRA exposure inhibits EMT, while RARα overexpression exerts an opposite effect on the process. In the breast cancer model represented by MCF10A cells, RARα overexpression disrupts the normal acinar structure of the 3D cultures, inducing features of the EMT status [45].
ATRA induces an epithelial differentiation pathway in the HER2+ SKBR3 and UACC812 cell lines, which are characterized by the co-amplification of the ERBB2 and RARA genes. Tight and adherens junctions are formed or reorganized in SKBR3 cells as a result. Moreover, in this cell line the retinoid inhibits migration triggered by the well-known EMT inducers EGF (Epithelial Growth Factor) and Heregulin-1 [27]. Finally, it is interesting to notice that exposure of SKBR3 cells to ATRA stimulates the expression of VE-cadherin and other endothelial genes. The observation suggests that ATRA can induce the trans-differentiation of cancer cells towards an endothelial-like phenotype which may be of significance for the homeostasis of the tumor vasculature [46, 47].
ATRA and breast cancer cell metabolism
Cancer cells have to rely on metabolic adaptation to sustain proliferation and the consequent biomass production. Increasing evidence supports the idea that specific genetic and epigenetic alterations in cancer cells are required to maintain a pro-anabolic state of their metabolism [48].
On one hand, ATRA is expected to interfere with cancer cells metabolic pathways as a consequence of its ability to affect the proliferation and the differentiation state of ATRA sensitive cancer cells. On the other hand, ATRA itself is a metabolite of the retinol metabolic pathway.
In the NB4 model of APL disease, ATRA-induced differentiation of the leukemic blasts causes metabolic reprogramming. Indeed, the retinoid activates aerobic glycolysis and it reduces OXPHOS-dependent ATP production [49]. Similarly in breast cancer cells, transcriptomic analysis identifies Oxidative Phosphorylation as a Hallmark gene-set enriched for genes down-regulated by ATRA in sensitive luminal and basal cell-lines [50]. This effect is associated with a decrease in the mitochondria pool generating deficits in the respiration/energy-balance of breast-cancer cells. In breast cancer, ATRA is also known to regulate the activity of well-known oncogenes and tumour suppressors affecting cell metabolism such as AKT1 and BCL-2 [23, 48,49,50,51,52].
Along with other well-known pathways such as amino acid metabolism, arachidonic acid metabolism, fatty acid metabolism and linoleic acid metabolism, retinol metabolism stands among the metabolic pathways differentially modulated in healthy individuals versus breast cancer carriers [53]. In addition, in vitro models indicate that alterations in cellular retinol metabolism contribute to differential retinoid responsiveness in normal human mammary epithelial cells versus breast cancer cells [54, 55].
Effects of ATRA on the mammary tumor micro-environment
The present chapter of the review focusses on the information available regarding the effects exerted by ATRA on the breast cancer micro-environment, which represents an important determinant of the progression and invasiveness of solid tumors (Fig. 2).

ATRA biological effects on the tumor micro-environment
Actions of ATRA on cancer associated fibroblasts
Fibroblasts play a key role in the production of the ECM (ExtraCellular Matrix), which is a major regulator of tissue repair and influences the function of epithelial, endothelial and immune cells [56, 57]. Normal fibroblasts are suggested to exert an anti-cancer action by preventing tumor expansion. In contrast, CAFs (Cancer Associated Fibroblasts) are considered to retain a tumor-suppressive function during the early stages of tumorigenesis, while they seem to increase the growth and the invasive/metastatic properties of late-stage cancer cells. CAFs act via remodeling of the ECM and the release of signaling molecules (growth factors, cytokines, chemokines and matrix re-organizing enzymes), which support cancer cell proliferation, angiogenesis and immune escape [56, 57].
In breast cancer, fibroblast-driven retinoid signaling seems to stimulate tumor progression, as indicated by studies conducted in mouse models of ErbB2-induced mammary tumors [58]. Indeed, experimental work based on tissue recombination technologies suggests that stromal RARβ promotes mammary gland tumorigenesis. In Rarb−/− mice (RARβ-null mice), ErbB2-induced mammary tumors display a decrease in the proliferation of neoplastic cells, as well as a diminution of the angiogenetic process, the levels of collagen and the recruitment of inflammatory cells. In addition, the tumor tissues are characterized by a decrease in chemokine expression as well as an increase of the apoptotic responses observed in cancer cells. In ErbB2-induced mammary tumors, RARβ was found expressed in a subpopulation of myofibroblasts and its loss dampens their expansion and activity. Fibroblast production of CXCL12/SDF-1 was shown to promote tumor cell proliferation by the activation of the CXCR4/ErbB2 axis. It is interesting to notice that the mammary fat pads of RARβ-null mice hosting ErbB2-transformed epithelium show the presence of small in situ ductal carcinomas. The observation supports the notion that the loss of RARβ is of no significance for the tumor initiation process activated by ErbB2. By converse, the absence of RARβ reduces the capacity of the surrounding stroma to provide the necessary micro-environment for the growth and invasion of tumor cells. Noticeably, RARβ expression distinguishes the tumor associated stroma from the adjacent normal stroma in laser-dissected stromal cells obtained from a small cohort of breast cancer patients [58]. The data reported for ErbB2-induced mammary tumors were confirmed also in the case of Wnt1-induced mammary tumorigenesis [59]. In this case, the absence of RARβ changes the composition and the expression profile of the tumor stroma sustaining mesenchymal traits in the tumor cells.
The lack of cell-specific markers and the diverse origin of CAFs suggest that these fibroblasts can be heterogeneous in terms of function, which is highly dependent on the tumor context. Thus, it is not a surprise that the ATRA-dependent regulation of CAFs causes tumor suppression in neoplastic diseases other than breast cancer. Stellate cells are a peculiar type of hepatic and pancreatic fibroblasts, which are capable of storing lipid droplets as well as ATRA and retinoid derivatives. The balance between activation and quiescence of stellate cells is involved in the control of pancreatic tissue homeostasis. In vitro and in vivo preclinical studies performed with appropriate mouse models indicate that ATRA induces the quiescence of pancreatic stellate cells, which results in a slowing of tumor progression [60]. In these models, ATRA suppresses force-mediated extracellular matrix remodeling and inhibits local cancer cell invasion [61]. The above mentioned observations provided the rationale for a completed phase I and an ongoing phase II clinical trial aimed at demonstrating that ATRA is a stromal-targeting agent which can be used in combination with Gemcitabine and nab-Paclitaxel (albumin and paclitaxel containing nanoparticles) for the treatment of pancreatic ductal adenocarcinoma [62]. It should be noticed that a study performed in SCC (Squamous Cell Carcinoma) and aimed at determining the nuclear receptors, which are involved in the regulation of CAF functionality, resulted in the identification of RARβ, PPARβ-δ, VDR (Vitamin D Receptor), GR (Glucocorticoid Receptor) and AR (Androgen Receptor) as key players in the attenuation of the invasiveness, proliferation, drug resistance, energy metabolism and oxidative stress observed in the neoplastic cell. In this study, the treatment of mice carrying subcutaneous xenografts of SCC cells and CAFs with combinations of cisplatin, RARβ and AR antagonists inhibits chemoresistance in recurring tumors [63].
Actions of ATRA on cancer associated adipocytes
Overweight and obesity are associated with an increased and decreased risk of breast cancer in post-menopausal and pre-menopausal women, respectively [64]. In addition, the two phenomena correlate with an increased risk of breast cancer–specific mortality in both post- and pre-menopausal women. Interestingly, adipocytes constitute the main cellular component of the breast tissue and neoplastic cells are embedded in the adipocyte-rich micro-environment of the mammary gland [65]. This is at the basis of the multiple functional interactions between adipocytes and breast cancer cells.
CAAs (Cancer Associated Adipocytes) diverge from their normal counterparts both in terms of phenotype and function. The interplay between CAAs and cancer cells confers oncogenic properties to the tumor micro-environment, favoring angiogenesis as well as the proliferation and local/distant dissemination of tumor cells. The mechanisms underlying these pro-oncogenic responses seem to involve adipokine regulation, extracellular matrix remodeling, immune cell modulation and metabolic reprogramming. Indeed, cancer cells establish a metabolic symbiosis with CAAs, absorbing the lactate, fatty acids and glutamine produced by neighboring adipocytes [66]. No published data related to the effects exerted by ATRA on CAAs are available. Nevertheless, it is reasonable to hypothesize that the retinoid may influence the behavior of CAAs, as adipocytes play an important role in Vitamin-A storage/metabolism and ATRA influences the homeostasis of adipose tissue [2]. With respect to this last point, it is established that retinol is mobilized from adipocytes when the circulating levels of Vitamin-A are insufficient. In addition, ATRA inhibits CEBPβ (CCAAT-Enhancer-Binding Protein beta)/PPARγ-mediated adipocyte differentiation of pre-adipocytes and mesenchymal progenitor cells in culture [67,68,69] and this inhibitory effect on adipogenesis is observed also in the living mouse [21, 70]. Furthermore, ATRA impairs adipocyte differentiation of human adipose-derived stem cells [71]. Indeed, single-cell gene-expression studies indicate that ATRA signaling modulates the activity of a particular subtype of mammalian ASPCs (Adipose Stem and Precursor Cells), which exert anti-adipogenic activity and are known as Aregs (Adipogenesis regulators) [72]. Finally, it is interesting to notice that the adipose tissue of breast cancer patients contains higher concentrations of retinol than the corresponding counterpart isolated from women bearing benign mammary tumors [73].
Actions of ATRA on tumor vascularization
ATRA plays a crucial role in the development of the mammalian vascular system. Indeed, ATRA controls endothelial cell proliferation and vascular remodeling during the process of tissue angiogenesis [74, 75]. In matrigel implant models, ATRA enhances the growth and function of mature micro-vessels supporting the therapeutic potential of the retinoid in pathological contexts characterized by defective angiogenesis [76]. In the skin, the RAR agonist, tazarotene, has been shown to promote the process of wound-healing via stimulation of tissue regeneration and neo-angiogenesis [77, 78].
In the tumor tissue, hypoxic cancer cells stimulate the generation of a dysfunctional vasculature which supports tumor growth and hampers immune responses [79]. TECs (Tumor-associated Endothelial Cells) are highly heterogeneous and differ from normal endothelial cells in terms of phenotype and function [80, 81]. TECs are endowed with genetic abnormalities and they are characterized by high levels of proliferative and transcriptional activities. In addition, TECs are involved in the generation of an immune-suppressive tissue micro-environment, as they contribute to the deficiency in vascular permeability and the significant modifications of the immune-modulatory signals that are observed in tumor tissues [79]. In preclinical models of SCC and APL, ATRA and its derivatives inhibit tumor related angiogenesis both directly, via actions on the cancer cell, and indirectly, via modulation of the endothelial cell function [82,83,84,85]. With respect to the direct effects of ATRA on endothelial cells, it is interesting to notice that the retinoid inhibits the endothelial-to-osteoblast transition, a process known to be involved in the process of prostate cancer metastatization to the bone [86]. In the context of breast cancer, there are no comprehensive studies on the effects exerted by ATRA on TECs. Nevertheless, the role played by ATRA in the homeostasis of normal vessels suggests that the retinoid is likely to modulate the function of TECs in the tissue. Indeed, ATRA controls the expression of genes, such as VEGF (Vascular Endothelial Growth Factor), FGF (Fibroblast Growth Factor), TGF-β (Transforming Growth Factor-beta) and Hedgehog, which are known to be involved in vascular patterning and morphogenesis [87]. Indeed, ATRA induces the expression of HIF-1α (Hypoxia-Inducible Factor 1-alpha) and VEGF in certain solid tumors and the ATRA/HIF-1α/VEGF pathway has been reported to promote tumor angiogenesis in HUVEC co-cultures and xenografts of the MCF-7 breast cancer cell line [88]. Interestingly in the context of the 4T1 syngeneic breast tumor model, ATRA was shown to increase the number of pericytes associated with intratumor endothelial cells and to normalize the tumor vessel morphology [89].
Actions of ATRA on the immune micro-environment
ATRA is involved in the regulation of the immune system and it plays a key role in the control of inflammatory responses [4]. With respect to this, Vitamin-A insufficiency, which affects 250.000–500.000 children worldwide, is associated with a significant rate of morbidity and mortality during common childhood infections [90]. Although increased susceptibility to childhood infections is believed to be partially due to an impairment of the protection afforded by the epithelial barrier to mucosal pathogens, dysregulation of the immune cell responses is also likely to play a significant role [91]. Indeed, different studies suggest that Vitamin-A metabolites support the differentiation and functional activity of immune cells including dendritic cells/macrophages and lymphocytes [4] [92]. In terms of induced immune-responses, ATRA has been described to exert both tolerogenic and pro-inflammatory effects [4, 92]. With respect to this, the main evidence comes from studies performed in the gut of mice exposed to commensal microorganisms and food antigens. In this setting, DCs (Dendritic Cells) play a pivotal role in antigen processing and in transferring micro-environmental cues to T/B-lymphocytes. Noticeably, these two processes are of fundamental importance for both the activation of immune responses and for the maintenance of immune tolerance [93]. ATRA has been shown to control the genetic program which regulates the maturation of the gut-homing precursors of DCs [94, 95]. In the intestine, DCs and macrophages synthesize ATRA, which, in turn, stimulates the expression of gut-homing molecules in T- and B-lymphocytes as well as in ILCs (Innate Lymphoid Cells) [96,97,98,99,100].
In the context of immune regulation, it must be emphasized that ATRA has also been shown to control the effector functions of T-lymphocytes. Indeed, the local production of ATRA by DCs and macrophages promotes the conversion of naïve CD4+ T-cells into iTregs (Induced regulatory T-cells) [101,102,103,104,105,106]. In addition, ATRA inhibits the IL-6 driven induction of pro-inflammatory Th17 cells [104,105,106,107]. Finally, the exposure of intestinal mucosa B-lymphocytes to ATRA promotes IgA class switching, a process which is required for optimal protection against intestinal pathogens [99, 108].
Although ATRA is predominantly known for its tolerogenic function, the retinoid can also trigger pro-inflammatory effects. Indeed, ATRA has been shown to evoke a tolerogenic or a pro-inflammatory effect depending on the micro-environment and the synergizing cytokines immune cells are exposed to. In physiological conditions, ATRA seems to represent a key determinant of the Treg-Th17 balance, favoring the differentiation of naïve T-lymphocytes into Tregs. At physiological concentrations, ATRA is also a critical determinant in the development of Th17 cells [109]. Upon infection, the local increase in the levels of IL-1 counteracts the ATRA-dependent inhibition of Th17 cells, while the cytokine enhances IL-6 responses, tilting the Treg-Th17 balance towards the Th17 arm [110]. In addition, ATRA is required to elicit the pro-inflammatory responses of CD4+ T-cells to infection and mucosal vaccination [91]. In models of vaccination and allogeneic graft rejection, whole body imaging demonstrates that ATRA signaling is temporally and spatially restricted to the site of inflammation. Conditional ablation of ATRA signaling in T-lymphocytes arrests inflammation by altering the function, migration, and polarity of these cells [109]. In an intestinal environment undergoing an IL15-dependent stress, ATRA acts as an adjuvant in promoting rather than inhibiting the cellular and humoral inflammatory responses to food antigen. In fact, in these conditions, ATRA decreases and stimulates the polarization of Treg and Th1 cells, respectively [111]. Finally, in the context of vaccinia virus infection, ATRA is required for the optimal differentiation of effector and effector memory CD8+ T-cells [112].
The relevance of ATRA for the cross-talk between tumor and immune cells is supported by an elegant study performed with B16 melanoma tumor models. Indeed, the study provides evidence on the specific activation of ATRA driven transcription at the site of tumor growth. In particular, the work identifies ATRA signaling as a critical step for the clonal proliferation of CD8+ T-cells and for the inhibition of tumor growth [113]. A further investigation performed in a mouse model of colitis-associated colon cancer demonstrates a marked deficiency in the levels of ATRA observed in the colon due to alterations in the metabolism of the retinoid which are mediated by microbiota-induced intestinal inflammation [114]. In this context, ATRA seems to exert an anti-tumor action via modulation of the immune micro-environment. In fact, inhibition of the ATRA-dependent signaling pathway promotes tumorigenesis, whereas ATRA supplementation reduces the tumor burden. The beneficial effect exerted by ATRA on the tumor burden is mediated by cytotoxic CD8+ T-cells, which are activated by MHCI up-regulation in colon cancer cells. In contrast, a paper focusing on the tumor micro-environment of sarcomas supports the idea that ATRA exerts an oncogenic action. In fact, the levels of ATRA are reported to be higher in mouse sarcoma as compared to the normal mesenchymal tissues [115]. In addition, tumor cells evade immune responses by producing ATRA, which stimulates and inhibits the differentiation of tumor-associated monocytes into immunosuppressive macrophages and DCs, respectively. As a consequence, intra-tumor injection of a pan-RAR antagonist, which suppresses ATRA activity in the tumor micro-environment, promotes monocyte differentiation into antigen presenting cells, enhancing anti-tumor T cell responses.
It is believed that cancer cell survival and proliferation are sustained by stromal cells of the neoplastic micro-environment whose function has been hijacked to allow tumor progression [116]. In the case of immune cells, tumor-secreted factors prevent normal myeloid cell differentiation, which leads to the accumulation of a heterogeneous population of immune-suppressive immature myeloid cells known as MDSCs (Myeloid Derived Suppressor Cells). MDSCs are recruited to the primary tumor and metastatic micro-environment from the bone marrow and secondary lymphoid tissues (e.g. spleen, lymph nodes) via the blood stream [117]. Evidence obtained in both tumor bearing mice and cancer patients supports the idea that the presence of MDSCs sustains the survival of primary and metastatic cancer cells. MDSCs are capable of inhibiting the immune responses mediated by T- and B-lymphocytes as well as NK (Natural Killer) cells. Thus, inhibition of the immunosuppressive properties of MDSCs can improve anti-tumor responses [117]. Many reports support a role for ATRA in the modulation of MDSC (Table 1). Early studies performed in appropriate mouse models indicate that ATRA promotes the differentiation of MDSCs into DCs and macrophages. The phenomenon seems to be at the basis of ATRA anti-tumor action [118, 119]. With respect to this last contention, it should be emphasized that the above-mentioned mouse models are characterized by the fact that ATRA is capable of increasing only the anti-tumor action of vaccines, as the retinoid exerts no direct effect on tumor cell proliferation. Indeed, the sole administration of combinations between ATRA and vaccines exerts an anti-tumor effect, which results in the inhibition of tumor growth. The reduction in the number and activity of MDSCs induced by the combination of ATRA and vaccines has also been observed during the course of a clinical trial performed in patients affected by extensive-stage small-cell lung cancer [120]. The data mentioned above are further supported by a study conducted with a mouse MC38 colon carcinoma model [121]. In this model, combinations of ATRA and radiotherapy induce the differentiation of tumor infiltrated monocytes into inflammatory iNOS/TNFα-producing macrophages, contemporaneously enhancing the priming/activation of tumor associated CD8+/CD4+ T-cells. The work provides evidence for a positive feedback loop between inflammatory macrophages and T-cells, which results in an inhibition of tumor growth at both the local and systemic level. Indeed, the combination of ATRA and ionizing radiation abrogates tumor re-growth after re-implantation of cancer cells into cured animals and it delays the growth of distant and non-irradiated co-implanted tumors. ATRA and immune-checkpoint inhibitors represent an additional example of retinoid-based combination therapy involving modulation of the immune micro-environment [122,123,124]. In mouse models of mesothelioma and fibrosarcoma, ATRA reduces the number of peripheral MDSCs and it induces an interferon-driven inflammatory tumor micro-environment enriched in CD8+ T-cells. This results in the sensitization of tumor cells to immune-checkpoint inhibitors [122]. Consistent with this, in a model of non-small-cell lung cancer resistant to immune-checkpoint inhibitors, ATRA restores sensitivity to anti-PD1 agents stimulating tumor-specific T-cell dependent immunity [123]. The MDSC suppressive and CD8+ T-cell activating properties of ATRA are supported by recent phase II clinical trials combining the retinoid with ipilimumab or pembrolizumab in melanoma [125, 126]. The results obtained in sarcoma tumor models are in apparent contrast with the stimulatory effects exerted by ATRA on the anti-tumor action of checkpoint inhibitors. In this model, intra-tumor injection of a pan-RAR antagonist enhances the anti-tumor activity of checkpoint inhibitors via promotion of an immune stimulatory tumor micro-environment [115].
In breast cancer, the treatment of mammary DA3 tumor-bearing mice with ATRA causes a significant reduction in the number of MDSCs [118]. However, administration of ATRA as a single agent does not exert any effect on the growth of the primary tumor instead improved immune response to vaccination. In particular, the retinoid reduces the expansion of tumor-associated immature myeloid cells by triggering their differentiation into mature DCs, macrophages, and granulocytes. Moreover, in an experimental model of mammary tumor vaccination, ATRA activity reverts tumor-induced CD4+ T-cell tolerance [118]. The ability of ATRA to improve antitumor immune responses and to enhance the effect of vaccination was described also in other tumor types [118]. ATRA has also been reported to modulate immune cell composition in the metastatic niche. Indeed, the retinoid enhances the metastatic behavior of breast tumors obtained by transplantation of the mouse 4T1 and 4TO7 cell lines in immune competent mice. This effect has been ascribed to a change in the composition of the myeloid cell population present in the specific metastatic sites. In these models too, ATRA retains the ability to promote the differentiation of myeloid cells. However, in the lung metastatic sites, ATRA drives the differentiation of immature myeloid cells into a macrophage lineage with stronger immunosuppressive ability [129]. In other tumor contexts, such as osteosarcoma, ATRA prevents the metastatic spread of cancer cells by inhibiting the activity of inflammatory macrophages [130]. In animals transplanted with the mouse 4T1 and TS/A mammary adenocarcinoma cell lines, ATRA administration enhances the effects of antiangiogenic agents [89]. In this experimental setting ATRA reduces the MDSC increase induced by a monoclonal antibody targeting murine VEGFR2. Moreover, the retinoid contributes to the stabilization of the tumor endothelium exerting vessel-normalizing effects, which supports the antitumor effect of the anti-angiogenic compound. Interestingly, ATRA treatment rescues the hypoxic conditions induced by this antibody.
Altogether the above data support the notion that ATRA potentiates or impairs cancer progression by acting on the immune system depending upon the costimulatory conditions used.
Activity of ATRA in association with current breast cancer treatments
Various pre-clinical studies indicate that ATRA improves the efficacy of current breast cancer treatments. For instance, ATRA has been used in association with the gold standard therapies for ER+ and HER2+ breast cancer. As far as ER+ tumors, ATRA potentiates the antiproliferative activity of tamoxifen, a well-known selective ER modulator used as a therapeutic agent in the clinics [51]. As the unliganded form of RARα is part of the ERα transcriptional complex, the cross-talk between RARα and ERα is thought to be at the basis of the observed antitumor efficacy of ATRA. Upon ATRA binding, RARα inhibits the proliferative effect trigger by the estrogen [25]. As far as HER2+ tumors, ATRA synergizes with the anti-HER2 therapeutic agents trastuzumab and lapatinib, two clinically useful HER2 kinase inhibitors [23, 131]. In particular, ATRA potentiates the HER2 phosphorylation inhibition induced by lapatinib [23].
Immunotherapy (Atezolizumab and Pembrolizumab) are approved for the treatment of TNBC and metastatic HER2+ tumors [132]. Specific studies in breast cancer are not available, although ATRA regulates tumor associated immune cells in various types of solid tumors (Table 1). This is the basis of the benefits observed with combinations of ATRA and immunotherapy, which supports the idea that ATRA + immunotherapeutics may be effective in breast cancer as well.
CDK4/6 inhibitors were shown to improve the survival in patients with metastatic breast cancer [132]. As a consequence, combinations of CDK4/6 inhibitors and endocrine therapeutic agents represent the new standard of care for first and second line treatment of advanced ER+/HER2− breast cancer. ATRA co-operates with the CDK4/6 inhibitor, Palbociclib, at the transcriptional level, resulting in additive anti-proliferative and differentiating effects in neuroblastoma cells [133]. Studies on breast cancer models are necessary to support a possible role of ATRA also in this type of tumor.
Adjuvant radiotherapy is an essential component of breast cancer treatment. Although clinical trials aimed at assessing the benefit of ATRA administration in this setting are not available in the scientific literature, there is preclinical evidence indicating that the retinoid enhances radiation efficacy. Indeed, in mouse cancer models, combinations of ATRA and radiation therapy (ionizing radiation, 15Gy) reprogram intra-tumor myeloid cells, resulting in an enhancement of systemic anti-tumor immunity and a stimulation of immune checkpoint inhibitor (ICI) therapeutic activity [121] (Table 1).
In addition, several studies provide evidence of synergistic interactions between ATRA and chemotherapeutic agents [134]. For instance, pre-clinical studies support the idea that ATRA sensitizes breast cancer cells to paclitaxel and adriamycin, two chemo-therapeutic agents commonly used in the treatment of this tumor [135].
In recent years, several specific pre-clinical studies aimed at developing nanocarriers permitting the contemporaneous delivery of ATRA and chemotherapeutic agents have been conducted. In the 4T1 mouse metastatic breast cancer model, micellar nanoparticles containing combinations of ATRA and doxorubicin were administered in a post-operatory setting to reduce inflammation and MDSC recruitment [136]. These nanoparticles suppress post-operative recurrences and pulmonary metastases. In a orthotopic xenograft model of TNBC, ATRA and doxorubicin containing nanoparticles stimulate the differentiation of cancer stem cells [137]. This reduces the tumor initiating activity of cancer stem cells and increases their sensitivity to doxorubicin. In the same model, doxorubicin-mediated cytotoxicity is potentiated by ATRA driven differentiation and Entinostat (histone-deacetylase-inhibitor) dependent epigenetic remodeling [138]. Similarly, ATRA sensitizes breast cancer cells to paclitaxel [135]. Co-delivery of ATRA and paclitaxel using albumin-bound paclitaxel nanoparticles generates a significantly improved anti-metastatic effect [139]. Notably, co-delivery nanoparticles exhibit more pronounced therapeutic effects than the combination of the two free drugs. Another proposed nanodrug formulation consists of ATRA and irinotecan along with the photothermal agent IR825 [140]. Indeed, the combination of ATRA with a chemotherapeutic drug (irinotecan) induces the differentiation and death of breast cancer stem cells, while NIR (Near to InfraRed) laser irradiation triggers a photothermal effect. In the mouse 4T1 breast cancer model, this combination causes a potent antitumor effect, which is superior to the effect observed with each single agent or double combination.
In conclusion, the results summarized above support the idea that ATRA-based therapeutic combinations with other anti-tumor agents may be of clinical significance in the management of breast cancer.
ATRA in breast cancer clinical trials
The current chapter aims at providing a brief summary of the data supporting the clinical potential of ATRA in the management of breast cancer. Indeed, the chapter focusses on the results obtained with clinical trials involving the use of this retinoid.
The available experimental evidence supports the idea that ATRA exerts a general and direct onco-suppressive action in breast cancer cells. By converse, the effects exerted by ATRA on the tumor micro-environment are dichotomic, as the retinoid causes both oncogenic and onco-suppressive responses. Despite the large number of pre-clinical studies performed with ATRA there are only four registered clinical trials (ClinTR1–4) on the use of the retinoid as a therapeutic agent in the oncological setting (Table 2). ClinTR1 is based on the use of ATRA as a single therapeutic agent in the treatment of patients affected by hormone-refractory, metastatic breast cancer and the results obtained lead to the conclusion that the retinoid is devoid of significant anti-tumor activity. However, the trial suffers from a number of limitations, including the low number of patients (14 patients altogether) and the high degree of inter-patient variability in terms of ATRA blood levels, following drug administration [141]. Two other trials (ClinTR2 and ClinTR3) provide data on the anti-tumor action exerted by combinations of ATRA and tamoxifen or chemotherapy in breast cancer. ClinTR2, which was performed in the context of ER+ mammary tumors [142], indicates that the maximal daily dose of ATRA that can be administered with tamoxifen is 190 mg/mq. In addition, ATRA must be administered using two weekly cycles per month. The results obtained indicate objective responses in a number of patients undergoing progression following treatment with tamoxifen alone. However, the study design and the limited number of patients enrolled (n = 25) does not permit to draw any significant conclusion on the anti-tumor activity of the retinoid. Similar to what was observed in the case of the clinical trial conducted by Sutton et al., a high degree of intra- and inter-patient variability in the plasma levels of ATRA are reported. ClinTR3 is a small pilot study involving 17 patients suffering from late stage breast cancer (15/17 tumors = stage III/IV) who were exposed to different types of therapeutic protocols [143]. The study demonstrates that the combination of ATRA (45 mg/mq/day) and paclitaxel is well-tolerated. In addition, the combination of ATRA and paclitaxel results in a modest response rate. Indeed, the time-to-progression and survival rates observed in ATRA plus paclitaxel treated patients are similar to those reported for paclitaxel alone. Nevertheless, treatment with the combination of the two drugs is associated with a relatively high rate of stable disease (58.8%). ClinTR4 is an ongoing trial (NCT04113863) aimed at evaluating the activity of ATRA in combination with anastrozole in postmenopausal women with newly diagnosed ER+/HER2−breast cancer.
Besides the clinical trials described above, it is worthwhile mentioning the publication of a small pre-operative study in locally advanced breast cancer. The main objective of this last study was to define the biological effects of ATRA following a 3-week administration in the presence and absence of tamoxifen or IFN2α (Interferon 2α) prior to the surgical remotion of the tumor [144]. Overall, ATRA administration exerts an influence on the tumor grade but it is devoid of effects on the cell cycle kinetics (G0-G1 phase) and cell proliferation (Ki67 levels). The lowest dose of ATRA producing a biological response is reported to amount to 15 mg/mq/day. ATRA induces the expression of the progesterone receptor and of RARβ in a subset of patients. Neither tamoxifen nor tamoxifen plus IFN2α potentiates the action of ATRA on the two genes. Once again, no significant conclusions can be drawn from the study, given the small number of patients enrolled (5 for each arm of the trial). In addition, the pharmacokinetic analyses performed in the study unveil a high level of heterogeneity among patients. Indeed, the plasma concentrations of ATRA determined in each patient are extremely variable and they do not show any linear correlation with the dose administered.
Conclusions
ATRA is considered to be the most important and biologically active metabolite of Vitamin-A. In the mammalian organism, ATRA exerts pleiotropic effects by the transcriptional modulation of hierarchical and integrated gene-networks which are involved in the control of tissue- and cell-specific functions [10]. In the oncological field, the use of ATRA as a potential anti-tumor agent should keep into consideration its diverse systemic effects and its specific action on disease associated stromal and immunological cells as well as the neoplastic cells themselves. While the role of ATRA as a successful therapeutic agent in the treatment of APL, where the retinoid induces terminal differentiation of the leukemic blast, is well established, the potential of ATRA in the management of solid tumors is still controversial [145]. In breast cancer, the growth-inhibitory and differentiating action of ATRA on the neoplastic cells is documented by a large number of pre-clinical studies [5]. From a mechanistic point of view, ATRA controls the expression of various core components of the tumor cell dictating cell-cycle progression and the retinoid exerts a fundamental action in the stimulation of interferon-dependent responses. Its antiproliferative actions depends upon breast tumor subtype and distinct genetic characteristics (e.g., RARA amplification, NOTCH1 activating deletion) [22, 23, 27]. Currently, there is little published evidence on the effects exerted by ATRA on the tumor micro-environment, which is an emerging determinant of the development and progression of the neoplastic disease. Indeed, in solid tumors, ATRA has been shown to determine opposite effects on the micro-environment, depending on the experimental setting considered. As discussed above, the retinoid seems to be effective only in a combinatorial setting where the cognate compound dictates its role. It is worth noticing that ATRA is a well-known and important morphogen that induces stem cell differentiation into various cell lineages and ATRA-based pharmacological combinations are used for the differentiation of pluripotent stem cells (iPSC) along different cell lineages [146, 147]. In this case too, the type of differentiation induced is dependent by the components of the combinations other than ATRA. With respect to the tumor niche, the action of ATRA on the tumor-associated immune-cell component of the micro-environment is the issue which has been the primary object of scientific attention. Of particular clinical relevance is the ATRA effect on the MDSC component sustained by a recent clinical trial [126]. However, a comprehensive picture of the role played by the retinoid is still largely incomplete. Moreover, we lack data on the action exerted by ATRA on other cell types of the tumor stroma, such as the adipocytes, which represent the main component of the mammary gland and are involved in retinoid storage. Thus, a full exploitation of the onco-suppressive properties of ATRA is likely to require further studies aimed at elucidating the action exerted by the retinoid on the tumor micro-environment. This type of studies will be facilitated by the recent development and implementation of technologies like spatial transcriptomics and spatial mass spectrometry. A final comment regards the emerging issue of drug bio-distribution in solid tumors, which suggests that investigations on new methods for the selective delivery of ATRA to the cancer tissue will be of fundamental importance for its efficacy.
Availability of data and materials
Not applicable.
Abbreviations
- ADHs:
-
Alcohol Dehydrogenases
- APL:
-
Acute Promyelocytic Leukemia
- AR:
-
Androgen Receptor
- Aregs:
-
Adipogenesis regulators
- ASPCs:
-
Adipose Stem and Precursor Cells
- ATRA:
-
All-trans retinoic acid
- B cells:
-
B- lymphocytes
- BRCA1:
-
BReast CAncer gene 1
- CAAs:
-
Cancer Associated Adipocytes
- CAF:
-
Cancer Associated Fibroblasts
- CAFs:
-
Cancer Associated Fibroblasts
- CEBPβ:
-
CCAAT-Enhancer-Binding Protein beta
- COUP-TFII:
-
Chicken Ovalbumin Upstream Promoter-Transcription Factor II
- CRABPI:
-
Cytosolic Retinoic Acid Binding Protein I
- CRABPII:
-
Cytosolic Retinoic Acid Binding Protein I
- CRISPR/CAS9:
-
Clustered Regularly Interspaced Short Palindromic Repeats-Cas CRISPR-associated protein 9
- CYP26A1:
-
Cytochrome P450 Family 26 Subfamily A Member 1
- CYP26B1:
-
Cytochrome P450 Family 26 Subfamily B Member 1
- CYP26C1:
-
Cytochrome P450 Family 26 Subfamily C Member 1
- DCs:
-
Dendritic Cells
- ECM:
-
ExtraCellular Matrix
- EGF:
-
Epithelial Growth Factor
- EMT:
-
Epithelial-to-Mesenchymal Transition
- ER+ :
-
Estrogen Receptor positive
- FABP5:
-
Fatty Acid Binding Protein 5
- FGF:
-
Fibroblast Growth Factor
- GR:
-
Glucocorticoid Receptor
- HER2+ :
-
Human Epidermal Growth Factor Receptor 2 positive
- HIF-1α:
-
Hypoxia-Inducible Factor 1-alpha
- HOXs:
-
Homeobox genes
- ICI:
-
immune checkpoint inhibitor
- IFN2α:
-
Interferon 2α
- ILCs:
-
Innate Lymphoid Cells
- iTregs:
-
Induced regulatory T-cells
- JNK2:
-
Janus Kinase 2
- LEP:
-
Luminal EPithelial
- MDSCs:
-
Myeloid Derived Suppressor Cells
- MEP:
-
MyoEPhitelial
- MMTV:
-
Mouse Mammary Tumor Virus
- MSK1:
-
Mitogen and Stress-activated Protein Kinase-1
- NK:
-
Natural Killer
- NOTCH1:
-
Neurogenic locus NOTCH Homolog protein 1
- NR1F2:
-
Nuclear Receptor 1F2
- NR2C2:
-
Nuclear Receptor 2C2
- NR2F2:
-
Nuclear Receptor 2F2
- p38MAPK:
-
p38 Membrane Associated Protein Kinase
- p42/p44 MAPK:
-
p42/44 Membrane Associated Protein Kinase
- PALB2:
-
Partner And Localizer of BRCA2
- PPARβ-δ:
-
Peroxisome Proliferator-Activator Receptor β/δ
- RALDHs:
-
Retinaldehyde Dehydrogenases
- RARE:
-
Retinoic Acid Responsive Element
- RARα:
-
Retinoic Acid Receptor alpha
- RBP4:
-
Retinol Binding Protein 4
- RDHs:
-
Retinol Dehydrogenases
- RORβ:
-
RAR-related Orphan Receptor Beta
- RXR:
-
Retinoid X Receptor
- SCC:
-
Squamous Cell Carcinoma
- SNR:
-
Steroid Nuclear Receptors
- STAT3-STAT5:
-
Signal Transducer and Activator of Transcription 3 and 5
- STRA6:
-
Signaling Receptor And Transporter of Retinol
- STRA6:
-
Signaling Receptor And Transporter of Retinol STRA6
- T cells:
-
T- lymphocytes
- TECs:
-
Tumor-associated Endothelial Cells
- TGF-β:
-
Transforming Growth Factor-beta
- TNBC:
-
Triple Negative Breast Cancer.
- TR4:
-
Testicular Receptor 4
- TTR:
-
Transthyretin
- VDR:
-
Vitamin D Receptor
- VEGF:
-
Vascular Endothelial Growth Factor
References
Alcohol RS. Retinoic acid, and Cancer. In: Zakhari S, Vasiliou V, Guo QM, editors. Alcohol and Cancer [internet]. New York, NY: Springer; 2011. p. 127–53. https://doi.org/10.1007/978-1-4614-0040-0_7.
Blaner WS. Vitamin a signaling and homeostasis in obesity, diabetes, and metabolic disorders. Pharmacol Ther. 2019;197:153–78.
Berenguer M, Duester G. Retinoic acid, RARs and early development. J Mol Endocrinol. 2022;69(4):T59–67. https://doi.org/10.1530/JME-22-0041.
Erkelens MN, Mebius RE. Retinoic acid and immune homeostasis: a balancing act. Trends Immunol. 2017;38(3):168–80.
Garattini E, Bolis M, Garattini SK, Fratelli M, Centritto F, Paroni G, et al. Retinoids and breast cancer: from basic studies to the clinic and back again. Cancer Treat Rev. 2014;40(6):739–49.
de Thé H, Pandolfi PP, Chen Z. Acute Promyelocytic leukemia: a paradigm for Oncoprotein-targeted cure. Cancer Cell. 2017;32(5):552–60.
Napoli JL. Quantification of physiological levels of retinoic acid. Methods Enzymol. 1986;123:112–24.
Noy N, Li L, Abola MV, Berger NA. Is retinol binding protein 4 a link between adiposity and Cancer? Horm Mol Biol Clin Investig. 2015;23(2):39–46.
Duester G. Retinoic acid synthesis and signaling during early organogenesis. Cell. 2008;134(6):921–31.
di Masi A, Leboffe L, De Marinis E, Pagano F, Cicconi L, Rochette-Egly C, et al. Retinoic acid receptors: from molecular mechanisms to cancer therapy. Mol Asp Med. 2015;1(41):1–115.
Dilworth FJ, Chambon P. Nuclear receptors coordinate the activities of chromatin remodeling complexes and coactivators to facilitate initiation of transcription. Oncogene. 2001;20(24):3047–54.
Laursen KB, Gudas LJ. Combinatorial knockout of RARα, RARβ, and RARγ completely abrogates transcriptional responses to retinoic acid in murine embryonic stem cells. J Biol Chem. 2018;293(30):11891–900.
Schug TT, Berry DC, Shaw NS, Travis SN, Noy N. Opposing effects of retinoic acid on cell growth result from alternate activation of two different nuclear receptors. Cell. 2007;129(4):723–33.
Stehlin-Gaon C, Willmann D, Zeyer D, Sanglier S, Van Dorsselaer A, Renaud JP, et al. All-trans retinoic acid is a ligand for the orphan nuclear receptor RORβ. Nat Struct Mol Biol. 2003;10(10):820–5.
Kruse SW, Suino-Powell K, Zhou XE, Kretschman JE, Reynolds R, Vonrhein C, et al. Identification of COUP-TFII orphan nuclear receptor as a retinoic acid-activated receptor. PLoS Biol. 2008;6(9):e227.
Zhou XE, Suino-Powell KM, Xu Y, Chan CW, Tanabe O, Kruse SW, et al. The orphan nuclear receptor TR4 is a vitamin A-activated nuclear receptor * ♦. J Biol Chem. 2011;286(4):2877–85.
Schug TT, Berry DC, Toshkov IA, Cheng L, Nikitin AY, Noy N. Overcoming retinoic acid-resistance of mammary carcinomas by diverting retinoic acid from PPARbeta/delta to RAR. Proc Natl Acad Sci U S A. 2008;105(21):7546–51.
Rochette-Egly C, Germain P. Dynamic and combinatorial control of gene expression by nuclear retinoic acid receptors (RARs). Nucl Recept Signal. 2009;8(7):e005.
Piskunov A, Rochette-Egly C. A retinoic acid receptor RARα pool present in membrane lipid rafts forms complexes with G protein αQ to activate p38MAPK. Oncogene. 2012;31(28):3333–45.
Berry DC, Levi L, Noy N. Holo-retinol-binding protein and its receptor STRA6 drive oncogenic transformation. Cancer Res. 2014;74(21):6341–51.
Berry DC, Noy N. All-trans-retinoic acid represses obesity and insulin resistance by activating both peroxisome proliferation-activated receptor beta/delta and retinoic acid receptor. Mol Cell Biol. 2009;29(12):3286–96.
Centritto F, Paroni G, Bolis M, Garattini SK, Kurosaki M, Barzago MM, et al. Cellular and molecular determinants of all-trans retinoic acid sensitivity in breast cancer: luminal phenotype and RARα expression. EMBO Mol Med. 2015;7(7):950–72.
Paroni G, Fratelli M, Gardini G, Bassano C, Flora M, Zanetti A, et al. Synergistic antitumor activity of lapatinib and retinoids on a novel subtype of breast cancer with coamplification of ERBB2 and RARA. Oncogene. 2012;31(29):3431–43.
Mangiarotti R, Danova M, Alberici R, Pellicciari C. All-trans retinoic acid (ATRA)-induced apoptosis is preceded by G1 arrest in human MCF-7 breast cancer cells. Br J Cancer. 1998;77(2):186–91.
Ross-Innes CS, Stark R, Holmes KA, Schmidt D, Spyrou C, Russell R, et al. Cooperative interaction between retinoic acid receptor-alpha and estrogen receptor in breast cancer. Genes Dev. 2010;24(2):171–82.
Kupumbati TS, Cattoretti G, Marzan C, Farias EF, Taneja R, Mira-y-Lopez R. Dominant negative retinoic acid receptor initiates tumor formation in mice. Mol Cancer. 2006;5:12. https://doi.org/10.1186/1476-4598-5-12.
Zanetti A, Affatato R, Centritto F, Fratelli M, Kurosaki M, Barzago MM, et al. All-trans-retinoic acid modulates the plasticity and inhibits the motility of breast Cancer cells: ROLE OF NOTCH1 AND TRANSFORMING GROWTH FACTOR (TGFβ). J Biol Chem. 2015;290(29):17690–709.
Dawson MI, Chao W, Pine P, Jong L, Hobbs PD, Rudd CK, et al. Correlation of retinoid binding affinity to retinoic acid receptor α with retinoid inhibition of growth of estrogen receptor-positive MCF-7 mammary carcinoma cells. Cancer Res. 1995;55(19):4446–51.
Cohn E, Ossowski L, Bertran S, Marzan C, Farias EF. RARα1 control of mammary gland ductal morphogenesis and wnt1-tumorigenesis. Breast Cancer Res BCR. 2010;12(5):R79.
Lu Y, Bertran S, Samuels TA, Mira-y-Lopez R, Farias EF. Mechanism of inhibition of MMTV-neu and MMTV-wnt1 induced mammary oncogenesis by RARα agonist AM580. Oncogene. 2010;29(25):3665–76.
van der Burg B, van der Leede BM, Kwakkenbos-Isbrücker L, Salverda S, de Laat SW, van der Saag PT. Retinoic acid resistance of estradiol-independent breast cancer cells coincides with diminished retinoic acid receptor function. Mol Cell Endocrinol. 1993;91(1–2):149–57.
Bolis M, Garattini E, Paroni G, Zanetti A, Kurosaki M, Castrignanò T, et al. Network-guided modeling allows tumor-type independent prediction of sensitivity to all-trans-retinoic acid. Ann Oncol off J Eur Soc Med Oncol. 2017;28(3):611–21.
Laganière J, Deblois G, Giguère V. Functional genomics identifies a mechanism for estrogen activation of the retinoic acid receptor α1 gene in breast Cancer cells. Mol Endocrinol. 2005;19(6):1584–92.
Lu M, Mira-y-Lopez R, Nakajo S, Nakaya K, Jing Y. Expression of estrogen receptor alpha, retinoic acid receptor alpha and cellular retinoic acid binding protein II genes is coordinately regulated in human breast cancer cells. Oncogene. 2005;24(27):4362–9.
Hua S, Kittler R, White KP. Genomic antagonism between retinoic acid and estrogen signaling in breast Cancer. Cell. 2009;137(7):1259–71.
Gardini A, Baillat D, Cesaroni M, Shiekhattar R. Genome-wide analysis reveals a role for BRCA1 and PALB2 in transcriptional co-activation. EMBO J. 2014;33(8):890–905.
Bolis M, Paroni G, Fratelli M, Vallerga A, Guarrera L, Zanetti A, et al. All-trans retinoic acid stimulates viral mimicry, interferon responses and antigen presentation in breast-Cancer cells. Cancers. 2020;12(5)
Coyle KM, Dean CA, Thomas ML, Vidovic D, Giacomantonio CA, Helyer L, et al. DNA methylation predicts the response of triple-negative breast cancers to all-trans retinoic acid. Cancers. 2018;10(11):397.
Cui J, Gong M, He Y, Li Q, He T, Bi Y. All-trans retinoic acid inhibits proliferation, migration, invasion and induces differentiation of hepa1-6 cells through reversing EMT in vitro. Int J Oncol. 2016;48(1):349–57.
Shi G, Zheng X, Wu X, Wang S, Wang Y, Xing F. All-trans retinoic acid reverses epithelial-mesenchymal transition in paclitaxel-resistant cells by inhibiting nuclear factor kappa B and upregulating gap junctions. Cancer Sci. 2019;110(1):379–88.
Woo YJ, Jang KL. All-trans retinoic acid activates E-cadherin expression via promoter hypomethylation in the human colon carcinoma HCT116 cells. Biochem Biophys Res Commun. 2012;425(4):944–9.
Berardi DE, Flumian C, Campodónico PB, Urtreger AJ, Diaz Bessone MI, Motter AN, et al. Myoepithelial and luminal breast cancer cells exhibit different responses to all-trans retinoic acid. Cell Oncol Dordr. 2015;38(4):289–305.
Loo SY, Toh LP, Xie WH, Pathak E, Tan W, Ma S, et al. Fatty acid oxidation is a druggable gateway regulating cellular plasticity for driving metastasis in breast cancer. Sci Adv. 2021;7(41):eabh2443.
Arisi MF, Starker RA, Addya S, Huang Y, Fernandez SV. All trans-retinoic acid (ATRA) induces re-differentiation of early transformed breast epithelial cells. Int J Oncol. 2014;44(6):1831–42.
Doi A, Ishikawa K, Shibata N, Ito E, Fujimoto J, Yamamoto M, et al. Enhanced expression of retinoic acid receptor alpha (RARA) induces epithelial-to-mesenchymal transition and disruption of mammary acinar structures. Mol Oncol. 2015;9(2):355–64.
Endo Y, Deonauth K, Prahalad P, Hoxter B, Zhu Y, Byers SW. Role of Sox-9, ER81 and VE-cadherin in retinoic acid-mediated trans-differentiation of breast cancer cells. PLoS One. 2008;3(7):e2714.
Prahalad P, Dakshanamurthy S, Ressom H, Byers SW. Retinoic acid mediates regulation of network formation by COUP-TFII and VE-cadherin expression by TGFbeta receptor kinase in breast cancer cells. PLoS One. 2010;5(4):e10023.
Pavlova NN, Zhu J, Thompson CB. The hallmarks of cancer metabolism: still emerging. Cell Metab. 2022;34(3):355–77.
Albanesi J, Noguera NI, Banella C, Colangelo T, De Marinis E, Leone S, et al. Transcriptional and metabolic dissection of ATRA-induced granulocytic differentiation in NB4 acute Promyelocytic leukemia cells. Cells. 2020;9(11):2423.
Terao M, Goracci L, Celestini V, Kurosaki M, Bolis M, Di Veroli A, et al. Role of mitochondria and cardiolipins in growth inhibition of breast cancer cells by retinoic acid. J Exp Clin Cancer Res CR. 2019;38(1):436.
Meligova AK, Siakouli D, Stasinopoulou S, Xenopoulou DS, Zoumpouli M, Ganou V, et al. ERβ1 sensitizes and ERβ2 desensitizes ERα-positive breast Cancer cells to the inhibitory effects of tamoxifen, Fulvestrant and their combination with all-trans retinoic acid. Int J Mol Sci. 2023;24(4):3747.
Giménez-Cassina A, Danial NN. Regulation of mitochondrial nutrient and energy metabolism by BCL-2 family proteins. Trends Endocrinol Metab. 2015;26(4):165–75.
Yoo HJ, Kim M, Kim M, Kang M, Jung KJ, Hwang SM, et al. Analysis of metabolites and metabolic pathways in breast cancer in a Korean prospective cohort: the Korean Cancer prevention study-II. Metabolom Off J Metabolomic Soc. 2018;14(6):85.
Hayden LJ, Satre MA. Alterations in cellular retinol metabolism contribute to differential retinoid responsiveness in normal human mammary epithelial cells versus breast cancer cells. Breast Cancer Res Treat. 2002;72(2):95–105.
Brown G. Deregulation of all-trans retinoic acid signaling and development in Cancer. Int J Mol Sci. 2023;24(15):12089.
Sahai E, Astsaturov I, Cukierman E, DeNardo DG, Egeblad M, Evans RM, et al. A framework for advancing our understanding of cancer-associated fibroblasts. Nat Rev Cancer. 2020;20(3):174–86.
Ping Q, Yan R, Cheng X, Wang W, Zhong Y, Hou Z, et al. Cancer-associated fibroblasts: overview, progress, challenges, and directions. Cancer Gene Ther. 2021;28(9):984–99.
Liu X, Nugoli M, Laferrière J, Saleh SM, Rodrigue-Gervais IG, Saleh M, et al. Stromal retinoic acid receptor beta promotes mammary gland tumorigenesis. Proc Natl Acad Sci U S A. 2011;108(2):774–9.
Liu X, Giguère V. Inactivation of RARβ inhibits Wnt1-induced mammary tumorigenesis by suppressing epithelial-mesenchymal transitions. Nucl Recept Signal. 2014;12:e004.
Froeling FEM, Feig C, Chelala C, Dobson R, Mein CE, Tuveson DA, et al. Retinoic acid-induced pancreatic stellate cell quiescence reduces paracrine Wnt-β-catenin signaling to slow tumor progression. Gastroenterol. 2011;141(4):1486–97.
Chronopoulos A, Robinson B, Sarper M, Cortes E, Auernheimer V, Lachowski D, et al. ATRA mechanically reprograms pancreatic stellate cells to suppress matrix remodelling and inhibit cancer cell invasion. Nat Commun. 2016;7(1):12630.
Kocher HM, Basu B, Froeling FEM, Sarker D, Slater S, Carlin D, et al. Phase I clinical trial repurposing all-trans retinoic acid as a stromal targeting agent for pancreatic cancer. Nat Commun. 2020;11(1):4841.
Chan JSK, Sng MK, Teo ZQ, Chong HC, Twang JS, Tan NS. Targeting nuclear receptors in cancer-associated fibroblasts as concurrent therapy to inhibit development of chemoresistant tumors. Oncogene. 2018;37(2):160–73.
T D, Cj L, S B, Ma C, Wa H. Obesity, Inflammation, and Cancer. Annu Rev Pathol. 2016 11 Available from: https://pubmed.ncbi.nlm.nih.gov/27193454/
Rybinska I, Mangano N, Tagliabue E, Triulzi T. Cancer-Associated Adipocytes in Breast Cancer: Causes and Consequences. Int J Mol Sci. 2021;22(7):3775. https://doi.org/10.3390/ijms22073775.
Munteanu R, Onaciu A, Moldovan C, Zimta AA, Gulei D, Paradiso AV, et al. Adipocyte-Based Cell Therapy in Oncology: The Role of Cancer-Associated Adipocytes and Their Reinterpretation as Delivery Platforms. Pharmaceutics. 2020;12(5)):402. Available from: https://pubmed.ncbi.nlm.nih.gov/32354024/
Schwarz EJ, Reginato MJ, Shao D, Krakow SL, Lazar MA. Retinoic acid blocks adipogenesis by inhibiting C/EBPbeta-mediated transcription. Mol Cell Biol. 1997;17(3):1552–61.
Xue JC, Schwarz EJ, Chawla A, Lazar MA. Distinct stages in adipogenesis revealed by retinoid inhibition of differentiation after induction of PPARgamma. Mol Cell Biol. 1996;16(4):1567–75.
Green AC, Kocovski P, Jovic T, Walia MK, Chandraratna RAS, Martin TJ, et al. Retinoic acid receptor signalling directly regulates osteoblast and adipocyte differentiation from mesenchymal progenitor cells. Exp Cell Res. 2017;350(1):284–97.
Mercader J, Ribot J, Murano I, Felipe F, Cinti S, Bonet ML, et al. Remodeling of White adipose tissue after retinoic acid Administration in Mice. Endocrinol. 2006;147(11):5325–32.
Takeda K, Sriram S, Chan XHD, Ong WK, Yeo CR, Tan B, et al. Retinoic acid mediates visceral-specific Adipogenic defects of human adipose-derived stem cells. Diabetes. 2016;65(5):1164–78.
Zachara M, Rainer PY, Hashimi H, Russeil JM, Alpern D, Ferrero R, et al. Mammalian adipogenesis regulator (Areg) cells use retinoic acid signalling to be non- and anti-adipogenic in age-dependent manner. EMBO J. 2022;22:e108206.
Shim E, Yeum KJ, Tang G, Ahn SH, Hwang J, Lee-Kim YC. Retinoids, carotenoids, and tocopherols in breast adipose tissue and serum of benign breast disease and breast cancer patients. Nutr Cancer. 2012;64(7):956–63.
Lai L, Bohnsack BL, Niederreither K, Hirschi KK. Retinoic acid regulates endothelial cell proliferation during vasculogenesis. Dev Camb Engl. 2003;130(26):6465–74.
Otto DME, Henderson CJ, Carrie D, Davey M, Gundersen TE, Blomhoff R, et al. Identification of novel roles of the cytochrome p450 system in early embryogenesis: effects on vasculogenesis and retinoic acid homeostasis. Mol Cell Biol. 2003;23(17):6103–16.
Gaetano C, Catalano A, Illi B, Felici A, Minucci S, Palumbo R, et al. Retinoids induce fibroblast growth factor-2 production in endothelial cells via retinoic acid receptor alpha activation and stimulate angiogenesis in vitro and in vivo. Circ Res. 2001;88(4):E38–47.
Saito A, Sugawara A, Uruno A, Kudo M, Kagechika H, Sato Y, et al. All-trans retinoic acid induces in vitro angiogenesis via retinoic acid receptor: possible involvement of paracrine effects of endogenous vascular endothelial growth factor signaling. Endocrinol. 2007;148(3):1412–23.
Zen AAH, Nawrot DA, Howarth A, Caporali A, Ebner D, Vernet A, et al. The retinoid agonist Tazarotene promotes angiogenesis and wound healing. Mol Ther. 2016;24(10):1745–59.
Nagl L, Horvath L, Pircher A, Wolf D. Tumor endothelial cells (TECs) as potential immune directors of the tumor microenvironment - new findings and future perspectives. Front Cell Dev Biol. 2020;8:766.
Lambrechts D, Wauters E, Boeckx B, Aibar S, Nittner D, Burton O, et al. Phenotype molding of stromal cells in the lung tumor microenvironment. Nat Med. 2018;24(8):1277–89.
Goveia J, Rohlenova K, Taverna F, Treps L, Conradi LC, Pircher A, et al. An integrated gene expression landscape profiling approach to identify lung tumor endothelial cell heterogeneity and Angiogenic candidates. Cancer Cell. 2020;37(1):21–36.e13.
Majewski S, Szmurlo A, Marczak M, Jablonska S, Bollag W. Inhibition of tumor cell-induced angiogenesis by retinoids, 1,25-dihydroxyvitamin D3 and their combination. Cancer Lett. 1993;75(1):35–9.
Lingen MW, Polverini PJ, Bouck NP. Inhibition of squamous cell carcinoma angiogenesis by direct interaction of retinoic acid with endothelial cells. Lab Investig J Tech Methods Pathol. 1996;74(2):476–83.
Lingen MW, Polverini PJ, Bouck NP. Retinoic acid and interferon alpha act synergistically as antiangiogenic and antitumor agents against human head and neck squamous cell carcinoma. Cancer Res. 1998;58(23):5551–8.
Kini AR, Peterson LA, Tallman MS, Lingen MW. Angiogenesis in acute promyelocytic leukemia: induction by vascular endothelial growth factor and inhibition by all-trans retinoic acid. Blood. 2001;97(12):3919–24.
Yu G, Corn PG, Shen PF, Song JH, Lee YC, Lin SC, et al. Retinoic acid receptor activation reduces metastatic prostate cancer bone lesions by blocking the endothelial-to-osteoblast transition. Cancer Res. 2022; can.22.0170
Bohnsack BL, Lai L, Dolle P, Hirschi KK. Signaling hierarchy downstream of retinoic acid that independently regulates vascular remodeling and endothelial cell proliferation. Genes Dev. 2004;18(11):1345–58.
Ciccone V, Terzuoli E, Donnini S, Giachetti A, Morbidelli L, Ziche M. Stemness marker ALDH1A1 promotes tumor angiogenesis via retinoic acid/HIF-1α/VEGF signalling in MCF-7 breast cancer cells. J Exp Clin Cancer Res CR.. 2018;12(37):311.
Bauer R, Udonta F, Wroblewski M, Ben-Batalla I, Santos IM, Taverna F, et al. Blockade of myeloid-derived suppressor cell expansion with all-trans retinoic acid increases the efficacy of antiangiogenic therapy. Cancer Res. 2018;78(12):3220–32.
Maziya-Dixon BB, Akinyele IO, Sanusi RA, Oguntona TE, Nokoe SK, Harris EW. Vitamin A deficiency is prevalent in children less than 5 y of age in Nigeria. J Nutr. 2006;136(8):2255–61. https://doi.org/10.1093/jn/136.8.2255.
Hall JA, Cannons JL, Grainger JR, Dos Santos LM, Hand TW, Naik S, et al. Essential role for retinoic acid in the promotion of CD4(+) T cell effector responses via retinoic acid receptor alpha. Immunity. 2011;34(3):435–47.
Raverdeau M, Mills KHG. Modulation of T cell and innate immune responses by retinoic acid. J Immunol. 2014;192(7):2953–8.
Zeng R, Bscheider M, Lahl K, Lee M, Butcher EC. Generation and transcriptional programming of intestinal dendritic cells: essential role of retinoic acid. Mucosal Immunol. 2016;9(1):183–93.
Zeng R, Oderup C, Yuan R, Lee M, Habtezion A, Hadeiba H, et al. Retinoic acid regulates the development of a gut-homing precursor for intestinal dendritic cells. Mucosal Immunol. 2013;6(4):847–56.
Klebanoff CA, Spencer SP, Torabi-Parizi P, Grainger JR, Roychoudhuri R, Ji Y, et al. Retinoic acid controls the homeostasis of pre-cDC-derived splenic and intestinal dendritic cells. J Exp Med. 2013;210(10):1961–76.
Saurer L, McCullough KC, Summerfield A. In vitro induction of mucosa-type dendritic cells by all-trans retinoic acid. J Immunol Baltim Md. 1950;179(6):3504–14.
Iwata M, Hirakiyama A, Eshima Y, Kagechika H, Kato C, Song SY. Retinoic acid imprints gut-homing specificity on T cells. Immunity. 2004;21(4):527–38.
Hammerschmidt SI, Friedrichsen M, Boelter J, Lyszkiewicz M, Kremmer E, Pabst O, et al. Retinoic acid induces homing of protective T and B cells to the gut after subcutaneous immunization in mice. J Clin Invest. 2011;121(8):3051–61.
Mora JR, Iwata M, Eksteen B, Song SY, Junt T, Senman B, et al. Generation of gut-homing IgA-secreting B cells by intestinal dendritic cells. Science. 2006;314(5802):1157–60.
Kim MH, Taparowsky EJ, Kim CH. Retinoic acid differentially regulates the migration of innate lymphoid cell subsets to the gut. Immunity. 2015;43(1):107–19.
Coombes JL, Siddiqui KRR, Arancibia-Cárcamo CV, Hall J, Sun CM, Belkaid Y, et al. A functionally specialized population of mucosal CD103+ DCs induces Foxp3+ regulatory T cells via a TGF-beta and retinoic acid-dependent mechanism. J Exp Med. 2007;204(8):1757–64.
Denning TL, Wang Y, chong, Patel SR, Williams IR, Pulendran B. Lamina propria macrophages and dendritic cells differentially induce regulatory and interleukin 17-producing T cell responses. Nat Immunol. 2007;8(10):1086–94.
Benson MJ, Pino-Lagos K, Rosemblatt M, Noelle RJ. All-trans retinoic acid mediates enhanced T reg cell growth, differentiation, and gut homing in the face of high levels of co-stimulation. J Exp Med. 2007;204(8):1765–74.
Mucida D, Park Y, Kim G, Turovskaya O, Scott I, Kronenberg M, et al. Reciprocal TH17 and regulatory T cell differentiation mediated by retinoic acid. Science. 2007;317(5835):256–60.
Kang SG, Lim HW, Andrisani OM, Broxmeyer HE, Kim CH. Vitamin a metabolites induce gut-homing FoxP3+ regulatory T cells. J Immunol Baltim Md. 1950;179(6):3724–33.
Sun CM, Hall JA, Blank RB, Bouladoux N, Oukka M, Mora JR, et al. Small intestine lamina propria dendritic cells promote de novo generation of Foxp3 T reg cells via retinoic acid. J Exp Med. 2007;204(8):1775–85.
Elias KM, Laurence A, Davidson TS, Stephens G, Kanno Y, Shevach EM, et al. Retinoic acid inhibits Th17 polarization and enhances FoxP3 expression through a Stat-3/Stat-5 independent signaling pathway. Blood. 2008;111(3):1013–20.
Seo GY, Jang YS, Kim HA, Lee MR, Park MH, Park SR, et al. Retinoic acid, acting as a highly specific IgA isotype switch factor, cooperates with TGF-β1 to enhance the overall IgA response. J Leukoc Biol. 2013;94(2):325–35.
Pino-Lagos K, Guo Y, Brown C, Alexander MP, Elgueta R, Bennett KA, et al. A retinoic acid-dependent checkpoint in the development of CD4+ T cell-mediated immunity. J Exp Med. 2011;208(9):1767–75.
Basu R, Whitley SK, Bhaumik S, Zindl CL, Schoeb TR, Benveniste EN, et al. IL-1 signaling modulates activation of STAT transcription factors to antagonize retinoic acid signaling and control the TH17 cell-iTreg cell balance. Nat Immunol. 2015;16(3):286–95.
DePaolo RW, Abadie V, Tang F, Fehlner-Peach H, Hall JA, Wang W, et al. Co-adjuvant effects of retinoic acid and IL-15 induce inflammatory immunity to dietary antigens. Nature. 2011;471(7337):220–4.
Allie SR, Zhang W, Tsai CY, Noelle RJ, Usherwood EJ. Critical role for all-trans retinoic acid for optimal effector and effector memory CD8 T cell differentiation. J Immunol Baltim Md. 1950;190(5):2178–87.
Guo Y, Pino-Lagos K, Ahonen CA, Bennett KA, Wang J, Napoli JL, et al. A retinoic acid—rich tumor microenvironment provides clonal survival cues for tumor-specific CD8+ T cells. Cancer Res. 2012;72(20):5230–9.
Bhattacharya N, Yuan R, Prestwood TR, Penny HL, DiMaio MA, Reticker-Flynn NE, et al. Normalizing microbiota-induced retinoic acid deficiency stimulates protective CD8(+) T cell-mediated immunity in colorectal Cancer. Immunity. 2016;45(3):641–55.
Devalaraja S, To TKJ, Folkert IW, Natesan R, Alam MZ, Li M, et al. Tumor-derived retinoic acid regulates Intratumoral monocyte differentiation to promote immune suppression. Cell. 2020;180(6):1098–1114.e16.
Binnewies M, Roberts EW, Kersten K, Chan V, Fearon DF, Merad M, et al. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat Med. 2018;24(5):541–50.
Veglia F, Sanseviero E, Gabrilovich DI. Myeloid-derived suppressor cells in the era of increasing myeloid cell diversity. Nat Rev Immunol. 2021;21(8):485–98.
Kusmartsev S, Cheng F, Yu B, Nefedova Y, Sotomayor E, Lush R, et al. All-trans-retinoic acid eliminates immature myeloid cells from tumor-bearing mice and improves the effect of vaccination. Cancer Res. 2003;63(15):4441–9.
Nefedova Y, Fishman M, Sherman S, Wang X, Beg AA, Gabrilovich DI. Mechanism of all-trans retinoic acid effect on tumor-associated myeloid-derived suppressor cells. Cancer Res. 2007;67(22):11021–8.
Iclozan C, Antonia S, Chiappori A, Chen DT, Gabrilovich D. Therapeutic regulation of myeloid-derived suppressor cells and immune response to cancer vaccine in patients with extensive stage small cell lung cancer. Cancer Immunol Immunother CII. 2013;62(5):909–18.
Rao E, Hou Y, Huang X, Wang L, Wang J, Zheng W, et al. All-trans retinoic acid overcomes solid tumor radioresistance by inducing inflammatory macrophages. Sci Immunol. 2021;6(60):eaba8426. https://doi.org/10.1126/sciimmunol.aba8426.
Tilsed CM, Casey TH, de Jong E, Bosco A, Zemek RM, Salmons J, et al. Retinoic Acid Induces an IFN-Driven Inflammatory Tumour Microenvironment, Sensitizing to Immune Checkpoint Therapy. Front Oncol. 2022;12:849793. https://doi.org/10.3389/fonc.2022.849793.
Li R, Salehi-Rad R, Crosson W, Momcilovic M, Lim RJ, Ong SL, et al. Inhibition of granulocytic myeloid-derived suppressor cells overcomes resistance to immune checkpoint inhibition in LKB1-deficient non-small cell lung Cancer. Cancer Res. 2021;81(12):3295–308.
Peng SY, Chen L, Deng RH, Li H, Liu XH, Zheng DW, et al. Non-depleting reformation of immunosuppressive myeloid cells to broaden the application of anti-PD therapy. Nanoscale. 2021;13(8):4420–31.
Tobin RP, Jordan KR, Robinson WA, Davis D, Borges VF, Gonzalez R, et al. Targeting myeloid-derived suppressor cells using all-trans retinoic acid in melanoma patients treated with Ipilimumab. Int Immunopharmacol. 2018;63:282–91.
Tobin RP, Cogswell DT, Cates VM, Davis DM, Borgers JSW, Van Gulick RJ, et al. Targeting MDSC differentiation using ATRA: a phase I/II clinical trial combining Pembrolizumab and all-trans retinoic acid for metastatic melanoma. Clin Cancer Res Off J Am Assoc Cancer Res. 2023;29(7):1209–19.
Heine A, Flores C, Gevensleben H, Diehl L, Heikenwalder M, Ringelhan M, Janssen KP, Nitsche U, Garbi N, Brossart P, Knolle PA, Kurts C, Höchst B. Targeting myeloid derived suppressor cells with all-trans retinoic acid is highly time-dependent in therapeutic tumor vaccination. Oncoimmunology. 2017;6(8):e1338995. https://doi.org/10.1080/2162402X.2017.1338995.
Liang Y, Wang W, Zhu X, Yu M, Zhou C. Inhibition of myeloid-derived suppressive cell function with all-trans retinoic acid enhanced anti-PD-L1 efficacy in cervical cancer. Sci Rep. 2022;12(1):9619. https://doi.org/10.1038/s41598-022-13855-1.
Hamilton MJ, Bosiljcic M, Lepard NE, Halvorsen EC, Ho VW, Banáth JP, et al. Macrophages are more potent immune suppressors ex vivo than immature myeloid-derived suppressor cells induced by metastatic murine mammary carcinomas. J Immunol Baltim Md. 1950;192(1):512–22.
Zhou Q, Xian M, Xiang S, Xiang D, Shao X, Wang J, et al. All-trans retinoic acid prevents osteosarcoma metastasis by inhibiting M2 polarization of tumor-associated macrophages. Cancer Immunol Res. 2017;5(7):547–59.
Koay DC, Zerillo C, Narayan M, Harris LN, DiGiovanna MP. Anti-tumor effects of retinoids combined with trastuzumab or tamoxifen in breast cancer cells: induction of apoptosis by retinoid/trastuzumab combinations. Breast Cancer Res BCR. 2010;12(4):R62.
Duranti S, Fabi A, Filetti M, Falcone R, Lombardi P, Daniele G, et al. Breast Cancer drug approvals issued by EMA: a review of clinical trials. Cancers. 2021;13(20):5198.
Ferguson KM, Gillen SL, Chaytor L, Poon E, Marcos D, Gomez RL, et al. Palbociclib releases the latent differentiation capacity of neuroblastoma cells. Dev Cell. 2023;58(19):1967–1982.e8.
Schultze E, Collares T, Lucas CG, Seixas FK. Synergistic and additive effects of ATRA in combination with different anti-tumor compounds. Chem Biol Interact. 2018;1(285):69–75.
Wang Q, Yang W, Uytingco MS, Christakos S, Wieder R. 1,25-Dihydroxyvitamin D3 and all-trans-retinoic acid sensitize breast Cancer cells to chemotherapy-induced cell Death1. Cancer Res. 2000;60(7):2040–8.
Lu Z, Ma L, Mei L, Ren K, Li M, Zhang L, et al. Micellar nanoparticles inhibit the postoperative inflammation, recurrence and pulmonary metastasis of 4T1 breast cancer by blocking NF-κB pathway and promoting MDSCs depletion. Int J Pharm. 2022;25(628):122303.
Sun R, Liu Y, Li SY, Shen S, Du XJ, Xu CF, et al. Co-delivery of all-trans-retinoic acid and doxorubicin for cancer therapy with synergistic inhibition of cancer stem cells. Biomater. 2015;1(37):405–14.
Merino VF, Nguyen N, Jin K, Sadik H, Cho S, Korangath P, et al. Combined treatment with epigenetic, differentiating, and chemotherapeutic agents cooperatively targets tumor-initiating cells in triple-negative breast Cancer. Cancer Res. 2016;76(7):2013–24.
Huang H, Shi H, Liu J, Min Y, Wang Y, Wang AZ, et al. Co-delivery of all-trans-retinoic acid enhances the anti-metastasis effect of albumin-bound paclitaxel nanoparticles. Chem Commun Camb Engl. 2016;53(1):212–5.
Xie X, Jiang K, Li B, Hou S, Tang H, Shao B, et al. A small-molecule self-assembled nanodrug for combination therapy of photothermal-differentiation-chemotherapy of breast cancer stem cells. Biomaterials. 2022;1(286):121598.
Sutton LM, Warmuth MA, Petros WP, Winer EP. Pharmacokinetics and clinical impact of all-trans retinoic acid in metastatic breast cancer: a phase II trial. Cancer Chemother Pharmacol. 1997;40(4):335–41.
Budd GT, Adamson PC, Gupta M, Homayoun P, Sandstrom SK, Murphy RF, et al. Phase I/II trial of all-trans retinoic acid and tamoxifen in patients with advanced breast cancer. Clin Cancer Res Off J Am Assoc Cancer Res. 1998;4(3):635–42.
Bryan M, Pulte ED, Toomey KC, Pliner L, Pavlick AC, Saunders T, et al. A pilot phase II trial of all-trans retinoic acid (Vesanoid) and paclitaxel (Taxol) in patients with recurrent or metastatic breast cancer. Investig New Drugs. 2011;29(6):1482–7.
Toma S, Raffo P, Nicolo G, Canavese G, Margallo E, Vecchio C, et al. Biological activity of all-trans-retinoic acid with and without tamoxifen and alpha-interferon 2a in breast cancer patients. Int J Oncol. 2000;17(5):991–1000.
Costantini L, Molinari R, Farinon B, Merendino N. Retinoic Acids in the Treatment of Most Lethal Solid Cancers. J Clin Med. 2020;9(2):360. https://doi.org/10.3390/jcm9020360.
Lyra-Leite DM, Gutiérrez-Gutiérrez Ó, Wang M, Zhou Y, Cyganek L, Burridge PW. A review of protocols for human iPSC culture, cardiac differentiation, subtype-specification, maturation, and direct reprogramming. STAR Protoc. 2022;3(3):101560.
Koterazawa Y, Koyanagi-Aoi M, Uehara K, Kakeji Y, Aoi T. Retinoic acid receptor γ activation promotes differentiation of human induced pluripotent stem cells into esophageal epithelium. J Gastroenterol. 2020;55(8):763–74.
Acknowledgments
We would like to thank the Associazione Italiana per la Ricerca sul Cancro (AIRC) for the funding to Enrico Garattini (Project code n° 22963).
Funding
Associazione Italiana per la Ricerca sul Cancro (AIRC), PI Enrico Garattini (Project code n° 22963).
Author information
Authors and Affiliations
Contributions
G.P. wrote the initial paper. MA.C., A.Z., M.T. and E.G., reviewed and significantly contributed to the final paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Caricasulo, M.A., Zanetti, A., Terao, M. et al. Cellular and micro-environmental responses influencing the antitumor activity of all-trans retinoic acid in breast cancer. Cell Commun Signal 22, 127 (2024). https://doi.org/10.1186/s12964-024-01492-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12964-024-01492-2