
Abstract
Background
Many advantages of hospital at home (HaH), as a modality of acute care, have been highlighted, but controversies exist regarding the cost-benefit trade-offs. The objective is to assess health outcomes and analytical costs of hospital avoidance (HaH-HA) in a consolidated service with over ten years of delivery of HaH in Barcelona (Spain).
Methods
A retrospective cost-consequence analysis of all first episodes of HaH-HA, directly admitted from the emergency room (ER) in 2017–2018, was carried out with a health system perspective. HaH-HA was compared with a propensity-score-matched group of contemporary patients admitted to conventional hospitalization (Controls). Mortality, re-admissions, ER visits, and direct healthcare costs were evaluated.
Results
HaH-HA and Controls (n = 441 each) were comparable in terms of age (73 [SD16] vs. 74 [SD16]), gender (male, 57% vs. 59%), multimorbidity, healthcare expenditure during the previous year, case mix index of the acute episode, and main diagnosis at discharge. HaH-HA presented lower mortality during the episode (0 vs. 19 (4.3%); p < 0.001). At 30 days post-discharge, HaH-HA and Controls showed similar re-admission rates; however, ER visits were lower in HaH-HA than in Controls (28 (6.3%) vs. 34 (8.1%); p = 0.044). Average costs per patient during the episode were lower in the HaH-HA group (€ 1,078) than in Controls (€ 2,171). Likewise, healthcare costs within the 30 days post-discharge were also lower in HaH-Ha than in Controls (p < 0.001).
Conclusions
The study showed higher performance and cost reductions of HaH-HA in a real-world setting. The identification of sources of savings facilitates scaling of hospital avoidance.
Registration
ClinicalTrials.gov (26/04/2017; NCT03130283).
Similar content being viewed by others


Introduction
Over the last twenty years, hospital at home (HaH) has reached maturity in various health systems worldwide [1,2,3],. Specific HaH programs in USA [4,5,6] and Australia [7,8,9,10] have played a leading role in contributing to the definition of the characteristics and the main challenges [5] of this modality of care. However, important differences are acknowledged among [1] and within countries [11], in terms of patients’ profiles, care delivery and reimbursement regimes. This service is currently considered a consolidated alternative to inpatient care for selected patients requiring hospital admission [4]. Furthermore, HaH has shown high potential to promote continuity of care by preventing hospitalizations and reinforcing transitional care after discharge [12, 13], thus enabling vertical integration between hospital and community-based care [14, 15].
Despite the promising results and potential benefits associated with HaH, some controversies have been raised regarding the extent of the value generation in healthcare [16,17,18]. These discrepancies are partly explained by differences in the complexity of target patients and service delivery context, with important implications regarding the characterization of its different modalities, reimbursement regimes, and adoption strategies [5, 19, 20]. This heterogeneous scenario stresses the need for investigating real-world experiences in implementing and deploying HaH services.
In our center, a university hospital providing specialized care to a catchment population of 520,000 citizens, HaH was implemented in 2006 as a mainstream service across specialties covering two modalities of HaH: hospital avoidance (HaH-HA) and early discharge (HaH-ED) [15, 21, 22]. The service provides acute, home-based, short-term care aiming at either entirely replacing conventional hospitalization (hospital avoidance) or accelerating discharge (early discharge). This model was progressively implemented across the entire healthcare system in our region between 2011 and 2015, with preliminary positive results [23,24,25]. These positive results prompted the Catalan Health Service, the only public health payer providing universal healthcare to the 7.7 million population, to scale up the HaH service across the region and set a specific reimbursement model between 2016 and 2020 [26].
The long-lasting experience with HaH service and analytical accounting used in our center sets a privileged scenario to investigate the benefits and costs associated with this service. Therefore, we conducted a cost-consequence analysis (CCA) [20] of all first episodes of HaH-HA registered within a one-year course after more than one decade of implementation and consolidation of the HaH service in our center.
The current study is one of the core components of a broader research endeavor conducted in Catalonia (Spain) to analyze different key dimensions of the HaH services. That is, (i) assessment of healthcare value generation using a Triple Aim approach [27], (ii) evaluation of HaH over a five-year period, 2015–2019, in the 27 service providers at the regional level [11], (iii) predictive modelling for service selection and personalized transitional care after discharge [21, 28], and (iv) analysis of the potential for generalization of the service across the OECD countries [29].
Methods
Study groups and design
This was a retrospective CCA of all first-time HaH-HA admissions issued from the emergency room department (ER) in the Hospital Clínic of Barcelona (HCB) among non-surgical patients between October 31, 2017, and November 1, 2018. The direct costs and outcomes of HaH-HA patients were compared with a 1:1 matched comparator group of conventional hospitalizations in our center. Patients under the modality HaH-ED were excluded from the analysis.
Candidates to HaH-HA were screened in the ER by trained professionals of the HaH team. Individuals were eligible for HaH-HA if: they were aged 18 years or older, lived in their house within the catchment area, had a formal or informal caretaker (including relatives) available 24 h per day, had a phone at home and signed the informed consent to be hospitalized at home. We considered all medical conditions.
The comparator group (controls) was built from non-surgical patients admitted for conventional hospitalization from the ER within the same period. We paired HaH-HA patients with control patients 1:1 using a propensity score matching (PSM) [30, 31] and genetic-matching technique [32]. For matching purposes, we took into account two sets of matching variables to ensure patients’ comparability regarding both baseline characteristics (i.e., before admission) and hospitalization characteristics.
The first set of matching variables included age, gender, number of admissions in the previous year, patient’s healthcare costs across the health system in the previous year, and health risk based on the adjusted morbidity groups (AMG) index [33]. The AMG is a summary measure of morbidity that considers a weighted sum of all chronic and relevant acute conditions from all diagnostic group codes of the International Classification of Diseases, clinical modification (ICD-10-CM). The AMG can be used as a numerical index or as population-based risk groups, defined according to percentile thresholds for the distribution of the AMG index across the entire population of Catalonia. Both the index and the risk groups have shown a good correlation with relevant health outcomes and the use of healthcare resources [34, 35].
The second set of variables for paring HaH-HA and control patients included relevant characteristics of the hospitalization episode, such as the main diagnosis at discharge based on the ICD-10-CM categories and the case mix index (CMI). The CMI summarizes the severity and complexity of the main diagnosis and health events occurring during the hospital stay.
Characteristics of home and conventional hospitalizations
The HaH-HA group followed the standard of care for HaH at HCB, which has been extensively reported elsewhere [24]. Briefly, a patient admitted to HaH-HA is assessed in person daily by the HaH team, which consists of either a nurse or a nurse and physician (at physician’s discretion) with remote access to the patient’s electronic record. Interventions available at home include regular tests (e.g., blood and microbiology tests, clinical ultrasound, electrocardiogram), most of the intravenous and nebulized treatments, and oxygen therapy. A pathway for elective transfer back to the hospital (e.g., for additional tests not available at home) and ER transfer in case of clinical deterioration are also available.
The control group followed the usual care for in-house hospitalizations; patients were assigned to a hospital bed within the corresponding service according to the primary diagnosis and followed up by the medical and nurse staff of the corresponding ward or service.
Upon discharge, patients in the two groups were transferred to the corresponding primary care teams, with access to electronic health records. However, the HaH team shares responsibilities with the primary care team during the transitional care period until 30 days after discharge.
Outcomes and costs
The CCA included health outcomes and direct costs [36] expressed as 2017 euros (€). Despite the study was constrained to the analysis of one center (HCB), a health system perspective was adopted. Health outcomes included length of hospital stay, 30-day mortality, and all-cause hospital admissions and visits to the ER within the 30 following discharge. In patients admitted to HaH-HA, we also collected the patient experience by administering a 9-item satisfaction questionnaire [24] on discharge.
Costs were estimated using an analytical accounting approach [37]. Direct costs included honoraria of staff professionals, pharmacological and non-pharmacological therapy, consumables, testing and procedures, transportation, catering, and structural costs. We also considered healthcare expenditure associated with any resource use of the healthcare system during the 30 days following discharge.
The two data sources used for the study were: the SAP Health Information System at HCB and the Catalan Health Surveillance System (CHSS) for analysis of the acute episode and calculations after discharge, respectively.
Deployment of HaH
The process of deployment of the service was analyzed using the Consolidated Framework for Implementation Research (CFIR) [38, 39]. Two sequential periods were considered: 2006–2015, adoption at HCB [24], and 2016–2018, expansion of HaH to the entire integrated care district of Barcelona-Esquerra (520 k citizens) [40].
Data analysis
Health outcomes and costs were described by the number and percentage over available data for categorical variables and mean and standard deviation (SD), or median and interquartile range (IQR, defined by the 25th and 75th percentiles), as appropriate. The matching parameters were tuned to enhance the covariate balancing, as follows: caliper: 0.2, function: logit, replace: FALSE, ratio: 1:1, matching method: Genetic Matching. Genetic Matching uses an optimization algorithm based on “GENetic Optimization Using Derivatives (GENOUD)” [41] to check and improve covariate balance iteratively, and it is a generalization of propensity score and Mahalanobis distance [42]. The matching was assessed by the Mahalanobis distance, Rubin’s B (the absolute standardized difference of the means of the linear index of the propensity score in the HaH-HA and Controls) and Rubin’s R [43] (the ratio of HaH-HA to Controls variances of the propensity score index) metrics. Quality of comparability between HaH-HA and Controls after PSM was considered acceptable if Rubin’s B was less than 0.25 and Rubin’s R was between 0.5 and 2. Unpaired Student T tests, Mann-Whitney, and Chi-squared tests comparing HaH-HA with Controls were used to assess changes in the costs and clinical outcomes. Data analyses were conducted using R [44], version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria). The threshold for significance was set at a two-sided alpha value of 0.05.
Results
Study participants
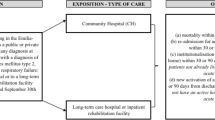
During the study period, the ER department dictated 586 unplanned non-surgical HaH-HA admissions in patients without previous episodes of HaH. The comparator group was built using a dataset of 2,631 conventional non-surgical admissions carried out during the study period. After propensity score matching, the two groups: HaH-HA and Controls, consisted of 441 cases each (Fig. 1).

Number and distribution of patients. Five-hundred eighty-six first episodes of HaH admissions, directly from the Emergency Room (HaH-HA), were registered during the study period. After propensity score matching, the HaH-HA group fell to 441 patients (Comparisons among the two study groups and the study population of 586 patients are reported in Tables 1S, 3 S and 4 S, see text for details)
We found no significant differences between the characteristics of the HaH-HA selected for the propensity-score matching (n = 441) and those of the entire series of patients admitted to HaH-HA within the investigated period (n = 586) (Table S1). Table 1 summarizes the baseline characteristics before admission, of individuals included in the HaH-HA and the comparator group. The two groups were well balanced regarding their demographic characteristics and previous use of hospital resources and healthcare expenditure. The health risk on admission, measured using the AMG index, was also similar between groups. However, the stratification of patients across the population-based categories of health risk showed that the HaH-HA had a higher percentage of individuals in the intermediate-risk group and a lower percentage of individuals in the high-risk group than the control group.
Hospitalization characteristics and outcomes
The main diagnosis at discharge in the two groups, HaH-HA and Controls, showed the same distribution of percentages across the ICD-10-CM disease groups: 25% were urinary tract infections, 15% chronic respiratory diseases, 13% pneumonia, 11% acute lower respiratory tract infections, 9% heart failure, 8% skin infections, 6% flu, 3% symptoms, injury, and poisoning, 3% hypertensive disease and other heart diseases, 3% pneumonitis caused by bronchial aspiration, 4% other conditions requiring admission. Detailed information is provided in Table 2S.
The characteristics of the acute hospitalization episode are summarized in Table 2. The two groups had similar CMI and length of stay. However, mortality during the acute episode was higher among patients with conventional hospitalization. Notably, no home-based fatalities were registered. However, in the HaH-HA group, 6 (1.4%) patients worsened their clinical condition during the episode, requiring a visit to the ER department and returning home. Likewise, 18 (4.1%) patients discontinued HaH-HA for similar reasons and were admitted to conventional hospitalization, all of them were successfully discharged. The administration of the satisfaction questionnaire to patients admitted to HaH-HA revealed that 97% were highly satisfied with the service (Figure S1). Comprehensive information on the acute episode is provided in Table 3 S.
Mortality and hospital admissions for any cause within the 30 days following discharge were similar in the two groups (Table 2). However, the conventional hospitalization group reported a significantly higher percentage of all-cause visits to the emergency room within the 30-day post-discharge period.
Healthcare costs
The total direct costs associated with the hospitalization episodes were € 475k and € 957k for the HaH-HA and comparator groups, respectively. Figure 2 displays the direct cost per patient (average according to concepts and cost distribution across each group). In the two groups, direct costs associated with staff salaries accounted for the greatest proportion of all items. The average cost per episode was € 1,078 and € 2,171 (p < 0.001) for HaH-HA and conventional hospitalization episodes, respectively. Cost savings per episode in HaH-HA compared to conventional hospitalization were mostly attributable to staff (€ 867 vs. € 1,539; p < 0.001), followed by catering (€ 0 vs. € 149), infrastructure (€ 13 vs. € 151; P < 0.001), testing (€ 21 vs. € 124; p < 0.001), and consumables (€ 31 vs. € 89; p < 0.001). HaH-HA had no statistically significant impact on costs associated with the treatment (€ 110 vs. € 119; p = 0.662). Contrarily, compared to usual care, HaH-HA showed significantly increased costs on staff transportation (€ 36 vs. € 0). In the HaH-HA group, none of the patients or their relatives required additional external support during the hospitalization episode. Transportation to the hospital, when needed, was afforded by the public healthcare payer.

Average cost per pacient. In the left panel, the two columns indicate the average cost per patient for HaH-HA (Hospital at Home-Hospital Avoidance) and matched Controls (conventional hospitalizations), respectively. The colors indicate the weight of the different cost components (see text for details). The right panel depicts the box plots of the cost analysis
The general healthcare expenditure within the 30 days following discharge was significantly lower in individuals admitted to HaH-HA than those with conventional hospitalization (€ 764 vs. € 1,022; P < 0.001). For the two groups, all post-discharge healthcare costs were afforded by the public healthcare payer; no indirect costs afforded by patients or their relatives were considered in the analysis. Table S4 provides a detailed list of costs associated with healthcare resource consumption within the 30 days following discharge.
The summary description of the deployment of HaH is depicted in the on-line supplementary material (Table 5 S).
Discussion
Main findings
In this control-matched comparison of HaH-HA and conventional hospitalization in a real-world setting, we found that HaH-HA was associated with lower visits to the emergency room within the 30 days following discharge. The overall cost per episode was nearly half in the HaH-HA compared with conventional hospitalization. This cost reduction was primarily attributed to staff, catering, infrastructure, and testing. Likewise, patients admitted for a HaH-HA showed significantly lower healthcare expenditure within the 30 days following discharge.
The accompanying studies on HaH-HA carried out at HCB [21, 27, 28] and at regional level [11, 29] during the period have provided a comprehensive picture of the modality of care and contributed to identify future directions toward quality assurance of the service delivery. While the current report provides analytical costs for the entire population of HaH patients attended at HCB during the study period, the Triple Aim assessment done in a subset of these patients [27] confirmed health value generation of HaH-HA reporting a positive impact on patient reported outcomes and patient reported experience. The message was further endorsed by the studies done using regional data [11, 29] wherein both health professionals’ engagement and users’ satisfaction were confirmed by a qualitative analysis of the service. The study by Gonzalez-Colom et al [11] reported a structured analysis of the heterogeneities of HaH-HA within the Catalan health system and proposed key performance indicators (KPI) for quality assurance of the service. We understand that the cost analysis described in the current study may contribute to formulate future reimbursement incentives aiming at reducing the heterogeneities of HaH-HA. The OECD report [29], based on modelling of regional data, produced relevant outcomes: (i) Confirming health value generation of HaH-HA, as well as its scalability, (ii) Quantifying the potential for cost savings of HaH-HA at health system level, and (iii) Identifying high level requirements for the service deployment with emphasis on potential inequities associated to limited HaH-HA accessibility for socially vulnerable patients. Last, but not least, the two studies assessing the role of predictive modelling for selection of candidates for HaH-HA [21] and enhanced transitional care after discharge [28] pave the way toward implementation of digital tools for clinical support of service delivery.
The health outcomes of the current study are in the upper range of care quality of HaH studies in Europe [45, 46] US [6, 47, 48], and Australia [7,8,9,10]. Furthermore, the maturity of both integrated care and digital support in Catalonia may positively influence the success of implementation and adoption strategies [15]. The change management with digital support of the service, which was gradually implemented in the early phases of HaH [24, 49] but accelerated during the study period, may have contributed to cost reduction and improved health outcomes observed in our analysis.
Strengths and limitations
The control-matched approach adopted in the current study required ruling out 145 patients out of the 586 episodes of HaH-HA within the investigated period. However, our analysis of the baseline characteristics showed no differences with the final analysis dataset; therefore, we do not expect this exclusion to limit the representativeness of our cohort. Other strengths of our analysis include the possibility of collecting integrated data regarding healthcare resource utilization (including primary care) before and after the hospitalization episode, as well as using of analytical accounting for the cost analysis. This approach provided a detailed picture of costs, which is impossible with case-mix payment tools, such as the diagnostic risk groups used in several reports.
However, we fully acknowledge the intrinsic limitations of the matching, which could be successfully done for the baseline characteristics of the patients but was limited in terms of severity of the acute episodes. Clearly, the clinical judgement of health professionals in the Emergency Room Department selecting candidates for HaH-HA is a critical variable that cannot be considered in the propensity score matching techniques. Nevertheless, we believe that this limitation does not hamper the conclusions drawn from the current cost analysis.
The study was also limited to the assessment of the direct costs of the healthcare provider, losing sight of indirect costs (e.g., home careers, etc…). More importantly, we could not gather societal costs or economic burdens for caretakers or patients’ relatives which constitutes a complex endeavor with low potential for generalization. We acknowledge that these variables may have relevant implications for the actual quality of care associated with availability of informal care [29]. Therefore, our cost-consequence analysis from the healthcare provider and healthcare system perspective shall be expanded in the future site implementations by including all these indirect and societal factors influencing accessibility to the service.
Perspectives
Aside from highlighting the need for a more comprehensive analysis of costs, our study paves the way to identifying key performance indicators that consider both site-specific and general features and allow for continuous monitoring of HaH performance. Another aspect of HaH to be explored is the implications of this type of care for improving the continuity of care by fostering vertical integration (i.e., between specialized and community-based care) and horizontal integration (i.e., between healthcare and social care). Although the role of HaH in these integrations was out of the scope of our analysis, health professionals working in a HaH are a natural bridge between specialized and community-based care during the transitional period during and after discharge [50]. Hence, HaH should be promoted as a facilitator of integrated care pathways, and future studies should investigate the contribution of HaH to maintaining the continuity of care in these transitions.
Conclusions
Our research indicates that HaH-HA adds overall value to healthcare providers and the healthcare system. The results of the current cost analysis can contribute to finetune reimbursement incentives aiming at enhancing the service delivery. The constellation of intertwined studies assessing HaH in Catalonia provide a comprehensive perspective of HaH that should be useful for transferability of this modality of care to other sites ensuring sustainable adoption and high quality of service delivery.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- HaH:
-
Hospital at home
- HaH-HA:
-
Hospital avoidance
- HaH-ED:
-
Early discharge
- CCA:
-
Cost-consequence analysis
- CFIR:
-
Consolidated Framework for Implementation Research
- HCB:
-
Hospital Clínic of Barcelona
- PSM:
-
Propensity score matching
- AMG:
-
Adjusted morbidity groups
- CMI:
-
Case mix index
- CHSS:
-
Catalan Health Surveillance System
- GENOUD:
-
GENetic Optimization Using Derivatives
References
Leong MQ, Lim CW, Lai YF. Comparison of Hospital-at-home models: a systematic review of reviews. BMJ Open. 2021;11:e043285.
Conley J, O’Brien CW, Leff BA, Bolen S, Zulman D. Alternative strategies to Inpatient hospitalization for Acute Medical conditions. JAMA Intern Med. 2016;176:1693.
Qaddoura A, Yazdan-Ashoori P, Kabali C, Thabane L, Haynes RB, Connolly SJ et al. Efficacy of Hospital at Home in Patients with Heart Failure: A Systematic Review and Meta-Analysis. Abete P, editor. PLoS One. 2015;10:e0129282.
Leff B. Defining and disseminating the hospital-at-home model. Can Med Assoc J. 2009;180:156–7.
Leff B, DeCherrie LV, Montalto M, Levine DM. A research agenda for hospital at home. J Am Geriatr Soc. 2022;70:1060–9.
Leff B, Burton L, Mader SL, Naughton B, Burl J, Inouye SK et al. Hospital at home: feasibility and outcomes of a program to provide hospital-level care at home for acutely III older patients. Ann Intern Med. 2005;143.
Montalto M. The 500-bed hospital that isn’t there: the Victorian Department of Health review of the hospital in the home program. Med J Aust. 2010. p. 598–601.
Montalto M, McElduff P, Hardy K. Home ward bound: features of hospital in the home use by major Australian hospitals, 2011–2017. Med J Aust 213:22–7.
Montalto M, Lui B, Mullins A, Woodmason K. Medically-managed hospital in the home: 7 year study of mortality and unplanned interruption. Aust Health Rev Aug;34(3).
Hecimovic A, Matijasevic V, Frost SA. Characteristics and outcomes of patients receiving hospital at Home Services in the South West of Sydney. BMC Health Serv Res 20.
González-Colom R, Carot-Sans G, Vela E, Espallargues M, Hernández C, Jiménez FX et al. Five years of hospital at Home adoption in Catalonia: impact and challenges. medRxiv. 2023;2023.01.25.23284997.
V DeCherrie L, Wajnberg A, Soones T, Escobar C, Catalan E, Lubetsky S, et al. Hospital at Home-Plus: a platform of facility-based care. J Am Geriatr Soc. 2019;J Am Geriatr Soc:596–602.
Federman AD, Soones T, DeCherrie LV, Leff B, Siu AL. Association of a Bundled Hospital-at-home and 30-Day postacute Transitional Care Program with Clinical outcomes and patient experiences. JAMA Intern Med. 2018;178:1033.
Heeringa J, Mutti A, Furukawa MF, Lechner A, Maurer KA, Rich E. Horizontal and Vertical Integration of Health Care Providers: a Framework for understanding various provider organizational structures. Int J Integr Care. 2020;20:2.
Hernandez C, Alonso A, Garcia-Aymerich J, Grimsmo A, Vontetsianos T, García Cuyàs F. Integrated care services: lessons learned from the deployment of the NEXES project. Int J Integr Care 15:15e006.
Shepperd S, Iliffe S, Doll HA, Clarke MJ, Kalra L, Wilson AD et al. Admission avoidance hospital at home. Cochrane Database Syst Reviews. 2016;1.
Gonçalves-Bradley DC, Iliffe S, Doll HA, Broad J, Gladman J, Langhorne P, et al. Early discharge hospital at home. Cochrane Database Syst Reviews. 2017;2021:7.
Goossens LMA, Vemer P, Rutten-van Mölken MPMH. The risk of overestimating cost savings from hospital-at-home schemes: a literature review. Int J Nurs Stud. 2020;109:103652.
DeCherrie LV, Leff B, Levine DM, Siu A. Hospital at home: setting a Regulatory Course to Ensure Safe, High-Quality Care. Joint Comm J Qual Patient Saf. 2022;48:180–4.
Hartfiel N, Edwards RT. Cost–consequence analysis of public health interventions. Applied Health Economics for Public Health Practice and Research. Oxford University Press; 2019. pp. 233–47.
Calvo M, González R, Seijas N, Vela E, Hernández C, Batiste G, et al. Health outcomes from home hospitalization: Multisource predictive modeling. J Med Internet Res. 2020;22:e21367.
Hernandez C, Alonso A, Garcia-Aymerich J, Grimsmo A, Vontetsianos T, García Cuyàs F, et al. Integrated care services: lessons learned from the deployment of the NEXES project. Int J Integr Care. 2015;15:1.
Arias-de la Torre J, Zioga EAM, Macorigh L, Muñoz L, Estrada O, Mias M, et al. Differences in results and related factors between Hospital-At-Home modalities in Catalonia: a cross-sectional study. J Clin Med. 2020;9:1461.
Hernández C, Aibar J, Seijas N, Puig I, Alonso A, Garcia-Aymerich J et al. Implementation of home hospitalization and early discharge as an integrated care service: a ten years pragmatic assessment. Int J Integr Care. 2018;18.
Catalan Ministry of Health. Health Plan for Catalonia 2011–2015 [Internet]. 2012 [cited 2024 Jan 28]. Available from: https://scientiasalut.gencat.cat/bitstream/handle/11351/5519/pla_salut_catalunya_2011_2015_ang.pdf?sequence=3&isAllowed=y
Catalan Health Service. Organisational model for Hospital at Home in Catalonia [Internet]. [cited 2024 Jan 28]. Available from: https://scientiasalut.gencat.cat/bitstream/handle/11351/9073/model_organitzatiu_hospitalitzacio_domicili_catalunya_alternativa_hospitalitzacio_convencional_2020_an.pdf?sequence=2&isAllowed=y.%20Cited:%2017/03/2023
Herranz C, González-Colom R, Baltaxe E, Seijas N, Asenjo M, Hoedemakers M et al. Prospective cohort study for assessment of integrated care with a triple aim approach: hospital at home as use case. BMC Health Serv Res. 2022;22.
González-Colom R, Herranz C, Vela E, Monterde D, Contel JC, Sisó-Almirall A, et al. Prevention of unplanned hospital admissions in multimorbid patients using computational modeling: observational retrospective cohort study. J Med Internet Res. 2023;25:e40846.
OCDE. Hospital-at-Home (H@H), Catalonia, Spain, in Integrating Care to Prevent and Manage Chronic Diseases: Best Practices in Public Health. Integrating Care to Prevent and Manage Chronic Diseases. 2023. https://doi.org/10.1787/9acc1b1d-en.
Austin PC. An introduction to Propensity score methods for reducing the effects of confounding in Observational studies. Multivar Behav Res. 2011;46:399–424.
Tsiachristas A, Ellis G, Buchanan S, Langhorne P, Stott DJ, Shepperd S. Should I stay or should I go? A retrospective propensity score-matched analysis using administrative data of hospital-at-home for older people in Scotland. BMJ Open. 2019;9:e023350.
Diamond A, Sekhon JS. Genetic matching for estimating Causal effects: a General Multivariate Matching Method for Achieving Balance in Observational studies. Rev Econ Stat. 2013;95:932–45.
Espieén ID, Vela E, Pauws S, Bescos C, Cano I, Cleries M et al. Proposals for enhanced health risk assessment and stratification in an integrated care scenario. BMJ Open. 2016;6.
Vela E, Clèries M, Monterde D, Carot-Sans G, Coca M, Valero-Bover D et al. Performance of Quantitative Measures of Multimorbidity: A Population-Based Retrospective Analysis. BMC Public Health. 2021;10.21203/rs.3.rs-209438/v1.
Monterde D, Vela E, Clèries M, Garcia-Eroles L, Roca J, Pérez-Sust P. Multimorbidity as a predictor of health service utilization in primary care: a registry-based study of the Catalan population. BMC Fam Pract. 2020;21:39.
Office of the European Union. Defining value in. ‘value-based healthcare’ [Internet]. 2019 [cited 2024 Jan 28]. Available from: https://op.europa.eu/en/publication-detail/-/publication/d7087e5e-ac2b-11e9-9d01-01aa75ed71a1.
Barberan-Garcia A, Ubre M, Pascual-Argente N, Risco R, Faner J, Balust J, et al. Post-discharge impact and cost-consequence analysis of prehabilitation in high-risk patients undergoing major abdominal surgery: secondary results from a randomised controlled trial. Br J Anaesth. 2019;123:450–6.
Warner G, Lawson B, Sampalli T, Burge F, Gibson R, Wood S. Applying the consolidated framework for implementation research to identify barriers affecting implementation of an online frailty tool into primary health care: a qualitative study. BMC Health Serv Res. 2018;18.
Kirk MA, Kelley C, Yankey N, Birken SA, Abadie B, Damschroder L. A systematic review of the use of the Consolidated Framework for Implementation Research. Implement Sci. 2016;11:1–13.
Font D, Escarrabill J, Gómez M, Ruiz R, Enfedaque B, Altimiras X. Integrated Health Care Barcelona Esquerra (Ais-Be): a global view of organisational development, re-engineering of processes and improvement of the information systems. The role of the tertiary university hospital in the transformation. Int J Integr Care. 2016;16.
Mebane WR, Sekhon JS. Genetic optimization using derivatives: the Rgenoud Package for R. JSS J Stat Softw. 2022;2011:42.
De Maesschalck R, Jouan-Rimbaud D, Massart DL. The mahalanobis distance. Chemometr Intell Lab Syst. 2000;50:1–18.
Rubin DB. Using propensity scores to help design observational studies: application to the tobacco litigation. Health Serv Outcomes Res Methodol. 2001;2:169–88.
R Core Team. R: A language and environment for statistical com-puting. R Foundation for Statistical Computing, Vienna, Austria. 2021.
Echevarria C, Gray J, Hartley T, Steer J, Miller J, Simpson AJ, et al. Home treatment of COPD exacerbation selected by DECAF score: a non-inferiority, randomised controlled trial and economic evaluation. Thorax. 2018;73:713–22.
Ponce González MA, Mirón Rubio M, Mujal Martinez A, Estrada Cuxart O, Fiuza Perez D, Salas Reinoso L, et al. Effectiveness and safety of outpatient parenteral antimicrobial therapy in acute exacerbation of chronic obstructive pulmonary disease. Int J Clin Pract. 2017;71:e13022.
Levine DM, Ouchi K, Blanchfield B, Saenz A, Burke K, Paz M, et al. Hospital-Level Care at Home for acutely ill adults. Ann Intern Med. 2020;172:77.
Cryer L, Shannon SB, Van Amsterdam M, Leff B. Costs for ‘Hospital At Home’ patients were 19% lower, with Equal or Better outcomes compared to similar inpatients. Health Aff. 2012;31:1237–43.
Hernandez C, Casas A, Escarrabill J, Alonso J, Puig-Junoy J, Farrero E, et al. Home hospitalisation of exacerbated chronic obstructive pulmonary disease patients. Eur Respir J. 2003;21:58–67.
Rennke S, Nguyen OK, Shoeb MH, Magan Y, Wachter RM, Ranji SR. Hospital-Initiated Transitional Care interventions as a Patient Safety Strategy. Ann Intern Med. 2013;158:433.
Acknowledgements
Thanks to all the HaH professionals who believe in the service and the patients and their families for trusting them. As well as CatSalut to boost its deployment.
Funding
This article was funded by JADECARE project- HP-JA-2019 - Grant Agreement nº 951442 (2020–2023), a European Union’s Health Program 2014–2020.
The funding body doesn’t have any role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
RG, IC, MCH, EV, MA, EB, NS, EC, JF, DN, JR and CH contributed to the preparation of this manuscript. RG, IC, MCH, EV, MA, EB, NS, EC, JF, DN, GC, JR and CH reviewed the full assessment report as well as this article, and can act as a guarantor for the overall content. MCH, GC, JC, RG and CH contributed to the sections relating to development of guidance and consultation and reviewed the manuscript for accuracy.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethical Committee for Human Research at Hospital approved the study protocol (refs. 2017 − 0451 and 2017 − 0452). All methods were conducted in accordance with the relevant guidelines and regulations, including the General Data Protection Regulation 2016/679 on data protection and privacy for all individuals within the European Union and the local regulatory framework regarding data protection.
Consent for publication
Not applicable.
Competing interests
All authors have disclosed no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hernandez, C., Herranz, C., Baltaxe, E. et al. The value of admission avoidance: cost-consequence analysis of one-year activity in a consolidated service. Cost Eff Resour Alloc 22, 30 (2024). https://doi.org/10.1186/s12962-024-00536-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12962-024-00536-1