
Abstract
Introduction
Community health workers (CHWs) are vital resources in delivering community-based primary health care, especially in low-and-middle-income countries (LMIC). However, few studies have investigated detailed time and task assessments of CHW's work. We conducted a time-motion study to evaluate CHWs' time on health conditions and specific tasks in Neno District, Malawi.
Methods
We conducted a descriptive quantitative study utilizing a time observation tracker to capture time spent by CHWs on focused health conditions and tasks performed during household visits. We observed 64 CHWs between 29 June and 20 August 2020. We computed counts and median to describe CHW distribution, visit type, and time spent per health condition and task. We utilized Mood’s median test to compare the median time spent at a household during monthly visits with the program design standard time. We used pairwise median test to test differences in median time duration for health conditions and assigned tasks.
Results
We observed 660 CHW visits from 64 CHWs, with 95.2% (n = 628) of the visits as monthly household visits. The median time for a monthly household visit was 34 min, statistically less than the program design time of 60 min (p < 0.001). While the CHW program focused on eight disease areas, pretesting with the observation tool showed that CHWs were engaged in additional health areas like COVID-19. Of the 3043 health area touches by CHWs observed, COVID-19, tuberculosis, and non-communicable diseases (NCDs) had the highest touches (19.3%, 17.6%, and 16.6%, respectively). The median time spent on sexually transmitted infections (STIs) and NCDs was statistically higher than in other health areas (p < 0.05). Of 3813 tasks completed by CHWs, 1640 (43%) were on health education and promotion. A significant difference was observed in the median time spent on health education, promotion, and screening compared to other tasks (p < 0.05).
Conclusion
This study demonstrates that CHWs spend the most time on health education, promotion, and screening per programmatic objectives but, overall, less time than program design. CHWs deliver care for a broader range of health conditions than the programmatic design indicates. Future studies should examine associations between time spent and quality of care delivery.
Similar content being viewed by others


Introduction
Community health workers (CHWs) play a vital role in the provision of community-based primary health care (PHC), especially in low- and middle-income countries (LMIC) in the journey towards Universal Health Coverage (UHC) [1,2,3]. Many CHWs share similar characteristics, including a community-based work setting, role definition connecting to facility-based primary care, and demographic factors, regardless of geographical location [4]. Generally, CHWs do not have professional training but are locally trained in the context of the specific intervention and primary care system and are chosen from the community they serve [5]. Ample literature demonstrates that CHWs contribute positively to primary health care with improved health outcomes, especially in remote and poor communities [2, 6,7,8,9,10,11,12,13,14,15].
With various needs and contexts worldwide, there are no standardized roles or responsibilities for CHWs [16]. However, despite different scopes and tasks, it is critical that CHWs are strongly supported, trained, and monitored for high-quality care delivery [17]. Several factors have been shown to affect CHW performance, including the number of assigned households and geographic areas, program complexity, training, knowledge and skills [18, 19]. The complexity of tasks and high demand can lead to additional workload and requests for CHW’s services, resulting in poor quality of programmatic outputs [20].
While there is no literature on the scope and workload of specific programs, several studies in sub-Saharan Africa, including Malawi, demonstrate that an increased number of households assigned to the CHW results in underperformance, dissatisfaction, and poor retention [11, 21,22,23,24,25,26,27,28,29]. With the increased workload, studies have shown that CHWs may select tasks that they prefer to do, especially ones they do best and or require less effort [4, 30, 31]. Despite the known challenges intrinsic to the intermediary CHW role in the community, there has been little research into directly observed time measurements and scope of CHW activities compared to programmatic expectations.
Direct observation of health care workers, such as time-motion study (TMS), provides a high level of detail that can effectively be used for programmatic improvement and balancing workload [32]. In TMS, an external observer captures detailed quantitative data on the actions and duration required to accomplish a specific task, coupled with an analysis focused on improving efficiency [33]. Despite the usefulness of programmatic performance, there are few direct time-motion studies focused on measuring CHW activities [33,34,35]. From our literature review, CHW time-motion studies in India, South Africa, and Tanzania has shown that CHWs largely spend time on documentation and travel [2, 34, 35]. To our knowledge, only one study on CHWs' time utilization in Malawi focuses on cervical cancer and family planning [36]. To evaluate CHWs' current contributions to the health care system and identify opportunities for programmatic improvement around efficiency, quality, and effectiveness, we conducted a time-motion study of CHW activities in Neno District, Malawi. We aimed to evaluate how CHWs spend their time on home visits, disease focus areas, and specific tasks for iteration and improvement of CHW program scope, design, and overall primary care delivery.
Methods
Study and CHW program setting
Neno District is a rural and remote district in southwestern Malawi with an estimated population of 153,132 in 2023 [37]. Most people in Neno are subsistence farmers who live on less than 1.90 USD daily and have little access to electricity in the district [38]. Few paved roads connect health facilities in most of the mountainous districts with rugged terrain challenging facility access with substantial interruptions in patients' ability to access and direct care delivery during the rainy season [39]. CHWs are vital for community-based primary care delivery with patient support and linkage to facility-level care.
Partners in Health (PIH), known locally in Malawi as Abwenzi Pa Za Umoyo (APZU), has accompanied the Government of Malawi through the Ministry of Health since 2007 to utilize CHWs in the delivery of rural community-based primary health care in the Neno district [15, 21]. CHWs are assigned to entire households to support the broader health needs of families with eight specific focus areas of high disease burden or need– HIV, tuberculosis (TB), non-communicable diseases (NCDs), sexually transmitted infections, child health, malnutrition, family planning (among women of childbearing age), maternal and neonatal health [15].
Neno District has 1233 CHWs providing care to all households in the district through monthly screening visits and targeted follow-up visits. Each CHW is assigned to between 20 and 40 households depending on the population and geographical region within the district. The CHWs are given a volunteer monthly stipend (38 USD) for time and transport, provided training and ongoing education and support, and service delivery tools such as flip charts. CHWs work within the Ministry of Health’s community health structure and alongside Health Surveillance Assistants (HSAs), community health care workers based at facilities in Malawi [11, 26]. HSAs supervise community activities, village clinics, immunization, and household-level care but are significantly understaffed and overworked within the healthcare system [26]. Thus, the CHWs act as “foot soldiers” for the HSAs within the community at a household level, providing screening, case finding, and follow-up.
Study design and sample size
We conducted a descriptive quantitative time-motion study utilizing a time observation tracker on CHWs in 6 of the 14 catchment areas in Neno District—Midzemba, Lisungwi, Matope, Nsambe, Magaleta, and Neno District Hospital (NDH). We selected these catchment areas due to diverse geography and representative populations. Midzemba, Lisungwi, and Matope are in a geographically flat area on the eastern side of the Neno district with easier terrain and transportation with large semi-urban populations. Conversely, Nsambe, Magaleta, and NDH catchment areas are located in mountainous, remote locations in the western part with rural, more secluded people (Fig. 1).

Map of Neno district showing the distribution of the catchment areas
Sixty-four CHWs were proportionately sampled from each of the six catchment areas using the following formula:
\({n}_{\mathrm{h}}\) is the CHW sample size for catchment area h, \({N}_{\mathrm{h}}\) is the CHW population size for catchment area h, N is the CHW total population size, and n is the total sample size, i.e. 64 CHWs. We further considered the CHW’s gender and distance to the health facility. To have the final CHW to be observed, we obtained the list of their names from the program team and used a random formula in Microsoft Excel to select.
Data collection
We developed a time observation tracker focusing on several critical visits within the CHW program (Additional file 1). At the centre of CHW functions is a monthly household visit where CHW screens all household members within eight health condition focus areas depending on sex and age. Patients with known acute or chronic diseases or those who are pregnant are followed up with additional targeted visits. Through the program’s design, CHWs are expected to spend 45 to 60 min during a monthly household visit and less than 30 min for other visits. This study focused on monthly household visits with the recording of data for different visit types only when a CHW had a follow-up visit during the study observations.
The time observation tracker tool for time-motion study captured CHW’s demographics, including gender, age, education, catchment, the village where the CHW live and work, and the day and date when the observation was done. The time observation tracker captured times for the CHW starting and finishing work at the household, and specific tasks categorized type of visit and disease area of focus. The eight categories of visits were; monthly household visits, daily HIV patient visits, daily TB patient visits, referral follow-up visits, postnatal care (PNC) visits, escorting the patient to/from the facility, time at the health facility with the patient, and other assignments at the facility. The observation tool recorded the start and end times for each CHW task conducted at the household during visits, including check-in, documentation, health talks, screening, psychosocial support, and leading village-level meetings.
For the data collection, we hired four external data collectors without knowledge of the CHW program to limit data collection bias. We trained them for 3 days on the study objectives, the observation time tracker tool, and observation techniques. We pretested the data collection tool on four CHWs selected randomly from the NDH catchment area, with adjustments in the observation tool from these results before data collection. Additional health condition areas of COVID-19/respiratory diseases, malaria, and water sanitation and hygiene (WASH) were added to the observation tool eight disease focus areas based on initial observation pretesting. Each of the four data collectors observed 16 CHWs between 29 June and 20 August 2020. Each CHW was observed at least three times, covering a minimum of three households resulting in over 600 visits during data collection. Data collectors shadowed CHWs for the entire working day and recorded the start and end times of all the visits and tasks performed by recording the disease area covered in each task.
We notified CHWs in advance of data collection that they would be observed. However, they were not informed about the focus of observations or data collection to limit the influence of data collection on their routine work. We obtained consent from each CHW and the head of the household or household representative interacting with the CHW during the visit. We entered data into an Excel database from a paper-based observation tool and performed daily quality checks during data collection.
Data analysis
The excel database was imported to R version 4.0.2 using Rstudio. We used descriptive statistics to characterize the community health worker’s demographic characteristics, tasks completed, and the health areas addressed. We utilized Mood’s median test to compare the median time spent at a household during monthly visits with the program design standard time. With a broad range of other types of visits, we only used data on the monthly household visits for further analysis of health areas and types of tasks. We grouped health conditions to track time into the following categories: (1) HIV, (2) TB, (3) non-communicable disease (NCDs), (4) COVID-19 and other respiratory diseases, (5) maternal and neonatal health, (6) family planning, (7) malnutrition for children under 5 years old, (8) child health for integrated management of childhood illnesses and immunizations, (9) sexually transmitted infections (STIs), (10) malaria and (11) other conditions. Other conditions included water sanitation and hygiene (WASH), malnutrition in persons over five years old, typhoid, and fever. We grouped the tasks completed during the household visit documented above into (i) health education and promotion, (ii) screening, (iii) documentation, (iv) psychosocial support, and (v) logistics. Logistics included patient check-in and check-out, introductions, medication side effect questions, and appointment reminders. We did not record the time it took for CHWs to travel from their house to their households. We used Mood’s median test post hoc test called the “Pairwise median test” to test differences in median time duration for health conditions and assigned tasks by producing box plots. In the boxplot output, the medians followed by a common letter, for example, “a” are not significantly different, and those with unique letters are significantly different from each other by the “pairwise median test” at a 95% confidence level of significance. Additional details regarding our study’s “Pairwise median tests” methods can be found in methodological studies published elsewhere [40,41,42].
Results
Demographics of CHWs
The 64 CHWs observed for this study represented 10.6% of the 601 total CHWs from these six sampled catchment areas. The proportion of CHWs observed from the total number of CHWs in each catchment area ranged from 7.3% to 12.1% (Table 1). Across all catchment areas, the CHW mean age was 37.8 years old, with estimated median households per CHW between 19.7 to 36.0 and 29 (45.3%) of the CHWs had primary-level education. There were slightly more female CHWs than males (65.5% vs. 34.5%), representing the total CHW workforce, where 66.9% are female (Table 1).
CHW visit type and time spent
We observed six hundred and sixty visits from the 64 CHWs, with an average of 10 visits during the study period. Most of the visits were monthly household visits (n = 628, 95.2%), with a median time of 34 min for the monthly household visits (Table 2). Of 628 monthly household visits observed, 147 (23.4%) were from the Neno District Hospital catchment area, with the least number of household visits from the Magareta catchment area (42, 6.7%) (Table 3). There was a considerable time range for monthly household visits, from 6 to 85 min. The median time of all monthly household visits (34.0 min, IQR 21.0) was statistically lower compared to the program estimates of 45–60 min (p < 0.001).
CHW time spent on health condition and task
There were 3043 touches on the tracked health conditions in the 628 observed monthly household visits. The highest number of touches for a health condition was 586 (19.3%) on COVID-19/respiratory disease, followed by 535 (17.6%) touches for TB and 506 (16.6%) for non-communicable diseases (NCDs). The fewest CHW touches were on malnutrition (n = 89, 2.9%) and child health (n = 48, 1.6%). CHWs spent the highest median time on STIs (9 min, IQR 7.0), followed by NCDs (6 min, IQR 9.0) (Table 4).
Despite the greatest number of touches, COVID-19/respiratory diseases only had a median time of 3 min (IQR 5.0). However, the few touches corresponded with short median times of 3 (IQR 3.0) and 2 (IQR 3.0) minutes for child health and malnutrition.
In the pairwise comparison of median time spent on health conditions, we observed a statistically significant difference between the median time observed on STIs and NCDs (each has a unique letter, i.e. “a” and “b” indicating the difference in the median time spent on each condition), and a statistically significant difference between NCDs and the remainder of health conditions (p < 0.05) (Fig. 2). We observed no statistically significant difference between the median time spent on tuberculosis and maternal and neonatal health (shares a joint letter “c”). Similarly, no statistically significant differences were observed between the median time spent on malaria, HIV, child health and COVID-19 and respiratory diseases (shares two joint letters “cd”).

Comparison of median time spent per health condition during monthly CHW visit
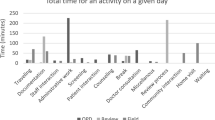
During the study period, CHW completed 3813 tasks in their monthly visits. Health education and promotion accounted for over 40% of all CHW tasks, with the longest median time of 6 min (IQR 8.0) (Table 5). Despite a high proportion of contacts with logistics, CHWs spent the shortest median time on this task at 1.0 min (IQR 1.0). Documentation and psychosocial support combined for 13% of all the tasks with the lowest median times at 2.0 min (IQR 3.0 and 2.0, respectively) (Table 5).
In comparing the median time spent per task during the CHW monthly home visits, there was a significant difference between health education and promotion and screening (each has a unique letter, i.e. “a” and “b”) with a higher median time compared to the time spent on other tasks (p < 0.05) (Fig. 3). We observed no significant difference between the median time spent on documentation and psychosocial support (shares a joint letter “c”) and similarly between psychosocial support and logistics (shares a joint letter “d”).

Comparison of median time spent per task during the monthly CHW visit
Discussion
To our knowledge, only one study has reported on CHWs’ time utilization using direct time-motion observation in Malawi, focusing on cervical cancer and family planning [36]. However, our study focused on household visits and time taken for specific tasks among diverse multiple health areas. We found that CHWs in the Neno district spend significantly less time on monthly household visits than expected through program design, with a median time of 34 min. Despite our study showing that CHWs spend less time on monthly household visits than the expected 60 min from program design, prior studies done in Neno have shown that CHWs provide high-quality, patient-centred care with improved health outcomes in the community associated with CHWs work [15, 43,44,45,46,47].
We found that CHWs were spending > 50% of their time on disease screening and providing health education and promotion within the monthly household visit—a core design of the CHW program in Neno District [15]. Similar findings have been reported in India and South Africa where on average, CHWs spend 30 min on similar health education activities, nutrition screening, family planning, and immunizations [48, 49] as their core activities. However, a study done in Burkina Faso, Nigeria and Uganda found that CHWs spend longer visit times between 56 and 77 min on activities of testing and treatment components [50], which makes sense for the type of activities.
In our study, four out of six catchment areas have greater than 33 households assigned to each CHW despite this being within the expected number of households in the Neno district. While it is true that not all catchment areas with higher numbers of households demonstrated reduced median time spent on monthly visits in our study, it is important to consider that CHWs assigned to such areas may experience an increased workload and with less available time to spend on each individual household as shown in other studies [26, 51]. Further studies of our CHW program and others are required to further understand the ideal amount of time for high-quality care depending on visit type and expected tasks.
During monthly household visits, however, we found few CHW touches for STIs with significantly higher median times than all other health areas. This finding may be partly due to this study’s small number of observations. Still, it could also be partly due to the stigma and discomfort present with sexual-related health conditions in many communities with potentially a lack of health knowledge in the community [52]. Following STIs, the median time spent on NCDs was statistically higher than the remainder of all other health areas. With a correspondingly high proportion of touches, this finding is likely due to the growing burden of NCDs encompassing a complex, diverse set of health conditions in Malawi [53]. There is extensive literature on how CHWs have improved outcomes for NCD patients from the follow-up for missed facility visits to treatment outcomes [15, 54,55,56]. However, further studies are required to estimate how much time would be required for optimal disease screening, including NCDs, and ascertain the quality of the screening to pick up the disease.
Following STIs and NCDs, TB and COVID-19/respiratory disease had frequent touches by CHWs. This finding is likely due to the COVID-19 pandemic during the study period. In Neno, at the onset of COVID-19, CHWs were trained on preventive measures and COVID-19 education provision to their communities. Similar approaches have been reported by other LMICs as part of the COVID-19 response [57, 58]. While CHWs could play an important role in the fight against emerging diseases like COVID-19, there need to balance their workload, studies have shown that increasing the workload leads to burnout and poor performance [11, 18,19,20].
Another critical function of CHWs is to provide psychosocial support and more needed, especially in light of the COVID-19 pandemic-induced stress and anxiety [59,60,61,62,63]. However, we found that CHWs only spent a median of 2 min in each household, considered less than necessary to support individuals. In addition to eight health condition focus areas and COVID-19, CHW also focused on malaria and other conditions, including water sanitation and hygiene. This is unsurprising as the district is in southern Malawi, a region with a higher prevalence of Malaria (averaging 26% annually) [64]. Neno also has frequent typhoid and diarrheal disease outbreaks [65, 66]. This finding supports that these health areas are of concern within the community and should be given consideration for additions to the program through training and education tools.
On child health and malnutrition, we found that CHWs spent only a median of 3 and 2 min, respectively, with few touches for both health areas. This finding could be explained in part due to a “no-touch” policy introduced for COVID-19 infection control with a lack of personal protective equipment (PPE) for CHWs in Malawi. Similar “no-touch” policies were implemented for CHW programs during the Ebola outbreak in Guinea, Liberia and Sierra Leone, indicating the adoption of a syndromic surveillance approach [67, 68]. Thus, mid-upper arm circumference (MUAC) for malnutrition screening was replaced with the visual screening of the child’s weight, wasting, hair colour and texture [69]. These findings suggest that through community and health workforce engagement with active participation in shaping CHW tasks and focus areas, additional screening processes for all health areas with special attention to childhood malnutrition and child health should be adapted within the CHW program with the ongoing pandemic and future infectious disease outbreaks.
While CHWs appropriately only spend a short time (median of 1 min) on logistics such as appointment reminders, these reminders are crucial to the patients and improve health outcomes [70]. A systematic review of 25 studies found that informative appointment reminders through phone calls or text messages, or actual household visits improve facility attendance twofold [39]. In Neno District, we have observed the same with programmatic retentions of patients in care at 85% for HIV and 72% for NCDs driven primarily by CHW follow-up and appointment reminders [45, 46]. Further investigation of CHW patient support functions is needed to ensure that CHWs properly provide psychosocial care, education, and reminders to their households for facility follow-up.
The results of this study can help inform community health policy and human resource decision-making in Malawi. The National Community Health Strategy recommends one Health Surveillance Assistant (HSA) for every 1000 people to provide integrated care delivery of primary care at the catchment facility level [71]. It recommends that Community Health Volunteers (CHVs), aligned to the level and scope of the community health workers in this study, support the HSAs in service delivery but still needs to define the number of CHWs and scope of work. This study can provide essential information on the potential scope of work for CHVs and estimates of the time required for specific tasks and numbers of CHVs required at the household level to inform upcoming Community Health guidelines and policy. Further work in measuring an association between the amount of time and service done with further studies to compare time spent on tasks to service quality, such as individual patient follow-up is required to optimize community-based primary care delivery.
Limitations
Our study has several limitations including limited generalizability with data from one rural district population in Malawi. However, we have cited numerous CHW programs in similar contexts and program designs worldwide in this study [2, 12, 30, 31, 34,35,36, 49, 56, 68] who could benefit from these findings on CHW time, health focus areas and time for specific tasks. Secondly, our sample size was small, which could influence our findings. However, we tried to minimize the effect of our CHW-limited sample size by a comprehensive approach to probabilistic selection criteria. This included considering geographic terrain, sex distribution of the CHW, and the CHW population within a specific catchment area relative to our sample; for example, the Magaleta catchment area has a smaller number of CHWs and finally, using a random function in Excel to generate the final list. We recommend conducting further studies that encompass a larger sample size of CHWs and are observed for more than two months with intervals within the year to compare potential seasonality or calendar changes in visits. Finally, with study observations during the onset of the COVID-19 pandemic, the CHW time spent in the household may have been affected due to fears of transmission and programmatic changes without the necessary PPE with adjustments in screening and time spent on specific health areas. However, these findings also provide valuable information on how CHW programs should adjust for incorporating COVID-19 and emerging outbreaks into essential health care.
Conclusion
This study is the first time-motion study conducted in Malawi on CHW time utilization linked to specific health areas and tasks in service delivery. We found that CHW allocates the most time to health education, promotion, and screening activities, aligning with programmatic objectives. However, the overall time CHWs spend is less than what was initially planned or designed for the program.
The findings provide valuable insights for CHW program redesign and improvement. They highlight areas where adjustments in time allocation could enhance program effectiveness. The next steps include further investigation into the time spent on a visit, task or health area in connection to the quality of care provided with a direct linkage to CHW numbers and scope for optimized service delivery.
Availability of data and materials
The datasets generated and/or analysed during the current study are available in the Zenodo repository, https://doi.org/10.5281/zenodo.6778792.
Abbreviations
- CHWs:
-
Community health workers
- PIH:
-
Partners In Health
- APZU:
-
Abwenzi Pa Za Umoyo
- TB:
-
Tuberculosis
- NCDs:
-
Non-communicable diseases
- S.T.I.s:
-
Sexually transmitted infections
- HIV:
-
Human immunodeficiency virus
- ART:
-
Antiretroviral therapy
- H.S.A.:
-
Health Surveillance Assistant
- PHC:
-
Primary Health Care
- LMIC:
-
Lower and middle income countries
- TMS:
-
Time-motion study
- PNC:
-
Postnatal care
- IQR:
-
Inter-quartile range
- NHSRC:
-
National Health Science Research Committee
References
Jaskiewicz W, Tulenko K. Increasing community health worker productivity and effectiveness: a review of the influence of the work environment. Hum Resour Health. 2012;10:38.
Odendaal WA, Lewin S. The provision of TB and HIV/AIDS treatment support by lay health workers in South Africa: a time-and-motion study. Hum Resour Health. 2014;12:18.
Perry HB, Zulliger R, Rogers MM. Community health workers in low-, middle-, and high-income countries: an overview of their history, recent evolution, and current effectiveness. Annu Rev Public Health. 2014;35:399–421.
Ingram M, Reinschmidt KM, Schächter KA, Davidson CL, Sabo SJ, De Zapien JG, et al. Establishing a professional profile of Community Health Workers: results from a national study of roles, activities and training. J Community Health. 2012;37:529–37.
LeBan K, Kok M, Perry HB. Community health workers at the dawn of a new era: 9. CHWs’ relationships with the health system and communities. Health Res Policy Syst. 2021;19:116.
Jerome J, Ivers L. Community health workers in health systems strengthening: a qualitative evaluation from rural Haiti. AIDS Lond Engl. 2010;24:S67-72.
Johnson AD, Thiero O, Whidden C, Poudiougou B, Diakité D, Traoré F, et al. Proactive community case management and child survival in periurban Mali. BMJ Glob Health. 2018;3: e000634.
Kim MH, Ahmed S, Buck WC, Preidis GA, Hosseinipour MC, Bhalakia A, et al. The Tingathe programme: a pilot intervention using community health workers to create a continuum of care in the prevention of mother to child transmission of HIV (PMTCT) cascade of services in Malawi. J Int AIDS Soc. 2012;15:17389.
McBain RK, Petersen E, Tophof N, Dunbar EL, Kalanga N, Nazimera L, et al. Impact and economic evaluation of a novel HIV service delivery model in rural Malawi. AIDS. 2017;31:1999–2006.
Muremyi R. Contribution of community health workers in the prevention of disease caused by malnutrition in Rwanda [Internet]. 2022 [cited 2022 Mar 16]. Available from: https://www.researchsquare.com/article/rs-41252/v1.
Ndambo MK, Munyaneza F, Aron MB, Nhlema B, Connolly E. Qualitative assessment of community health workers’ perspective on their motivation in community-based primary health care in rural Malawi. BMC Health Serv Res. 2022;22:179.
Olaniran A, Madaj B, Bar-Zev S, van den Broek N. The roles of community health workers who provide maternal and newborn health services: case studies from Africa and Asia. BMJ Glob Health. 2019;4: e001388.
Palazuelos D, Farmer PE, Mukherjee J. Community health and equity of outcomes: the Partners In Health experience. Lancet Glob Health. 2018;6:e491–3.
Schurer JM, Fowler K, Rafferty E, Masimbi O, Muhire J, Rozanski O, et al. Equity for health delivery: Opportunity costs and benefits among Community Health Workers in Rwanda. PLoS ONE. 2020;15: e0236255.
Wroe EB, Nhlema B, Dunbar EL, Kulinkina AV, Kachimanga C, Aron M, et al. A household-based community health worker programme for non-communicable disease, malnutrition, tuberculosis, HIV and maternal health: a stepped-wedge cluster randomised controlled trial in Neno District, Malawi. BMJ Glob Health. 2021;6: e006535.
Hartzler AL, Tuzzio L, Hsu C, Wagner EH. Roles and functions of community health workers in primary care. Ann Fam Med. 2018;16:240.
World Health Organisation. Community health workers: a strategy to ensure access to primary health care services [Internet]. 2016 p. 37. Available from: https://apps.who.int/iris/bitstream/handle/10665/249563/EMROPUB_2016_EN_1760.pdf?.
Oliver M, Geniets A, Winters N, Rega I, Mbae SM. What do community health workers have to say about their work, and how can this inform improved programme design? A case study with CHWs within Kenya. Glob Health Action. 2015;8: 27168.
Sharma R, Webster P, Bhattacharyya S. Factors affecting the performance of community health workers in India: a multi-stakeholder perspective. Glob Health Action. 2014;7:25352.
Callaghan-Koru JA, Hyder AA, George A, Gilroy KE, Nsona H, Mtimuni A, et al. Health workers’ and managers’ perceptions of the integrated community case management program for childhood illness in Malawi: the importance of expanding access to child health services. Am J Trop Med Hyg. 2012;87:61.
Dunbar EL, Wroe EB, Nhlema B, Kachimanga C, Gupta R, Taylor C, et al. Evaluating the impact of a community health worker programme on non-communicable disease, malnutrition, tuberculosis, family planning and antenatal care in Neno, Malawi: protocol for a stepped-wedge, cluster randomised controlled trial. BMJ Open. 2018;8: e019473.
Goudge J, de Kadt J, Babalola O, Muteba M, Tseng Y, Malatji H, et al. Household coverage, quality and costs of care provided by community health worker teams and the determining factors: findings from a mixed methods study in South Africa. BMJ Open. 2020;10: e035578.
Hayhoe B, Cowling TE, Pillutla V, Garg P, Majeed A, Harris M. Integrating a nationally scaled workforce of community health workers in primary care: a modelling study. J R Soc Med. 2018;111:453–61.
Johnson LJ, Schopp LH, Waggie F, Frantz JM. Challenges experienced by community health workers and their motivation to attend a self-management programme. Afr J Prim Health Care Fam Med. 2022;14:2911.
Kok MC, Broerse JEW, Theobald S, Ormel H, Dieleman M, Taegtmeyer M. Performance of community health workers: situating their intermediary position within complex adaptive health systems. Hum Resour Health. 2017;15:59.
Kok MC, Muula AS. Motivation and job satisfaction of Health Surveillance Assistants in Mwanza, Malawi: an explorative study. Malawi Med J. 2013;25:5.
Musoke D, Nyashanu M, Bugembe H, Lubega GB, O’Donovan J, Halage AA, et al. Contested notions of challenges affecting Community Health Workers in low- and middle-income countries informed by the Silences Framework. Hum Resour Health. 2022;20:4.
Smith S, Deveridge A, Berman J, Negin J, Mwambene N, Chingaipe E, et al. Task-shifting and prioritization: a situational analysis examining the role and experiences of community health workers in Malawi. Hum Resour Health. 2014;12:24.
Suri A, Gan K, Carpenter S. Voices from the field: perspectives from community health workers on health care delivery in Rural KwaZulu-Natal, South Africa. J Infect Dis. 2007;196:S505–11.
Baatiema L, Sumah AM, Tang PN, Ganle JK. Community health workers in Ghana: the need for greater policy attention. BMJ Glob Health. 2016;1: e000141.
Hermann K, Van Damme W, Pariyo GW, Schouten E, Assefa Y, Cirera A, et al. Community health workers for ART in sub-Saharan Africa: learning from experience—capitalizing on new opportunities. Hum Resour Health. 2009;7:31.
Kalne PS, Mehendale AM. The purpose of time-motion studies (TMSs) in healthcare: a literature review. Cureus. 2022;14:e29869.
Lopetegui M, Yen P-Y, Lai A, Jeffries J, Embi P, Payne P. Time motion studies in healthcare: what are we talking about? J Biomed Inform. 2014;49:292–9.
Chebolu-Subramanian V, Sule N, Sharma R, Mistry N. A time motion study of community mental health workers in rural India. BMC Health Serv Res. 2019;19:878.
Tani K, Stone A, Exavery A, Njozi M, Baynes CD, Phillips JF, et al. A time-use study of community health worker service activities in three rural districts of Tanzania (Rufiji, Ulanga and Kilombero). BMC Health Serv Res. 2016;16:461.
Chinkhumba J, Low D, Ziphondo E, Msowoya L, Rao D, Smith JS, et al. Assessing community health workers’ time allocation for a cervical cancer screening and treatment intervention in Malawi: a time and motion study. BMC Health Serv Res. 2022;22:1196.
NSO. Malawi National and District Population Projections 2018–2050. Zomba, Malawi: National Statistical Office; 2020; p. 1–276.
National Statistical office. Malawi Demographic and Health Survey 2015–16 [Internet]. 2017 Feb. Available from: https://dhsprogram.com/publications/publication-fr319-dhs-final-reports.cfm.
Government of Malawi. Neno District Council Socio-economic profile 2017 - 2022 [Internet]. 2020. Report No.: September 2020. Available from: https://integrationpoint.mw/wp-content/uploads/2020/12/Neno-District-Council-Socio-Economic-Profile-2017-2022.pdf.
Mangiafico SS. Summary and Analysis of Extension Program Evaluation in R [Internet]. New Brunswick, NJ: Rutgers Cooperative Extension; 2016 [cited 2023 May 16]. Available from: https://rcompanion.org/documents/RHandbookProgramEvaluation.pdf.
Saville DJ. Multiple comparison procedures—cutting the Gordian Knot. Agron J. 2015;107:730–5.
Piepho H-P. Letters in mean comparisons: what they do and don’t mean. Agron J. 2018;110:431–4.
Kachimanga C, Dunbar EL, Watson S, Cundale K, Makungwa H, Wroe EB, et al. Increasing utilisation of perinatal services: estimating the impact of community health worker program in Neno, Malawi. BMC Pregnancy Childbirth. 2020;20:22.
Wroe EB, Kalanga N, Mailosi B, Mwalwanda S, Kachimanga C, Nyangulu K, et al. Leveraging HIV platforms to work toward comprehensive primary care in rural Malawi: the Integrated Chronic Care Clinic. Healthcare. 2015;3:270–6.
Wroe EB, Kalanga N, Dunbar EL, Nazimera L, Price NF, Shah A, et al. Expanding access to non-communicable disease care in rural Malawi: outcomes from a retrospective cohort in an integrated NCD–HIV model. BMJ Open. 2020;10: e036836.
Wroe EB, Mailosi B, Price N, Kachimanga C, Shah A, Kalanga N, et al. Economic evaluation of integrated services for non-communicable diseases and HIV: costs and client outcomes in rural Malawi. BMJ Open. 2022;12: e063701.
Wroe EB, Dunbar EL, Kalanga N, Dullie L, Kachimanga C, Mganga A, et al. Delivering comprehensive HIV services across the HIV care continuum: a comparative analysis of survival and progress towards 90-90-90 in rural Malawi. BMJ Glob Health. 2018;3:e000552–e000552.
Besada D, Eagar D, Rensburg R, Shabangu G, Hlahane S, Daviaud E. Resource requirements for community-based care in rural, deep-rural and peri-urban communities in South Africa: a comparative analysis in 2 South African provinces. PLoS ONE. 2020;15: e0218682.
Jain A, Walker DM, Avula R, Diamond-Smith N, Gopalakrishnan L, Menon P, et al. Anganwadi worker time use in Madhya Pradesh, India: a cross-sectional study. BMC Health Serv Res. 2020;20:1130.
Castellani J, Mihaylova B, Ajayi IO, Siribié M, Nsungwa-Sabiiti J, Afonne C, et al. Quantifying and valuing community health worker time in improving access to malaria diagnosis and treatment. Clin Infect Dis. 2016;63:S298-305.
Kambarami RA, Mbuya MN, Pelletier D, Fundira D, Tavengwa NV, Stoltzfus RJ. Factors Associated With Community Health Worker Performance Differ by Task in a Multi-Tasked Setting in Rural Zimbabwe. Glob Health Sci Pract. 2016;4:238–50.
National Academies of Sciences E, Division H and M, Practice B on PH and PH, States C on P and C of STI in the U, Crowley JS, Geller AB, et al. Supporting and expanding the future STI workforce. Sex Transm Infect Adopt Sex. Health Paradigm. National Academies Press (US); 2021 [cited 2022 May 26]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK573165/.
Ministry of Health and Population. Malawi National stepwise survey for Non- Communicable Diseases risk factors 2017 report [Internet]. Lilongwe; 2017. Available from: https://extranet.who.int/ncdsmicrodata/index.php/catalog/629/study-description.
Rachlis B, Naanyu V, Wachira J, Genberg B, Koech B, Kamene R, et al. Community perceptions of community health workers (CHWs) and their roles in management for HIV, tuberculosis and hypertension in western Kenya. PLoS ONE. 2016;11: e0149412.
Long H, Huang W, Zheng P, Li J, Tao S, Tang S, et al. Barriers and facilitators of engaging community health workers in non-communicable disease (NCD) prevention and control in China: a systematic review (2006–2016). Int J Environ Res Public Health. 2018;15:2378.
Jeet G, Thakur JS, Prinja S, Singh M. Community health workers for non-communicable diseases prevention and control in developing countries: evidence and implications. PLoS ONE. 2017;12: e0180640.
Feroz AS, Khoja A, Saleem S. Equipping community health workers with digital tools for pandemic response in LMICs. Arch Public Health. 2021;79:1.
Rahman R, Ross A, Pinto R. The critical importance of community health workers as first responders to COVID-19 in USA. Health Promot Int. 2021;36:1498–507.
Han H-R, Kim K, Murphy J, Cudjoe J, Wilson P, Sharps P, et al. Community health worker interventions to promote psychosocial outcomes among people living with HIV—a systematic review. PLoS ONE. 2018;13: e0194928.
Mistry SK, Harris-Roxas B, Yadav UN, Shabnam S, Rawal LB, Harris MF. Community health workers can provide psychosocial support to the people during COVID-19 and beyond in low- and middle- income countries. Front Public Health. 2021;9: 666753.
Peretz PJ, Islam N, Matiz LA. Community health workers and Covid-19—addressing social determinants of health in times of crisis and beyond. N Engl J Med. 2020;383: e108.
Rahman MS, Rahman MA, Afroze L, Islam SMS. Unmet needs for mental care services for older people in Bangladesh during the COVID-19 pandemic. Gen Psychiatry. 2020;33: e100294.
Vanden Bossche D, Lagaert S, Willems S, Decat P. Community health workers as a strategy to tackle psychosocial suffering due to physical distancing: a randomized controlled trial. Int J Environ Res Public Health. 2021;18:3097.
National Malaria Control Programme (NMCP) and ICF. Malawi Malaria Indicator Survey 2017 [Internet]. Lilongwe, Malawi, and Rockville, Maryland, USA: NMCP and ICF; 2018 p. 145. Available from: https://dhsprogram.com/pubs/pdf/MIS28/MIS28.pdf.
Bennett SD, Lowther SA, Chingoli F, Chilima B, Kabuluzi S, Ayers TL, et al. Assessment of water, sanitation and hygiene interventions in response to an outbreak of typhoid fever in Neno District, Malawi. PLoS ONE. 2018;13:1–13.
Dupas P, Nhlema B, Wagner Z, Wolf A, Wroe E. Expanding access to clean water for the rural poor: experimental evidence from Malawi. Cambridge: National Bureau of Economic Research; 2020.
Siekmans K, Sohani S, Boima T, Koffa F, Basil L, Laaziz S. Community-based health care is an essential component of a resilient health system: evidence from Ebola outbreak in Liberia. BMC Public Health. 2017;17:84.
Miller NP, Milsom P, Johnson G, Bedford J, Kapeu AS, Diallo AO, et al. Community health workers during the Ebola outbreak in Guinea, Liberia, and Sierra Leone. J Glob Health. 2018;8: 020601.
Cumber SN, Ankraleh NB, Monju N. Mothers’ knowledge on the effects of malnutrition in children 0–5 years in Muea Health Area Cameroon. J Fam Med Health Care. 2016;2:36.
Anglada-Martinez H, Riu-Viladoms G, Martin-Conde M, Rovira-Illamola M, Sotoca-Momblona JM, Codina-Jane C. Does mHealth increase adherence to medication? Results of a systematic review. Int J Clin Pract. 2015;69:9–32.
Ministry of Health. Malawi National Community Health Strategy 2017 - 2022 [Internet]. Lilongwe, Malawi; 2017 Jul. Available from: https://www.healthynewbornnetwork.org/resource/malawi-national-community-health-strategy-2017-2022/.
Acknowledgements
We are grateful to the CHWs, SCHWs, Healthcare workers, patients, and community members who participated in the study. We acknowledge the Samuel Family Foundation for the financial support and the APZU community health, clinical, monitoring and evaluation, and operations departments for the collaborations. We recognize the District Health Management Team and health care workers of the Neno District for the work they do for patients and the support given to the CHWs. We appreciate the help rendered by the following research assistants: Edwin Kambanga, Beatrice Kasanda, Sakina Phiri, and Khumbata Gondwe.
Funding
This study was supported by the Samuel Family Foundation, Canada (PIHC project MA.LI.CHW.17). The funding body had no role in the study's design, data collection, analysis, interpretation of data, or manuscript write-up.
Author information
Authors and Affiliations
Contributions
MKN, BN, FM, and EC conceptualized and designed the study. MKN facilitated data collection. MBA and MM analysed data. MKN and MBA drafted the manuscript with assistance from BN and EC. All authors reviewed the manuscript, provided input, and suggested additions and changes. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the National Health Science Research Committee (NHSRC) in Malawi with protocol number 1059, titled "Lessons Learned from Monitoring and Evaluation of Community Health Initiatives in Neno District, Malawi." Before data collection, research assistants obtained written informed consent from CHWs and household participants. Upon obtaining verbal and written consent, the CHW introduced the observer to the household members and made it clear that the observer was there to observe the CHW without recording details of the individual. In case of confidentiality issues, the CHW could ask the observer to step away from a conversation and then join at the end to record time for the remainder of the visit. Households with no household head at the time of the study were not observed.
Consent for publication
Not applicable.
Competing interests
All authors are employees of Partners In Health/Abwenzi Pa Za Umoyo. The authors declare no additional competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
CHW Data collection observation tool.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Aron, M.B., Ndambo, M.K., Munyaneza, F. et al. A time-motion study of community health workers delivering community-based primary health care in Neno District, Malawi. Hum Resour Health 21, 51 (2023). https://doi.org/10.1186/s12960-023-00839-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12960-023-00839-z