
Abstract
Background
Increasing number of studies have demonstrated certain patterns of microbial changes in gynecological diseases; however, the interaction between them remains unclear. To evaluate the consistency or specificity across multiple studies on different gynecological diseases and microbial alterations at different sites of the body (gut and genital tract), we conducted a systematic review and meta-analysis.
Methods
We searched PubMed, Embase, Web of Science, and Cochrane Library up to December 5, 2022(PROSPERO: CRD42023400205). Eligible studies focused on gynecological diseases in adult women, applied next-generation sequencing on microbiome, and reported outcomes including alpha or beta diversity or relative abundance. The random-effects model on standardized mean difference (SMD) was conducted using the inverse-variance method for alpha diversity indices.
Results
Of 3327 unique articles, 87 eligible studies were included. Significant decreases were found in gut microbiome of patients versus controls (observed species SMD=-0.35; 95%CI, -0.62 to -0.09; Shannon index SMD=-0.23; 95%CI, -0.40 to -0.06), whereas significant increases were observed in vaginal microbiome (Chao1 SMD = 1.15; 95%CI, 0.74 to 1.56; Shannon index SMD = 0.51; 95%CI, 0.16 to 0.86). Most studies of different diagnostic categories showed no significant differences in beta diversity. Disease specificity was observed, but almost all the changes were only replicated in three studies, except for the increased Aerococcus in bacterial vaginosis (BV). Patients with major gynecological diseases shared the enrichment of Prevotella and depletion of Lactobacillus, and an overlap in microbes was implied between BV, cervical intraepithelial neoplasia, and cervical cancer.
Conclusions
These findings demonstrated an association between alterations in gut and genital microbiota and gynecological diseases. The most observed results were shared alterations across diseases rather than disease-specific alterations. Therefore, further investigation is required to identify specific biomarkers for diagnosis and treatment in the future.
Similar content being viewed by others


Introduction
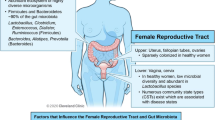
Gut microbiome, the “second genome” of human body, is the most abundant microbiome in the human body and most studied human microbiome that relates to obesity, inflammation, metabolism, cancer and so on [1,2,3,4]. Microbiota in the genital tract are mainly found in the lower genital tract (vagina, cervix) which has long been considered sterile [5]. Thanks to the rapid advancements of next-generation sequencing (NGS) technologies and bioinformatics, the understanding of microbiome colonized in various parts of human body is gradually improved, with more and more relative studies being carried out. Based on a recent study, the upper genital tract, including the uterus, fallopian tubes, and peritoneal fluid, harbors diverse communities of bacteria despite their low abundance [6]. However, very few studies could be retrieved due to the difficulty of invasive sampling of the upper reproductive tract.
Major gynecological diseases include bacterial vaginosis (BV), aerobic vaginitis (AE), vulvovaginal candidiasis (VVC), human papillomavirus infection (HPV), polycystic ovary syndrome (PCOS), endometriosis (EM), adenomyosis (AM), cervical intraepithelial neoplasia (CIN), cervical cancer (CCA), endometrial cancer (EC), uterine fibroids (UF) and ovarian cancer (OC) [7,8,9,10]. Systematic reviews in individual gynecological diseases have identified certain patterns of microbial changes. Women with EM had higher levels of Proteobacteria, Enterobacteriaceae, Streptococcus and E. coli. [11] More remarkably, patients with endometriosis have been found to have an increased Firmicutes to Bacteroidetes ratio, similar to irritable bowel syndrome [12]. Patients with PCOS had an increase in Lactobacillus, Escherichia/Shigella and Bacteroides, and a decrease in biodiversity in the gut microbiome [13]. L. iners was associated with higher HPV prevalence compared to L. crispatus, a protective factor in the progression from CIN to CCA [14, 15]. Another study demonstrated the protective effect of each Lactobacillus species against vaginal dysbiosis, as well as a strong probiotic multi-microbial consortium by L. iners, L. jensenii, L. gasseri, and L. acidophilus against AV and BV [16]. However, the specificity and reproducibility of the microbial changes among different diseases require further exploration because of the inconsistent results from the individual studies. Consequently, it is crucial to characterize the microbial diversity and composition across a broader range of gynecological diseases.
Our aim was to discover the bidirectional interaction between gynecological diseases and microbial alterations at different sites of the body (gut and genital tract) and to evaluate the consistency or specificity across multiple studies focused on gynecological diseases in adult women, which in turn may provide potential biomarkers. Therefore, in the present, we conducted a systematic review and meta-analysis of studies that characterized the composition of the microbiota between women with and without gynecological diseases. In addition to the studies on the intestinal tract, those on the genital tract were also included.
Methods
The protocol of study was preregistered with PROSPERO (CRD42023400205). We also followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline [17].
Search strategy and information sources
The search was conducted using PubMed, Embase, Web of Science, and Cochrane Library and was last updated on December 5, 2022. The search strings have been presented in Appendix S1. Included studies were limited to those including human studies and were published in English since 2005. The reference lists of relevant reviews were also manually examined to identify additional eligible studies missed by the initial search.
Eligibility criteria and study selection
Studies were eligible if they [1] focused on major gynecological diseases in adult women as previous described in introduction, [2] applied next-generation sequencing on the microbiome from the intestinal tract, genital tract, peritoneal fluid, or biopsy sample, and [3] reported outcomes including alpha or beta diversity or relative abundance. Interventional studies and studies without control groups were excluded. Two reviewers independently screened titles and abstracts. A full-text assessment was then performed by them. Discrepancies were resolved by discussion with a third author or among all reviewers.
Data extraction and assessment of risk of bias
A pilot-tested form was used to extract data from eligible studies. For each study, the following information was extracted: first author’s name, year of publication, country, number of patients and controls, age and Body Mass Index (BMI) of participants, sampling type, sequencing platform, and database. As for primary outcomes, we extracted the alpha and beta diversity of microbial communities, as well as the relative abundance of taxonomic findings at the phylum, family, and genus levels.
The quality of included studies was examined independently by two reviewers using the Newcastle–Ottawa Scale (NOS) for case–control studies [18]. The NOS is based on three dimensions: selection, comparability, and outcome. A total NOS score of ≤ 5 was considered low-quality.
Data synthesis
For studies that did not provide original data but box plots of alpha diversity indices, we used WebPlotDigitizer version 4.6 to extract the data from the figures according to previously published methods [19]. The sample mean and standard deviation were estimated using a web-based tool (https://www.math.hkbu.edu.hk/~tongt/papers/median2mean.html) with the sample size, median, range, and interquartile range [20]. If the data were significantly skewed, an alternative validated procedure was followed [21]. In consideration of the high likelihood of between-study differences, the random-effects model on standardized mean difference (SMD) was conducted using the inverse-variance method and were visualized by means of forest plots. Tests for heterogeneity were reported using the I2 statistic, which was categorized as low (25-50%), moderate (51-75%), or high (> 75%). Publication bias was examined with funnel plots. Preplanned subgroup analyses were performed by specific type of gynecological disease. In addition, further subgroup analyses were performed by country and body weight of participants in studies on PCOS, as there are sufficient studies for such a classification. All statistical analyses were conducted in Review Manager version 5.4 for Windows (Cochrane Collaboration).
Results
Study selection
A total of 3327 articles were identified through the preliminary search. After removing duplicates, 1876 articles were screened based on the titles and abstracts. A total of 177 full-text articles were retrieved for a detailed eligibility evaluation, 90 of which were excluded. As a result, 87 studies across nine diseases were included in our meta-analysis (Fig. 1). The number of studies included for each disease was 13 for BV, 13 for EM, one for AM, 26 for PCOS, 10 for CIN, 14 for CCA, four for OC, five for EC, and one for UF.

PRISMA flowchart showing the study selection process
Study characteristics and methodologies
Table S1 describes the characteristics of the included studies. In total, 7726 participants were included, and the sample sizes of the included studies ranged from 13 to 439. Most studies (n = 58) were conducted in East Asia (45 in China), 12 in Europe, 14 in North and South America, one in Africa, and two in multiple countries.
The methodology of composition analysis and sequencing details were various, with 16 S rRNA sequencing being most common (Table S2). We also noted heterogeneity regarding the amplified region of the 16 S rDNA, with the most widely used being V3-V4 (n = 37 studies), and V4 (n = 20). Most of these sequencing analyses were conducted on the Illumina MiSeq, Illumina HiSeq, Ion PGM, and 454 GS platforms. The remaining three studies used shotgun metagenomics and created metagenome libraries. The most widely used databases were the Greengenes database and Ribosomal Database Project (RDP) Classifier. Besides, most studies (76/87) were matched by age, some of which also carried out subgroup analyses stratified by BMI, stage of disease, HPV status, smoking, or other disease-related factors.
Risk of bias of included studies
As shown in Table S3, all of the included studies were assessed using the Newcastle-Ottawa Scale (NOS) and received a moderate score ranging from 6 to 8 (mean = 7.10). None of the included studies scored in the non-response rate category, which is not applicable to these study methodologies. No study was excluded because of the risk of bias (Table S3).
Alpha diversity
79 of the 87 studies assessed the alpha diversity of the microbial communities, among which 64 provided statistical charts or accurate data between the patients and controls. Within each sample type, indices with sufficient studies (n > 5) were included in the meta-analysis. The most widely used indices were the Shannon index, Chao1, observed species, and Simpson index. Visual inspection revealed no evidence of publication bias in any of the funnel plots (Figure S1).
Regarding the richness of the gut microbiome, 13 studies reported observed species in patients (n = 366) and controls (n = 283) [22,23,24,25,26,27,28,29,30,31,32,33,34]. A significant decrease in patients (standardized mean difference [SMD]=-0.35, [95%CI: -0.62, -0.09], I2 = 58%) was observed when pooling the data during the meta-analysis (Fig. 2A). Within individual diagnoses, there was a significant decrease in PCOS. Twelve studies reported Chao1 in patients (n = 413) and controls (n = 331), with no statistically significant change in the pooled estimate (SMD=-0.21, [95%CI: -0.53, 0.10], I2 = 74%) (Fig. 2B) [24,25,26,27, 30, 32,33,34,35,36,37,38].

Forest Plots of Alpha Diversity in the Gut Microbiota of Patients with Gynecological Diseases Compared with Healthy Controls. (A) Observed species. (B) Chao1. (C) Shannon index. (D)Simpson index
Regarding the diversity of the gut microbiome, 24 studies reported the Shannon index in patients (n = 929) and controls (n = 1042) [22, 25, 26, 28, 29, 31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49]. There was a significant decrease in patients (SMD=-0.23, [95%CI: -0.40, -0.06], I2 = 66%) (Fig. 2C). Considering individual diagnoses, there was a significant decrease only in EM and PCOS. Six studies reported Simpson in patients (n = 156) and controls (n = 118), and no significant difference between groups was observed (SMD=-0.24, [95%CI: -0.62, 0.15], I2 = 57%) (Fig. 2D) [22, 32, 37, 40, 46, 49].
To understand inter-study heterogeneity, we further performed a subgroup analysis according to the BMI and country of participants for sufficient studies in PCOS (Table S4). It should be noted that BMI may have an association with findings. Decreases in alpha diversity indices were consistently seen in obese PCOS patients and heterogeneity between studies was substantially reduced to 0%. We noticed that the majority of studies were conducted in China, suggesting whether the findings were influenced by dietary structures between different countries. All three indices showed different outcomes in China compared with others, with moderate heterogeneity still observed.
With regard to vaginal microbiome composition, 10 studies provided data on Chao1 in patients (n = 656) versus controls (n = 736), and there was a significant increase in patients (SMD = 1.15, [95%CI: 0.74, 1.56], I2 = 91%) (Fig. 3A) [50,51,52,53,54,55,56,57,58,59]. Data on Shannon index were reported by 17 studies in patients (n = 771) versus controls (n = 925) [39, 50, 51, 53,54,55,56,57,58,59,60,61,62,63,64,65,66]. The pooled estimate demonstrated a significant increase in patients (SMD = 0.51, [95%CI: 0.16, 0.86], I2 = 91%) (Fig. 3B). Seven studies provided data on Simpson in patients (n = 231) vs. controls (n = 233), and the difference between them was not significant (SMD = 0.44, [95%CI: -0.18, 1.07], I2 = 90%) (Fig. 3C) [50, 54, 55, 62, 63, 65, 67]. Within diagnostic categories, those increases were mainly seen in CIN and CCA with moderate to high heterogeneity.

Forest Plots of Alpha Diversity in the Genital Microbiota of Patients with Gynecological Diseases Compared with Healthy Controls. (A to C) Alpha Diversity in the vaginal microbiota (A) Chao1. (B) Shannon index. (C) Simpson index. (D) Shannon index in the cervical microbiota
As for cervical microbiota, nine studies provided data on the Shannon index in patients (n = 81) versus controls (n = 105) [39, 40, 64, 66, 68,69,70,71,72]. The pooled data showed no significant differences (SMD = 0.08, [95%CI: -0.23, 0.38], I2 = 66%) (Fig. 3D). Only four studies provided data on Simpson, which were not included in the meta-analysis [40, 70,71,72].
Beta diversity
Beta diversity compares the differences in microbial community composition between samples from different body sites in patients and controls. 68 of the 87 studies conducted beta diversity using variable measures (Table S5). Regarding fecal microbiota, 30 studies assessed the beta diversity between patients and controls. Among them, 3 of 5 studies in EM, 4 of 21 in PCOS, and 1 of 3 in cervical cancer reported significant differences. In the vaginal microbiota, 4 of 5 studies in BV showed significant differences between groups, and one study showed consistently significant difference of beta diversity between groups with HPV infection, cervical dysplasia, and cervical cancer. In the cervical microbiota, consistent no significant differences were reported by all three studies in EM and one in PCOS. Because of the different grades of lesions in patients with CIN and cervical cancer, the beta diversity of the different studies could not be combined for analysis. All of the two studies in ovarian tissue and more than half of the studies of peritoneal fluid reported significant differences, while most of the studies of endometrial tissue showed no significant difference.
Differentially abundant microbial taxa
We summarized the representative taxa at three levels (phylum, family, and genus). Seventy of the 87 studies assessed the relative abundance of microbial taxa between patients and control groups. Overall, 22 phyla, 50 families, and 154 genera were identified from six different sample types, including stool, vaginal swab, cervical mucus, endometrial tissue (ET), ovarian tissue (OT), and peritoneal fluid (PF). To summarize within- and between- disease comparisons for the microbial taxa, in studies reporting the same microbes, findings with less than 60% agreement were categorized as “not consistent” (Fig. 4).

Summary of Changes in Relative Abundance of Microbial Taxa (Phylum, Family, Genus) by at Least 2 Studies from a Diagnostic Category. ET, endometrial tissue; PF, peritoneal fluid; * consistent in 3 or more studies
Disease specificity
If a taxon was altered in the same direction in only a single disease and was consistent in more than two studies, it was considered a candidate for disease specificity. Thus, our findings indicate some disease-specific alterations, such as the depletion of Odoribacter and Paraprevotella in PCOS. We also observed a depletion of Bifidobacterium in CIN. There was also evidence of the enrichment of Aerococcus, Eggerthella and Gemella in BV. However, there was limited evidence of these disease specificities because the majority of the consistent within-disease alterations were reproduced in only three studies.
Shared alteration across diseases
Our study indicates a consistent alteration across diseases for certain microbes. The most consistent changes were the enrichment of Prevotella (PCOS, BV, and CC) and the depletion of Lactobacillus in three diseases (PCOS, BV, and CC). The Clostridium and Megasphaera genera were enriched in both BV and CIN, whereas Sneathia was enriched in both BV and CC. Therefore, an overlap between BV, CIN, and CC was implied in the vaginal microbiota.
Discussion
This meta-analysis assessed microbiota alterations with the aim of evaluating consistency or specificity across a spectrum of gynecological diseases. We summarized the alpha diversity (within sample), beta diversity (between samples), and differentially abundant microbial taxa at the phylum, family, and genus levels. The main findings were as follows: [1] a small effect size decrease in observed species and Shannon index of gut microbiota; a moderate to large effect size increase in Chao1 and Shannon index of vaginal microbiota; [2] significant differences of β diversity were reported mostly in EM and BV, whereas no significant differences were frequently reported; [3] disease specificity was observed in three diseases, but almost all the changes were only replicated in three studies, except for Aerococcus in BV; [4] patients with major gynecological diseases shared the general changes of the enrichment of Prevotella and the depletion of Lactobacillus in vaginal samples; an overlap was implied between BV, CIN, and CC.
In terms of alpha diversity, our meta-analysis showed that both richness and diversity of the gut microbiota in patients with gynecological diseases showed a statistically significant decrease. In terms of individual diagnosis, the Shannon index of gut microbiota was significantly decreased in EM patients with no heterogeneity between studies. In previous animal experiments, EM mice showed a significant decrease in Shannon index and metabolites like alpha-linolenic acid, which can increase the expression of the ZO-2 protein in the intestinal wall, reduce the content of LPS and the aggregation of macrophages in the peritoneum, as well as decreased the oxidative stress and inflammation [73,74,75]. However, Yuan et al. [76] reported no significant difference in Shannon index. The pooled estimate of our meta-analysis favored a reduction in the diversity of the intestinal flora of the EM patients, in accordance to the hypothesis that diverse communities may increase the stability and productivity of an ecosystem. Moreover, antibiotic-induced microbiota-depleted mice has shown a reduction of endometriotic lesion, possibly by fecal metabolite like quinic acid and modulation of immune cell populations like macrophages in peritoneum [77].
On the other hand, the observed species and Shannon index in PCOS patients were significantly decreased. The subgroup analysis on their BMI demonstrated that observed species, Chao1, and Shannon index were significantly decreased in obese PCOS patients with 0-13% heterogeneity, but no significant differences were shown of Chao1 and Shannon in non-obese patients. Obesity is one of the representative features of PCOS, which was associated with lower alpha diversity of the gut microbiome in previous meta-analyses [78,79,80]. As we suspected, metabolism and obesity have specific interactions with the gut microbiome of PCOS, but the mechanism remains to be further demonstrated. Generally, gut microbiome may contributed to PCOS by affecting energy absorption, short chain fatty acids, lipopolysaccharide, choline and bile acid, intestinal permeability and the brain-gut axis [81]. Meanwhile, in the reproductive endocrine system, the gut microbiome has a complex interaction with insulin, estrogen, and testosterone. The intestinal flora promotes the glucose metabolism disorder of PCOS possibly through the FXR signaling pathway, while the removement of it decreases serum testosterone levels, ameliorated insulin resistance and increased relative FXR mRNA levels [30]. Microbiome is also affected by genetic, nutritional, and environmental factors, resulting in a high heterogeneity among individuals [9]. Through meta-analysis and subgroup analysis, we tried to minimize the effect of heterogeneity among studies and obtained more trustworthy pooled results.
Vaginal microbiota dysbiosis, characterized by a progressive replacement of certain Lactobacillus species by pathogenic microorganisms who can develop biofilms, plays an important role in gynecological diseases [82, 83]. Analysis showed that Chao1 and Shannon indices were significantly increased in patients, mainly in CIN and CCA, which proved that vaginal dysbiosis was associated with an increased risk of persistent HPV infection and cervical dysplasia, as previous studies carried out [14, 15, 84, 85]. Meanwhile, no significant differences were observed in cervical microbiota.
In our meta-analysis, we found that studies related to upper genital tract remain very few. A recent study revealed that intracellular microbiota in breast tumor tissue regulated the host-cell viability and metastatic colonization through reorganizing actin cytoskeleton and enhancing resistance to fluid shear stress [86]. Another study has demonstrated the microbial continuum in the female reproductive tract, with different microbial communities distributed from lower to upper genital tract. ET and PF samples contains lower bacterial biomass but higher diversity than vaginal sites, which is similar to tumor tissue [6]. These findings give us a hint that future studies can investigate more about the microbiota in tissues and its mechanism to uterine-related diseases such as EM, EC, and OC.
As for beta diversity, most studies of different diagnostic categories and sites demonstrated no significant differences between patients and controls, or conflicting results between studies. No consistent changes were observed, suggesting that the measurement of beta diversity may not be suitable as a diagnostic biomarker.
In general, disease specificity was observed in PCOS, BV, and CIN, but these alterations were weakly reproduced because most of the consistent within-disease changes were replicated in only three studies. It is worth noting that the Aerococcus genus was enriched in four of seven studies on BV (Figure S2D), which can also cause urinary tract infections and infective endocarditis [87, 88]. Furthermore, the Odoribacter genus was decreased in PCOS, which is a promising probiotic for its ability to improve glucose tolerance and inflammation related to obesity [89]. Researchers have found that the trypsin-degrading property is conserved in all Paraprevotella strains, which were also decreased in PCOS [90]. In addition, the Streptococcus genus, a pro-inflammatory microbe, was increased in the fecal and peritoneal fluid of EM patients, which is consistent with a previous meta-analysis reporting its enrichment in cervical mucus and endometrial tissue [11]. This indicated the migration of microbes along the genital tract, thus contributing to the imbalance of bacteria in the peritoneal fluid.
Our findings indicate shared alterations of vaginal microbial changes between BV, CIN, and CC, as mentioned before. Most consistently in vaginal microbiota, the Clostridium, Sneathia, Megasphaera, and Prevotella genera were enriched, while the Lactobacillus genus was depleted. A study on Prevotella reported its relation with the production of sialidase, an enzyme that enhances the ability of microorganisms to invade and destroy tissue [91]. Candidate gene analysis also showed associations between genetic variants of interleukin-5 and the abundance of Prevotella spp [92]. Recently, another study suggested that Prevotella was significantly correlated with the expression levels of NF-κB and C-myc in cervical cells, influencing the occurrence of HPV infection and cervical lesions [93].
Strengths and limitations
To the best of our knowledge, this is the first meta-analysis that integrates microbiota alterations across the wide range of gynecological diseases. However, the limitations of this study must be mentioned. First, the modest sample sizes of some included studies and the small number of studies on the upper genital tract may have undermined the reliability of the related results, requiring further validation with larger sample sizes. Second, inter-study heterogeneity was observed, especially in vaginal samples, which makes the findings difficult to replicate and the quality of the evidence reported low. Additional subgroup analyses are required to explore the sources of heterogeneity. Third, because of the exclusion of studies with interventions, we were unable to explore the confounding effects of antibiotics or other treatments, since we know antimicrobial resistance has been more frequent especially in BV [94]. Finally, our study focused on microbial composition rather than function. The role of gut and genital microbiota in gynecological diseases should be further elucidated by functional analysis.
Conclusion
Our study demonstrated that alterations in gut and genital microbiota are associated with major gynecological diseases. The overall results showed a decrease of diversity in gut microbiota and an increase in genital tract. The most observed results were shared alterations across diseases rather than disease-specific alterations. Therefore, further investigation is required to identify specific biomarkers that may serve as promising diagnostics in the future and to explore the mechanisms and pathways between gynecological diseases and microbial alterations.
Data availability
The authors confirm that the data are available within the article, supplementary materials, and referenced literature, from which the data were extracted.
References
Ley RE, Bäckhed F, Turnbaugh P, Lozupone CA, Knight RD, Gordon JI. Obesity alters gut microbial ecology. Proc Natl Acad Sci U S A. 2005;102(31):11070–5.
Cai J, Sun L, Gonzalez FJ. Gut microbiota-derived bile acids in intestinal immunity, inflammation, and tumorigenesis. Cell Host Microbe. 2022;30(3):289–300.
Visconti A, Le Roy CI, Rosa F, Rossi N, Martin TC, Mohney RP, et al. Interplay between the human gut microbiome and host metabolism. Nat Commun. 2019;10(1):4505.
Gopalakrishnan V, Helmink BA, Spencer CN, Reuben A, Wargo JA. The influence of the gut microbiome on Cancer, immunity, and Cancer Immunotherapy. Cancer Cell. 2018;33(4):570–80.
Ansbacher R, Boyson WA, Morris JA. Sterility of the uterine cavity. Am J Obstet Gynecol. 1967;99(3):394–6.
Chen C, Song X, Wei W, Zhong H, Dai J, Lan Z, et al. The microbiota continuum along the female reproductive tract and its relation to uterine-related Diseases. Nat Commun. 2017;8:875.
Salinas AM, Osorio VG, Endara PF, Salazar ER, Vasco GP, Vivero SG, et al. Bacterial identification of the vaginal microbiota in Ecuadorian pregnant teenagers: an exploratory analysis. PeerJ. 2018;6:e4317.
Salinas AM, Osorio VG, Pacha-Herrera D, Vivanco JS, Trueba AF, Machado A. Vaginal microbiota evaluation and prevalence of key pathogens in Ecuadorian women: an epidemiologic analysis. Sci Rep. 2020;10(1):18358.
Qi X, Yun C, Pang Y, Qiao J. The impact of the gut microbiota on the reproductive and metabolic endocrine system. Gut Microbes. 2021;13(1):1894070.
Borella F, Carosso AR, Cosma S, Preti M, Collemi G, Cassoni P, et al. Gut microbiota and gynecological cancers: a summary of pathogenetic mechanisms and future directions. ACS Infect Dis. 2021;7(5):987–1009.
Leonardi M, Hicks C, El-Assaad F, El‐Omar E, Condous G. Endometriosis and the microbiome: a systematic review. BJOG. 2020;127(2):239–49.
Salmeri N, Sinagra E, Dolci C, Buzzaccarini G, Sozzi G, Sutera M, et al. Microbiota in irritable bowel syndrome and endometriosis: birds of a feather flock Together—A. Rev Microorganisms. 2023;11(8):2089.
Guo J, Shao J, Yang Y, Niu X, Liao J, Zhao Q, et al. Gut microbiota in patients with polycystic ovary syndrome: a systematic review. Reprod Sci. 2022;29(1):69–83.
Norenhag J, Du J, Olovsson M, Verstraelen H, Engstrand L, Brusselaers N. The vaginal microbiota, human papillomavirus and cervical dysplasia: a systematic review and network meta-analysis. BJOG: Int J Obstet Gy. 2020;127(2):171–80.
Wang H, Ma Y, Li R, Chen X, Wan L, Zhao W. Associations of Cervicovaginal Lactobacilli with High-Risk Human Papillomavirus Infection, cervical intraepithelial neoplasia, and Cancer: a systematic review and Meta-analysis. J Infect Dis. 2019;220(8):1243–54.
Pacha-Herrera D, Erazo-Garcia MP, Cueva DF, Orellana M, Borja-Serrano P, Arboleda C, et al. Clustering analysis of the Multi-microbial Consortium by Lactobacillus species against vaginal dysbiosis among Ecuadorian women. Front Cell Infect Microbiol. 2022;12:863208.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5.
Nikolova VL, Hall MRB, Hall LJ, Cleare AJ, Stone JM, Young AH. Perturbations in Gut Microbiota Composition in Psychiatric disorders: a review and Meta-analysis. JAMA Psychiatry. 2021;78(12):1343–54.
Shi J, Luo D, Weng H, Zeng XT, Lin L, Chu H, et al. Optimally estimating the sample standard deviation from the five-number summary. Res Synth Methods. 2020;11(5):641–54.
Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14(1):135.
Shan J, Ni Z, Cheng W, Zhou L, Zhai D, Sun S, et al. Gut microbiota imbalance and its correlations with hormone and inflammatory factors in patients with stage 3/4 endometriosis. Arch Gynecol Obstet. 2021;304(5):1363–73.
Eyupoglu ND, Ergunay K, Acikgoz A, Akyon Y, Yilmaz E, Yildiz BO. Gut microbiota and oral contraceptive use in overweight and obese patients with polycystic ovary syndrome. J Clin Endocrinol Metabolism. 2020;105(12):e4792–800.
He F, Li Y. The gut microbial composition in polycystic ovary syndrome with insulin resistance: findings from a normal-weight population. J Ovarian Res. 2021;14(1):50.
Liang Y, Ming Q, Liang J, Zhang Y, Zhang H, Shen T. Gut microbiota dysbiosis in polycystic ovary syndrome: association with obesity — a preliminary report. Can J Physiol Pharmacol. 2020;98(11):803–9.
Liang Z, Di N, Li L, Yang D. Gut microbiota alterations reveal potential gut–brain axis changes in polycystic ovary syndrome. J Endocrinol Invest. 2021;44(8):1727–37.
Liu R, Zhang C, Shi Y, Zhang F, Li L, Wang X et al. Dysbiosis of Gut Microbiota Associated with Clinical Parameters in Polycystic Ovary Syndrome. Front Microbiol [Internet]. 2017 Feb 28 [cited 2023 Apr 6];8. Available from: http://journal.frontiersin.org/article/https://doi.org/10.3389/fmicb.2017.00324/full.
Mammadova G, Ozkul C, Yilmaz Isikhan S, Acikgoz A, Yildiz BO. Characterization of gut microbiota in polycystic ovary syndrome: Findings from a lean population. Eur J Clin Invest [Internet]. 2021 Apr [cited 2023 Feb 22];51(4). Available from: https://onlinelibrary.wiley.com/doi/https://doi.org/10.1111/eci.13417.
Torres PJ, Siakowska M, Banaszewska B, Pawelczyk L, Duleba AJ, Kelley ST, et al. Gut Microbial Diversity in Women with Polycystic Ovary Syndrome correlates with hyperandrogenism. J Clin Endocrinol Metabolism. 2018;103(4):1502–11.
Yang YL, Zhou WW, Wu S, Tang WL, Wang ZW, Zhou ZY, et al. Intestinal Flora is a key factor in insulin resistance and contributes to the development of polycystic ovary syndrome. Endocrinology. 2021;162(10):bqab118.
Zhou L, Ni Z, Yu J, Cheng W, Cai Z, Yu C. Correlation between fecal metabolomics and gut microbiota in obesity and polycystic ovary syndrome. Front Endocrinol. 2020;11:628.
Zhou L, Ni Z, Cheng W, Yu J, Sun S, Zhai D, et al. Characteristic gut microbiota and predicted metabolic functions in women with PCOS. Endocr Connections. 2020;9(1):63–73.
Kang GU, Jung DR, Lee YH, Jeon SY, Han HS, Chong GO, et al. Dynamics of Fecal Microbiota with and without Invasive Cervical Cancer and its application in early diagnosis. Cancers. 2020;12(12):3800.
Wang Z, Wang Q, Zhao J, Gong L, Zhang Y, Wang X, et al. Altered diversity and composition of the gut microbiome in patients with Cervical cancer. AMB Expr. 2019;9(1):40.
Chen F, Chen Z, Chen M, Chen G, Huang Q, Yang X, et al. Reduced stress-associated FKBP5 DNA methylation together with gut microbiota dysbiosis is linked with the progression of obese PCOS patients. Npj Biofilms Microbiomes. 2021;7(1):60.
Insenser M, Murri M, del Campo R, Martínez-García MÁ, Fernández-Durán E, Escobar-Morreale HF. Gut microbiota and the polycystic ovary syndrome: influence of sex, sex hormones, and obesity. J Clin Endocrinol Metabolism. 2018;103(7):2552–62.
Li G, Liu Z, Ren F, Shi H, Zhao Q, Song Y, et al. Alterations of gut microbiome and fecal fatty acids in patients with polycystic ovary syndrome in Central China. Front Microbiol. 2022;13:911992.
Yin G, Chen F, Chen G, Yang X, Huang Q, Chen L, et al. Alterations of bacteriome, mycobiome and metabolome characteristics in PCOS patients with normal/overweight individuals. J Ovarian Res. 2022;15(1):117.
Ata B, Yildiz S, Turkgeldi E, Brocal VP, Dinleyici EC, Moya A, et al. The Endobiota Study: comparison of Vaginal, cervical and gut microbiota between women with stage 3/4 endometriosis and healthy controls. Sci Rep. 2019;9(1):2204.
Huang L, Liu B, Liu Z, Feng W, Liu M, Wang Y, et al. Gut microbiota exceeds cervical microbiota for early diagnosis of endometriosis. Front Cell Infect Microbiol. 2021;11:788836.
Svensson A, Brunkwall L, Roth B, Orho-Melander M, Ohlsson B. Associations between endometriosis and Gut Microbiota. Reprod Sci. 2021;28(8):2367–77.
Dong S, jiao J, Jia S, Li G, Zhang W, Yang K, et al. 16S rDNA full-length assembly sequencing technology analysis of intestinal Microbiome in Polycystic Ovary Syndrome. Front Cell Infect Microbiol. 2021;11:634981.
Hassan S, Kaakinen MA, Draisma H, Zudina L, Ganie MA, Rashid A, et al. Bifidobacterium is enriched in gut microbiome of Kashmiri women with polycystic ovary syndrome. Genes. 2022;13(2):379.
Lüll K, Arffman RK, Sola-Leyva A, Molina NM, Aasmets O, Herzig KH, et al. The gut Microbiome in Polycystic Ovary Syndrome and its Association with metabolic traits. J Clin Endocrinol Metabolism. 2021;106(3):858–71.
Qi X, Yun C, Sun L, Xia J, Wu Q, Wang Y, et al. Gut microbiota–bile acid–interleukin-22 axis orchestrates polycystic ovary syndrome. Nat Med. 2019;25(8):1225–33.
Yang Z, Fu H, Su H, Cai X, Wang Y, Hong Y, et al. Multi-omics analyses reveal the specific changes in gut metagenome and serum metabolome of patients with polycystic ovary syndrome. Front Microbiol. 2022;13:1017147.
Zhu X, Li Y, Jiang Y, Zhang J, Duan R, Liu L, et al. Prediction of Gut Microbial Community structure and function in polycystic ovary syndrome with high low-density lipoprotein cholesterol. Front Cell Infect Microbiol. 2021;11:665406.
Sims TT, Colbert LE, Zheng J, Delgado Medrano AY, Hoffman KL, Ramondetta L, et al. Gut microbial diversity and genus-level differences identified in Cervical cancer patients versus healthy controls. Gynecol Oncol. 2019;155(2):237–44.
Mao X, Peng X, Pan Q, Zhao X, Yu Z, Xu D. Uterine fibroid patients reveal alterations in the gut Microbiome. Front Cell Infect Microbiol. 2022;12:863594.
Ling Z, Kong J, Liu F, Zhu H, Chen X, Wang Y, et al. Molecular analysis of the diversity of vaginal microbiota associated with bacterial vaginosis. BMC Genomics. 2010;11(1):488.
Srinivasan S, Hoffman NG, Morgan MT, Matsen FA, Fiedler TL, Hall RW et al. Bacterial Communities in Women with Bacterial Vaginosis: High Resolution Phylogenetic Analyses Reveal Relationships of Microbiota to Clinical Criteria. Ratner AJ, editor. PLoS ONE. 2012;7(6):e37818.
Zozaya M, Ferris MJ, Siren JD, Lillis R, Myers L, Nsuami MJ, et al. Bacterial communities in penile skin, male urethra, and vaginas of heterosexual couples with and without bacterial vaginosis. Microbiome. 2016;4(1):16.
Kunaseth J, Waiyaput W, Chanchaem P, Sawaswong V, Permpech R, Payungporn S et al. Vaginal microbiome of women with adenomyosis: A case-control study. Staley C, editor. PLoS ONE. 2022;17(2):e0263283.
Hong X, Qin P, Huang K, Ding X, Ma J, Xuan Y, et al. Association between polycystic ovary syndrome and the vaginal microbiome: a case-control study. Clin Endocrinol. 2020;93(1):52–60.
Lu C, Wang H, Yang J, Zhang X, Chen Y, Feng R, et al. Changes in vaginal Microbiome Diversity in Women with Polycystic Ovary Syndrome. Front Cell Infect Microbiol. 2021;11:755741.
Nieves-Ramírez ME, Partida-Rodríguez O, Moran P, Serrano-Vázquez A, Pérez-Juárez H, Pérez-Rodríguez ME et al. Cervical Squamous Intraepithelial Lesions Are Associated with Differences in the Vaginal Microbiota of Mexican Women. Claesen J, editor. Microbiol Spectr. 2021;9(2):e00143-21.
Xia Y, Feng Y, Qin T, Zhao X, Lu J, Ma C. Characteristics of Vaginal Microbiome in Reproductive-Age Females with HPV Infection in Xinjiang, China. Tebyaniyan H, editor. Evidence-Based Complementary and Alternative Medicine. 2022;2022:1–10.
Zhang Y, Xu X, Yu L, Shi X, Min M, Xiong L, et al. Vaginal microbiota changes caused by HPV Infection in Chinese women. Front Cell Infect Microbiol. 2022;12:814668.
Chen Y, Qiu X, Wang W, Li D, Wu A, Hong Z, et al. Human papillomavirus Infection and cervical intraepithelial neoplasia progression are associated with increased vaginal microbiome diversity in a Chinese cohort. BMC Infect Dis. 2020;20(1):629.
Ceccarani C, Foschi C, Parolin C, D’Antuono A, Gaspari V, Consolandi C, et al. Diversity of vaginal microbiome and metabolome during genital Infections. Sci Rep. 2019;9(1):14095.
Chen HM, Chang TH, Lin FM, Liang C, Chiu CM, Yang TL, et al. Vaginal microbiome variances in sample groups categorized by clinical criteria of bacterial vaginosis. BMC Genomics. 2018;19(S10):876.
Tao Z, Zhang L, Zhang Q, Lv T, Chen R, Wang L, et al. The pathogenesis of Streptococcus anginosus in aerobic vaginitis. IDR. 2019;12:3745–54.
Hernandes C, Silveira P, Rodrigues Sereia AF, Christoff AP, Mendes H, de Valter LF, et al. Microbiome Profile of Deep Endometriosis patients: comparison of Vaginal Fluid, Endometrium and Lesion. Diagnostics. 2020;10(3):163.
Lin S, Zhang B, Lin Y, Lin Y, Zuo X. Dysbiosis of cervical and vaginal microbiota Associated with Cervical Intraepithelial Neoplasia. Front Cell Infect Microbiol. 2022;12:767693.
Xie Y, Feng Y, Li W, Zhan F, Huang G, Hu H, et al. Revealing the disturbed vaginal micobiota caused by Cervical Cancer using high-throughput sequencing technology. Front Cell Infect Microbiol. 2020;10:538336.
Zhang Z, Li T, Zhang D, Zong X, Bai H, Bi H, et al. Distinction between vaginal and cervical microbiota in high-risk human papilloma virus-infected women in China. BMC Microbiol. 2021;21(1):90.
Lynch T, Peirano G, Lloyd T, Read R, Carter J, Chu A et al. Molecular Diagnosis of Vaginitis: Comparing Quantitative PCR and Microbiome Profiling Approaches to Current Microscopy Scoring. Munson E, editor. J Clin Microbiol. 2019;57(9):e00300-19.
Akiyama K, Nishioka K, Khan KN, Tanaka Y, Mori T, Nakaya T et al. Molecular detection of microbial colonization in cervical mucus of women with and without endometriosis. Am J Reprod Immunol [Internet]. 2019 Aug [cited 2023 Feb 22];82(2). Available from: https://onlinelibrary.wiley.com/doi/https://doi.org/10.1111/aji.13147.
Audirac-Chalifour A, Torres-Poveda K, Bahena-Román M, Téllez-Sosa J, Martínez-Barnetche J, Cortina-Ceballos B et al. Cervical Microbiome and Cytokine Profile at Various Stages of Cervical Cancer: A Pilot Study. Tornesello ML, editor. PLoS ONE. 2016;11(4):e0153274.
Kwon M, Seo SS, Kim M, Lee D, Lim M. Compositional and functional differences between Microbiota and Cervical Carcinogenesis as identified by Shotgun Metagenomic sequencing. Cancers. 2019;11(3):309.
Wu S, Ding X, Kong Y, Acharya S, Wu H, Huang C, et al. The feature of cervical microbiota associated with the progression of Cervical cancer among reproductive females. Gynecol Oncol. 2021;163(2):348–57.
Zhai Q, Zhang W, Zhang Z, Fu Y, Li Y, Wang X, et al. Characteristics of the Cervicovaginal Microenvironment in Childbearing-Age women with different degrees of cervical lesions and HR-HPV positivity. Pol J Microbiol. 2021;70(4):489–500.
Pınar N, Soylu Karapınar O, Özcan O, Özgür T, Bayraktar S. Effect of alpha-lipoic acid on endometrial implants in an experimental rat model. Fundam Clin Pharmacol. 2017;31(5):506–12.
Ni Z, Sun S, Bi Y, Ding J, Cheng W, Yu J, et al. Correlation of fecal metabolomics and gut microbiota in mice with endometriosis. Am J Reprod Immunol. 2020;84(6):e13307.
Ni Z, Ding J, Zhao Q, Cheng W, Yu J, Zhou L, et al. Alpha-linolenic acid regulates the gut microbiota and the inflammatory environment in a mouse model of endometriosis. Am J Reprod Immunol. 2021;86(4):e13471.
Yuan M, Li D, Zhang Z, Sun H, An M, Wang G. Endometriosis induces gut microbiota alterations in mice. Hum Reprod. 2018;33(4):607–16.
Chadchan SB, Naik SK, Popli P, Talwar C, Putluri S, Ambati CR, et al. Gut microbiota and microbiota-derived metabolites promotes endometriosis. Cell Death Discov. 2023;9(1):28.
Wa W, Z X. R K. Meta-analyses of human gut microbes associated with obesity and IBD. FEBS letters [Internet]. 2014 Nov 17 [cited 2023 May 20];588(22). Available from: https://pubmed.ncbi.nlm.nih.gov/25307765/.
Sze MA, Schloss PD. Looking for a Signal in the noise: revisiting obesity and the Microbiome. mBio. 2016;7(4):e01018–16.
Mm F, Tj S, Tj L, Ks P. A taxonomic signature of obesity in the microbiome? Getting to the guts of the matter. PloS one [Internet]. 2014 Aug 1 [cited 2023 May 20];9(1). Available from: https://pubmed.ncbi.nlm.nih.gov/24416266/.
Zhao X, Jiang Y, Xi H, Chen L, Feng X. Exploration of the relationship between gut microbiota and polycystic ovary syndrome (PCOS): a review. Geburtshilfe Frauenheilkd. 2020;80(2):161–71.
Han Y, Liu Z, Chen T. Role of vaginal microbiota dysbiosis in Gynecological Diseases and the potential interventions. Front Microbiol. 2021;12:643422.
Machado A, Foschi C, Marangoni A. Editorial: vaginal dysbiosis and biofilms. Front Cell Infect Microbiol. 2022;12:976057.
Gillet E, Meys JFA, Verstraelen H, Verhelst R, De Sutter P, Temmerman M et al. Association between Bacterial Vaginosis and Cervical Intraepithelial Neoplasia: Systematic Review and Meta-Analysis. Atashili J, editor. PLoS ONE. 2012;7(10):e45201.
Brusselaers N, Shrestha S, van de Wijgert J, Verstraelen H. Vaginal dysbiosis and the risk of human papillomavirus and Cervical cancer: systematic review and meta-analysis. Am J Obstet Gynecol. 2019;221(1):9–18e8.
Fu A, Yao B, Dong T, Chen Y, Yao J, Liu Y, et al. Tumor-resident intracellular microbiota promotes metastatic colonization in Breast cancer. Cell. 2022;185(8):1356–1372e26.
Schuur PM, Kasteren ME, Sabbe L, Vos MC, Janssens MM, Buiting AG. Urinary tract Infections with Aerococcus urinae in the south of the Netherlands. Eur J Clin Microbiol Infect Dis. 1997;16(12):871–5.
Sunnerhagen T, Nilson B, Olaison L, Rasmussen M. Clinical and microbiological features of infective endocarditis caused by aerococci. Infection. 2016;44(2):167–73.
Huber-Ruano I, Calvo E, Mayneris-Perxachs J, Rodríguez-Peña MM, Ceperuelo-Mallafré V, Cedó L, et al. Orally administered Odoribacter laneus improves glucose control and inflammatory profile in obese mice by depleting circulating succinate. Microbiome. 2022;10:135.
Li Y, Watanabe E, Kawashima Y, Plichta DR, Wang Z, Ujike M, et al. Identification of trypsin-degrading commensals in the large intestine. Nature. 2022;609(7927):582.
Am B, Bj M, Ce S, Sl H. Sialidases (neuraminidases) in bacterial vaginosis and bacterial vaginosis-associated microflora. Journal of clinical microbiology [Internet]. 1992 Mar [cited 2022 Oct 30];30(3). Available from: https://pubmed.ncbi.nlm.nih.gov/1551983/.
Si J, You HJ, Yu J, Sung J, Ko G. Prevotella as a hub for vaginal microbiota under the influence of Host Genetics and Their Association with obesity. Cell Host Microbe. 2017;21(1):97–105.
Dong B, Huang Y, Cai H, Chen Y, Li Y, Zou H, et al. Prevotella as the hub of the cervicovaginal microbiota affects the occurrence of persistent human papillomavirus Infection and cervical lesions in women of childbearing age via host NF-κB/C-myc. J Med Virol. 2022;94(11):5519–34.
Muñoz-Barreno A, Cabezas-Mera F, Tejera E, Machado A. Comparative effectiveness of treatments for bacterial vaginosis: a Network Meta-Analysis. Antibiotics. 2021;10(8):978.
Acknowledgements
We sincerely thank Dr. Zhaohua Zhu (Clinical Research Centre, Zhujiang Hospital, Southern Medical University, Guangzhou, China) for the critical reading of this manuscript, and to Liujing Huang (Obstetrics and Gynecology Medical Center, Zhujiang Hospital, Southern Medical University, Guangzhou, China) for her kind help and support in the design of the study.
Funding
This work was supported by Guangdong Basic and Applied Basic Research Foundation (Grant Nos. 2022A1515011880, 2023A1515011688), and the President Foundation of Zhujiang Hospital, Southern Medical University (Grant No. yzjj2022ms18) to Ying Ma.
Author information
Authors and Affiliations
Contributions
Conceptualization, Y.M. and Z.Z; methodology, Z.Z.; screening and assessment of eligible studies, Y.F. and L.X.; data extraction, Y.F., L.X., Z.C., and S.M.; quality assessment, L.X. and S.M.; original draft preparation, Z.Z.; supervision and funding acquisition, Y.M. All authors have reviewed and agreed to the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
No ethical approval was required for this systematic review with meta-analysis.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhou, Z., Feng, Y., Xie, L. et al. Alterations in gut and genital microbiota associated with gynecological diseases: a systematic review and meta-analysis. Reprod Biol Endocrinol 22, 13 (2024). https://doi.org/10.1186/s12958-024-01184-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12958-024-01184-z