
Abstract
Background
Laparoscopic and robotic surgery for transverse colon cancer are difficult due to complex fusion of the foregut and midgut and variation of the vessels of the transverse colon. Although the vessels of the right colon have been investigated, middle colic artery (MCA) variation and the relationship with vessels around the transvers colon are unknown. We investigated variation of the MCA using computed tomography angiography (CTA) and cadaver specimen and the relationship between the superior mesenteric vein (SMV) and MCA using CTA. The classification of vessels around the transverse colon may lead to safer and reliable surgery.
Methods
This study included 505 consecutive patients who underwent CTA in our institution from 2014 to 2020 and 44 cadaver specimens. Vascular anatomical classifications and relationships were analyzed using CT images.
Results
The MCA was defined as the arteries arising from the superior mesenteric artery (SMA) that flowed into the transverse colon at the distal ends. The classifications were as follows: type I, branching right and left from common trunk; type II, the right and left branches bifurcated separately from the SMA; and type III, the MCA branched from a vessel other than the SMA. Type II was subclassified into two subtypes, type IIa with one left branch and type IIb with two or more left branches from SMA. In the CTA and cadaver studies, respectively, the classifications were as follows: type I, n = 290 and n = 31; type IIa, n = 211 and n = 13; type IIb, n = 3 and n = 0; and type III, n = 1 and n = 0. We classified the relationship between the MCA and left side of the SMV into three types: type A, a common trunk runs along the left edge of the SMV (n = 173; 59.7%); type B, a right branch of the MCA runs along the left edge of the SMV (n = 116; 40.0%); and type C, the MCA runs dorsal of the SMV (n = 1; 0.3%).
Conclusions
This study revealed that The MCA branching classifications and relationship between the SMV and MCA. Preoperative CT angiography may be able to reliably identify vessel variation, which may be useful in clinical practice.
Similar content being viewed by others

Background
Colorectal cancer is increasing worldwide. In Japan, the number of morbidities is also increasing. The standard strategy for colorectal cancer is surgical resection. Laparoscopic and robotic surgery have become widespread as minimally invasive approaches for colorectal cancer. Clinical studies showing the benefits of laparoscopic and robotic surgery often excluded transverse colon cancer [1,2,3]. Laparoscopic and robotic surgery for transverse colon cancer are associated with a greater degree of difficulty because of the complex fusion of the foregut and midgut and variation of the vessels of the transverse colon.
The frequency of ileocolic artery and right colic artery and vein variations [4,5,6,7,8,9,10,11,12] and accessary middle colic artery [13,14,15,16] has been reported, but few of studies have focused on the middle colic artery (MCA) [17, 18], and few studies have focused on the relationship between the MCA and superior mesenteric vein (SMV) and demonstrated vessel abnormalities using preoperative and perioperative visualization [19,20,21]. We considered that the relationship between the MCA and SMV has been very important in the case of lymph node dissection around the MCA. We considered that the safety and accuracy of lymph node dissection in transverse colon cancer have been increased based on research on vessels around the transverse colon mesentery.
We researched the variation of MCA bifurcation using cadaver specimens and dynamic computed tomography angiography. Moreover, using dynamic computed tomography (CT), we researched the relationship between the MCA and SMV and the frequency of variation of the MCA and artery of Moskowitz and the confluence of the inferior mesenteric vein (IMV).
In this study, we investigated the vessel variation and the interrelationships among the arteries and veins related to blood supply to the transverse colon. We considered that the classification of the variation and the frequency of the variation would be practically useful.
Methods
Patients
In the present study, 505 consecutive patients (male, n = 329; female, n = 176; median age 70 years [range, 21–97 years]) who underwent CT angiography at Ehime University Hospital from January 2014 to December 2020 were prospectively enrolled.
Cadavers
A total of 44 cadavers were dissected (male, n = 18; female, n = 26). The cadavers were excluded if there was any evidence of previous upper abdominal surgery or if peritoneal dissemination of digestive cancer was observed macroscopically in the peritoneal cavity.
CT angiography protocol and workstation
Patients underwent three-dimensional (3D) CT angiography using a 96- or 128- or 320-detector CT scanner. The tube potential was 120 kVp, and the tube current was adjusted by automatic exposure control with a noise index of 10 and a slice thickness of 0.5 mm. Iomeprol (350 mg I/ml, iomeron 350; Eisai, Tokyo, Japan) was used as contrast agent. Patients were injected with 0.6 g/kg iodine (upper limit, 47.25g) for 30 s at a rate of 2.6–4.5 ml/s. The bolus tracking method was initiated when the contrast in the thoracic aorta (diaphragm level) reached 150 Hounsfield units. Sixty seconds after the injection of iomeprol, the venous phase image was acquired. One hundred twenty seconds after the injection of contrast agent, the equilibrium phase image was acquired. An image processing analysis was performed using a 3D volume rendering technique with the Advantage Workstation system version 4.5 (GE Health care, Tokyo, Japan).
Definition of the middle colic artery and accessory middle colic artery
The MCA was defined as the arteries arising from the SMA that flowed into the transverse colon at the distal ends. In this study, when the MCA had two or three branches, the distance from the caudal branch was measured. The branching from vessels other than the SMA into the transverse colon was defined as the accessory middle colic artery. These definitions were developed according to 3D-CT images and axial and coronal CT scans. When the right and left branch branched from the common trunk, the length of the common trunk from the SMA was measured.
In the cadavers, the SMA was identified and the ventral peritoneum was incised. Then the SMA was dissected ventrally to reach the branch of the MCA. The first branch was dissected to the distal end, the right and left branches were identified, and the length of the common trunk was measured. In addition, the ventral dissection of the SMA was extended on the cranial side to check for other branches.
Intersectional patterns of the MCA and SMV
The MCA has a right branch that feeds the right side of the transverse colon and a left branch that feeds the left side. We evaluated the vessels running left ventral side of the SMV. We classified the MCA as common trunk running left on the ventral side of the SMV and a right branch; when there were two or more branches of the MCA, the first branch from the SMA was considered to be the right branch.
The artery of Moskowitz
The Moskowitz artery was defined as the vessel that directly anastomoses the middle and left colic artery. The Moskowitz artery was detected using 3D- and coronal two-dimensional CT images.
Drainage site of the inferior mesenteric vein (IMV)
The major portal vein is formed by the confluence of the splenic vein, SMV, and IMV. The IMV confluence was detected according to axial and coronal CT images in the venous phase.
Statistical analyses
All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). More precisely, it is a modified version of R commander designed to add statistical functions frequently used in biostatistics [22].
The results are expressed as the number of cases evaluated. Fisher’s exact test was used for categorical variables, and the Mann-Whitney U test was used for continuous variables. All P values were two-tailed. P values of < 0.05 were considered to indicate statistical significance.
Results
Classification of the MCA bifurcation
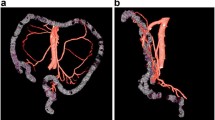
First, we classified middle colic arterial branching variation into three types (Fig. 1). According to the CT angiography and cadaver studies, respectively, the variation was classified as follows: type I, n = 290 and n = 31; type IIa, n = 211 and n = 13; type IIb, n = 3 and n = 0; and type III, n = 1 and n = 0 (Table 1). The frequency in the CT angiography and cadaver studies did not differ to a statistically significant extent (p = 0.182).

Classification of the MCA bifurcation. Type I, one right branch and one left branch of the MCA branch from the common trunk. Type II, one right branch and one left branch of the MCA branch separately from the SMA. Type II is divided into two subtypes. Type IIa, one right branch and one left branch of the MCA branch from the SMA. Type IIb, one right branch and two left branches of the MCA branch from the SMA. Type III, an MCA branches from a vessel other than the SMA. CA, celiac artery; MCA, middle colic artery; SMA, superior mesenteric artery
The length of the common trunk of the MCA
We investigated the length of the common trunk from the SMA to the bifurcation in type I. The length in the CT angiography and cadaver examinations was 2.6 cm (median, 0.1–9.0) and 2.8 cm (median, 0.5–6.3), respectively. There was no significant difference between the CT and cadaver studies (p = 0.713).
The distance from the first branch to other branches
In type II, the MCA has one or more branches from the SMA. Type IIa has one other branch and type IIb has two or more branches. In type IIa, the median distance was 1.8 cm (0.2–4.7 cm).
The relationship between the SMV and MCA
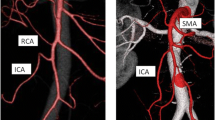
We classified the relationship between the MCA and the left side of the SMV into three types: in type A, a common trunk runs along the left edge of SMV (n = 173; 59.7%); in type B, a right branch of the MCA runs along the left edge of the SMV (n = 116; 40.0%); and in type C, the MCA runs dorsal of the SMV (n = 1; 0.3%) (Fig. 2).

The relationship between the SMV and the MCA. Type A, a common trunk runs along the left edge of the SMV. Type B, the right branch of the MCA runs along the left edge of the SMV. Type C, the MCA runs dorsal of the SMV. MCA, middle colic artery; SMV, superior mesenteric vein
Origin of the accessory MCA and the artery of Moskowitz
Eighteen cases had an accessory MCA. In SMA flow, 3 cases had a jejunal artery and 6 cases had a pancreatic artery. In celiac flow, 1 case had a celiac artery and 1 case had a common hepatic artery and 7 cases had a splenic artery (Table 2). A Moskowitz artery was present in 12 cases (2.4%).
Drainage site of IMV
We classified the drainage site of the IMV into three types: splenic vein (n = 226; 44.8%); SMV (n = 210; 41.6%); and simultaneous merging (n = 69; 13.6%) (Fig. 3).

The drainage site of the inferior mesenteric vein (IMV). a The IMV flows into the splenic vein and forms the portal vein. b The IMV flows into the superior mesenteric vein and forms the portal vein. c The IMV, SMV and splenic vein merge simultaneously to form the portal vein. IMV, inferior mesenteric vein; SMV, superior mesenteric vein
Discussion
The present study demonstrated three main points. The first point was the middle colic artery (MCA) branchial variation classification and frequency of accessory MCA (AMCA) branching from vessels other than the superior mesenteric artery (SMA) in cadaver and CT angiography studies. The second point was the relationship between the left edge of the superior mesenteric vein (SMV) and the MCA branch. The third point was the frequency of inferior mesenteric vein (IMV) drainage site.
Regarding the middle colic artery branchial variation classification and frequency of AMCA branching from vessels other than the SMA in cadaver and CT angiography studies, many reports have described the anatomy of the ileocolic and right colic artery and vein [4,5,6,7,8,9,10,11,12, 23,24,25]. Moreover, the effect of lymph node dissection in the right colectomy has been reported [26, 27]. Surgery for transverse colon cancer is highly difficult because of the many variations of the MCA and SMV branches. Clinical trials that provided evidence related to laparoscopic surgery, excluded subjects with transverse colon cancer due to the high degree of difficulty in these operations [1,2,3, 28, 29]. Since then, an approach to safely perform surgery for transverse colon cancer has been reported [30] and has gradually become popular. Hence, an understanding of the anatomy of the branching of the MCA is important for lymph node dissection. This current study presented the variation of these branch types and the frequency of the AMCA. According to the tumor location, lymph node dissection along the MCA is required for adequate dissection [31,32,33]. However, by cutting the root of the MCA, residual intestinal blood flow may be reduced, and the rates of postoperative complication such as anastomotic leakage may be higher. In the case of colon cancer surgery involving the liver flexure, while the main lymph node is dissected by cutting at the middle colic trunk in type I cases, the main lymph nodes are resected by isolating the right branch of the MCA in type II cases, and the residual transverse flow can be sufficient for the left branch flow. However, for middle or left transverse colon cancer, in type II, both branches of the MCA must be ligated in order to perform central vascular ligation (Fig. 4). In a CT angiography study, some cases were reported in which there was no margin at Griffiths’ point [34]; this was disadvantageous as peripheral vessels were not adequately contrasted [35]. The studies comparing preoperative CT angiography and intraoperative findings had shown that CT angiography was able to accurately detect the vessel root of the mesentery [19, 20]. On the other hand, cadaver research for colon vessels has been reported. In the cadaver study, in all cases, the splenic flexure was supplied by the marginal artery, and there was no area with poor blood flow [36]. Improvements in computed tomography quality have enabled the vessel construction to be studied in detail.

CT angiography and intraoperative findings of type I and type IIa MCA bifurcation. a CT imaging of a type I MCA bifurcation. The right and left branches of the MCA branch from the common trunk. b Intraoperative findings after main lymph node dissection by cutting the common trunk for extended right hemicolectomy in a case with a type I MCA. c CT imaging of a type IIa MCA bifurcation. The right and left branches of the MCA branch separately from the SMA. d Intraoperative view after main lymph node dissection with ligation of the right and left branches of a type IIa MCA for extended right hemicolectomy. CT, computed tomography; MCA, middle colic artery; MCV, middle colic vein; SMV, superior mesenteric vein; GCT, gastrocolic trunk
The analysis of the frequency of the AMCA has been reported [13,14,15,16]. Some studies focused on the splenic flexure and its relationship to the left colic artery [37, 38]. The analytical methods have been reported, with some studies using CT angiography and others using cadavers; the AMCA was reported to be present in 6.8–49.2%. In the present study, the MCA was defined as branching from the SMA. A recent meta-analysis reported the frequency of the AMCA and AMCA at the root. In the meta-analysis, an MCA was defined as an AMCA in a case in which it had a branch away from the first MCA branch [4]. Based on the results of our study, it is possible to reclassify vessels classified as an AMCA based on the proximal distance from the first MCA branch.
In the present study, the Moskowitz artery [39,40,41] was found in 2.4% of patients. The marginal artery was present in all cadavers in our cadaver study. We considered that the Moskowitz artery may develop laterally in collateral circulation due to stenosis or occlusion of the IMA. In our cases in which a Moskowitz artery was found, the calcification around the IMA was stronger in comparison to other cases.
The second point was the relationship between the left edge of the SMV and the MCA branch. It was considered that the SMV could be used as a landmark for lymph node dissection in the region of the MCA. The classification of the relationship between MCA bifurcation position and left edge of SMV has been reported [21]. In this study, we showed the patterns of intersection between the left edge of the SMV and the MCA branch and the frequency of each relationship [42]. It was suggested that the SMV could be used a landmark for sufficient and necessary lymph node dissection.
The third point was revealing the frequency of the IMV drainage site. The complex fusion of the fascial structures of the foregut, midgut, and hindgut makes resection for transverse colon cancer more difficult. Although the frequency of arterial branch variations has been investigated, confluence of the IMV had been reported to be very rare. It has been accepted that the IMV merges with the splenic vein. However, cadaver studies have reported that in this confluence, the IMV drainages to the splenic vein or SMV or the simultaneous SMV, IMV, and splenic vein [43]. Moreover, it has been reported—based on CT angiography and a physical model study—that the IMV drains to the splenic vein, the SMV, or the jejunal vein [44]. In our study, we revealed the frequency of IMV merging using CT angiography and classified the types of confluence. This result supported the theory that the IMV and portal vein are the main flow vessels during embryonic development. It was considered that the diameter of the IMV was relatively narrower because of the abundant blood flow in the SMV and splenic vein.
The present study was associated with some limitations. First, vascular bifurcation was detected on CT angiography but was not confirmed during actual surgery. However, we considered that CT angiography was useful because of reports comparing it to actual intraoperative findings. Second, the definitions of the MCA and AMCA differed in each study. In our study, we considered that the MCA branched from the SMA and showed the distance between each branch and the length of the common trunk. Third, the present study was conducted in a single institution and only analyzed Japanese subjects.
Conclusions
We reported our MCA branching classifications and the relationship between the left edge of the SMV and the MCA. We considered that preoperative CT angiography may be able to reliably identify vessel variations, which may be practically useful.
Availability of data and materials
Not applicable.
Abbreviations
- MCA:
-
Middle colic artery
- SMV:
-
Superior mesenteric vein
- CT:
-
Computed tomography
- IMV:
-
Inferior mesenteric vein
- 3D:
-
Three dimensional
- AMCA:
-
Accessory middle colic artery
- GCT:
-
Gastrocolic trunk
References
Jayne DG, Guillou PJ, Thorpe H, Quirke P, Copeland J, Smith AM, et al. Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J Clin Oncol. 2007;25(21):3061–8.
Yamamoto S, Inomata M, Katayama H, Mizusawa J, Etoh T, Konishi F, et al. Short-term surgical outcomes from a randomized controlled trial to evaluate laparoscopic and open D3 dissection for stage II/III colon cancer: Japan Clinical Oncology Group Study JCOG 0404. Ann Surg. 2014;260(1):23–30.
Buunen M, Veldkamp R, Hop WC, Kuhry E, Jeekel J, Haglind E, et al. Survival after laparoscopic surgery versus open surgery for colon cancer: long-term outcome of a randomised clinical trial. Lancet Oncol. 2009;10(1):44–52.
Cirocchi R, Randolph J, Davies RJ, Cheruiyot I, Gioia S, Henry BM, et al. A systematic review and meta-analysis of variants of the branches of the superior mesenteric artery: the Achilles heel of right hemicolectomy with complete mesocolic excision? Colorectal Dis. 2021;23(11):2834–45.
Gamo E, Jiménez C, Pallares E, Simón C, Valderrama F, Sañudo JR, et al. The superior mesenteric artery and the variations of the colic patterns. A new anatomical and radiological classification of the colic arteries. Surg Radiol Anat. 2016;38(5):519–27.
Murono K, Kawai K, Ishihara S, Otani K, Yasuda K, Nishikawa T, et al. Evaluation of the vascular anatomy of the right-sided colon using three-dimensional computed tomography angiography: a single-center study of 536 patients and a review of the literature. Int J Colorectal Dis. 2016;31(9):1633–8.
Tajima Y, Ishida H, Ohsawa T, Kumamoto K, Ishibashi K, Haga N, et al. Three-dimensional vascular anatomy relevant to oncologic resection of right colon cancer. Int Surg. 2011;96(4):300–4.
Ogino T, Takemasa I, Horitsugi G, Furuyashiki M, Ohta K, Uemura M, et al. Preoperative evaluation of venous anatomy in laparoscopic complete mesocolic excision for right colon cancer. Ann Surg Oncol. 2014;21(Suppl 3):S429-35.
Kuzu MA, İsmail E, Çelik S, Şahin MF, Güner MA, Hohenberger W, et al. Variations in the vascular anatomy of the right colon and implications for right-sided colon surgery. Dis Colon Rectum. 2017;60(3):290–8.
Yamaguchi S, Kuroyanagi H, Milsom JW, Sim R, Shimada H. Venous anatomy of the right colon: precise structure of the major veins and gastrocolic trunk in 58 cadavers. Dis Colon Rectum. 2002;45(10):1337–40.
Lee SJ, Park SC, Kim MJ, Sohn DK, Oh JH. Vascular anatomy in laparoscopic colectomy for right colon cancer. Dis Colon Rectum. 2016;59(8):718–24.
Hamabe A, Park S, Morita S, Tanida T, Tomimaru Y, Imamura H, et al. Analysis of the vascular interrelationships among the first jejunal vein, the superior mesenteric artery, and the middle colic artery. Ann Surg Oncol. 2018;25(6):1661–7.
Cheruiyot I, Cirocchi R, Munguti J, Davies RJ, Randolph J, Ndung’u B, et al. Surgical anatomy of the accessory middle colic artery: a meta-analysis with implications for splenic flexure cancer surgery. Colorectal Dis. 2021;23(7):1712–20.
Miyake H, Murono K, Kawai K, Hata K, Tanaka T, Nishikawa T, et al. Evaluation of the vascular anatomy of the left-sided colon focused on the accessory middle colic artery: a single-centre study of 734 patients. Colorectal Dis. 2018;20(11):1041–6.
Yano M, Okazaki S, Kawamura I, Ito S, Nozu S, Ashitomi Y, et al. A three-dimensional computed tomography angiography study of the anatomy of the accessory middle colic artery and implications for colorectal cancer surgery. Surg Radiol Anat. 2020;42(12):1509–15.
Murono K, Miyake H, Hojo D, Nozawa H, Kawai K, Hata K, et al. Vascular anatomy of the splenic flexure, focusing on the accessory middle colic artery and vein. Colorectal Dis. 2020;22(4):392–8.
Ueki T, Nagai S, Manabe T, Koba R, Nagayoshi K, Nakamura M, et al. Vascular anatomy of the transverse mesocolon and bidirectional laparoscopic D3 lymph node dissection for patients with advanced transverse colon cancer. Surg Endosc. 2019;33(7):2257–66.
Milnerowicz S, Milnerowicz A, Taboła R. A middle mesenteric artery. Surg Radiol Anat. 2012;34(10):973–5.
Nesgaard JM, Stimec BV, Bakka AO, Edwin B, Ignjatovic D. Navigating the mesentery: a comparative pre- and per-operative visualization of the vascular anatomy. Colorectal Dis. 2015;17(9):810–8.
Nesgaard JM, Stimec BV, Bakka AO, Edwin B, Ignjatovic D. Navigating the mesentery: part II. Vascular abnormalities and a review of the literature. Colorectal Dis. 2017;19(7):656–66.
Andersen BT, Stimec BV, Edwin B, Kazaryan AM, Maziarz PJ, Ignjatovic D. Re-interpreting mesenteric vascular anatomy on 3D virtual and/or physical models: positioning the middle colic artery bifurcation and its relevance to surgeons operating colon cancer. Surg Endosc. 2022;36(1):100–8.
Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48(3):452–8.
Nigah S, Patra A, Chumber S. Analysis of the variations in the colic branching pattern of the superior mesenteric artery: a cadaveric study with proposal to modify its current anatomical classification. Cureus. 2022;14(5):e25025.
Alsabilah JF, Razvi SA, Albandar MH, Kim NK. Intraoperative archive of right colonic vascular variability aids central vascular ligation and redefines gastrocolic trunk of henle variants. Dis Colon Rectum. 2017;60(1):22–9.
Ignjatovic D, Sund S, Stimec B, Bergamaschi R. Vascular relationships in right colectomy for cancer: clinical implications. Tech Coloproctol. 2007;11(3):247–50.
Spasojevic M, Stimec BV, Dyrbekk AP, Tepavcevic Z, Edwin B, Bakka A, et al. Lymph node distribution in the d3 area of the right mesocolon: implications for an anatomically correct cancer resection. A postmortem study. Dis Colon Rectum. 2013;56(12):1381–7.
Yada H, Sawai K, Taniguchi H, Hoshima M, Katoh M, Takahashi T. Analysis of vascular anatomy and lymph node metastases warrants radical segmental bowel resection for colon cancer. World J Surg. 1997;21(1):109–15.
Lacy AM, García-Valdecasas JC, Delgado S, Castells A, Taurá P, Piqué JM, et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet. 2002;359(9325):2224–9.
Nelson H, Sargent DJ, Wieand HS, Fleshman J, Anvari M, Stryker SJ, et al. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med. 2004;350(20):2050–9.
Egi H, Nakashima I, Hattori M, Mukai S, Kochi M, Taguchi K, et al. Surgical techniques for advanced transverse colon cancer using the pincer approach of the transverse mesocolon. Surg Endosc. 2019;33(2):639–43.
Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S. Standardized surgery for colonic cancer: complete mesocolic excision and central ligation–technical notes and outcome. Colorectal Dis. 2009;11(4):354–64 (discussion 64-5).
West NP, Hohenberger W, Weber K, Perrakis A, Finan PJ, Quirke P. Complete mesocolic excision with central vascular ligation produces an oncologically superior specimen compared with standard surgery for carcinoma of the colon. J Clin Oncol. 2010;28(2):272–8.
Yang SY, Kim MJ, Kye BH, Han YD, Cho MS, Jeong SY, et al. Prospective study of oncologic outcomes after laparoscopic modified complete mesocolic excision for non-metastatic right colon cancer (PIONEER study): study protocol of a multicentre single-arm trial. BMC Cancer. 2020;20(1):657.
Toh JWT, Matthews R, Kim SH. Arc of riolan-preserving splenic flexure takedown during anterior resection: potentially critical to prevent acute anastomotic ischemia. Dis Colon Rectum. 2018;61(3):411–4.
Spasojevic M, Stimec BV, Fasel JF, Terraz S, Ignjatovic D. 3D relations between right colon arteries and the superior mesenteric vein: a preliminary study with multidetector computed tomography. Surg Endosc. 2011;25(6):1883–6.
Kuzu MA, Güner MA, Kocaay AF, İsmail E, Arslan MN, Tekdemir İ, et al. Redefining the collateral system between the superior mesenteric artery and inferior mesenteric artery: a novel classification. Colorectal Dis. 2021;23(6):1317–25.
Ke J, Cai J, Wen X, Wu X, He Z, Zou Y, et al. Anatomic variations of inferior mesenteric artery and left colic artery evaluated by 3-dimensional CT angiography: Insights into rectal cancer surgery - A retrospective observational study. Int J Surg. 2017;41:106–11.
Miyamoto R, Nagai K, Kemmochi A, Inagawa S, Yamamoto M. Three-dimensional reconstruction of the vascular arrangement including the inferior mesenteric artery and left colic artery in laparoscope-assisted colorectal surgery. Surg Endosc. 2016;30(10):4400–4.
Fisher DF Jr, Fry WJ. Collateral mesenteric circulation. Surg Gynecol Obstet. 1987;164(5):487–92.
Garcia-Granero A, Sánchez-Guillén L, Carreño O, Sancho Muriel J, Alvarez Sarrado E, Fletcher Sanfeliu D, et al. Importance of the Moskowitz artery in the laparoscopic medial approach to splenic flexure mobilization: a cadaveric study. Tech Coloproctol. 2017;21(7):567–72.
Karatay E, Javadov M. The importance of the Moskowitz artery as a lesser-known collateral pathway in the medial laparoscopic approach to splenic flexure mobilisation and its evaluation with preoperative computed tomography. Wideochir Inne Tech Maloinwazyjne. 2021;16(2):305–11.
Stimec BV, Andersen BT, Benz SR, Fasel JHD, Augestad KM, Ignjatovic D. Retromesenteric course of the middle colic artery-challenges and pitfalls in D3 right colectomy for cancer. Int J Colorectal Dis. 2018;33(6):771–7.
Al-Asari SF, Lim D, Min BS, Kim NK. The relation between inferior mesenteric vein ligation and collateral vessels to splenic flexure: anatomical landmarks, technical precautions and clinical significance. Yonsei Med J. 2013;54(6):1484–90.
Andersen BT, Stimec BV, Kazaryan AM, Rancinger P, Edwin B, Ignjatovic D. Re-interpreting mesenteric vascular anatomy on 3D virtual and/or physical models, part II: anatomy of relevance to surgeons operating splenic flexure cancer. Surg Endosc. 2022;36(12):9136–45.
Acknowledgements
The authors thank the experts at Japan Medical Communication by Brian Quinn for English copyediting.
Funding
The authors declare that they have no funding, and this study received no funding.
Author information
Authors and Affiliations
Contributions
Y.O. drafted the manuscript. E.H., K.I., S.K., M.Y., S.K., S.A., H.S., H.M., T.S., and A.T. collected the radiological and cadaver data and helped draft the manuscript. E.H and Y.W. reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Because this study was a retrospective study, informed consent was replaced by the obligation of information to the participants to opt out. This study was approved by the Ethics Committee of the Ehime university (number: 1902016).
Consent for publication
Because this study was a retrospective study, agreement to use their medical data for research and publication was replaced by the obligation of information to opt out.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ogi, Y., Egi, H., Ishimaru, K. et al. Cadaveric and CT angiography study of vessels around the transverse colon mesentery. World J Surg Onc 21, 36 (2023). https://doi.org/10.1186/s12957-023-02919-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-023-02919-9