
Abstract
Purpose
The aim of the present study was to explore the efficacy and safety of transurethral needle electrode resection and transurethral holmium laser resection of non-muscular invasive bladder cancer (NMIBC).
Patients and methods
In this prospective, case-control study, patients from the Urinary Surgery or Oncology Department who met the inclusion and exclusion criteria received transurethral needle electrode resection (n = 52) or transurethral holmium laser resection (n = 51).
Results
A total of 103 patients with NMIBC were included in the present study, with 68 males and 35 females. Their mean age was 57.3 years. Sixty-two patients had Ta, 15 patients had T1, and 26 patients had Tis. Operative time, intraoperative blood loss, postoperative gross hematuria time, bladder irrigation time, and postoperative hospitalization time were all significantly lower in the transurethral holmium laser resection group than the transurethral needle electrode resection group. After resection, transurethral holmium laser resection significantly decreased the value of HGF, TSH, and TNF-α versus the transurethral needle electrode resection group. The incidence of obturator reflex was significantly lower in the transurethral holmium laser resection group than the transurethral needle electrode resection group. There was no significant difference in disease-free survival rate and progression-free survival rate between the two groups.
Conclusions
Transurethral holmium laser resection has clinical advantages in the treatment of NMIBC.
Similar content being viewed by others


Introduction
Bladder cancer is a common malignancy of the urinary system, and its incidence ranks 9th in the world, 6th in men, and 10th in women. The ratio of male to female incidence is 3:1. According to a 2018 epidemiological report, there were about 78,100 new cases of bladder cancer in China (including about 60,600 cases of male, 17,500 of female), and the incidence is 5.71/10 (8.65/10 of male, 2.62/10 of female). Currently, bladder cancer still carries the highest incidence of urinary reproductive system tumors in China. Pathologically, bladder cancer is divided into muscle- and non-muscle-invasive bladder cancer (NMIBC). NMIBC, which can further develop into muscle-infiltrating bladder cancer, accounts for 70 ~ 80% bladder cancer cases, and 20 ~ 25% of patients with NMIBC have poor prognosis [1,2,3]. At present, the main problems in clinical practice are insufficient understanding of the risk of NMIBC, which is generally considered to be a low-grade malignancy with a low diagnosis rate of carcinoma in situ (CIS), irregular treatment of special histological types of NMIBC, inadequate treatment of high-risk NMIBC, irregular bladder perfusion treatment, and other problems worthy of attention. The surgical methods of NMIBC include transurethral resection of bladder tumor, photodynamic therapy, transurethral laser surgery, partial cystectomy, and radical cystectomy (RC). RC is divided into three types: open, laparoscopic, and robot-assisted laparoscopic RC. There is substantial evidence that RC is still the most commonly used treatment for high-risk NMIBC or patients who develop muscle-layer infiltration [4, 5].
In this study, we aimed to explore the efficacy of transurethral needle electrode resection and transurethral holmium laser resection for NMIBC based on a prospective case-control study and to provide a basis for the selection of clinical treatment.
Patients and methods
Patient selection
This prospective case-control study was conducted from January 2015 to November 2016 at the Department of Urology, Renmin Hospital, Shiyan, China. The study was approved and monitored by the Ethics Committee of Renmin Hospital, Hubei Medical University (approval no. 2017-017). Patients, who were admitted to the Urinary Surgery or Oncology Department, were recruited if they met the following criteria: (1) age ≥ 18 years; (2) pathologically or histologically confirmed primary non-muscular invasive urothelial carcinoma of the bladder (Ta, Tis, T1); (3) Eastern Cooperative Oncology Group (ECOG) performance status (PS) score 0–2; (4) imaging examination showed that bladder cancer did not involve the bladder muscle layer and there was no lymph node metastasis or distant metastasis; (5) subjects who agreed to receive transurethral needle electrode resection or transurethral holmium laser resection and who can be followed up according to postoperative routine perfusion treatment; (6) the function of the main organs (heart, liver, lung, and kidney) was basically normal and ECOG performance status (PS) score 0–2; (7) bladder capacity ≥ 200 mL; and (8) patients provided written informed consent.
Exclusion criteria were as follows: (1) patients diagnosed with muscle-infiltrating urothelial carcinoma of the bladder (stage T2 or above); (2) patients had a history of bladder contracture or bladder functional volume less than 200 mL; (3) severe urethral stricture did not allow entry of a cystoscope; (4) pelvic computed tomography (CT) scan or systemic physical examination revealed tumor metastasis; (5) patients had other concurrent uropoiesis reproductive system tumors (above upper tract urothelial carcinoma, etc.) or tumor in other organs; (6) patients had hereditary or acquired coagulation disorders or were using anticoagulant drugs; (7) significant dysfunction of the main internal organs, such as 1.5 times greater than the upper normal limit of creatinine, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and total bilirubin; (8) decreased hematopoietic function of the bone marrow: leucocytes < 3.0 × 109/L, hemoglobin < 80 g/L, neutrophils < 1.5 × 109/L, platelets < 75 × 109/L, or other hematological diseases; (9) known immunodeficiency, acquired or congenital immunodeficiency, or a history of organ transplantation; (10) metastasis or invasion of the tumor center or various mental disorders; (11) patients had severe cardiovascular and cerebrovascular diseases, such as myocardial infarction, severe/unstable angina pectoris, coronary/peripheral artery bypass graft, symptomatic congestive heart failure, cerebrovascular accident or transient ischemic attack, or pulmonary embolism, who cannot tolerate transurethral resection of bladder tumor (TURBT) surgery; (12) severe hypertension (systolic blood pressure ≥ 180 mmHg, diastolic blood pressure ≥ 110 mmHg), or serious complications of hypertension, or serious complications of diabetes; (13) subjects with fever exceeding 38 °C and significant active infections that may affect the clinical trial, such as acute pneumonia, active tuberculosis, and severe urinary tract infection; (14) those who participated in other clinical trials within 3 months before screening; (15) patients who had received chemotherapeutic drugs or bacille Calmette-Guérin (BCG) perfusion therapy within the last 3 months; (16) severe side effects (symptoms of bladder irritation, etc.) occurred during the treatment of bladder perfusion and the patient was unable to tolerate them; (17) pregnant women, critically ill subjects, and other cases with contraindications, in case of serious cardiovascular disease, significant abnormal coagulation function, non-transitional epithelial tumor (such as adenocarcinoma, squamous cell carcinoma), acute cystitis, spinal deformity and patients cannot lie flat, urethral stricture, etc.; and 18 those who were considered by the researchers to compromise surgical efficacy and safety evaluation or have poor compliance.
This study aimed to explore the efficacy of transurethral needle electrode resection and transurethral holmium laser resection for Non-muscular invasive bladder cancer (NMIBC). The patients were prospectively included in this study and divided into the two groups by the types of surgery.
Surgical method
Transurethral needle electrode resection
The location, number, diameter, and base of the tumor in the bladder were observed by transurethral electrotomy after continuous epidural anesthesia and disinfection. Then, 5% (v/v) mannitol rinse solution was applied to adjust the output power of the electric cutting current to 120 W and the output power of the electric coagulation current to 80 W. The bladder was kept in a filling state, about 1 cm away from the base of the tumor, and the mucosa, submucosa, and deep muscle layer were excised cystoscopically with a needle electrode close to the bladder mucosa. A blunt needle electrode was used to push and peel the deep surface of the deep muscle layer, and the tumor tissues were lifted upward by the impact of water flow, and the tumor base was well exposed. Under the endoscope, tumor tissues and normal tissues could be clearly distinguished. Clockwise or counterclockwise electric cutting was performed along the tumor base until the whole tumor pedicle was completely removed. During the operation, coagulation and cutting were performed to effectively control bleeding and keep the visual field clear. If necessary, the fat in the outer layer of the bladder can be cut. Small tumors were sucked out directly by Elick, while larger tumors were hooked out by a ring-like electrotomy from the operating channel. One tri-lumen indwelling catheter was placed postoperatively, and the bladder was irrigated with normal saline.
Transurethral holmium laser resection
After continuous epidural anesthesia and disinfection, a cystoscope was placed through the urethra to observe the location, number, diameter, and base of the tumor in the bladder. A holmium laser fiber was inserted into the bladder through the cystoscope operating hole using normal saline for rinsing. The holmium laser fiber was placed close to the tumor body, and the tumor was cut about 1 cm from the tumor base. When the muscle layer was cut, the tumor tissue was lifted up with water flow. The small tumors were sucked out by Elick directly, while larger tumors were hooked out by a ring-like electrotomy from the operating channel. One tri-lumen indwelling catheter was placed postoperatively, and the bladder was irrigated with normal saline.
Data collection
Patient baseline information and clinical efficacy data were collected. The baseline information included age, gender, height, weight, body mass index (BMI), tumor size, tumor focality, tumor location, pathological classification, preoperative/postoperative tumor grade, and comorbid disease. The clinical efficacy data included operative time, intraoperative time, postoperative gross hematuria time, bladder irrigation time, postoperative hospitalization time, indwelling time, complications, secondary operation, tumor residual rate at the second operation, disease-free survival rate (1-year, 2-year, 3-year), progression-free survival rate (1-year, 2-year, 3-year), hepatocyte growth factor (HGF), tumor-specific growth factor (TSGF), and tumor necrosis factor alpha (TNF-α). In the follow-up period, B ultrasound and cystoscopy were performed to evaluate recurrence or progress.
Statistical analysis
Statistical analyses were completed using SPSS17.0. Data were reported as mean (standard deviation) or number (%). Outcomes were compared between two groups with two-sided t test for continuous variables and chi-square test for categorical variables. Survival data were analyzed by Kaplan-Meier method. All tests were two-sided, and P < 0.05 was considered to be statistically significant.
Results
Comparison of baseline characteristics in patients
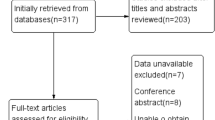
A total of 103 patients with NMIBC were included in the present study, 52 patients in the transurethral needle electrode resection group, and 51 patients in the transurethral holmium laser resection group (Fig. 1). The patients included 68 males and 35 females, with a mean age of 57.3 years. The pathological classification of NMIBC was as follows: 62 patients in Ta, 15 patients in T1, and 26 patients in Tis. The tumor size was 25.7 (12.6) mm in the transurethral needle electrode resection group, 25.7 (13.9) mm in the transurethral holmium laser resection group. Table 1 shows a comparison of baseline characteristics in patients between the two groups. No statistically significant differences were observed in baseline characteristics of the patients between the two groups (all P > 0.05).

Comparison of tumor recurrence in the follow-up time between the two groups (log-rank test: χ2 = 0.569, P = 0.451)
Figures 2, 3, and 4 presented the imaging examination of the bladder tumor on the right posterior wall; Fig. 5 is the histopathologic examination about papillary urothelial carcinoma; Fig. 6 is the histopathologic examination about infiltrating papillary urothelial carcinoma; Fig. 7 is the surgical process about transurethral holmium laser resection; and Fig. 8 is the surgical process about transurethral needle electrode resection.

Imaging examination

Imaging examination

Imaging examination

Histopathologic examination

Histopathologic examination

Surgical process

Surgical process
Comparison of clinical outcome variables in patients
A comparison was made of the perioperative indicators, complications, and secondary operation after resection between the groups (Table 2). In the transurethral holmium laser resection group, the operative time (28.8 ± 3.6 min vs. 31.5 ± 4.4 min), estimated intraoperative blood loss (27.0 ± 3.9 mL vs. 34.2 ± 6.2 mL), postoperative gross hematuria time (2.8 ± 1.5 days vs. 3.5 ± 1.1 days), bladder irrigation time (1.9 ± 0.5 days vs. 2.2 ± 0.4 days), and postoperative hospitalization time (6.2 ± 1.3 days vs. 6.7 ± 1.3 days) were all significantly decreased after resection when compared with the transurethral needle electrode resection group (P < 0.05 or P < 0.01). The incidence of obturator reflex was significantly lower in the transurethral holmium laser resection group (2.0%) than the transurethral needle electrode resection group (15.4%) (P < 0.05). There was no significant difference in indwelling time, urethral stricture, secondary operation, and tumor residual rate at the second operation between the two groups (all P > 0.05).
In the subgroup analysis by tumor size, there was a significant difference in operative time, estimated intraoperative blood loss, and bladder irrigation time between the two groups with tumor size < 3 cm; there was a significant difference in postoperative gross hematuria time between the two groups with tumor size ≥ 3 cm. In the subgroup analysis by tumor focality, there was a significant difference in operative time, estimated intraoperative blood loss, postoperative gross hematuria time, and bladder irrigation time between the two groups with unifocal tumor. In the subgroup analysis by tumor location, there was a significant difference in operative time, estimated intraoperative blood loss, postoperative gross hematuria time, bladder irrigation time, and postoperative hospitalization time between the two groups with lateral wall tumor; there was a significant difference in operative time, postoperative gross hematuria time, and bladder irrigation time between the two groups with posterior wall tumor. In the subgroup analysis by tumor stage, there was a significant difference in operative time, estimated intraoperative blood loss, and bladder irrigation time between the two groups with Ta tumor; there was a significant difference in estimated intraoperative blood loss between the two groups in T1 tumor; and there was a significant difference in estimated intraoperative blood loss and bladder irrigation time between the two groups in Tis tumor.
In the transurethral needle electrode resection group, the 1-, 2-, and 3-year disease-free survival rate was 78.8%, 71.4%, and 64.6%, respectively; the 1-, 2-, and 3-year progression-free survival rate was 73.1%, 61.2%, and 43.8%, respectively. In the transurethral holmium laser resection group, the 1-, 2-, and 3-year disease-free survival rate was 73.1%, 61.2%, and 43.8%, respectively; the 1-, 2-, and 3-year progression-free survival rate was 80.4%, 72.0%, and 54.3%, respectively. There was no significant difference in disease-free survival rate and progression-free survival rate between the two groups (Table 3).
There was no significant difference in the perioperative value of HGF, TSH, and TNF-α between the two groups (all P > 0.05, Table 4). After the resection, the transurethral holmium laser resection group had a significant decrease in the levels of HGF (10.89 ± 2.47 vs. 16.80 ± 1.45), TSH (2.4 ± 0.4 vs. 3.6 ± 0.3), and TNF-α (76.01 ± 4.82 vs. 99.14 ± 6.01 days) as compared to the transurethral needle electrode resection group (all P > 0.05, Table 4).
Discussion
Bladder tumors can be divided into two categories: stage Tis, Ta, and T1 non-muscle-infiltrating bladder tumors, and above T2 muscle-infiltrating bladder tumors. NMIBC, also known as superficial bladder tumors, is confined to the mucosa (Ta-Tis) and submucosa (T1) and accounts for about 80 ± 5%. Muscular invasive bladder tumors account for 20 ± 5%. The proportion of Ta, T1, and Tis lesions in NMIBC is about 70%, 20%, and 10%, respectively. According to different recurrence probabilities and prognosis risks, NMIBC can be divided into three levels: low risk, medium risk, and high risk. Risk factors for recurrence are the number of primary tumors, the university, the degree of infiltration and the recurrence probability (especially whether the recurrence time is within 3 months after the surgery), etc., while pathological grade and stage of tumors are associated with tumor progression [6,7,8,9,10].
Traditional TURBT has been widely used in clinical practice, but this method requires the removal of the tumor in sections and layers. During the operation, the tumor is morselized and removed. This method violates the principle of no tumor in traditional surgery and may lead to tumor cell dispersion and implantation, increasing the recurrence rate of bladder tumor after surgery. Secondly, this kind of operation inevitably destroys the tumor layer, and the specimen may miss the muscle layer, resulting in the inaccuracy of postoperative pathological staging, thus affecting subsequent treatment. In addition, some specific sites, such as tumors located near the lateral posterior wall of the bladder, are prone to obturator nerve reflex during surgery because the pelvic segment of the obturator nerve travels along the lateral wall of the pelvis and is close to the lateral posterior wall of the bladder [11,12,13,14,15,16].
Currently, the treatment options of NMIBC include surgical treatment, postoperative cystic-perfusion chemotherapy, and cystic-perfusion immunotherapy. The surgical treatment includes transurethral resection of bladder tumor, transurethral laser surgery, and photodynamic therapy. TURBT is the current “gold standard” for the treatment of NMIBC and also the main treatment [17,18,19]. The objectives of TURBT are as follows: first, complete removal of all tumors within the field of vision to achieve the effect of radical surgical resection; second, resection of tissues for evaluation of pathological grade and stage, determination of the next postoperative treatment plan of the patient, and assessment of prognosis and risk of recurrence. In 1966, lasers began to be used in urology. This technique has been widely used in clinical practice for its advantages of safety, simplicity, less damage, and definite curative effect. In recent years, holmium laser, green laser, and thulium laser have been developed and put into clinical use, showing a good clinical application prospect. Holmium laser was used to treat bladder tumors in the mid-1990s and has been widely used because of its good cutting and electrocoagulation, shallow tissue penetration, and low heat loss [20,21,22,23].
TURBT is the preferred surgical method for the treatment of NMIBC at present. It mainly relies on electrothermal effect to remove tumors. Due to the physical characteristics of electrotomy, this surgical method has some unavoidable defects. The TURBT circuit current can easily induce obturator nerve reflex during tumor resection of the lateral wall of the bladder. Strong obturator nerve reflex can cause complications such as bladder perforation. If the tumor location is unique, risks such as ureteral orifice stricture, urethral stricture, tumor residue, and disseminated implantation may occur after TURBT, as well as disadvantages such as easy burning of tumor specimens to form eschar and difficulty in accurate pathological staging [24,25,26,27].
Holmium laser is a pulsed solid-state laser, which generates strong heat in an instant and can be absorbed by superficial tissues efficiently. Its tissue penetration depth is 4 mm, and it has good vaporization cutting and coagulation hemostatic ability, which can precisely cut tumor tissues to effectively avoid bladder perforation. In addition, the holmium laser does not generate an electric field during surgery and can completely eliminate the obturator nerve reflex. It is suitable for patients with cardiac pacemaker and arrhythmia. It is worth noting that the temperature of the local tissue can be as high as 100 ~ 300 °C [28]. In contrast, the local tissue temperature during laser treatment of NMIBC is only 40 ~ 75 °C, and the thermal damage of the surrounding tissues is relatively small. Therefore, postoperative wound healing is fast and the indwelling catheter time is short.
In our study, the operative time, estimated intraoperative blood loss, postoperative gross hematuria time, bladder irrigation time, and postoperative hospitalization time were all significantly lower in the transurethral holmium laser resection group as compared to the transurethral needle electrode resection group. After resection, transurethral holmium laser resection significantly decreased the value HGF, TSH, and TNF-α as compared to transurethral needle electrode resection. The incidence of obturator reflex was significantly lower in the transurethral holmium laser resection group than the transurethral needle electrode resection group.
Conclusion
In the treatment of NMIBC, holmium laser resection has the advantages of fewer complications, better safety, faster postoperative recovery, and lower recurrence rate versus traditional transurethral needle electrode resection. The limitations of this study include the small number of cases and lack of randomized controlled study with TURBT, so it is still necessary to carry out a large-scale randomized controlled clinical study with long-term follow-up to verify its long-term therapeutic effect.
Availability of data and materials
The datasets during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CIS:
-
Carcinoma in situ
- HGF:
-
Hepatocyte growth factor
- NMIBC:
-
Non-muscular invasive bladder cancer
- RC:
-
Radical cystectomy
- TNF-α:
-
Tumor necrosis factor alpha
- TSGF:
-
Tumor-specific growth factor
- RC:
-
Radical cystectomy
- ECOG:
-
Eastern Cooperative Oncology Group
- PS:
-
Performance status
- CT:
-
Computed tomography
- AST:
-
Aspartate aminotransferase
- ALT:
-
Alanine aminotransferase
- TURBT:
-
Transurethral resection of bladder tumor
- BCG:
-
Bacille Calmette-Guérin
- BMI:
-
Body mass index
References
Antoni S, Ferlay J, Soerjomataram I, Znaor A, Jemal A, Bray F. Bladder cancer incidence and mortality: a global overview and recent trends. Eur Urol. 2017;71(1):96–108.
Chavan S, Bray F, Lortet-Tieulent J, Goodman M, Jemal A. International variations in bladder cancer incidence and mortality. Eur Urol. 2014;66(1):59–73.
Dy GW, Gore JL, Forouzanfar MH, Naghavi M, Fitzmaurice C. Global burden of urologic cancers, 1990-2013. Eur Urol. 2017;71(3):437–46.
Aron M. Variant histology in bladder cancer-current understanding of pathologic subtypes. Current urology reports. 2019;20(12):80.
Gurram S, Muthigi A, Egan J, Stamatakis L. Imaging in localized bladder cancer: can current diagnostic modalities provide accurate local tumor staging? Current urology reports. 2019;20(12):82.
Bladder Cancer Treatment (PDQ(R)): Patient Version. In: PDQ Cancer Information Summaries. edn. Bethesda (MD); 2002.
Richters A, Aben KKH, Kiemeney L. The global burden of urinary bladder cancer: an update. World J Urol. 2019.
Veskimae E, Espinos EL, Bruins HM, Yuan Y, Sylvester R, Kamat AM, Shariat SF, Witjes JA, Comperat EM. What is the prognostic and clinical importance of urothelial and nonurothelial histological variants of bladder cancer in predicting oncological outcomes in patients with muscle-invasive and metastatic bladder cancer? A European association of urology muscle invasive and metastatic bladder cancer guidelines panel systematic review. European urology oncology. 2019;2(6):625–42.
Taylor J, Becher E, Steinberg GD. Update on the guideline of guidelines: non-muscle-invasive bladder cancer. BJU Int. 2019.
Babjuk M, Burger M, Comperat EM, Gontero P, Mostafid AH, Palou J, van Rhijn BWG, Roupret M, Shariat SF, Sylvester R, et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ) - 2019 Update. Eur Urol. 2019;76(5):639–57.
Timo K. Nykopp, Jose Batista da Costa, Miles Mannas, Peter C Black: Current clinical trials in non-muscle invasive bladder cancer. Curr Urol Rep. 2018;19(12):101.
Baumeister P, Zamboni S, Mattei A, et al. Histological variants in non-muscle invasive bladder cancer. Transl Androl Urol. 2019;8(1):34–8.
Akand M, Muilwijk T, Raskin Y, et al. Quality control indicators for transurethral resection of non-muscle-invasive bladder cancer. Clin Genitourin Cancer. 2019;17(4):e784–92.
Onishi T, Sugino Y, Shibahara T, et al. Randomized controlled study of the efficacy and safety of continuous saline bladder irrigation after transurethral resection for the treatment of non-muscle-invasive bladder cancer. BJU Int. 2017;119(2):276–82.
Hayashida Y, Miyata Y, Matsuo T, et al. A pilot study to assess the safety and usefulness of combined transurethral endoscopic mucosal resection and en-bloc resection for non-muscle invasive bladder cancer. BMC Urol. 2019;19(1):56.
Onishi T, Sekito S, Shibahara T, et al. The role of continuous saline bladder irrigation after transurethral resection in patients with high-grade non-muscle-invasive bladder cancer. Scand J Urol. 2018;52(5-6):385–8.
Ghandour R, Singla N, Lotan Y. Treatment options and outcomes in nonmetastatic muscle invasive bladder cancer. Trends in cancer. 2019;5(7):426–39.
Soria F, Marra G, D'Andrea D, Gontero P, Shariat SF. The rational and benefits of the second look transurethral resection of the bladder for T1 high grade bladder cancer. Translational andrology and urology. 2019;8(1):46–53.
Dobruch J, Borowka A, Herr HW. Clinical value of transurethral second resection of bladder tumor: systematic review. Urology. 2014;84(4):881–5.
Gendy R, Delprado W, Brenner P, Brooks A, Coombes G, Cozzi P, Nash P, Patel MI. Repeat transurethral resection for non-muscle-invasive bladder cancer: a contemporary series. BJU Int. 2016;117(Suppl 4):54–9.
Babjuk M, Bohle A, Burger M, Capoun O, Cohen D, Comperat EM, Hernandez V, Kaasinen E, Palou J, Roupret M, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: Update 2016. Eur Urol. 2017;71(3):447–61.
Wigmore GJ, Anstey JR, St John A, Greaney J, Morales-Codina M, Presneill JJ, Deane AM, MacIsaac CM, Bailey M, Tatoulis J, et al. 20% human albumin solution fluid bolus administration therapy in patients after cardiac surgery (the HAS FLAIR study). J Cardiothorac Vasc Anesth. 2019;33(11):2920–7.
Rolevich AI. Evmenenko AA: [A systematic review and meta-analysis to assess the recurrence-free survival in non-muscle invasive bladder cancer after transurethral resection guided by 5-aminolevulinic acid-induced photodynamic diagnosis compared with white-light transurethral resect]. Urologiia. 2016;4:137–46.
Balci M, Tuncel A, Keten T, et al. Comparison of monopolar and bipolar transurethral resection of non-muscle invasive bladder cancer. Urol Int. 2018;100(1):100–4.
Gordon PC, Thomas F, Noon AP, et al. Long-term outcomes from re-resection for high-risk non-muscle-invasive bladder cancer: a potential to rationalize use. Eur Urol Focus. 2019;5(4):650–7.
Li C, Liang G, Zhang J, et al. The effect of holmium laser resection versus standard transurethral resection on non-muscle-invasive bladder cancer: a systematic review and meta-analysis. Lasers Med Sci. 2020;31.
Zapała P, Dybowski B, Poletajew S, et al. Clinical rationale and safety of restaging transurethral resection in indication-stratified patients with high-risk non-muscle-invasive bladder cancer. World J Surg Oncol. 2018;16(1):6.
Muta M. Issa: Technological advances in transurethral resection of the prostate: bipolar versus monopolar TURP. J Endourol. 2008;22(8):1587–95.
Acknowledgements
None.
Funding
This study was performed without funding.
Author information
Authors and Affiliations
Contributions
YZ, ZLZ, and HYM contributed to the study conception and design. YZ, ZLZ, and MHL contributed to data collection and analysis. YZ and ZLZ contributed to the literature review and drafting of the manuscript. HYM contributed to the critical review and approval of the final manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This was a prospective study involving human subjects treated according to the standard clinical practice. All permissions granted by competent Ethics Committees and other authorities were obtained, and all informed consents required by the existing law and regulations were collected.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhou, Y., Zhang, ZL., Luo, MH. et al. Transurethral needle electrode resection and transurethral holmium laser resection of bladder cancer. World J Surg Onc 18, 166 (2020). https://doi.org/10.1186/s12957-020-01943-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-020-01943-3