
Abstract
Background
Desmoid tumors, which are associated with familial adenomatous polyposis (FAP), tend to occur frequently in the abdominal wall and mesentery. Currently, there are no recognized treatments other than surgery, and frequent surgeries result in gastrointestinal obstructions and functional gastrointestinal disorders.
Case presentation
After surgery that was performed on a 39-year-old patient with FAP, we performed a second tumor excision which was the procedure used for frequently occurring mesenteric desmoid tumors. It was determined that the enlarged tumor would be difficult to operate on through an abdominal incision. Subsequently, the carbon ion radiotherapy of 50 Gy was then performed on the patient. Three years later, the tumor still remains reduced in size. In addition, we have not observed any negative effect on the digestive tract.
Conclusions
This is the first instance that the carbon ion radiotherapy has been effective for the unresected desmoid tumor, and it is believed that this will become the one effective option for the treatment of desmoid tumors.
Similar content being viewed by others


Background
Desmoid tumors associated with familial adenomatous polyposis (FAP) are classified as benign, but clinically considered to be a disease similar to malignancies because of their tendency to occur as multiple lesions in the abdominal wall or mesentery. Surgical therapy is the first choice of treatment, but repeated procedures for recurrent tumors may cause gastrointestinal stenosis or dysfunction. Although hormone therapy and chemotherapy for desmoid tumors have been described in the literature, no established treatment is available other than surgical resection. We report a case of inoperable growing desmoid tumor in the abdominal wall that shrank in response to heavy ion radiotherapy and has remained stable and free of effects on the adjacent intestinal tract for 3 years. No cases like this have been reported anywhere in the world. We believe that heavy-ion radiotherapy has the potential to become an effective treatment option for patients with desmoid tumors.
Case presentation
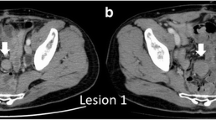
The patient was a 49-year-old man diagnosed with familial adenomatous polyposis (FAP) caused by a defect in the adenomatous polyposis coli (APC) gene. In March 1998 (aged 36), he underwent total proctocolectomy and ileostomy for polyps involving the entire colon, and the stoma was closed 9 months later. Pathological findings showed that the polyps were adenomas. In August 2001 (aged 39) and August 2003 (aged 41), multiple mesenteric tumors were removed, which were pathologically diagnosed as desmoid tumors characterized by invasive growth of fibroblasts into the surrounding muscle layer. He subsequently experienced repeated episodes of ileus symptoms attributable to intestinal adhesion as a postoperative complication and to recurrent mesenteric desmoid tumors; thus, duodenojejunostomy was performed in March 2011 (aged 49). Around December 2011, 9 months after the operation, a desmoid tumor of the abdominal wall was found immediately above the peritoneum just below the previous operative wound, which grew to 7.3 cm in the longest diameter in 3 months (Fig. 1a). It was considered surgically unresectable partly because tumor adhesion to the intestinal tract and peritoneum was severe and partly because tumor removal would have resulted in a large defect in the abdominal wall. Among the available treatment options for desmoid tumor of the abdominal wall, chemotherapy, carbon ion radiotherapy, etc. were proposed. After a thorough discussion about informed consent, the patient selected carbon ion radiotherapy, which is a type of radiotherapy that can deliver high-dose radiation to a tumor while minimizing the dose delivered to the organs at risk. From May to July 2012, he received carbon ion beam irradiation at a total dose of 50 Gy (relative biological effectiveness [RBE])Footnote 1 in 25 fractions at the Hyogo Ion Beam Medical Center (HIBMC). Figure 1b shows the carbon ion treatment plan for this patient. The solid abdominal wall tumor continued to grow until 2 months after treatment, reaching 12 cm in diameter, and then gradually shrank to 7.8 cm at 5 months. One year after treatment, the contents of the tumor had liquefied, and the tumor had shrunk to 4.3 cm in diameter. The liquid components consisted primarily of fibrin, with no malignant cells. Currently, 3 years after the operation, the abdominal wall tumor remains stable, with a diameter of 3.3 cm, and is being followed up (Fig. 1c).

Abdominal computed tomography (CT) scan. CT scan revealed the desmoid tumor in abdominal wall (solid white arrow in a and c). a Pretreatment phase, b Carbon ion treatment plan and c 3 years after ion radiotherapy were shown
Discussion
Desmoid tumor is a rare with 2.4~4.3 cases occurring per one million individuals each year [1]. It has been correlated with the FAP [2], and the overall incidence of desmoid tumor in patients with FAP is 10–20 %, which equates to relative risk of 852 compared to the general population [3]. Desmoid tumor is a benign fibromatosis that originate from fascia and muscular aponeuroses, with an infiltrating growth pattern. As indicated by its name, aggressive fibromatosis, a desmoid tumor is characterized by a clinically malignant course, with a reported recurrence rate up to 45 % after surgical resection [4].
Treatment of desmoid tumor is a complex condition with many recognized treatments including active observation, hormonal therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), chemotherapy, radiotherapy, and surgical resection [5]. As desmoid tumors sometimes exhibit characteristics of stable or regress, the conservative approach is recommended [6]. In this case, the tumor grew more than 7 cm in just 3 months and the patient complained the tumor pain, so it was necessary to provide the aggressive treatments. Radiotherapy has been adopted as a primary treatment in patients who undergo progression during observation. Mounting literature supports this approach, with several groups reporting long term local control in 70–93 % of patients at doses of 50–60 Gy (1.8–2 Gy/fraction) [7, 8]. It is also reported that the radiotherapy combined with surgical resection results in better progression-free survival time (PFS) than surgery alone [9]. But simultaneously, radiotherapy has a risk to cause damage to the neighboring intestine and organ such as perforation or abscess formation, and potential late radiation effects, including second malignancies [10]. It was reported a partial response of hormone therapy (tamoxifen) for desmoid tumor in male patients, 24~54 months after treatment initiation as well as female patients [11]. And, there is some evidence that the treatments are most effective when NSAIDs and hormonal therapies are given together [12]. Various chemotherapy regimes were reported and most of them were used as combination, included methotrexate with vinblastine or vinorelbine, doxorubicin with dacarbazine, doxorubicin with cyclophosphamide and vincristine, and actinomycin-D-based chemotherapy. The average response rate of them was 50 % (range 17~100 %) [13]. Although hormonal therapies, nonsteroidal anti-inflammatory drugs (NSAIDs), interferon, or chemotherapy are options for unresectable or recurrent disease, the appropriate therapeutic approach has not yet been fully elucidated [14].
Carbon ion radiotherapy can precisely irradiate the target lesion, thereby reducing its adverse effects on the adjacent intestinal tracts. Photon beam sensitivity varies with the type of tumor, whereas carbon ion radiotherapy, which uses carbon (C) molecules, can be expected to have potent effects on all types of tumor, irrespective of sensitivity [15]. The finding that carbon ion radiotherapy was effective for recurrent desmoid tumor of the abdominal wall in this patient will lead to an increase in treatment options and thus have important implications for patients suffering from this disease and for the physicians treating them. In addition, this is the first report of a case of desmoid tumor successfully treated with carbon ion radiotherapy. We hope that our report will be of some help in determining the treatment strategy for this disease.
Conclusions
This report presents a first case that the carbon ion radiotherapy has been effective for the unresected desmoid tumor.
Notes
The carbon ion beam dose is reported in Gy (RBE), which is defined as the physical dose multiplied by the RBE of the protons or carbon ions. For example, 2 Gy (RBE) of carbon ion radiotherapy is biologically equivalent to 2 Gy of photon radiotherapy. Biological effects of carbon ion radiotherapy at HIBMC have been evaluated in vitro and in vivo, and the RBE values for carbon ion irradiation were determined to be 2–3.7 (depending on the depth in the spread-out Bragg peaks) [16].
Abbreviations
- APC:
-
adenomatous polyposis coli
- cm:
-
centimeter
- CT:
-
Computed tomography
- FAP:
-
Familial adenomatous polyposis
- Gy:
-
Gray
- NSAIDs:
-
Nonsteroidal anti-inflammatory drugs
References
Reitamo JJ, Hayry P, Nykyri E, Saxen E. The desmoid tumor. I. Incidence, sex-, age- and anatomical distribution in the Finnish population. Am J Clin Pathol. 1982;77(6):665–73.
Soravia C, Berk T, McLeod RS, Cohen Z. Desmoid disease in patients with familial adenomatous polyposis. Dis Colon Rectum. 2000;43(3):363–9.
Seow-Choen F. The management of desmoids in patients with familial adenomatous polyposis (FAP). Acta Chir Iugosl. 2008;55(3):83–7.
Nuyttens JJ, Rust PF, Thomas Jr CR, Turrisi III AT. Surgery versus radiation therapy for patients with aggressive fibromatosis or desmoid tumors: a comparative review of 22 articles. Cancer. 2000;88(7):1517–23.
Eastley N, McCulloch T, Esler C, Hennig I, Fairbairn J, Gronchi A, Ashford R. Extra-abdominal desmoid fibromatosis: a review of management, current guidance and unanswered questions. Eur J Surg Oncol. 2016. doi:10.1016/j.ejso.2016.02.012.
Bonvalot S, Desai A, Coppola S, Pechoux CL, Terrer P, Domont J, Cense L. The treatment of desmoid tumors: a stepwise clinical approach. Ann Oncol. 2012. doi:10.1093/annonc/mds298.
Spear MA, Jennings LC, Mankin HJ, Spiro IJ, Springfields DS, Gebhardt MC, Rosenberg AE, Efird JT, Suit HD. Individualizing management of aggressive fibromatoses. Int J Radiat Oncol Biol Phys. 1998;40(3):637–45.
Ballo MT, Zagars GK, Pollack A. Radiation therapy in the management of desmoid tumors. Int J Radiat Oncol Biol Phys. 1998;42(5):1007–14.
Baumert BG, Spahr MO, Hochsteller AV, Beauvois S, Landmann C, Fridrich K, Villa S, Kirschner MJ, Storme G, Thum P, Streuli HK, Lombriser NL, Maurer R, Ries G, Bleher EA, Willi A, Allemann J, Buehler U, Blessing H, Luetolf UM, Davis JB, Seifert B, Infanger M. The impact of radiotherapy in the treatment of desmoid tumours. An international survey of 110 patients. A study of the Rare Cancer Network. Radiat Oncol. 2007; doi: 10.1186/1748-717X-2-12.
Ray ME, Lawrence TS. Radiation therapy for aggressive fibromatosis (desmoid tumor). J Clin Oncol. 2006;24(22):3714–5.
Izes JK, Zinman LN, Larsen CR. Regression of large pelvic desmoid tumor by tamoxifen and sulindac. Urology. 1996;47(5):756–9.
Hansmann A, Adolph C, Vogel T, Unger A, Moeslein G. High-dose tamoxifen and sulindac as first-line treatment for desmoid tumors. Cancer. 2004;100(3):612–20.
Janinis J, Patriki M, Vini L, Aravantinos G, Whelan JS. The pharmacological treatment of aggressive fibromatosis: a systematic review. Ann Oncol. 2003;14(2):181–90.
Fiore M, Rimareix F, Mariani L, Domont J, Collini P, Le Pechoux C, Casalli PG, Le Cesne A, Gronchi A, Bonvalot S. Desmoid-type fibromatosis: a front-line conservative approach to select patients for surgical treatment. Ann Surg Oncol. 2009;16(9):2587–93.
Kamada T, Tsujii H, Blakely EA, Debus J, De Neve W, Durante M, Jakel O, Mayer R, Oreccia R, Potter R, Vatnitsky S, Chu WT. Carbon ion radiotherapy in Japan: an assessment of 20 years of clinical experience. Lancet Oncol. 2015;16(2):e93–e100. doi:10.1016/S1470-2045(14)70412-7.
Kagawa K, Murakami M, Hishikawa Y, Abe M, Akagi T, Yanou T, Kagiya G, Furusawa Y, Ando K, Nojima K, Aoki M, Kanai T. Preclinical biological assessment of proton and carbon ion beams at Hyogo Ion Beam Medical Center. Int J Radiat Oncol Biol Phys. 2002;54(3):928–38.
Acknowledgements
We would like to acknowledge Dr. Kazuhiro Tsukada who passed away on the 5 March 2016. Dr. Tsukada provided us with many helpful suggestions for this work.
Funding
Authors received the funding in partially from JSPS KAKENHI (15 K10181) for writing of this manuscript.
Availability of data and materials
Not applicable.
Authors’ contributions
TN, TO, SS, and YS performed several operations for this desmoid tumor. YD, NH, NF, and TO planned and performed the carbon ion radiotherapy for this case. TN and YD were involved in drafting the manuscript. TO and NH reviewed the literature. SS and NF provided the figures. YS revised the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that have no competing interests.
Consent for publication
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Ethics approval and consent to participate
The ethics committee of Toyama university hospital approved the study (24–4).
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article is available at http://dx.doi.org/10.1186/s12957-017-1154-z.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Nagata, T., Demizu, Y., Okumura, T. et al. Carbon ion radiotherapy for desmoid tumor of the abdominal wall: a case report. World J Surg Onc 14, 245 (2016). https://doi.org/10.1186/s12957-016-1000-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-016-1000-8