
Abstract
Background
Though breast cancer is the most common cancer among women in Kerala, India, epidemiological data on breast cancer in the state is largely lacking. The objectives of this study were to analyze the survival pattern of female breast carcinoma in this region of the country and to compare the differences in survival with different hormone-receptor expressions.
Methods
One hundred eighty-nine female breast cancer patients who were operated between 1 August 2008 and 3 July 2009 were followed up over telephone to obtain data on five-year survival. Grade, stage of the disease, and hormone-receptor (HR) status were obtained from treatment records. Logistic regression and the Kaplan-Meier survival analysis were used for statistical analysis.
Results
The mean age of the study population was 49.07 (SD, 10.35) years. A majority of the patients had estrogen receptor (ER)+/progesterone receptor (PR) + tumors (n = 103, 54.5%), followed by 72 (38.1%) ER−/PR−, 10 (5.3%) ER−/PR+, and 4 (2.1%) ER+/PR−. Stage of the disease, axillary nodal status, and hormone-receptor status showed statistically significant association with overall survival in breast cancer. Overall survival rate at the end of 5 years was 71.4%. Mortality was found to be highest for the ER − PR − group (47.2%).
Conclusions
Women in Kerala are diagnosed with breast carcinoma at a relatively younger age, yet the overall five-year survival for the disease is low when compared to developed nations. It is imperative that comprehensive breast cancer screening and treatment strategies be developed to enable earlier diagnosis and improve the survival of breast cancer in the state.
Similar content being viewed by others

Background
Breast cancer is the most common cancer among women in many regions of India [1-3]. It is highly heterogeneous, with a wide range of biological, pathological, and clinical characteristics [4]. Among these, hormone receptors (estrogen receptor (ER), progesterone receptor (PR)) greatly influence clinical outcome, and their role as a prognostic and therapeutic tool is widely accepted [5,6]. Though the incidence of breast cancer in Kerala has been steadily mounting, data on epidemiology and survival of breast cancer in the state is scarce.
The objectives of this study were to analyze the survival pattern of female breast carcinoma in this region of the country and to compare the differences in survival with different hormone-receptor expressions.
Methods
A retrospective cohort study was conducted on 189 female patients who were diagnosed with invasive ductal carcinoma and had undergone surgery between 1 August 2008 and 31 July 2009 in the Department of General Surgery, Government Medical College, Thrissur. The required information was collected from the treatment records of the patients maintained at the Medical Records Library. All data including age, menopausal status, and pathological characteristics [grade (modified Bloom-Richardson grade), stage of the disease (AJCC), tumor size, and axillary nodal status] were recorded. Patients whose hormone-receptor status was not analyzed were excluded from the study. Patients who had either ER or PR positive tumors were treated with hormonal therapy. Overall survival was calculated in months, either from the date of diagnosis or from the date of surgery up to 31 December, 2013. Five-year survival at the end of the study period was obtained from follow-up records for those who were on regular follow-up and was confirmed by contacting the patients or their relatives over telephone. Those who had been lost to follow-up were also traced over telephone.
All post-mastectomy specimens were evaluated for hormone-receptor expression (ER and PR) by immunohistochemistry. In accordance with the American Society of Clinical Oncology (ASCO) guidelines [7], which were being followed when the assays were done, specimens in which more than 10% of the tumor-nuclei stained positive were reported hormone-receptor positive. ER status was determined using the BioGenex monoclonal mouse IgG (Clone 1D5) (BioGenex, USA), and PR status was determined using BioGenex monoclonal mouse IgG (Clone 1A6) (BioGenex, USA). Antigen retrieval was done using the BioGenex EZ-Retriever system (BioGenex, USA). Based on hormone-receptor expression, patients were grouped into four categories, that is, ER + PR+ (ER positive PR positive), ER + PR−(ER positive PR negative), ER − PR+ (ER negative PR positive), and ER − PR−(ER negative PR negative).
Pathologic variables were compared using chi-square test. Logistic regression analysis was carried out to assess the independent association between different variables and survival. The Kaplan-Meier method was used to estimate the overall survival.
Results
One hundred eighty-nine female patients with invasive ductal breast cancer were included in the study. The age of the patients ranged from 27 to 80 with a median of 49.07 ± 10 years. ER expression was seen in 107 patents (56.6%) and PR expression in 113 patients (59.8%).
General characteristics
The general characteristics of the study group are shown in Table 1. Out of the 189 patients, 111 (58.7%) were pre-menopausal. One hundred twenty-seven patients (67.2%) were between 41 and 60 years of age. Distribution of patients according to their age and hormone-receptor expression is shown in Table 2. A majority (n = 127, 67.2%) had stage 2 breast cancer at presentation. One hundred four patients (55%) had grade 2 tumor, and 120 (63.2%) had tumor size between 2 and 5 cm.
Hormone-receptor expression and outcome
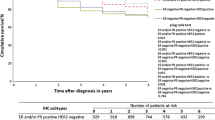
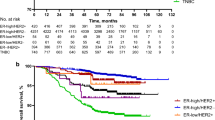
In this breast cancer cohort, 103 patients (54.5%) were ER + PR+, 72 patients (38.1%) were ER − PR−, 10 patients (5.3%) were ER − PR+, and 4 patients (2.1%) ER + PR−. Mean follow-up time was 52 months. 71.4% of the patients (n = 135) were found to have survived to five years from the time of diagnosis. Mortality was found to be highest for the ER − PR − group (n = 38, 47.2%). Data regarding the four types of hormone-receptor expression and the outcomes of patents that belonged to each group is shown in Figure 1. Among the different age groups, patients aged 50 years or younger were found to have a higher mortality (Table 2). The Kaplan-Meier survival curve was plotted for the different types of hormone-receptor expression and for overall survival (Figures 2 and 3).

Pattern of hormone-receptor expression and survival.

Kaplan-Meier Curve for overall survival.

Kaplan-Meier Curve for survival for different hormone-receptor expression.
Tables 3 and 4 show the association between different variables and survival in breast cancer. Stage of the disease (adjusted risk ratio (RR) 1.274), nodal status (adjusted RR 1.055), and hormone-receptor status (adjusted RR 2.859) showed statistically significant association with overall survival.
Discussion
Breast cancer is the most common cancer among urban women and second most common among rural women in India [1]. Breast cancer is a heterogeneous disease that can be classified into several subtypes on the basis of various clinical and pathological features [8]. Hormone-receptor (ER and PR) status is now routinely determined for all patients to assess the possibility of providing them specific adjuvant hormone therapy [6].
The median age of the study group was 49.07 ± 10.35 years, which is very low compared to the USA, where the median age at diagnosis of breast cancer is 61 years [9-11]. This considerable difference can likely be due to the genetic, racial, and socioeconomic differences between the two populations.
Data from the study showed that 56.6% patients were ER+ and 54.5% patients were ER + PR+. This is low when compared to data from the USA, where the overall ER positivity is reported to be 77% [10]. The findings are consistent with earlier studies from India [12-15]. We also have a higher proportion of ER − PR − tumors compared to the West. It has been noted that ER and PR expression in the study subjects increase with age. This is in concordance with earlier studies [16,17]. A greater number of ER − PR − tumors were seen in patients younger than 50 years of age.
Population-based studies on breast cancer in Bangalore [18] and Chennai [19] showed five-year survival rates of 42.3% and 48%, respectively. The five-year survival rate of the current study cohort was much higher, at 71.43%. The differences in the survival rate can be explained by differences in the study settings. The USA has an average five-year survival rate of 89.2% for patients diagnosed with breast cancer [10]. The overall survival rate is still low compared to the West. Five-year survival rates of more than 80% have been reported in many studies from the West and also from a developed Asian country [20,21]. Ethnicity and race have been documented as important factors that influence the survival rate [22]. Along with these factors, well-established screening programs and early detection of the disease also help improve the survival rate.
ER + PR+ breast cancer has been independently associated with decreased breast cancer mortality in many studies [4,19,23,24]. A similar survival pattern was also noted in the current cohort, with highest mortality in the ER − PR − group.
Stage of the disease, axillary nodal status, and hormone-receptor status showed statistically significant association with overall survival in breast cancer. Among these, the axillary nodal status and stage of the disease are established prognostic factors for carcinoma breast [5,16]. Along with their proven role in determining therapeutic course, hormone receptors (ER and PR) can also be used as a predictive tool for breast cancer survival.
ER − PR+ is a rare subtype of breast cancer based on hormone-receptor expression that accounts for 1% to 4% of all cases reported in literature [25]. The study cohort has a similar fraction of patients (5.3%) with ER − PR+ expression, and 90% survival has been noted in this particular group. The predictive value of PR in the absence of ER expression is controversial [26,27]. Some reports suggest that positive PR in the absence of ER has a higher response to hormone therapy, but this finding is not universal [28-30]. Unfortunately, because of the relatively small number of patients in the study group who belonged to this subset, it is difficult to comment on the role of this particular type of receptor expression on disease outcome.
Conclusions
The overall five-year survival rate of breast cancer patients in Kerala is low compared to developed nations. The lack of an effective cancer screening program is an important reason for this. The higher proportion of hormone-receptor (HR)-negative tumors in our population may be due to delayed diagnosis along with other genetic, ethnic, and cultural variations. Since data on epidemiology and risk factors of the breast cancer in the state is inadequate, it is very crucial to further explore these aspects of the disease to develop a prevention and control strategy to improve the survival rate.
Abbreviations
- HR status:
-
Hormone-receptor status
- ER:
-
Estrogen receptor
- PR:
-
Progesterone receptor
- RR:
-
Risk ratio
- ASCO:
-
American Society of Clinical Oncology
- AJCC:
-
American Joint Committee on Cancer
References
Programme NCR. Consolidated Report of the Population based cancer registries 1990–1996. New Delhi: Indian Council of Medical Research; 2001.
Population based cancer registry, Biennial report, 2000 and 2001, 2002, Department of Epidemiology and Bio-Statistics, Kidwai Memorial Institute of Oncology, Bangalore, India, 2004 and 2005.
National Cancer Registry Programme. Ten year consolidated report of the hospital based cancer registries 1984–1993. In: An assessment of the burden and care of cancer patients. New Delhi: Indian Council of Medical Research; 2001.
Di CS, Baselga J. Management of breast cancer with targeted agents: importance of heterogenecity. Nat Rev Clin Oncol. 2010;7:139–47.
Fitzgibbons PL, Page DL, Weaver D, Thor AD, Craig Allred D, Clark GM, et al. Prognostic factors in breast cancer: College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med. 2000;124:966–78.
Rastelli F, Crispino S. Factors predictive of response to hormone therapy in breast cancer. Tumori. 2008;94:370–83.
Hammond MEH, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, et al. ASCO-CAP guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol. 2010;28:2784–95.
Blows FM, Driver KE, Schmidt MK, Broeks A, van Leewen FE, et al. Subtyping of breast cancer by immunohistochemistry to investigate a relationship between subtype and short and long term survival: a collaborative analysis of data for 10,159 cases from 12 studies. PlosMed. 2010;7(5):e 1000279.
Rhodes A, Jasani B, Balaton AJ, Barnes DM, Miller KD. Frequency of estrogen and progesterone receptor positivity by immunohistochemical analysis in 7016 breast carcinomas: correlation with patient age, assay sensitivity, threshold value, and mammographic screening. Clin Pathol. 2000;53:688–96.
SEER-Stat database [http://seer.cancer.gov/statfacts/html/breast.html]
Leong SPL, Shen ZZ, Liu TJ, Agarwal G, Tajima T, Paik N, et al. Is breast cancer the same disease in Asian and western countries? World J Surg. 2010;34:2308–24.
Rashmi K, Jaishree S, Satinder SM, Kavita M. Hormone receptor status of breast cancer in the Himalayan region of Northern India. Indian J Surg Oncol. 2011;73(1):9–12.
Dey S, Boffetta P, Mathews A, Brennan P, Soliman A, Mathew A. Risk factors according to estrogen receptor status of breast cancer patients in Trivandrum South India. Int J Cancer. 2009;125(7):1663–70.
Shet T, Agrawal A, Nadkarni M, Palkar M, Havaldar R, Parmar V, et al. Hormone receptors over the last 8 years in a cancer referral centre in India:what was and what is? Indian J Pathol Microbiol. 2009;52(2):171–4.
Manjunath S, Jyothi SP, Rohini K, Marjorie C, Sridhar TS. Estrogen receptor negative breast cancer in India: do we really have higher burden of this subtype? Indian J Surg Oncol. 2011;2(2):122–5.
Dunnwald LK, Rossing MA, Li CI. Hormone receptor status, tumor characteristics, and prognosis: a prospective cohort of breast cancer patients. Breast Cancer Res. 2007;9:R6.
Azizun-Nisa Bhurgri Y, Raza F, Kayani N. Comparison of ER, PR and HER-2/neu (C-erb B 2) reactivity pattern with histologic grade, tumor size and lymph node status in breast cancer. Asian Pac J Cancer Prev. 2008;9:553–6.
Murthy NS, Agarwal UK, Chaudhry K, Saxena S. A study on time trends in incidence of breast cancer-Indian scenario. Eur J Cancer Care. 2007;16:185–6.
Gajalakshmi CK, Shanta V, Swaminathan R, Sankaranarayanan R, Black RJ. A population-based survival study on female breast cancer in Madras India. Br J Cancer. 1997;75:771–5.
Berrino F, De Angelis R, Sant M, Rosso S, Bielska-Lasota M, Coebergh JW, et al. Survival for eight major cancers and all cancers combined for Europian adults diagonosed in1995-99: results of the EUROCARE-4 study. Lancet Oncol. 2007;8:773–83.
Tsukuma H, Ajiki W, Ioka A, Oshima A. Research Group of Population-Based Cancer Registries of Japan. Survival of cancer patients diagnosed in 1993–1996: collaborative study of population-based cancer registries in Japan. Jpn J Clin Oncol. 2006;36:602–7.
Joslyn SA, West MM. Racial differences in breast carcinoma survival. Cancer. 2000;88:114–23.
Anderson WF, Chu KC, Chatterjee N, Brawely O, Brinton LA. Tumor variants by hormone receptor expression in white patients with node negative breast cancer from the surveillance, epidemiology, and end result data base. J Clin Oncol. 2001;19:18–27.
Pichon MF, Broet P, Magdelenat H, Delarue JC, Spyratos F, Basuyau JP, et al. Prognostic value of steroid receptors after long term follow up of 2257 operable breast cancers. Br J Cancer. 1996;73:1545–51.
Navani S, Bhaduri AS. High incidence of estrogen receptor negative progesterone receptor positive phenotypes in breast cancer: fact or fiction? Indian J Pathol Microbiol. 2005;48(2):199–201.
Rhodes A, Jasani B. The oestrogen receptor-negative/progesterone receptor-positive breast tumour: a biological entity or a technical artefact? J Clin Pathol. 2009;62:95–6.
De Maeyer L, Van Limbergen E, De Nys K, Moerman P, Pochet N, Hendrickx W, et al. Does estrogen receptor negative/progesterone receptor positive breast carcinoma exist? J Clin Oncol. 2008;26:335–6.
Bardou VJ, Arpino G, Elledge RM, Osborne CK, Clark GM. Progesterone receptor status significantly improves outcome prediction over estrogen receptor alone for adjuvant endocrine therapy in two large breast cancer data bases. J Clin Oncol. 2003;21:1973–9.
Early Breast Cancer Trialists’ Collaborative Group. Tamoxifen for early breast cancer: an overview of the randomized trials. Lancet. 1998;35:1451–67.
Olivotto IA, Truong PT, Speers CH, Bernstein V, Allan SJ, Kelly SJ, et al. Time to stop progesterone receptor testing in breast cancer management. J Clin Oncol. 2004;22:1769–70.
Acknowledgements
The State Board of Medical Research, Kerala, India provided funds and support. Dr. Jayadev V K, assistant professor, Department of Community Medicine, helped with drafting the protocol. Achuth Ajith Kumar, Aarati Krishnan and Amitha Abraham, 27th batch MBBS students, helped in data collection.
Funding
Funding was provided by the State Board of Medical Research, Kerala, India.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AVL participated in the study design, collected and interpreted data, and prepared the manuscript. RC was involved in the study design, coordinated the study, and revised the manuscript. TBC assisted with the study design, coordinated the study, and revised the manuscript. SMV helped in drafting the protocol, performed statistical analysis, and interpreted data. GR was involved in the preparation of the manuscript. SVK revised the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Vettuparambil, A., Chirukandath, R., Culas, T.B. et al. Hormone-receptor expression and survival patterns in operated cases of female invasive ductal breast carcinoma in Kerala: a retrospective cohort study. World J Surg Onc 13, 160 (2015). https://doi.org/10.1186/s12957-015-0582-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12957-015-0582-x