
Abstract
Background
To examine the associations of the independent and combined healthy lifestyle factors with health-related quality of life (HRQOL) in adolescents, and to test the moderating role of gender.
Methods
This cross-sectional study included 5125 adolescents aged between 11 and 20 years. They provided self-reported data on six healthy lifestyle factors, including never smoking, never drinking, good sleep quality, sufficient sleep duration, appropriate Internet use, and adequate physical activity. Adolescents’ HRQOL was evaluated using the Pediatric Quality of Life Inventory version 4.0. Linear regression models were conducted to explore the association of individual and combined healthy lifestyle factors with adolescents’ HRQOL. We further performed stratified analyses and likelihood ratio test to explore the moderating role of gender in these associations.
Results
Of the included adolescents, the proportions with 0–2, 3, 4, and 5–6 healthy lifestyle factors were 13.6%, 26.4%, 44.3%, and 15.7%, respectively. Compared to adolescents with composite healthy lifestyle scores of 0–2, those with scores of 3, 4, or 5–6 had significantly higher HRQOL scores across all dimensions, summary scales, and total scale in both unadjusted and adjusted models. Specifically, adolescents with 5–6 healthy lifestyle factors had a total scale score that was 19.03 (95%CI: 17.76 to 20.30) points higher than their counterparts who only had 0–2 healthy lifestyle factors. Significant dose-response patterns were also observed in aforementioned associations. Gender was a significant moderator in the associations between composite healthy lifestyle groups and HRQOL scores, except for the social functioning dimension.
Conclusions
Our results confirmed that combined healthy lifestyle factors were associated with improved HRQOL among adolescents, with a stronger association observed in girls. These findings underscore the necessity for education and healthcare authorities to design health-promoting strategies that encourage multiple healthy lifestyle factors in adolescents, with the objective of enhancing their overall health outcomes.
Similar content being viewed by others

Introduction
Health-related quality of life (HRQOL) is a subjective measure that could reflect an individual’s overall health, encompassing physical, mental, and social well-being [1]. It is widely used in clinical practice to assess and monitor patients’ well-being, thereby informing treatment decisions [1,2,3,4]. In recent years, HRQOL has been applied to the general population [5,6,7]. Previous studies have found that lower HRQOL scores were associated with increased risks of hospitalization and even mortality [8,9,10]. HRQOL has also been integrated into clinical practice and public health research for children and adolescents [11].
Various factors, such as age, gender, socioeconomic status, and the presence of chronic diseases, can influence HRQOL [12,13,14]. There is also evidence suggesting that healthy lifestyle factors, e.g., abstaining from smoking and drinking, maintaining good sleep quality and sufficient sleep duration, appropriate Internet use, and engaging in adequate physical activity, are associated with higher HRQOL scores in children and adolescents [15,16,17,18,19,20]. For instance, a cross-sectional study has found that non-smoking adolescents reported better self-rated health and life satisfaction compared to active or passive smokers [15]. Another randomized controlled trial has shown that adolescents who received interventions to reduce binge drinking had higher HRQOL scores than those in the control group [16]. Similar positive associations have also been found between good sleep health and better HRQOL in adolescents [17, 18]. In addition, a cross-sectional study has revealed that adolescents with adaptive Internet use exhibited fewer depressive symptoms and higher HRQOL scores than those with maladaptive and pathological Internet use [19]. Furthermore, a previous study has found a positive association between higher level of physical activity and better HRQOL among Chinese adolescents [20]. While many studies have addressed the impact of individual lifestyle factors on HRQOL, research has suggested that these lifestyle factors often co-occur [21] and are cumulatively linked to health outcomes [22, 23]. Consequently, there is a need to further explore the influence of cumulative lifestyle factors on HRQOL in adolescents, in order to inform early interventive strategies. However, limited research conducted in Europe and Australia have explored this issue in adolescents [24,25,26]. Since lifestyle patterns and self-rated HRQOL vary among adolescents from different countries due to cultural and socioeconomic differences [27,28,29], it is therefore crucial to investigate the associations between cumulative healthy lifestyle factors and HRQOL in the context of Chinese culture.
In addition, the role of gender in the associations between healthy lifestyle factors and health outcomes remain inconsistent [26, 30]. A longitudinal study conducted in Australia has revealed that compared to adolescents with 0 or 1 healthy lifestyle factor, those reporting 4 or 5 healthy lifestyle factors had significantly higher scores of physical HRQOL in both boys and girls [26]. However, such impact on the total HRQOL scores was only significant in boys, but not in girls [26]. Furthermore, a meta-analysis of 38 articles has found no gender difference in the association between physical activity, sedentary behavior, and self-rated health among children and adolescents [30]. These inconsistent findings may result from the heterogeneous healthy lifestyle factors and HRQOL measures that were investigated, highlighting the need for further research to clarify the role of gender in the association between combined healthy lifestyle factors and HRQOL in Chinese adolescents.
Therefore, in this study, we aimed to explore the association of a composite healthy lifestyle score that was generated based on smoking status, drinking status, sleep quality, sleep duration, Internet addiction, and physical activity, with HRQOL in adolescents attending middle schools. Stratified analyses and tests for interaction were further conducted to evaluate the potential moderating role of gender in this association.
Methods
Study design and population
This cross-sectional study was conducted between November and December 2021 and recruited middle school students from the Huangpu district of Guangzhou, China. In order to obtain a representative study sample, we randomly selected six middle schools, proportional to the district’s total number of middle schools. The selection comprised four junior middle schools and two combined junior and senior middle schools. We invited all students from these schools, along with their parents, to participate in the study. Out of the invited participants, 6982 adolescents, including 4330 junior middle school students and 2652 senior middle school students, with parental consent had completed the questionnaires, yielding a 90.1% response rate. We then excluded 1729 adolescents due to incomplete information on healthy lifestyle factors and 128 adolescents with missing data on HRQOL. Ultimately, a total of 5125 adolescents were included in the current analysis.
The present research project was approved by the Ethics Committee of School of Public Health, Sun Yat-sen University (Reference number: 2021[116]). Prior to the survey, parents of each student have signed an informed consent for their children to participate in this study.
Assessment of health-related quality of life
Adolescents’ HRQOL was evaluated using the Pediatric Quality of Life Inventory version 4.0 (PedsQL 4.0). This multidimensional instrument consists of 23 items that evaluate emotional functioning (5 items), physical functioning (8 items), social functioning (5 items), and school functioning (5 items) [31,32,33,34]. The reliability and validity of PedsQL 4.0 have been confirmed among Chinese children and adolescents [35]. Each item was rated based on a five-point Likert scale ranging from 0 to 4 (0 = never a problem, 1 = almost never a problem, 2 = sometimes a problem, 3 = often a problem, and 4 = almost always a problem). To calculate HRQOL scores, responses were reversely scored and linearly transformed into a 0 to 100 scale, where higher scores represented better HRQOL. The score for each dimension was calculated by averaging the scores of all items within that dimension. In addition, the scores of the psychosocial health summary scale were calculated as the average scores of the emotional, social, and school functioning dimensions. The total scale scores were further computed as the average scores of all items in the questionnaire.
Assessment of composite healthy lifestyle score
Smoking and drinking status were divided into ever and never users by asking the questions “Have you ever smoked an entire cigarette?” and “Have you ever had a glass of wine/beer?”, respectively.
Sleep quality and duration were assessed by the Pittsburgh Sleep Quality Index (PSQI) questionnaire [36]. which has been validated and proven to be reliable in Chinese children and adolescents [37]. The questionnaire measures seven different sleep dimensions, including subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleep medications, and daytime dysfunction. A global PSQI score ranging from 0 to 21 was calculated by summing scores of the seven dimensions, with higher scores indicating poorer sleep quality. We defined good sleep quality as a PSQI global score ≤ 7 in Chinese version [37]. Sufficient sleep duration was determined using cutoff values of 9 h per night for junior middle school students and 8 h per night for senior middle school students, according to the Chinese guideline [38].
The Young Diagnostic Questionnaire (YDQ) was used to assess the addiction level of Internet use [39], a valid and reliable instrument in Chinese young population [40]. The questionnaire consists of eight items regarding Internet addiction, such as “feeling preoccupied with the Internet”, “feeling the need to use the Internet for an increasing amount of time”, and “unsuccessful efforts to control Internet use”. Each of the item was dichotomized as either yes (coded as 1) or no (coded as 0). The cumulative YDQ score was calculated by adding up the eight items, with higher scores representing a higher level of Internet addiction. We defined the group with appropriate Internet use as those with a YDQ score < 5 and the group with Internet addiction as those with a score of 5 or above [39].
To assess physical activity, the validated Chinese version of the International Physical Activity Questionnaire-Short Form (IPAQ-SF) was used [41]. It covers questions related to the frequency and duration of vigorous, moderate, and light physical activity, as well as the daily duration of sedentary behavior, in the past seven days. We defined adequate physical activity as having moderate or vigorous physical activity for at least 60 min per day and having at least 10 min vigorous physical activity for more than three days per week according to the Physical Activity Guidelines for Chinese adolescents [42].
We assigned 1 point for each of the aforementioned healthy lifestyle factors: i.e., never smoking, never drinking, good sleep quality, sufficient sleep duration, appropriate Internet use, and adequate physical activity. A composite healthy lifestyle score (range: 0–6 points) was generated by summing the points for these six healthy lifestyle factors, with higher scores representing a healthier lifestyle. The composite healthy lifestyle scores were further reclassified into four groups according to the distribution among the participants: (1) 0–2 healthy lifestyle factors, (2) 3 healthy lifestyle factors, (3) 4 healthy lifestyle factors, and (4) 5–6 healthy lifestyle factors.
Covariates
Adolescents
Adolescents provided self-reported information on their age, gender, single child status, primary caregiver, and boarding school attendance. Single child status was identified as having only one child in the family (yes) or having more than one child in the family (no). Primary caregivers were categorized as either parents or others. Boarding school attendance was dichotomized as attending a boarding school (yes) and not attending a boarding school (no).
Parents
Parental socio-demographic characteristics, including age, marital status, and occupational status, were also collected. Parents self-reported their age and occupational status through online questionnaire. Occupational status was classified as employed or unemployed. Marital status was reported by their children, which was categorized as currently married or unmarried. The latter included single, divorced, separated, and widowed.
Statistical analysis
Descriptive statistics for continuous and categorical variables were presented as means with standard deviation (SD) and frequencies with percentage, respectively. To compare differences in characteristics across the composite healthy lifestyle groups, one-way analysis of variance (ANOVA) was used for continuous data and Chi-squared test was applied for categorical data. To assess trends in characteristics across different composite healthy lifestyle groups, polynomial comparisons were used for continuous data and Mantel-Haenszel statistic was applied for categorical data.
Linear regression models were established to assess the associations of both individual and combined healthy lifestyle factors with HRQOL. Crude models were first constructed. Then, adjusted models were further established with adjustment for adolescents’ age, gender, single child status, primary caregiver, and boarding school attendance, as well as parental age, marital status, and occupational status. When the exposure was the individual healthy lifestyle factor, models were further mutually adjusted for other healthy lifestyle factors. When the exposure was the composite healthy lifestyle groups, dose-response associations with adolescents’ HRQOL were assessed with trend tests. The linear regression assumptions of linearity, normality, homoscedasticity, and absence of multicollinearity were verified for all models. Results were reported as beta coefficient (β) with corresponding 95% confidence intervals (CI). Stratified analyses were further conducted by gender. The potential moderating role of gender in the association between healthy lifestyle scores and HRQOL was assessed by likelihood ratio test.
All data analyses were performed with Stata/SE 17.0. Statistical significance was two-sided with a P value < 0.05.
Results
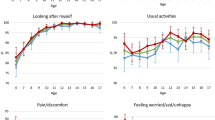
Of the 5125 adolescents included in the study, 2690 (52.5%) were boys and the average age was 14.6 (SD: 1.6) years. The prevalence of healthy lifestyle factors was 97.3% for never smoking, 69.4% for never drinking, 82.0% for good sleep quality, 12.6% for sufficient sleep duration, 83.2% for appropriate Internet use, and 15.3% for adequate physical activity. In terms of the combined healthy lifestyle factors, the proportions of adolescents with 0–2, 3, 4, and 5–6 healthy lifestyle factors were 13.6%, 26.4%, 44.3%, and 15.7%, respectively. In general, compared to adolescents with 0–2 healthy lifestyle factors, those with a composite healthy lifestyle score of 5–6 tended to be younger, were more likely to be boys, have parents as their primary caregivers, and not attend boarding schools. The parents of adolescents with a composite healthy lifestyle score of 5–6 were also more likely to be younger and married compared to the group with a composite healthy lifestyle score of 0–2 (Table 1). Furthermore, as the composite healthy lifestyle score increased, the HRQOL scores across all HRQOL dimensions, summary scales, and total scale were significantly higher (Fig. 1).

Comparison of adolescents’ HRQOL across the composite healthy lifestyle groups
The association between the six individual healthy lifestyle factors and adolescents’ HRQOL is displayed in Table 2. In crude models, all healthy lifestyle factors were significantly associated with higher HRQOL scores across all dimensions, summary scale, and total scale. After including covariates and mutually adjusting for other healthy lifestyle factors, each healthy lifestyle factor maintained its association with higher HRQOL scores, although the risk estimates were attenuated and some of the associations became statistically non-significant. Specifically, for the HRQOL total scale score, the effect estimates (β) of the associations were 4.30 for never smoking (95% CI: 2.16, 6.43), 2.36 for never drinking (95% CI: 1.57, 3.14), 13.93 for good sleep quality (95% CI: 12.99, 14.86), 1.63 for sufficient sleep duration (95% CI: 0.58, 2.67), 8.89 for appropriate Internet use (95% CI: 7.94, 9.84), and 1.67 for adequate physical activity (95% CI: 0.79, 2.56).
Table 3 presents the association between the composite healthy lifestyle groups and HRQOL scores in adolescents. Compared to adolescents with a composite healthy lifestyle score of 0–2, those with scores of 3, 4, or 5–6 had significantly higher HRQOL scores across all dimensions, summary scales, and total scale. These significant associations persisted in the adjusted models. Notably, when compared to adolescents with a composite healthy lifestyle score of 0–2, those reporting 5 or 6 healthy lifestyle factors had significantly higher scores of emotional functioning (β = 28.71, 95% CI: 26.69, 30.73), social functioning (β = 15.13, 95% CI: 13.62, 16.64), school functioning (β = 19.42, 95% CI: 17.73, 21.10), physical functioning (β = 12.85, 95% CI: 11.52, 14.18), psychosocial health summary scale (β = 21.09, 95% CI: 19.68, 22.49), and total scale (β = 19.03, 95% CI: 17.76, 20.30). Specifically, significant dose-response associations were observed between the composite healthy lifestyle groups and the HRQOL scores for all dimensions, summary scales, and total scale in both crude and adjusted models.
The associations of the composite healthy lifestyle groups with adolescents’ HRQOL scores were further evaluated by their genders (Table 4). In both gender groups, significant dose-response associations were observed between the composite healthy lifestyle groups and higher HRQOL scores across all dimensions, summary scales, and total scale (all P value for trend < 0.001). We also found that gender was a significant moderator in the associations of the composite healthy lifestyle groups with emotional functioning, school functioning, physical functioning, psychosocial health summary scale, and total scale (all P value < 0.05), with girls being more sensitive to healthy lifestyle factors than boys. In contrast, the moderating role of gender in the association between composite healthy lifestyle groups and social functioning was not statistically significant (P value = 0.352).
Discussion
In this cross-sectional study, we found that healthy lifestyle factors, including never smoking, never drinking, good sleep quality, sufficient sleep duration, appropriate Internet use, and adequate physical activity, were independently associated with better HRQOL in adolescents. In addition, the composite healthy lifestyle scores showed a dose-response pattern with HRQOL across all dimensions, summary scales, and total scale. Gender was a significant moderator in the association between the composite healthy lifestyle scores and different HRQOL dimensions, summary scales, and total scale, with the exception of the social functioning dimension. Girls were found to be more sensitive to healthy lifestyle factors than boys.
Our findings of the positive associations between composite healthy lifestyle scores and adolescents’ HRQOL were in line with previous studies conducted in European counties [24, 25]. One study in Spain has considered five healthy lifestyle factors, including physical activity, adherence to the Mediterranean diet, sleep quality, sleep duration, and screen time [24]. The results indicated that the number of healthy lifestyle factors was positively associated with HRQOL scores measured by the KIDSCREEN-10 questionnaire [24]. Another cross-sectional study of 5024 adolescents has included healthy lifestyle factors of physical activity, screen-based time, sleep duration, fruit and vegetable consumption, drinking, and smoking, and demonstrated a significant association of the composite healthy lifestyle measure with better self-rated health and higher HRQOL [25]. Similar findings have also been reported in studies focusing on other outcomes in children and adolescents [43, 44]. For example, a cross-sectional study has found that a lower number of healthy lifestyle factors was associated with higher risks of depressive symptoms among Chinese adolescents [43]. Moreover, a nationwide cross-sectional study in China has shown that compared with adolescents who had a healthy lifestyle, those with an unhealthy lifestyle had a higher risk of obesity [44].
The mechanisms underlying the positive association between healthy lifestyle factors and HRQOL scores are not yet fully understood. Several possible explanations might account for such associations. First, previous studies have indicated that healthy lifestyle factors could reduce chronic inflammatory levels, subsequently leading to improved HRQOL [45,46,47]. Second, unhealthy lifestyle factors such as sleep problems and Internet addiction have been shown to be associated with stress and negative emotions, which might stimulate the hypothalamic-pituitary-adrenal axis, increase cortisol levels, and ultimately lead to mental problems in adolescents, resulting in worse HRQOL [48,49,50,51,52]. Conversely, healthy lifestyle factors can help maintain better HRQOL among adolescents. Third, appropriate Internet use is beneficial to facilitate technical skills, social connection, and communication in adolescents, thereby promoting their mental well-being and ultimately better HRQOL [53, 54]. Therefore, the significant association between healthy lifestyle factors and better HRQOL was plausible.
Our study also found a moderating role of gender in the association between cumulative healthy lifestyle scores and adolescents’ HRQOL across all dimensions, except for social functioning. Although there are limited similar studies to compare with, this finding aligns with previous studies that have identified gender-specific associations between healthy lifestyle factors and other health-related outcomes in adolescents [43, 55]. For example, a cross-sectional study among 3967 Chinese adolescents aged 11–19 years has observed a stronger association between the number of unhealthy lifestyle factors and depressive symptoms in girls compared to boys [43]. Similarly, research conducted in India has also found a link between cumulative unhealthy lifestyle factors and obesity in girls, while boys only exhibited an increased BMI [55]. However, contradictory findings were reported in another study in China, which has shown a relatively larger effect size in boys compared to girls regarding the association between reduced weekend sleep duration and abdominal obesity [56]. One possible explanation of the discrepancies might be attributed to the diverse healthy lifestyle factors investigated across different studies. In addition, while most prior studies focused on a specific health outcome, our study employed a multidimensional construct that could reflect the overall self-rated health. Nevertheless, further studies are still needed to explore the possible gender-specific association between the combined healthy lifestyle factors and HRQOL in young populations, and to uncover the possible underlying mechanisms.
Our study benefited from a large sample size, which allowed us to conduct analyses with sufficient statistical power. By using HRQOL as the outcome, we were able to assess the overall health of the young population. In addition, we assessed not only the impact of individual healthy lifestyle factors, but also the combined impact of these healthy lifestyle factors on adolescents’ HRQOL. We also evaluated the moderating role of gender in this association to identify sensitive populations. Nevertheless, several limitations should be acknowledged as well. First, due to the cross-sectional nature of the study, we were unable to establish a causal relationship between the exposure and the outcome. Future longitudinal studies are needed to better understand the temporal association between healthy lifestyle factors and adolescents’ HRQOL. Second, our participants were recruited exclusively from one megacity. The generalizability of the findings should be considered with caution. Third, although a healthy diet has been recognized as a critical healthy lifestyle factor associated with HRQOL in adolescents [57], we did not include it in our study due to data unavailability. Fourth, we utilized the composite healthy lifestyle scores in our analyses, assuming each lifestyle factor equally impacts HRQOL. While this approach might not reflect the real-life situation, it is straightforward and can be easily understood by adolescents during preventive interventions. Furthermore, we have assessed the associations with consideration of different weighting for each lifestyle factor in sensitivity analysis (data not shown) and the findings were consistent, indicating the reliability of our conclusions. Last, while several confounders were controlled in the multivariate analyses, unmeasured confounders and modifiers may still be present [58,59,60].
Conclusions
In conclusion, we found that adherence to an overall healthy lifestyle, including never smoking, never drinking, good sleep quality, sufficient sleep duration, appropriate Internet use, and adequate physical activity, was associated with higher HRQOL scores in adolescents. In addition, the associations tended to be stronger in girls. These findings implied that health education and public health interventions aimed at promoting healthy lifestyle factors in adolescents may be an effective strategy for improving their HRQOL, especially among girls. However, further randomized controlled trials are needed to confirm the conclusion.
Data Availability
The datasets used and analyzed during the current study are not publicly available for ethical and privacy reasons but are available from the corresponding author upon reasonable request.
References
Guyatt GH, Feeny DH, Patrick DL. Measuring health-related quality of life. Ann Intern Med. 1993;118:622–9.
Toh Y, Morita M, Yamamoto M, et al. Health-related quality of life after esophagectomy in patients with Esophageal cancer. Esophagus. 2022;19:47–56.
Wong CK, Guo VY, Chen J, et al. Methodological and reporting quality of comparative studies evaluating Health-Related Quality of Life of Colorectal Cancer patients and controls: a systematic review. Dis Colon Rectum. 2016;59:1073–86.
Wong MY, Yang Y, Cao Z, et al. Effects of health-related quality of life on health service utilisation in patients with colorectal Neoplasms. Eur J Cancer Care. 2018;27:e12926.
Lam CLK, Guo VY, Wong CKH, et al. Poverty and health-related quality of life of people living in Hong Kong: comparison of individuals from low-income families and the general population. J Public Health. 2017;39:258–65.
Bedford LE, Guo VY, Yu EYT, et al. Do negative Emotional States play a Role in the Association between Intimate Partner Violence and Poor Health-Related Quality of Life in Chinese women from low-income families? Violence against Women. 2020;26:2041–61.
Wong CK, Fung CS, Siu SC, et al. The impact of work nature, lifestyle, and obesity on health-related quality of life in Chinese professional drivers. J Occup Environ Med. 2012;54:989–94.
Phyo AZZ, Gonzalez-Chica DA, Stocks NP, et al. The utility of assessing health-related quality of life to predict cognitive decline and dementia. J Alzheimers Dis. 2021;80:895–904.
Pinheiro LC, Reshetnyak E, Sterling MR, et al. Using health-related quality of life to predict cardiovascular disease events. Qual Life Res. 2019;28:1465–75.
Gobbens RJJ, van der Ploeg T. The prediction of mortality by quality of life assessed with the WHOQOL-BREF: a longitudinal analysis at the domain and item levels using a seven-year follow-up period. Qual Life Res. 2021;30:1951–62.
Wallander JL, Koot HM. Quality of life in children: a critical examination of concepts, approaches, issues, and future directions. Clin Psychol Rev. 2016;45:131–43.
Shin H, Jeon S, Cho I. Factors influencing health-related quality of life in adolescent girls: a path analysis using a multi-mediation model. Health Qual Life Outcomes. 2022;20:50.
Aschalew AY, Yitayal M, Minyihun A. Health-related quality of life and associated factors among patients with Diabetes Mellitus at the University of Gondar referral hospital. Health Qual Life Outcomes. 2020;18:62.
Otto C, Haller AC, Klasen F, et al. Risk and protective factors of health-related quality of life in children and adolescents: results of the longitudinal BELLA study. PLoS ONE. 2017;12:e0190363.
Heshmat R, Qorbani M, Safiri S, et al. Association of passive and active Smoking with self-rated health and life satisfaction in Iranian children and adolescents: the CASPIAN IV study. BMJ open. 2017;7:e012694.
Vargas-Martínez AM, Trapero-Bertran M, Lima-Serrano M, et al. Measuring the effects on quality of life and alcohol consumption of a program to reduce binge drinking in Spanish adolescents. Drug Alcohol Depend. 2019;205:107597.
Potter MN, Howell DR, Dahab KS, et al. Sleep Quality and Quality of Life among Healthy High School Athletes. Clin Pediatr. 2020;59:170–7.
Wong CKH, Wong RS, Cheung JPY, et al. Impact of sleep duration, physical activity, and screen time on health-related quality of life in children and adolescents. Health Qual Life Outcomes. 2021;19:145.
Takahashi M, Adachi M, Nishimura T, et al. Prevalence of pathological and maladaptive internet use and the association with depression and health-related quality of life in Japanese elementary and junior high school-aged children. Soc Psychiatry Psychiatr Epidemiol. 2018;53:1349–59.
Dong X, Ding M, Chen W, et al. Relationship between Smoking, physical activity, screen time, and quality of life among adolescents. Int J Environ Res Public Health. 2020;17:8043.
Spring B, Moller AC, Coons MJ. Multiple health behaviours: overview and implications. J Public Health. 2012;34 Suppl 1:i3–i10.
Li Y, Pan A, Wang DD, et al. Impact of healthy lifestyle factors on life expectancies in the US Population. Circulation. 2018;138:345–55.
Liu ZY, Wang C, Zhang YJ, et al. Combined lifestyle, mental health, and mortality in US cancer survivors: a national cohort study. J Translational Med. 2022;20:376.
Solera-Sanchez A, Adelantado-Renau M, Moliner-Urdiales D, et al. Health-related quality of life in adolescents: individual and combined impact of health-related behaviors (DADOS study). Qual Life Res. 2021;30:1093–101.
Marques A, Peralta M, Santos T, et al. Self-rated health and health-related quality of life are related with adolescents’ healthy lifestyle. Public Health. 2019;170:89–94.
Gopinath B, Louie JCY, Flood VM, et al. Influence of obesogenic behaviors on health-related quality of life in adolescents. Asia Pac J Clin Nutr. 2014;23:121–7.
Bräker AB, Soellner R. Alcohol drinking cultures of European adolescents. Eur J Pub Health. 2016;26:581–6.
Gariepy G, Danna S, Gobiņa I, et al. How are adolescents sleeping? Adolescent sleep patterns and sociodemographic differences in 24 European and North American Countries. J Adolesc Health. 2020;66 Suppl 6:81–88.
Ow N, Mayo NE. Health-related quality of life scores of typically developing children and adolescents around the world: a meta-analysis with meta-regression. Qual Life Res. 2020;29:2311–32.
Zhang T, Lu G, Wu XY. Associations between physical activity, sedentary behaviour and self-rated health among the general population of children and adolescents: a systematic review and meta-analysis. BMC Public Health. 2020;20:1343.
Varni JW, Seid M, Kurtin PS. PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39:800–12.
Chen D, Lin L, Li C, et al. Maternal adverse childhood experiences and health-related quality of life in preschool children: a cross-sectional study. Child Adolesc Psychiatry Mental Health. 2023;17:19.
Xiang H, Lin L, Chen W, et al. Associations of excessive screen time and early screen exposure with health-related quality of life and behavioral problems among children attending preschools. BMC Public Health. 2022;22:2440.
Luo S, Lin L, Chen W, et al. Association between maternal intimate partner Violence and health-related quality of life in their preschool children: the mediating role of maternal parenting styles. Front Psychiatry. 2022;13:996971.
Hao Y, Tian Q, Lu Y, et al. Psychometric properties of the Chinese version of the pediatric quality of life inventory 4.0 generic core scales. Qual Life Res. 2010;19:1229–33.
Buysse DJ, Reynolds CF 3rd, Monk TH, et al. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213.
Liu X, Tang M, Hu L et al. Reliability and validity of the Pittsburgh Sleep Quality Index (Chinese Version). Chin J Psychiatry. 1996:103–7.
The State Council of China. Healthy China Action Plan (2019–2030). In: The State Council of China, ed. Beijing, 2019.
Young KS. Internet addiction: the emergence of a new clinical disorder. CyberPsychology & Behavior. 1998;1:237–44.
Zhang X, Zhang K, Zhu Y, et al. Evaluation of four internet addiction scales in college students. Chin J Sch Health. 2021;42:1193–7.
Ren YJ, Su M, Liu QM, et al. Validation of the simplified Chinese-character version of the international physical activity questionnaire-long form in urban community-dwelling adults: a cross-sectional study in Hangzhou, China. Biomed Environ Sci. 2017;30:255–63.
Zhang Y, Chen C, Liu S, et al. Guidelines for physical activity of children and adolescents in China. Chin J Evidence-Based Pediatr. 2017;12:401–9.
Cao R, Gao T, Ren H, et al. Unique and cumulative effects of lifestyle-related behaviors on depressive symptoms among Chinese adolescents. Int J Soc Psychiatry. 2022;68:354–64.
Lian R, Wang ZH, Zou ZY, et al. Does a healthy lifestyle lower the elevated risk of obesity caused by Caesarian Section Delivery in Children and adolescents? Nutrients. 2022;14:3528.
Costello EJ, Copeland WE, Shanahan L, et al. C-reactive protein and substance use disorders in adolescence and early adulthood: a prospective analysis. Drug Alcohol Depend. 2013;133:712–7.
Metsios GS, Moe RH, Kitas GD. Exercise and inflammation. Best Pract Res Clin Rheumatol. 2020;34:101504.
Atrooz F, Salim S. Sleep deprivation, oxidative stress and inflammation. Adv Protein Chem Struct Biology. 2020;119:309–36.
Sadeh A, Tikotzky L, Kahn M. Sleep in infancy and childhood: implications for emotional and behavioral difficulties in adolescence and beyond. Curr Opin Psychiatry. 2014;27:453–9.
Nollet M, Wisden W, Franks NP. Sleep deprivation and stress: a reciprocal relationship. Interface Focus. 2020;10:20190092.
Yang Q, Wu Z, Yang X, et al. Associations between uncertainty stress, life stress and internet addiction among medical students. Front Public Health. 2021;9:809484.
Lupien SJ, McEwen BS, Gunnar MR, et al. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat Rev Neurosci. 2009;10:434–45.
Zajkowska Z, Gullett N, Walsh A, et al. Cortisol and development of depression in adolescence and young adulthood - a systematic review and meta-analysis. Psychoneuroendocrinology. 2022;136:105625.
O’Reilly M, Dogra N, Hughes J, et al. Potential of social media in promoting mental health in adolescents. Health Promot Int. 2019;34:981–91.
Aliverdi F, Farajidana H, Tourzani ZM, et al. Social networks and internet emotional relationships on mental health and quality of life in students: structural equation modelling. BMC Psychiatry. 2022;22:451.
Moitra P, Madan J, Verma P. Independent and combined influences of physical activity, screen time, and sleep quality on adiposity indicators in Indian adolescents. BMC Public Health. 2021;21:2093.
Liu M, Cao B, Luo Q, et al. Associations between sleep duration, wake-up time, bedtime, and abdominal obesity: results from 9559 Chinese children aged 7–18 years. Front Endocrinol (Lausanne). 2021;12:735952.
Victoria-Montesinos D, Tárraga-Marcos A, Brazo-Sayavera J, et al. Adherence to the Mediterranean Diet and Health-Related Quality of Life during the COVID-19 lockdown: a cross-sectional study including preschoolers, children, and adolescents from Brazil and Spain. Nutrients. 2023;15:677.
Guo VYW, Wong CKH, Wong RSM, et al. Spillover effects of maternal chronic Disease on children’s quality of life and behaviors among low-income families. The Patient. 2018;11:625–35.
Guo VY, Yu EYT, Wong RSM, et al. Maternal mental quality of life mediates the associations between intimate partner abuse against mothers and their children’s behaviours and quality of life in low-income Chinese families. Qual Life Res. 2017;26:3297–306.
Wong R, Guo V, Ip P, et al. Mothers’ health-related quality of life: its relationship with children’s health-related quality of life and behavior in low-income families. Family Med Community Health. 2016;4:4–12.
Acknowledgements
The authors would like to express their gratitude to the participants for their support of this study.
Funding
This work was supported by the National Natural Science Foundation of China (Grant number 82204069), the Fundamental Research Funds for the Central Universities, Sun Yat-sen University (Grant number 22qntd4201), and the start-up fund from the Sun Yat-sen University (Grant number 51000-18841211).
Author information
Authors and Affiliations
Contributions
Conceptualization: VYG; Methodology: HX, XF, and VYG; Data curation: HX, LL, SL, and VYG; Formal analysis and investigation: HX and XF; Writing - original draft preparation: HX, XF, and VYG; Writing - review and editing: all authors; Funding acquisition: VYG. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The research was performed by the Helsinki Declaration, and obtained ethical approval from the Ethics Committee of School of Public Health, Sun Yat-sen University (Ethical approval number: 2021[116]). After the intention and procedure of this study had been fully explained in detail, each parent has signed an informed consent before attending this study.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xiang, H., Feng, X., Lin, L. et al. Association between healthy lifestyle factors and health-related quality of life among Chinese adolescents: the moderating role of gender. Health Qual Life Outcomes 21, 119 (2023). https://doi.org/10.1186/s12955-023-02201-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-023-02201-2