
Abstract
Background
The 12-item MOS Short-form Health Survey version 2 (SF-12v2) and the Veterans RAND 12-item Health Survey (VR-12) are generic health-related quality of life measures. They are fairly similar, but their differences in scores have not been assessed. Therefore, this study aimed to assess the differences between the SF-12v2 and the VR-12 in a Chinese population.
Methods
We conducted a household survey of 500 Chinese adults in Hong Kong. Both the SF-12v2 and the VR-12 were self-administered. The physical component summary score (PCS) and the mental component summary score (MCS) of each instrument were computed using well established algorithms. Their mean differences were assessed using 95% confidence interval (CI), and their individual differences were assessed by Bland–Altman analysis.
Results
The participants had a mean age of 38 years (range: 18–80 years). The mean PCS and MCS scores of the SF-12v2 were 50.3 (SD = 6.5) and 49.0 (SD = 9.0), while those of the VR-12 were 49.6 (SD = 6.2) and 49.7 (SD = 8.8), respectively. The corresponding paired differences (SF-12v2—VR-12) of the PCS and MCS were 0.8, 95% CI (0.4–1.1) and − 0.7, 95% CI (− 1.2 to − 0.2), respectively. All confidence limits fell within the minimal clinical important difference (MCID) of 3. The 95% limits of agreement were − 7.0, 8.5 for PCS and − 11.2, 9.9 for MCS, which fell outside the corresponding MCID for individual responses.
Conclusion
The SF-12v2 and the VR-12 reached mean equivalence at the group sample level, but there was a range of individual differences.
Similar content being viewed by others

Background
Self-reported outcome instruments are used worldwide to measure health-related quality of life (HRQL). The 12-item Medical Outcomes Study (MOS) Short-form Health Survey (SF-12) and the 12-item Veterans RAND Health Survey (VR-12) are two generic instruments used to assess quality of life in the general population. The MOS SF-12 is a proprietary instrument, while the VR-12 is regarded as a low-cost alternative. Both instruments were derived from the RAND SF-36 Health Survey, which was developed in 1988 as part of the Medical Outcomes Study (MOS) [1, 2]. The RAND SF-36 Health Survey, also known as the MOS SF-36 Health Survey, comprises 36 items. Based on these items, two component scores are measured, namely the physical summary component score (PCS) and the mental component summary score (MCS); the items cover eight scales designed to assess various aspects of quality of life in the general population, namely physical functioning (PF), role limitations due to physical problems (RP), bodily pain (BP), general health perceptions (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE), and mental health (MH) [3]. Since then, the two instruments have undergone development separately. Thus, they are similar but have differently worded questions and different scoring algorithms.
The MOS SF-12 is a shortened version of the MOS SF-36 Health Survey that reproduces the PCS and MCS scores of the MOS SF-36 [3, 4]. The development of the SF-36v2 Health Survey in 1996 improved the clarity of the original item wording, changed dichotomous choices for seven items in the RP and RE scales to five choices, and removed a response option from items in the MH and VT scales [1]. These same changes were applied to the corresponding items in the MOS SF-12, resulting in the SF-12v2 Health Survey [5, 6]. On the other hand, the VR-12 was derived from the Veterans RAND 36-item Health Survey (VR-36), which was modified from the MOS SF-36 by increasing the response choices for RP and RE items to five-point Likert choices [7, 8]. The VR-12 also reproduces the PCS and MCS of the VR-36 and comprises the same eight scales of the MOS SF-36 [7, 9].
Both the MOS SF-36v2 and the VR-36 have demonstrated adequate measurement properties in the general population [1, 10], and the PCS and MCS reproduced from their short forms, SF-12v2 and VR-12, have also been commonly used in general population studies [8, 11]. The VR-12, in particular, has shown that it can be accurately linked to the global health scale of the Patient-Reported Outcome Measurement Information System (PROMIS) [12]. Although the SF-12v2 and the VR-12 basically comprise the same set of 12 items, there are differences in the item wording, response choices, and scoring (Table 1). Specifically, there are differences in the item wording. Moreover, the order of the response choices for the two RP items and the two RE items of the SF-12v2 are reversed in those of the VR-12 [13]. In addition, the two MH items and the VT item of the SF-12v2 have five response choices, whereas those of VR-12 have six response choices.
Apart from format differences, the SF-12v2 and the VR-12 also have different scoring procedures despite both procedures being standardized by the norms from a general population in the United States (US). First, they do not share the same item coding. Second, the SF-12v2 uses proprietary norms, collected in 1998 and 2009, whereas the VR-12 uses the non-proprietary 1990 US population norms, which have been updated in 2009 and 2018 [14, 15].
Although the PCS of the MOS SF-12 has shown a strong correlation with that of the VR-12 [16], item format and type have been shown to affect the psychometric properties, such as the internal reliability and structural validity, of an instrument [17, 18]. Moreover, the MOS SF-12 and the VR-12 have been shown to have distributional differences in the US population [19]. A similar result was observed in the German versions of the MOS SF-12 and the VR-12 [20]. Moreover, the PCS and MCS of the SF-12 were derived from orthogonal rotation, whereas those of the VR-12 were derived from oblique rotation [19]. In view of the differences, scores of the SF-12v2 and VR-12 in an US population have been linked [21, 22]. However, there were no direct comparisons made between the PCS and the MCS of the SF-12v2 and those of the VR-12 in a Chinese population. Estimating their differences would help to assess whether there are discernible differences between the two instruments. If not, the VR-12 would be a viable alternative to the SF-12v2. Therefore, this study aimed to directly compare the two instruments in a Chinese population.
Methods
Design and participants
This study was part of a cross-sectional household survey. The details of the survey have been described elsewhere [23,24,25].
Between February 2018 and September 2019, we recruited 500 participants who were 18 or older. We excluded those who had hearing problems, sleep problems sleep disturbances, or psychiatric illnesses. They were sampled from a representative sampling frame purchased from the Hong Kong Census and Statistics Department, which covered the entire territory. All participants signed an informed consent form before they completed the self-administered study questionnaires.
Ethics approval was obtained from the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (UW 17-011).
Measurements
The sociodemographic questionnaire, the SF-12v2, and the VR-12 were administered in paper form. Specifically, each participant first completed the SF-12v2, followed by four survey modules that comprised 52 items, and then the VR-12. Other self-reported instruments that were administered have been described elsewhere [23,24,25].
The sociodemographic data collected were age, sex, marital status, education level, occupation, and chronic illnesses.
The standard Chinese version of the SF-12v2 was self-administered [26, 27]. The SF-12v2 had been well tested with satisfactory psychometric performance in both the adult and adolescent populations [26, 27]. It can be scored as eight scales and as the PCS and the MCS scores. They were scored in accordance with its scoring manual, using normative data from the 1998 US population for norm-based scoring [28]. The PCS and the MCS typically were normed to a US population with a higher score indicating a better quality of life in the corresponding scale/component.
The Chinese version of the VR-12 was also administered [29]. It was obtained from rigorous forward–backward translation, taking account of cultural differences, and had been psychometrically evaluated [29]. We obtained the R code from the developer for scoring using the 1990 US normative data [9]. The PCS and the MCS also were standardized and normed to a US population, with a higher score indicating a better quality of life in the corresponding component [30]. The eight scales were not normed but were standardized in the range of 0–100.
Statistical analysis
The eight scales and the two components of the SF12-v2 and the VR-12, as well as the sample characteristics were summarized using descriptive statistics. We first assessed the average differences between the PCS, the MCS, and the eight scales of the SF12-v2 and the VR-12 by obtaining a 95% confidence interval (CI) for each component’s paired difference. The equivalence of a component was verified if the corresponding 95% CI was within its ± minimal clinically important difference (MCID). For the general population, the MCID was 3 for both the PCS, the MCS, and the eight scales [31, 32]. We also assessed the individual agreement between the two components by conducting a Bland–Altman analysis [33]. The 95% limits of agreement were obtained by the mean ± 1.96 standard deviation (SD) for the paired differences, which covered 95% of the differences [34]. Individual differences were verified if the agreement fell within the ± MCID for individual responses that accounted for the test precision. For the PCS, the MCID for individual responses was 6, whereas for the MCS it was 7 [31].
Linear regression was applied to examine the factors associated with the differences between the PCS and the MCS of the two instruments. Model adequacy was assessed by examining the model residuals. All statistical analyses were performed using R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Table 2 summarizes the sociodemographic characteristics of the participants (N = 500). The average age of the participants was 39 years (SD = 12; range = 18–80), 332 (66%) participants were female, 307 (61%) were married/cohabiting, 250 (82%) had a secondary school education, 370 (74%) were in the workforce, and 410 (82%) did not have any long-term illnesses.
Table 3 provides the mean and SD for the component and scale scores of the two instruments and their differences. The mean PCS of the SF-12v2 and the VR-12 were 50.3 and 49.6, respectively. The mean MCS of the SF-12v2 and the VR-12 were 49.0 and 49.7, respectively. Among the eight scales, the GH scale showed the largest mean difference, whereas the VT scale showed the largest absolute difference (Table 3). The Spearman rank correlation between PCS of the two instruments was 0.78 and that between MCS of the two instruments was 0.80. Figure 1 presents the scatterplots of the two instruments for each component. For the eight scales, the polychoric correlation between the two instruments was the lowest for the SF scale (r = 0.68), followed by the RE scale (r = 0.73). The correlation for the other scales was at least 0.83 (Table 3).

Scatter plots of a the physical component score (PCS), and b the mental component score (MCS), between the SF-12v2 and the VR-12
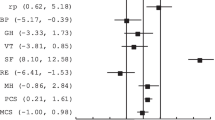
Figure 2 shows the 95% CIs for the paired differences of the component and scale scores of the two instruments. The average paired difference between the PCS of the SF-12v2 and that of the VR-12 (SF- 12v2—VR-12) was 0.7 for the PCS, 95% CI (0.4–1.1), which fell within its MCID of 3. For the MCS, the average difference was − 0.7, 95% CI (− 1.2 to − 0.2), which also fell within its MCID of 3. Among the eight scales, only the PF, BP and MH scales had their 95% CIs fell entirely within the MCID of 3 (Fig. 2).

95% confidence intervals for the pair differences of the two component and eight scale scores of the SF-12v2 and VR-12
The Bland–Altman plots for assessing the agreement between the PCS and the MCS of the two scales are shown in Fig. 3. The 95% limits of agreement for the PCS were − 7.0, 8.5, which fell outside the MCID of 6 for individual responses. For the MCS, the 95% limits of agreement were − 11.2, 9.9, which also fell outside the MCID of 7 for individual responses. Figure 4 depicts the Bland–Altman plots for all the eight scales. Their lower and upper limits of agreement were at least − 20.7 and 19.8, respectively.

Bland–Altman Plots for the differences of a the physical component score (PCS), and b the mental component score (MCS), between the SF-12v2 and the VR-12

Bland–Altman Plots for the differences of the eight scales, between the SF-12v2 and the VR-12
Table 4 shows the potential factors of the differences between the PCS and the MCS of the SF-12v2 and the VR-12. Examining the residuals did not reveal a substantial model inadequacy. Those with a higher age (estimate = − 0.03; p = 0.027) or separated/divorced/widowed (estimate = − 1.6; p = 0.029) reported a significantly lower PCS from the SF-12v2 than from the VR-12. However, the effect sizes were all within the two MCID units for the PCS. No significant factors were found for the MCS.
Discussion
To the best of our knowledge, this is the first study to investigate the differences between the SF-12v2 and the VR-12 in the Chinese population, and the first to use the Bland–Altman analysis to measure the extent of agreement between the SF-12v2 and the VR-12 on an individual basis. We found no discernible average differences between the PCS, MCS and some scales of the SF-12v2 and the VR-12. However, there were substantial individual differences.
Despite differences in item format and type between the SF-12v2 and the VR-12, this study found no average differences between the PCS and the MCS of the SF-12v2 and the VR-12, based on the MCID of 3 for both component scores. This supports the results of a previous study that the two component scores of the MOS SF-12 and the VR-12 yielded similar results when comparing patients with osteoarthritis and those with focal cartilage defects, although the MOS SF-12 version 1 was used instead of the version 2 used here [35]. Moreover, a group of patients who underwent spinal treatment completed the MOS SF-36 and had its PCS and MCS compared with the corresponding VR-12 component scores that were converted from the MOS SF-36 using a conversion algorithm from the Boston University School of Public Health. The PCS and the MCS of the MOS SF-36 were strongly correlated with the corresponding converted VR-12 component scores (correlation coefficient = 0.85–0.97) [36]. The correlation was higher than that in our sample when the SF-12v2 was used, which was 0.78–0.80. The lower observed association in our sample may be due to the use of much fewer items resulting in a greater variability. Nevertheless, the SF-12v2 and VR-12 remains strongly associated in their two component scores. The equivalence of the average PCS and MCS between the two instruments facilitates the use of either instrument to compare group differences. Moreover, including studies using either instrument in a meta-analysis or systematic review would not induce substantial study heterogeneity.
Among the eight scales, no average differences were also found in the PF, BP, SF and MH scales. However, the other four scales, RP, GH, VT and RE, did not have their 95% confidence intervals fall entirely within the 3 units of average equivalence limits. For both the RP and RE scales, item responses from the VR-12 require reverse code but those from the SF-12v2 do not. For GH, the item responses from the SF-12v2 and the VR-12 are coded differently. Moreover, the VT scale comprises only one item which was scored on a 5-point Likert scale in the SF-12v2 but on a 6-point Likert scale in the VR-12. Such method effects may have contributed to the systematic differences in their scale scores between the SF-12v2 and the VR-12. However, the MH scale had both of its items share the same difference in scoring as in the item of the VT scale. The observed average equivalence of the MH scale but not the VT scale may be because the MH scale comprises more items than the VT scale. All the PF, BP and SF scales between the SF-12v2 and the VR-12 share the same scoring methods, with generally only minor differences in item wording. Item 2a is the only item having a noticeable cultural difference in terms of the activities considered, with practicing Tai-Chi in the SH-12v2 and playing golf in the VR-12. Interestingly, the PF scale that includes item 2a did not show an average difference. This may be due to both golf and Tai-Chi being common activities nowadays.
Based on the Bland–Altman analysis, there were large individual differences in both the PCS and the MCS of the SF-12v2 and the VR-12 when compared with the MCIDs for individual responses of the two components. We explored the potential factors contributing to these differences, but none of them showed a substantial impact on the response differentials. In general, self-reported responses, as opposed to objective measurements, carry higher variability because of the extra intrapersonal variation even when the underlying construct remains stable. Therefore, a self-reported instrument would often be considered unreliable when comparing individual responses from specific individuals [37]. This echoes a much larger MCID when comparing individual responses. For example, the MCID for PCS is 3 for group comparisons but 6 for individual comparisons, while that for MCS is 3 for group comparisons and 7 for individual comparisons [31]. In our context of comparing the SF-12v2 and the VR-12, the difference in item format and type as well as scoring mechanism could have added variation to the individual responses, possibly resulting in a larger difference in the component scores between the two instruments. Hence, comparing the individual scores of the two components of the SF-12v2 and the VR-12 is not recommended.
All the eight scales showed individual differences between the SF-12v2 and the VR-12. Despite the eight scales do not possess a MCID for individual responses, their limits of agreement were much wider than those of the PCS and the MCS. Among the eight scales, the PF scale had the shortest limits of (− 20.7, 19.8), which are much beyond the MCIDs for individual responses of 6 and 7, respectively, for the PCS and the MCS. Indeed, it is known that not all scales have performed well in Chinese [26, 27, 32]. The MH scale of the SF-12v2 was shown to have low internal consistency [26]. Moreover, several scales did not possess equivalence between the English and Chinese languages, nor resemble the corresponding scales in the SF-36v2 [26, 27]. In general, there was also more interest on the two component scores [6, 38], and there should be cautious use of the eight scales with a good understanding of their limitations.
There are several limitations to this study. First, we have only assessed the equivalence in the estimates obtained from the two instruments. Assessing the structural equivalence may provide stronger evidence in terms of comparable validity and interpretation. However, items of the two instruments may not have the same number of response choices nor the same scoring scheme. Such differences may pose challenges to the application of multiple group confirmatory factor analysis and differential item functioning for assessing the structural equivalence. Second, it will be useful to compare the two instruments with external criteria for determining which one is better. For instance, the comprehensive item bank of physical function items from the Patient-Reported Outcomes Information System can be a useful criterion that future studies may consider [39]. Third, we have not considered newer 2009 norms and 2000–2002 norms for scoring the SF-12v2 and the VR-12, respectively. Future studies that examine the comparisons using the new norms would be useful. Fourth, we did not randomize the order of administering the SF-12v2 and the VR-12. The participants had to complete 52 other items before completing the VR-12 that may reduce the chance of recalling the earlier responses, the order effect may induce systematic differences and thus confound the observed differences between the two instruments. Further studies that randomize the order of administration would be desirable. Fifth, we focused on the Chinese versions of the SF-12v2 and the VR-12. Similar comparisons on other language versions, would be desirable to assess the generalizability of our results.
Conclusion
The two component scores PCS and MCS of the SF-12v2 and the VR-12 are equivalent when they are used in group comparisons. While the SF-12v2 has been well developed and tested in many ethnic groups, the VR-12 is a low-cost alternative. However, they have considerable individual differences, and caution should be exercised when comparing individual responses for their use in clinical practice.
Availability of data and materials
The datasets generated and/or analyzed in this study are not publicly available due to confidentiality.
References
Ware JE, Kosinski M, Bjorner J, Turner-Bowker D, Gandek B, Maruish M. User’s manual for the SF-36v2 health survey. Lincoln: Quality Metric Incorporated; 2007.
Iqbal SU, Rogers W, Selim A, Qian S, Lee A, Ren XS, et al. The Veterans Rand 12 item health survey (VR-12): what it is and how it is used. Boston University, pp 1–12. https://www.bu.edu/sph/files/2015/01/veterans_rand_12_item_health_survey_vr-12_2007.pdf. Accessed 17 June 2022.
Jenkinson C, Layte R, Jenkinson D, Lawrence K, Petersen S, Paice C, et al. A shorter form health survey: can the SF-12 replicate results from the SF-36 in longitudinal studies? J Public Health Med. 1997;19(2):179–86.
Lam CLK, Tse EYY, Gandek B. Is the standard SF-12 health survey valid and equivalent for a Chinese population? Qual Life Res. 2005;14(2):539–47.
Lam CLK, Wong CKH, Lam ETP, Lo YYC, Huang W-W. Population norm of Chinese (HK) SF-12 health survey-version 2 of Chinese adults in Hong Kong. Hong Kong Pract. 2010;32(2):77–86.
Fleishman JA, Selim AJ, Kazis LE. Deriving SF-12v2 physical and mental health summary scores: a comparison of different scoring algorithms. Qual Life Res. 2010;19(2):231–41.
Jones D, Kazis L, Lee A, Rogers W, Skinner K, Cassar L, et al. Health status assessments using the veterans SF-12 and SF-36: methods for evaluating outcomes in the veterans health administration. J Ambul Care Manag. 2001;24(3):68–86.
Kazis LE, Miller DR, Skinner KM, Lee A, Ren XS, Clark JA, et al. Applications of methodologies of the veterans health study in the VA healthcare system: conclusions and summary. J Ambul Care Manag. 2006;29(2):182–8.
Boston University. VR-36, VR-12 and VR-6D. Boston University School of Public Health. https://www.bu.edu/sph/about/departments/health-law-policy-and-management/research/vr-36-vr-12-and-vr-6d/. Accessed 7 Dec 2021.
Kazis LE, Lee A, Spiro A 3rd, Rogers W, Ren XS, Miller DR, et al. Measurement comparisons of the medical outcomes study and veterans SF-36 health survey. Health Care Financ Rev. 2004;25(4):43–58.
Wan EYF, Yu EYT, Chin WY, Choi EPH, Wu T, Lam CLK. Evaluation of the responsiveness of Short Form-12 Health Survey version 2 (SF-12v2) in Chinese patients with hypertension in primary care. Qual Life Res. 2019;28(10):2851–7.
Lapin BR, Kinzy TG, Thompson NR, Krishnaney A, Katzan IL. Accuracy of linking VR-12 and PROMIS global health scores in clinical practice. Value Health. 2018;21(10):1226–33.
Kazis LF, Miller DR, Clark JA, Skinner KM, Lee A, Ren XS, et al. Improving the response choices on the veterans SF-36 health survey role functioning scales: results from the veterans health study. J Ambul Care Manag. 2004;27(3):263–80.
Selim A, Rogers W, Qian S, Rothendler JA, Kent EE, Kazis LE. A new algorithm to build bridges between two patient-reported health outcome instruments: the MOS SF-36A (R) and the VR-12 Health Survey. Qual Life Res. 2018;27(8):2195–206.
Selim AJ, Rogers W, Fleishman JA, Qian SX, Fincke BG, Rothendler JA, et al. Updated US population standard for the Veterans RAND 12-item Health Survey (VR-12). Qual Life Res. 2009;18(1):43–52.
Jenkins NW, Parrish JM, Nolte MT, Hrynewycz NM, Brundage TS, Singh K. Validating the VR-12 physical function instrument after anterior cervical discectomy and fusion with SF-12, PROMIS, and NDI. HSS J. 2020;16(2_suppl):443–51.
AlKhatib HS, Brazeau G, Akour A, Almuhaissen SA. Evaluation of the effect of items’ format and type on psychometric properties of sixth year pharmacy students clinical clerkship assessment items. BMC Med Educ. 2020;20(1):190.
Maydeu-Olivares A, Kramp U, García-Forero C, Gallardo-Pujol D, Coffman D. The effect of varying the number of response alternatives in rating scales: experimental evidence from intra-individual effects. Behav Res Methods. 2009;41(2):295–308.
Lee A, Oakley Browne M, Villanueva E. Consequences of using SF-12 and RAND-12 when examining levels of well-being and psychological distress. Aust N Z J Psychiatry. 2008;42(4):315–23.
Buchholz I, Feng Y-S, Buchholz M, Kazis LE, Kohlmann T. Translation and adaptation of the German version of the Veterans Rand-36/12 Item Health Survey. Health Qual Life Outcomes. 2021;19(1):137–137.
Schalet BD, Rothrock NE, Hays RD, Kazis LE, Cook KF, Rutsohn JP, et al. Linking physical and mental health summary scores from the veterans RAND 12-Item Health Survey (VR-12) to the PROMIS((R)) Global Health Scale. J Gen Intern Med. 2015;30(10):1524–30.
Kazis L, Rogers W, Rothendler J, Qian S, Selim A. Scoring of the VR-12© to Best Match Scores of the SF-12v2® in the Medical Expenditure Panel Survey. Boston University Technical Report to the Agency for Health Care Research and Quality (AHRQ); 2019.
Li S, Fong DYT, Wong JYH, McPherson B, Lau EYY, Huang L, et al. Noise sensitivity associated with nonrestorative sleep in Chinese adults: a cross-sectional study. BMC Public Health. 2021;21(1):643.
Li S, Fong DYT, Wong JYH, McPherson B, Lau EYY, Huang L, et al. Indoor nocturnal noise is associated with body mass index and blood pressure: a cross-sectional study. BMC Public Health. 2021;21(1):815.
Li S, Fong DYT, Wong JYH, McPherson B, Lau EYY, Ip MSM. The association between nonrestorative sleep and health-related quality of life in Chinese adults: a cross-sectional study. Qual Life Res. 2021;30:2521–30.
Fong DYT, Lam CLK, Mak KK, Lo WS, Lai YK, Ho SY, et al. The Short Form-12 Health Survey was a valid instrument in Chinese adolescents. J Clin Epidemiol. 2010;63(9):1020–9.
Lam ET, Lam CL, Fong DY, Huang WW. Is the SF-12 version 2 Health Survey a valid and equivalent substitute for the SF-36 version 2 Health Survey for the Chinese? J Eval Clin Pract. 2013;19(1):200–8.
Saris-Baglama RN, Deway CJ, Chisholm GB, Kosinsk M, Bjorner J, Ware J. SF health outcomes scoring software user’s guide. Johnston: Quality Metric Inc; 2004.
Boston University. Translations. https://www.bu.edu/sph/about/departments/health-law-policy-and-management/research/vr-36-vr-12-and-vr-6d/about-the-vr-36-vr-12-and-vr-6d/translations/. Accessed 13 Aug 2021.
Boston University. Scoring and Population Norms. https://www.bu.edu/sph/about/departments/health-law-policy-and-management/research/vr-36-vr-12-and-vr-6d/how-to-use-the-instruments/scoring-and-population-norms/. Accessed 13 Aug 2021.
Maruish ME. User’s manual for the SF-36v2 health survey. Johnston: Quality Metric Incorporated; 2011.
Fong DYT, Wong JYH, Choi EPH, Lam KF, Kwok C. The English and Chinese language versions of the Short Form 12-item Health Survey are equivalent. Health Qual Life Outcomes. 2021;19(1):14.
Giavarina D. Understanding Bland Altman analysis. Biochem Medica. 2015;25(2):141–51.
Altman DG, Bland JM. Measurement in medicine: the analysis of method comparison studies. J R Stat Soc Ser D (Stat). 1983;32(3):307–17.
Gilat R, Haunschild ED, Patel S, Yang J, DeBenedetti A, Yanke AB, et al. Understanding the difference between symptoms of focal cartilage defects and osteoarthritis of the knee: a matched cohort analysis. Int Orthop. 2021;45(7):1761–6.
Gornet MF, Copay AG, Sorensen KM, Schranck FW. Assessment of health-related quality of life in spine treatment: conversion from SF-36 to VR-12. Spine J. 2018;18(7):1292–7.
Pekruna R. Commentary: self-report is indispensable to assess students’ learning. Frontline Learn Res. 2020;8(3):185–93.
Montazeri A, Vahdaninia M, Mousavi SJ, Asadi-Lari M, Omidvari S, Tavousi M. The 12-item medical outcomes study short form health survey version 2.0 (SF-12v2): a population-based validation study from Tehran, Iran. Health Qual Life Outcomes. 2011;9:12.
Rose M, Bjorner JB, Becker J, Fries JF, Ware JE. Evaluation of a preliminary physical function item bank supported the expected advantages of the Patient-Reported Outcomes Measurement Information System (PROMIS). J Clin Epidemiol. 2008;61(1):17–33.
Funding
This study was funded by the Health and Medical Research Fund (Grant No. 14150801), the Food and Health Bureau, Hong Kong Special Administrative Region.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Fong DYT and Chan BKY. The first draft of the manuscript was written by Chan BKY and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Ethics approval of this study was obtained from the Institutional Review Board of the Unisversity of Hong Kong/Hospital Authority Hong Kong West Cluster (Ref. No.: UW17-011). Written informed consent was obtained from all individual participants included in the study.
Consent for publication
All authors read and approved final manuscript submission. All authors agree to publish this prepared manuscript and no other submission of this manuscript to other journal.
Competing interests
The authors declare no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fong, D.Y.T., Chan, B.K.Y., Li, S. et al. Average and individual differences between the 12-item MOS Short-form Health Survey version 2 (SF-12 V.2) and the veterans RAND 12-item Health Survey (VR-12) in the Chinese population. Health Qual Life Outcomes 20, 102 (2022). https://doi.org/10.1186/s12955-022-02010-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12955-022-02010-z