
Abstract
Background
HIV and Hepatitis C Virus (HCV) infections are responsible for a significant burden of mortality and morbidity, particularly in developing countries. This study sought to determine the prevalence of HIV and Hepatitis C among injecting drug users in Afghanistan, Iran, and Pakistan.
Methods
This review conforms to the Preferred Reporting Guidelines for Systematic Reviews and Meta-Analysis (PRISMA) statement. Databases including PubMed, Scopus, Web of Science/Knowledge, SID.ir, and MAGIRAN were searched. Studies that were published from 2003 up to 2018 were considered for analysis. Studies were screened for inclusion in duplicate, and also, that data were narratively synthesized.
Results
We report on data from 79 articles. The total number of participants in studies that assessed the prevalence of HIV among injecting drug users included 68,926 participants, while those from studies that assessed HCV prevalence were 23,016 participants. Overall HIV and HCV prevalence among injecting drug users in the three selected countries were 9.1% (95% CI 6.9–12.0%) and 48.3% (95% CI 43.9–52.7%), respectively. Iran had the highest HIV prevalence of 11.0% among injectable drug users (95% CI 8.4–14.2%), while Afghanistan had the lowest HIV prevalence of 3.1% (95% CI 1.5–6.3%) among three selected countries. In Pakistan, the prevalence of HIV was 8.6% (95% CI 4.8–15.0%). Regarding HCV prevalence, Pakistan had the highest while Afghanistan had the lowest, 54.4% (95% CI 33.5–73.9%) and 37.3% (95% CI 35.2–39.4%), respectively. HCV prevalence in Iran was 47.7% (95% CI 43.4–52.0%).
Conclusion
Injecting drug users form a special cohort of persons at risk of HIV and Hepatitis C infections. The prevalence of HIV and Hepatitis noted from our findings is significantly high. Awareness of the grave risk of spreading HIV and Hepatitis C associated with sharing needles is recommended among this sub-group of drug users.
Similar content being viewed by others

Background
HIV and Hepatitis C Virus (HCV) infections are among the most significant public health challenges globally. They bear a significant burden of mortality and morbidity, particularly in developing countries. In 2017, WHO reported that 36.9 million people were living with HIV globally with record of 940,000 deaths [1]. HIV suppresses the immune system, in so doing, it makes the infected person susceptible to infectious diseases that may lead to death [2]. HIV can also invade the central nervous system that leads to severe neurological problems [3]. With regard to HCV, there are 177.5 million infected adults globally and up to 0.5 million deaths every year. Hepatitis due to HCV has the potential to become chronic, consequently leading to cirrhosis of the liver which may cause liver cancer and death [4]. Both HIV and HCV can be spread through body fluids. Certain behaviors like sharing injection equipment can lead to transmission of such pathogens[3, 5].
Estimates have indicated that, in Afghanistan, 5900 people living with HIV, in Iran and Pakistan 60,000 and 150,000 people living with HIV, respectively [1]. The prevalence of HCV in Afghanistan according to a systematic review in 2015 was estimated to be 0.7% among the general population [6]. In Pakistan and Iran, the prevalence of HCV among the general population was 4.8% and 0.3%, respectively [7, 8]. HCV and HIV are heavily associated with injecting drug users (IDUs) are highly susceptible to transmission of HIV and HCV through sharing sharp materials such as infected needles/syringes[9].
Globally, there are approximately 13 million IDUs; of these, estimates have shown that 1.7 million are infected with HIV[1, 10]. In addition, approximately 10% of HIV infections are transmitted through sharing materials during injectable drug usage. Concerning HCV, the prevalence of HCV among injecting drug users is estimated at 67% globally. Co-infection of HCV and HIV accounts for about 2.2 million people, with more than half of these being among IDUs [1].
Furthermore, Aceijas and colleagues (2007) revealed that about 50% of IDUs were HCV positive in 49 countries. Prevalence of HCV was reported with significant variance from 2% up to 100% [11]. There was no study assessing the extent of HIV and HCV among IDUs in the WHO-EMRO region to the best of our knowledge. Needless to say, this region has profound significance concerning drug production and usage. In fact, Afghanistan is the leading producer of opium in the world [12]. This does not only influence drug usage; it has a fundamental role in distribution chains to other countries, especially those in the neighborhood, particularly Pakistan and Iran.
Moreover, decades of political instability in this region have caused millions of people to migrate to Iran and Pakistan. This said trafficking of drugs goes hand in hand with the movement of people between borders. This can increase the risk of transmission of disease between countries specifically among IDUs relative to other regions of the world.
Prevention efforts among IDUs which focus only on individual behavior modification are likely to result in only a partial decrease in HIV and HCV transmission. To tackle this problem effectively, there is a need for regional interventions at the macro-level. In order to have a collaborative effort toward controlling HIV and HCV among IDUs in an effective manner, baseline data are needed. To serve this goal, we performed a systematic review of studies in these three countries.
Review Question
What is the prevalence of HIV and HCV among IDUs in Afghanistan, Pakistan, and Iran?
Methods
Protocol This review conforms to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement (Moher, 2009). To ensure that there was no similar work to ours, we did a preliminary scoping search in the International prospective registers of systematic reviews (PROSPERO), Cochrane Library, and Google scholar. The search was done on 1/12/2020.
Eligibility criteria Studies that reported the prevalence of HIV and HCV among injecting drug users published in English and Persian languages in peer-review Journals from 2003 up to 2018 in Afghanistan, Pakistan, and Iran were included (see Table 1).
Databases Articles were searched in PubMed, Scopus, Web of Science, Embase, SID.ir, and MAGIRAN.
Search strategy Keywords included “Human Immunodeficiency Virus” “Hepatitis C Virus,” “Substance abuse,” “Injecting Drug User,” “Injecting Drug Abuser,” “Intravenous Drug Abuse” “Drug Misuse,” “Drug Abuse,” “Drug Dependence,” “Afghanistan,” “Pakistan,” and “Iran” from 2003 up to 2018 (Table 2). The reference lists of the selected articles were also hand-searched to find additional relevant studies.
Study selection We created an endnote (version X.7) Library to store and manage the references. Two reviewers independently search for the articles compared to their articles found and always reached consensus on studies to exclude or include based on the inclusion criteria described above.
Data collection process For articles that met the inclusion criteria, information was extracted and recorded in piloted data set in an excel spreadsheet. For included studies, we assessed the study findings' main outcome, including the prevalence of HIV or HCV. Selected articles were kept for future narrative, and excluded articles were also kept in a separate file for future reference was appropriate. The following items were extracted from studies: author, country, year, study design, setting, sample size, and HIV or HCV prevalence.
Risk of bias in individual studies The studies were appraised based on the selection criteria (Table 1) and the Joanna Briggs Institute (JBI) critical appraisal tool for systematic reviews checklist for prevalence studies [13]. This tool is a rating list with nine criteria, which can be answered as yes (coded as 1), no (coded as 0), not applicable (coded as NA), or unclear (coded as?); thus, the score for each study ranged from 0 to 9. Depending on its score, we rated each study as low risk [7,8,9], moderate risk [4,5,6], or high risk of bias [1,2,3].
Data analysis We used a Random Effects model to estimate the pooled prevalence. The result was displayed in a forest plot and shown high heterogeneity. Our review resulted in 83 peer-review articles from three countries concentrated on HIV and HCV prevalence. Data were reported as the proportion of the infected numbers among total injecting drug users. Prevalence from each article was collected in the form of a table (Table 3, 4, and 5) and then inserted in Comprehensive Meta-Analysis (CMA) version 3. The pooled prevalence of HIV and HCV was calculated with a 95% confidence interval and stratified by country.
Results
Characteristics and quality of included studies
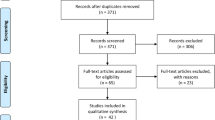
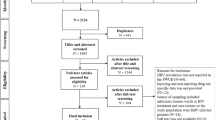
In this review, 116 studies were screened, and 79 articles were included for data extraction (Fig. 1), 57 studies from Iran, 18 from Pakistan, and four from Afghanistan. The total number of participants in studies that assessed the prevalence of HIV among IDUs included 68,926 participants, while those from studies that assessed the prevalence of HCV were 23,016 participants. The study of Emmanuel (2013) contributed the highest number of participants (n = 46,351). Most studies identified were conducted in Iran. The majority of studies in Iran were carried out in non-community settings such as health centers and prisons. Those conducted in Pakistan and Afghanistan were carried out in community settings. All studies used a cross-sectional study design (Table 3 and 4). In Iran, the country-level analysis revealed that 17,261 IDUs were identified for HIV prevalence analysis while 17,894 participants were included in HCV analysis. In Pakistan, 49,547 IDUs were included in HIV studies, while 3004 participants were identified for the HCV prevalence analysis. In Afghanistan, a total of 2118 IDUs were included in both HIV and HCV prevalence analysis. Co-infection was reported in 15 articles with 5252 participants in three countries. Tables 3, 4, and 5 show the prevalence of HIV, HCV, and co-infection from studies identified in the three selected countries. The JBI assessment tool showed that 58 articles were with low risk of bias, 20 with moderate, and 1 with a high risk of bias (Table 3 and 4).

PRISMA flow diagram
Prevalence of HIV and HCV in Iran, Pakistan, and Afghanistan
Overall, HIV and HCV prevalence among IDUs in the three selected countries were 9.1% (95% CI 6.9–12.0%) and 48.3% (95% CI 43.9–52.7%), respectively. In country level analysis, Iran had the highest HIV prevalence among IDUs while Afghanistan had the lowest among three selected countries, 11.0% (95% CI 8.4–14.2%) and 3.1% (95% CI 1.5–6.3%), respectively. In Pakistan, the prevalence of HIV was 8.6% (95% 4.8–15.0%).
With respect to HCV prevalence, Pakistan had the highest prevalence while Afghanistan had the lowest, 54.4% (95% CI 33.5–73.9%) and 37.3% (95% CI 35.2–39.4%), respectively. HCV prevalence in Iran was 47.7% (95% CI 43.4–52.0%). Co-infection of HIV and HCV in three selected countries was 7.6% (95% CI 4.4–12.8%).
Publication bias
There was no significant publication bias on HCV rate as shown by the result of the Egger test (P = 0.1), while there was publication bias on HIV rate (P = 0.001).
Discussion
We present seminal evidence on the prevalence of HIV and HCV among IDUs in three selected countries in the EMRO-WHO region. These countries are in the neighborhood of each other. The pooled prevalence of HIV and HCV was assessed separately using country-level findings.
HCV prevalence rate was significantly high in the three selected countries; overall prevalence was 48.3% (95% CI 43.9–52.7%). We report an overall average HIV prevalence of 9.1% (95% CI 6.9–12.0%). We acknowledge the fact that most studies have been done mainly in Iran. Indeed, a review of HIV among IDUs in the Middle East and North Africa also indicated that only Iran had a substantial number of studies on this subject [14]. Nonetheless, similar studies have reported a higher prevalence of HIV in Iran 15% [5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25], Pakistan 10.8% (9.6–12.1), and Afghanistan 3.4% (1.7–5.1) [15]. These estimates are similar to the findings of our review.
Another systematic review that sought to estimate the global prevalence of HCV infection among IDUs revealed that HCV prevalence among IDUs in Pakistan ranged from 78 to 93%, while that in Iran ranged from 54.9 to 80.1% [11]. This is inconsistent with our finding primarily due to differences regarding sources of information that were used. This could be attributed to the time difference and grey literature considered in the former review. Those studies were done a decade ago, and also substantial numbers of grey literature and experts' views were included in the analysis. Noteworthy, in our study, we used only peer-reviewed articles; however, the former reviews considered various sources, including peer-reviewed papers, reports from relevant organizations, books and booklets, slides, press articles, and personal communiqués. These provide a broad scope of findings; however, they are liable to systematic bias associated with such designs.
The large range estimates reflect uncertainty about estimates derived from these studies. Secondly, the time difference between these studies may affect the results.
The variability among countries in terms of the number of studies that reported prevalence of HIV and HCV among IDUs might be due to varied research capacity across the three selected countries and varying investment in research capacity building. This issue may be a basis to initiate collaborations aimed at capacity building. Moreover, it could serve as a turning point and priority for tackling various public health challenges.
Regarding the geographical scope of the studies, nearly all of the included articles in our review were from the largest cities of these three selected countries. This is in one way reflective of the availability of resources in these cities and, on the other hand, imbalanced research attention to countrysides. The Iceberg term can be used for this situation due to those geographic areas that are deprived of resources. In order to have a clear picture of the situation, we need studies with larger sample sizes. These should also include different geographical areas.
The available evidence has emphasized that HIV and HCV infections represented a major adverse health consequence among IDUs. This causes a considerable health burden in this region. Our review is the first research of its kind that illustrates HIV and HCV rates among IDUs in the context of three neighboring countries that are highly implicated in drug smuggling and production globally. Comprehensive public health interventions are required to address this problem nationally and internationally.
However, the limitation of the study should be considered in the time of using the findings, in which grey literature was not included in the study. Due to the low capacity of research, especially in Afghanistan, this could influence the result and hide the actual rate of HIV and HCV among IDUs.
Conclusions
Our review revealed that the prevalence of HIV and HCV is significantly high among IDUs in Iran, Afghanistan, and Pakistan. Injecting drug users are at high risk of HIV and HCV transmission and can spread infections to the community due to unhealthy behavior, including syringe change and unsafe sex. Therefore, interventions are required at different levels of prevention for this high-risk group.
Availability of data and material
Not applicable for this study.
Abbreviations
- HIV:
-
Human immunodeficiency virus
- HCV:
-
Hepatitis C Virus
- IDUs:
-
Injecting drug users
- WHO-EMRO:
-
World Health Organization-East Mediterranean Regional Office
References
WHO. HIV/AIDS. Website. 2018.
Grossman Z, Meier-Schellersheim M, Paul WE, Picker LJ. Pathogenesis of HIV infection: what the virus spares is as important as what it destroys. Nat Med. 2006;12(3):289.
Long H. What is AIDS? Med Care. 2001;916:874–7720.
Petruzziello A, Marigliano S, Loquercio G, Cozzolino A, Cacciapuoti C. Global epidemiology of hepatitis C virus infection: an up-date of the distribution and circulation of hepatitis C virus genotypes. World J Gastroenterol. 2016;22(34):7824.
Bostan N, Mahmood T. An overview about hepatitis C: a devastating virus. Crit Rev Microbiol. 2010;36(2):91–133.
Chemaitelly H, Mahmud S, Rahmani AM, Abu-Raddad LJ. The epidemiology of hepatitis C virus in Afghanistan: systematic review and meta-analysis. Int J Infect Dis. 2015;40:54–63.
Mahmud S, Akbarzadeh V, Abu-Raddad LJ. The epidemiology of hepatitis C virus in Iran: systematic review and meta-analyses. Sci Rep. 2018;8(1):150.
Qureshi H, Bile K, Jooma R, Alam S, Afrid H. Prevalence of hepatitis B and C viral infections in Pakistan: findings of a national survey appealing for effective prevention and control measures. 2010.
Nasir A, Todd CS, Stanekzai MR, Bautista CT, Botros BA, Scott PT, et al. Prevalence of HIV, hepatitis B and hepatitis C and associated risk behaviours amongst injecting drug users in three Afghan cities. Int J Drug Policy. 2011;22(2):145–52.
Aceijas C, Stimson GV, Hickman M, Rhodes T. Global overview of injecting drug use and HIV infection among injecting drug users. AIDS. 2004;18(17):2295–303.
Aceijas C, Rhodes T. Global estimates of prevalence of HCV infection among injecting drug users. Int J Drug Policy. 2007;18(5):352–8.
Todd CS, Nasir A, Stanekzai MR, Fiekert K, Rasuli MZ, Vlahov D, et al. Prevalence and correlates of HIV, syphilis, and hepatitis B and C infection and harm reduction program use among male injecting drug users in Kabul, Afghanistan: a cross-sectional assessment. Harm Reduct J. 2011;8(1):22.
Munn Z, Moola S, Riitano D, Lisy K. The development of a critical appraisal tool for use in systematic reviews addressing questions ofprevalence. Int J Health Policy Manag. 2014;3(3):123–8. https://doi.org/10.15171/ijhpm.2014.71.
Mumtaz GR, Weiss HA, Thomas SL, Riome S, Setayesh H, Riedner G, et al. HIV among people who inject drugs in the Middle East and North Africa: systematic review and data synthesis. PLoS Med. 2014;11(6):e1001663.
Mathers BM, Degenhardt L, Phillips B, Wiessing L, Hickman M, Strathdee SA, et al. Global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review. Lancet. 2008;372(9651):1733–45.
Rahimi-Movaghar A, Razaghi EM, Sahimi-Izadian E, Amin-Esmaeili M. HIV, hepatitis C virus, and hepatitis B virus co-infections among injecting drug users in Tehran, Iran. Int J Infect Dis. 2010;14(1):e28–33.
Khajehkazemi R, Osooli M, Sajadi L, Karamouzian M, Sedaghat A, Fahimfar N, et al. HIV prevalence and risk behaviours among people who inject drugs in Iran: the 2010 National Surveillance Survey. Sex Transm Infect. 2013:sextrans-2013-051204.
Javadi A, Ataei B, Yaran M, Nokhodian Z, Kassaian N, Tayeri K, et al. Prevalence of HIV infection and related risk factors in Isfahan Drop in Centers. 2013.
Imani R, Karimi A, Rouzbahani R, Rouzbahani A. Seroprevalence of HBV, HCV and HIV infection among intravenous drug users in Shahr-e-Kord, Islamic Republic of Iran. East Mediterr Health J. 2008;14(5):1136–41.
Zamani S, Ichikawa S, Nassirimanesh B, Vazirian M, Ichikawa K, Gouya MM, et al. Prevalence and correlates of hepatitis C virus infection among injecting drug users in Tehran. Int J Drug Policy. 2007;18(5):359–63.
Khani M, Vakili MM. Prevalence and risk factors of HIV, hepatitis B virus and hepatitis C virus infections in drug addicts among Zanjan prisoners. 2003.
Mirahmadizadeh AR, Majdzadeh R, Mohammad K, Forouzanfar M. Prevalence of HIV and hepatitis C virus infections and related behavioral determinants among injecting drug users of drop-in centers in Iran. 2009.
Davoodian P, Dadvand H, Mahoori K, Amoozandeh A, Salavati A. Prevalence of selected sexually and blood-borne infections in Injecting drug abuser inmates of bandar abbas and roodan correction facilities, Iran, 2002. Braz J Infect Dis. 2009;13(5):356–8.
Hosseini M, SEYED ANS, KHEYR AP, ESMAEILI JGR, Shirzad H, Karami N, et al. Prevalence and correlates of co-infection with human immunodeficiency virus and hepatitis C virus in male injection drug users in Iran. 2010.
Malekinejad M, Mohraz M, Razani N, Akbari G, McFarland W, Khairandish P, et al. High HIV prevalence in a respondent-driven sampling survey of injection drug users in Tehran, Iran. AIDS Behavior. 2015;19(3):440–9.
Nikkhooy A, Nikkhooy M, Saadati N. Determination of relative frequency of HBS Ag, HCV and HIV antibodies serum markers among admitted intravenous drug users in infectious disease ward of Razi Hospital in Ahvaz, 2004–2005. J Health Res. 2012;1(1):26–33.
Parvin kazerouni. Prevalence of human immunodeficiency virus infection and related risk factors among injective substance abusers in Shiraz, Southern part of Iran. J Fund Mental Health. 2009;11(43): 175–184. [Persian]
Aminzadehv Z, Sarhangi KA. Seroepidemiology of HIV, syphilis, Hepatitis B and C in intravenous drug users at Loghman Hakim hospital. Iran J Med Microbiol. 2007;1(3):53–6.
Moradi AR, Emdadi A, Soori B, Mostafavi E. Prevalence of Human Immunodeficiency Virus Infection among Injection Drug Users Released from Jail. Addict Health. 2012;4(3–4):151.
Kheirandish P, SeyedAlinaghi S, Jahani M, Shirzad H, Ahmadian MS, Majidi A, et al. Prevalence and correlates of hepatitis C infection among male injection drug users in detention, Tehran, Iran. J Urban Health. 2009;86(6):902.
Zamani S, Kihara M, Gouya MM, Vazirian M, Ono-Kihara M, Razzaghi EM, et al. Prevalence of and factors associated with HIV-1 infection among drug users visiting treatment centers in Tehran, Iran. AIDS. 2005;19(7):709–16.
Ramezani A, Amirmoezi R, Volk JE, Aghakhani A, Zarinfar N, McFarland W, et al. HCV, HBV, and HIV seroprevalence, coinfections, and related behaviors among male injection drug users in Arak, Iran. AIDS Care. 2014;26(9):1122–6.
Sofian M, Aghakhani A, Banifazl M, Azadmanesh K, Farazi A-A, McFarland W, et al. Viral hepatitis and HIV infection among injection drug users in a central Iranian City. J Addict Med. 2012;6(4):292–6.
Kuo I, Galai N, Thomas DL, Zafar T, Ahmed MA, Strathdee SA. High HCV seroprevalence and HIV drug use risk behaviors among injection drug users in Pakistan. Harm Reduct J. 2006;3(1):26.
Emmanuel F, Archibald C, Razaque A, Sandstrom P. Factors associated with an explosive HIV epidemic among injecting drug users in Sargodha, Pakistan. JAIDS J Acquired Immune Deficiency Syndromes. 2009;51(1):85–90.
Alipour A, Haghdoost AA, Sajadi L, Zolala F. HIV prevalence and related risk behaviours among female partners of male injecting drugs users in Iran: results of a bio-behavioural survey, 2010. Sexually transmitted infections. 2013;89(Suppl 3):iii41–4.
Achakzai M, Kassi M, Kasi PM. Seroprevalences and co-infections of HIV, hepatitis C virus and hepatitis B virus in injecting drug users in Quetta, Pakistan. Trop Doctor. 2007;37(1):43–5.
Todd CS, Abed AM, Strathdee SA, Scott PT, Botros BA, Safi N, et al. HIV, hepatitis C, and hepatitis B infections and associated risk behavior in injection drug users, Kabul, Afghanistan. Emerg Infect Dis. 2007;13(9):1327.
Alavi SM, Behdad F. Seroprevalence study of hepatitis C and Hepatitis B virus among hospitalized intravenous drug users in Ahvaz, Iran (2002–2006). Hepat Mon. 2010;10(2):101.
Mir-Nasseri MM, Poustchi H, Nasseri-Moghadam S, Tavakkoli H, Mohammadkhani A, Afshar P, et al. Hepatitis C seroprevalence among intravenous drug users in Tehran. J Res Med Sci. 2008;13(6):295–302.
Mir-Nasseri MM, Poustchi H, Nasseri-Moghadam S, Nouraie SM, Tahaghoghi S. Afshar P, Mohammadkhani A, Tavakoli H, Malekzadeh R. HCV Intravenous Drug Users Govaresh. 2005;10(2):80–122.
Alireza Kaffashian , zari Nokhodian , Nazila Kassaian , Anahita Babak , Majid Yaran , Parisa Shoaei , Behrooz Ataei , Peyman Adibi. The Experience of Hepatitis C Screening among Prison Inmates with Drug Injection History ; Vol 28 (Special Issue on Hepatitis C):1565–1571.
Behrooz Ataei, Anahita Babak, Majid Yaran, Nazila Kassaian, Zari Nokhodian, Marjan Meshkati, Peyman Adibi. Hepatitis C in Intravenous Drug Users: Seroprevalence and Risk Factors. Journal of Isfahan Medical School. 2011; Vol 28 (Special Issue on Hepatitis C):1537–1545.
Amin-Esmaeili M, Rahimi-Movaghar A, Razaghi EM, Baghestani AR, Jafari S. Factors correlated with hepatitis C and B virus infections among injecting drug users in Tehran, IR Iran. Hepat Mon. 2012;12(1):23.
Nokhodian Z, Meshkati M, Adibi P, Ataei B, Kassaian N, Yaran M, et al. Hepatitis C among intravenous drug users in Isfahan, Iran: a study of seroprevalence and risk factors. Int J Prev Med. 2012;3(Suppl1):S131.
Alavi SM, Etemadi A. HIV/HBV, HIV/HCV and HIV/HTLV-1 co infection among injecting drug user patients hospitalized at the infectious disease ward of a training hospital in Iran. Pak J Med Sci. 2007;23(4):510.
ur Rehman L, Ullah I, Ali I, Khan IA, Iqbal A, Khan S, et al. Active hepatitis C infection and HCV genotypes prevalent among the IDUs of Khyber Pakhtunkhwa. Virol J. 2011;8(1):327.
Akhtar AM, Majeed S, Jamil M, Rehman A, Majeed S. Hepatitis-C virus infection among injecting drug users in Lahore, Pakistan: A cross sectional study. Pak J Med Sci. 2016;32(2):373.
Khorvash F, Dastjerdi Fasihi M, Emami Naeini A.R. Paraclinical disorders and prevalence of viral infections in inection drug users. J Qazuin Univ Med Sci. Summer 2009.
Sarveqad MR, Nadiri HR. Farokhniya M, Bajadi A. assessment of infectiouns among injecting drug users at Department of infectious disease, Amam Reza Hospital, Mashhad. Med J Mashhad Univ Med Sci. Spring 2005.
Rahbar AR, Rooholamini S, Khoshnood K. Prevalence of HIV infection and other blood-borne infections in incarcerated and non-incarcerated injection drug users (IDUs) in Mashhad, Iran. Int J Drug Policy. 2004;15(2):151–5. https://doi.org/10.1016/j.drugpo.2003.07.001.
Zamani S, Radfar R, Nematollahi P, Fadaie R, Meshkati M, Mortazavi S, Kihara M, et al. Prevalence of HIV/HCV/HBV infections and drug-related risk behaviours amongst IDUs recruited through peer-driven sampling in Iran. Int J Drug Policy. 2010;21(6):493–500. https://doi.org/10.1016/j.drugpo.2010.04.006.
Zadeh AOT, SeyedAlinaghi SA, Hassanzad FF, Hajizadeh M, Mohamadi SN, Emamzadeh-Fard S, Hosseini M, et al. Prevalence of HIV infection and the correlates among homeless in Tehran, Iran. Asian Pac J Trop Biomed. 2014;4(1):65–8. https://doi.org/10.1016/S2221-1691(14)60210-0.
Ghasemian R, Najafi N, Amirkhanloo K. The study of infections due to injection drug abuse in the injecting drug users hospitalized at Imam Khomeini Hospital in Sari and Razi Hospital in Ghaemshahr in 2007–2009. J Mazandaran Univ Med Sci. 2011;21(83):9–15.
Alavi SM, Nadimi M, Shokri S, Zamani G. Seroepidemiology of human immunodeficiency virus in Illicit substance users in Ahvaz, Iran: 2005–2006. Jundishapur J Microbiol. 2012;5(3):474–8. https://doi.org/10.5812/jjm.3446.
Dibaj R, Ataei B, Yaran M, Nokhodian Z, Tayeri K, Ali Z. Prevalence of HIV infection in inmates with history of injection drug use and evaluation of risk factors, in Isfahan, Iran. Pak J Med Sci. 2013;29(1 SUPPL):399–402. https://doi.org/10.12669/pjms.291(Suppl).3542.
Ilami O, Sarkari B, Khosravani A, Tori MA, Hosseini Z. HIV seroprevalence among high-risk groups in kohgiloyeh and boyerahmad province, Southwest of Iran, a behavioral surveillance survey. AIDS Behav. 2012;16(1):86–90. https://doi.org/10.1007/s10461-010-9874-x.
Alizadeh AHM, Alavian SM, Jafari K, Yazdi N. Prevalence of hepatitis C virus infection and its related risk factors in drug abuser prisoners in Hamedan - Iran. World J Gastroenterol. 2005;11(26):4085–9. https://doi.org/10.3748/wjg.v11.i26.4085.
Mir-Nasseri MM, Mohammadkhani A, Tavakkoli H, Ansari E, Poustchi H. Incarceration is a major risk factor for blood-borne infection among intravenous drug users. Hepat Mon. 2011;11(1):19–22.
Sharif M, Sherif A, Sayyah M. Frequency of HBV, HCV and HIV infections among hospitalized injecting drug users in Kashan. Indian J Sexu Transm Dis. 2009;30(1):28–30. https://doi.org/10.4103/0253-7184.55477.
Khodadadizadeh A, Esmaeili-Nadimi A, Hosseini SH, Shabani-Shahrbabaki Z. The Prevalence of HIV, HBV and HCV in Narcotic addicted Persons Referred to the out Patient Clinic of Rafsanjan University of Medical Sciences in 2003. J Rafsanjan Univ Med Sci. 2006;1(5):23–30.
Hashemipour M, Nokhodian Z, Yaran M, Ataei B, Tayeri K, Nobari RF, Ali Z. Prevalence of HIV infection in individuals with history of intravenous drug use via community announcement in Isfahan-Iran. Pak J Med Sci. 2013;29(1 SUPPL):395–8. https://doi.org/10.12669/pjms.291(Suppl).3541.
Sharifi-Mood B, Metanat M. Infection among hospitalized injection drug users. J Med Sci. 2006;6(4):686–9. https://doi.org/10.3923/jms.2006.686.689.
Bokhari A, Nizamani NM, Jackson DJ, Rehan NE, Rahman M, Muzaffar R, Thaver I, et al. HIV risk in Karachi and Lahore, Pakistan: An emerging epidemic in injecting and commercial sex networks. Int J STD AIDS. 2007;18(7):486–92. https://doi.org/10.1258/095646207781147201.
Platt L, Vickerman P, Collumbien M, Hasan S, Lalji N, Mayhew S, Hawkes S et al. Prevalence of HIV, HCV and sexually transmitted infections among injecting drug users in Rawalpindi and Abbottabad, Pakistan: evidence for an emerging injection-related HIV epidemic. Sex Transm Infect. 2009. https://doi.org/10.1136/sti.2008.034090
Khanani MR, Ansari AS, Khan S, Somani M, Kazmi SU, Ali SH. Concentrated epidemics of HIV, HCV, and HBV among Afghan refugees. J Infect. 2010;61(5):434–7. https://doi.org/10.1016/j.jinf.2010.08.009.
Emmanuel F, Salim M, Akhtar N, Arshad S, Reza TE. Second-generation surveillance for HIV/AIDS in Pakistan: results from the 4th round of Integrated Behavior and Biological Survey 2011–2012. Sex Transm Infect. 2013;89(SUPPL. 3):23–8. https://doi.org/10.1136/sextrans-2013-051161.
Eskandarieh S, Nikfarjam A, Tarjoman T, Nasehi A, Jafari F, Saberi-Zafarghandi MB. Descriptive aspects of injection drug users in Iran’s national harm reduction program by methadone maintenance treatment. Iran J Public Health. 2013;42(6):588.
Jat MI, Rind GR. Frequency of Hbv, Hcv, and Hiv among injection drug users (Idus), and co-relation with socioeconomic status, type use and duration of substance use. Prof Med J. 2019;26(07):1147–50. https://doi.org/10.29309/tpmj/2019.26.07.3788.
Abbasi S, Faqir F, Khan S, Zaidi SK, Ahmed SQ, Abdulsattar MS. A serological study of hepatitis C and human immunodeficiency virus in a cohort of intravenous drug users in Quetta, Balochistan. JPMI - J Postg Med Inst. 2009;23(1):3–6.
Ruiseñor-Escudero H, Wirtz AL, Berry M, Mfochive-Njindan I, Paikan F, Yousufi HA, Vu A, et al. Risky behavior and correlates of HIV and Hepatitis C Virus infection among people who inject drugs in three cities in Afghanistan. Drug Alcohol Depend. 2014;143(1):127–33. https://doi.org/10.1016/j.drugalcdep.2014.07.022.
Amiri ZM, Rezvani M, Shakib RJ, Shakib AJ. Prevalence of hepatitis C virus infection and risk factors of drug using prisoners in Guilan province. EMHJ-Eastern Mediterranean Health J. 2007;13(2):250–6.
Nobari RF, Meshkati M, Ataei B, Yazdani MR, Heidari K, Kassaian N, Adibi P, et al. Identification of patients with hepatitis c virus infection in persons with background of intravenous drug use: The first community announcementbased study from Iran. Int J Prev Med. 2012;3(4):170–5.
Honarvar B, Odoomi N, Moghadami M, Kazerooni PA, Hassanabadi A, Dolatabadi PZ, Farzanfar E, Lankarani KB. Blood-borne hepatitis in opiate users in iran: a poor outlook and urgent need to change nationwide screening policy. PLoS ONE. 2013;8(12):82230.
Alavi SM, Alavi L. Seroprevalence study of HCV among hospitalized intravenous drug users in Ahvaz, Iran (2001–2006). J Infect Public Health. 2009;2(1):47–51. https://doi.org/10.1016/j.jiph.2009.01.001.
Kassaian N, Adibi P, Kafashaian A, Yaran M, Nokhodian Z, Shoaei P, Ataei B, et al. Hepatitis C virus and associated risk factors among prison inmates with history of drug injection in Isfahan, Iran. Int J Prevent Med. 2012;3(Suppl1):S156.
Butt A, Jafri W, Janjua N, Pasha O. Seroprevalence and Risk Factors for Hepatitis C Infection among Male Prisoners in Karachi, Pakistan: 303. Am J Gastroenterol. 2010;105:S112.
Rehan N, Bokhari A, Nizamani NM, Jackson D, Naqvi HR, Qayyum K, Muzaffar R, et al. National study of reproductive tract infections among high risk groups of Lahore and Karachi. J College Phys Surg Pakistan. 2009;19(4):228–31. https://doi.org/10.2009/JCPSP.228231.
Ali I, Siddique L, Rehman LU, Khan NU, Iqbal A, Munir I, Aslam MS, et al. Prevalence of HCV among the high risk groups in Khyber Pakhtunkhwa. Virol J. 2011;8:2–5. https://doi.org/10.1186/1743-422X-8-296.
SeyedAlinaghi SA, Farhoudi B, Mohraz M, Pahlaviani FG, Hosseini M, Farnia M, Shahbazi M, Alasvand R, Tashakoriyan M. Prevalence and correlates of HIV infection among male prisoners in Tehran, Iran. Arch Iran Med. 2017;20(6).
Parviz S, Fatmi Z, Altaf A, McCormick JB, Fischer-Hoch S, Rahbar M, Luby S. Background demographics and risk behaviors of injecting drug users in Karachi. Pak Int J Infect Dis. 2006;10(5):364–71.
Altaf A, Shah SA, Zaidi NA, Memon A, Wray N. High risk behaviors of injection drug users registered with harm reduction programme in Karachi, Pakistan. Harm Reduct J. 2007;4(1):7.
Akram B, Ilyas M. Coping strategies, mental health and HIV status: Predictors of suicidal behaviour among PWIDs. JPMA. 2017;67(568).
Sharhani A, Mehrabi Y, Noroozi A, Nasirian M, Higgs P, Hajebi A, Hamzeh B, Khademi N, Noroozi M, Shakiba E, Etemad K. Hepatitis C virus seroprevalence and associated risk factors among male drug injectors in Kermanshah, Iran. Hepatitis Mon. 2017;17(10).
Rezaei F, Noroozi A, Armoon B, Farhoudian A, Massah O, Sharifi H, Ahounbar E, Khodadost M, Mohammadi F, Barkhordar N, Mansourian M. Social determinants and hepatitis C among people who inject drugs in Kermanshah, Iran: socioeconomic status, homelessness, and sufficient syringe coverage. J Substance Use. 2017 ;22(5):474–8.
Alavian SM, Mirahmadizadeh A, Javanbakht M, Keshtkaran A, Heidari A, Mashayekhi A, Salimi S, Hadian M. Effectiveness of methadone maintenance treatment in prevention of hepatitis C virus transmission among injecting drug users. Hepatitis Mon. 2013;13(8).
Ataei B, Meshkati M, Karimi A, Yaran M, Kassaian N, Nokhodian Z, Shoaei P, Adibi P. Hepatitis C screening in intravenuos drug users in golpayegan, Isfahan through Community Announcement: Pilot Study. Journal of Isfahan Medical School. 2011 ;29:28.
Keramat F, Eini P, Majzoobi MM. Seroprevalence of HIV, HBV and HCV in persons referred to hamadan behavioral counseling center, west of Iran. Iran Red Crescent Med J. 2011 ;13(1):42.
Mirnaseri S, Poustchi H, Naseri MS, Tavakoli H, Mohammad KA, Afshar P, Malekzadeh R. Hepatitis C seroprevalence among intravenous drug users in Tehran.
Moradi G, Gouya MM, Azimizan Zavareh F, Mohamadi Bolbanabad A, Darvishi S, Aghasadeghi MR, Nabavi M, Alasvand R, Tashakorian M, Nouri B, Rahmani K. Prevalence and risk factors for HBV and HCV in prisoners in Iran: a national bio-behavioural surveillance survey in 2015. Trop Med Int Health. 2018;23(6):641–9.
Waheed Y, Najmi MH, Aziz H, Waheed H, Imran M, Safi SZ. Prevalence of hepatitis C in people who inject drugs in the cities of Rawalpindi and Islamabad, Pakistan. Biomed Rep. 2017;7(3):263–6.
Acknowledgements
We wish to thank all scientists that have tremendously contributed to this field of research and, most importantly, those whose studies have been used in this review.
Funding
The authors declare that they received no funding for this project.
Author information
Authors and Affiliations
Contributions
SJS &RN contributed to curation and methodology. SJS, RN, and FK contributed to methodology, database search, data extraction, and writing the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable to this study.
Consent for publication
Not applicable for this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shayan, S.J., Nazari, R. & Kiwanuka, F. Prevalence of HIV and HCV among injecting drug users in three selected WHO-EMRO countries: a meta-analysis. Harm Reduct J 18, 59 (2021). https://doi.org/10.1186/s12954-021-00505-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12954-021-00505-4