
Abstract
Background
Injection drug use is associated with HIV and hepatitis C transmission, overdose, and other preventable harms. These harms are heightened for structurally vulnerable injection drug-using populations, as their social conditions pose barriers to safer injecting. Previous research on injection cessation has largely focused on adult drug-using populations. Little qualitative work has examined the social, structural, and environmental factors that shape periods of injection cessation among youth and young adults. Such research is essential to understanding how we can best reduce harms among this vulnerable population as they move in and out of periods of injection cessation.
Methods
We conducted 22 semi-structured, qualitative interviews with street-involved young people who use drugs (SY), focused on characterizing their transitions into periods of injection cessation and perceived barriers to injection cessation. Adopting an ethno-epidemiological approach, participants who had experienced at least 6 months of injection cessation were purposively recruited from an ongoing prospective cohort study of SY in Vancouver, Canada to participate in qualitative interviews. Qualitative interview findings were triangulated with the findings of a longitudinal program of ethnographic research with SY in this setting. This ethno-epidemiological approach allowed for a more robust exploration of contextual factors surrounding drug use patterns than would be possible through traditional epidemiological methods alone.
Results
Findings indicate that periods of injection cessation were influenced by access to harm reduction-informed youth-focused services, transitions in route of administration (e.g., from injecting methamphetamine to the smoking of methamphetamine), and the provision of housing and social supports (e.g., from friends, family, and care providers). Conversely, participants indicated that inadequate social supports and, for some, abstinence-focused treatment methods (e.g., 12-step programs), impeded efforts to cease injecting.
Conclusions
To reduce harms, it is imperative to reorient attention toward the social, structural, and spatial contexts that surround injection drug use and shape periods of injection cessation for SY. There is an urgent need for more comprehensive youth-focused services for those engaged in injection drug use, and further study of innovative means of engaging youth.
Similar content being viewed by others

Background
Injection drug use is associated with the transmission of blood-borne viruses such as HIV (human immunodeficiency virus) and hepatitis C (HCV), fatal and non-fatal overdose, and other preventable harms [1,2,3,4]. It is recognized, however, that many of the risks and harms accompanying injection drug use do not come from the actual act of injecting. Rather, research shows that social, structural, and environmental factors create the conditions that shape harmful injection drug use practices (e.g., syringe sharing) and risk (e.g., of overdose) [5, 6]. The risks and harms associated with injection drug use are heightened for structurally vulnerable populations [7, 8], as the social and structural inequities shaping their lives make safer injecting difficult.
The reduction of harms associated with injection drug use represents an important public health goal. Harm reduction approaches related to injection drug use in Canada include the promotion of non-injection routes of drug administration such as intranasal, oral, or inhalation drug use, as well as the transition to opioid agonist therapies (OAT) such as methadone and buprenorphine-naloxone (Suboxone). Route transitions can serve to reduce the health risks associated with injection drug use such as overdose, vein damage, bacterial infection, and blood-borne virus transmission [9,10,11,12].
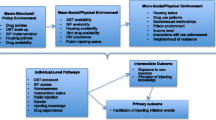
Research and public health interventions attentive to the mitigation of harms associated with injection drug use have typically centered on individual behavioral change [6, 13]. However, the growing prominence of social ecological approaches such as Rhodes’ risk environment framework are evidence of an increasing appreciation of how factors exogenous to the individual shape risks and harms, as well as attempts to reduce those risks and harms [13]. The risk environment framework prioritizes examination of the social, structural, and environmental factors operating across micro- (e.g., drug use settings), meso- (e.g., institutional), and macro- (e.g., societal) levels, which shape drug-related practices and behaviors [5, 13, 14]. Indeed, previous qualitative studies examining injection cessation have highlighted the importance of social and structural factors such as peer norms and treatment programs including methadone maintenance therapy [15,16,17,18], housing, drug prohibition and incarceration [18,19,20,21,22], and environmental factors such as injection setting and neighborhood characteristics [23, 24].
Though early intervention has been found to be an important factor in mediating the harms associated with injection drug use, studies examining injection cessation have largely focused on adult people who inject drugs (PWID) rather than young people [19]. Increased focus on the injection drug use patterns of young people is critical, as young PWID in Canada experience numerous negative health and social outcomes. These include unstable housing [25], involvement in dangerous income generation activities such as drug dealing and survival sex work [26], increased vulnerability to police and criminal justice encounters [27], and higher mortality rates in comparison to the rest of the Canadian population [28, 29]. In the province of British Columbia (BC), drug overdose deaths for young people between the ages of 10 and 18 years old doubled from 2015 to 2016, and overdose deaths of young people from ages 19 to 29 increased from 116 to 202 people in the same time period [30]. Notably, a report that examined youth drug overdose death in BC indicated that Indigenous youth between ages 13 and 23 were significantly over-represented between 2009 and 2013 [31]. Due to dramatic increases in opioid-related drug overdose deaths in BC, the Provincial Health Officer declared a public health emergency in April 2016 [32, 33]. Vulnerable street-involved young people who use drugs (SY; defined as those temporarily or absolutely without housing or accessing street youth services) are particularly vulnerable to these harms.
Vancouver, Canada, is the site of well-established illicit drug scenes, located in the Downtown Eastside (DTES) and Downtown South neighborhoods. The DTES is a particularly stigmatized and impoverished neighborhood in the city’s downtown core, characterized by a highly visible street-based drug scene (including drug use, the selling of illegal drugs and other street-based income generation, and homelessness) [34]. This setting is also unique in terms of the high concentration of addictions services located there. Available services include harm reduction-informed programs such as needle exchange programs, methadone maintenance therapy (MMT) and Suboxone programs, and the provision of take home opioid antagonist (naloxone) kits [35]. The city is home to two federally approved supervised injection facilities (Insite and the Dr. Peter Centre), several temporary emergency overdose prevention sites located in DTES, and two harm reduction-informed detox facilities (Onsite and Directions Youth Detox). Abstinence-based programs (e.g., 12-step programs) are also accessible, including in residential settings such as recovery houses and detoxification (detox) and drug treatment facilities. In comparison to harm reduction informed programs and facilities, these programs and settings tend to have more rigid and structured policies, and prohibit any use of illicit drugs [35].
While downtown Vancouver is characterized by a high concentration of addiction services, young people in this setting nevertheless continue to experience several unique barriers to accessing these services. As has been found elsewhere across North America, these barriers include long wait times, age restrictions, experiences of discrimination based on gender, race, and sexuality, a lack of trained providers and access to OAT [36,37,38,39,40,41]. There are also significant gaps in addictions services coverage locally, including a dire shortage of dedicated residential treatment beds for young people [41]. In terms of the broader landscape in which these services are embedded, a lack of affordable and appropriate housing for youth in the City of Vancouver (one of the most expensive cities in North America to live in) has created a significant youth homelessness problem. In 2016, Vancouver’s homeless census identified 191 homeless youth under age 25 [42], with one youth shelter reporting that over 1400 young people access their services each year, a number that may be more representative [43]. Youth-dedicated community-based services, including drop-in centers, shelters, and food programs are under-resourced [41]. For Vancouver’s SY, homelessness has been found to be a predictor to injection drug use initiation [44]. Research in Vancouver has further documented high rates of syringe sharing among SY, particularly among young women, placing this population at high risk of blood borne infections and overdose [45].
This ethno-epidemiological study draws upon qualitative interviews, informed by longitudinal ethnographic work, to explore how SY in Vancouver with a history of injection drug use characterized their transitions into periods of injection cessation, as well as perceived barriers to injection cessation in this setting. In the context of semi-structured, in depth interviews, in which study participants were asked about the circumstances surrounding periods of injection cessation, SY tended to emphasize the importance of everyday conditions in their lives, rather than the specific mechanisms through which they achieved injection cessation. In this paper, we are therefore careful to locate SY’s experiences with injection cessation within the broader social, structural, and environmental contexts that powerfully shaped drug-related behaviors, decision-making, risks, and harms among these individuals.
Methods
Participants for this ethno-epidemiological study were recruited from the At-Risk Youth Study (ARYS), a prospective cohort of street-involved and drug-using youth that has been described in detail elsewhere [46]. Initial recruitment of study participants takes place via community outreach and drop-in at a storefront research office located in Vancouver’s Downtown South. Participants are encouraged to refer their peers to the study, and health and social services professionals can also refer their clients to the study. ARYS cohort participants are between 14 and 26 years of age at the time of enrolment, and self-report the use of illicit drugs other than or in addition to cannabis during the past 30 days. Baseline and biannual follow-up visits consist of interviewer-administered questionnaire and blood tests for HIV and HCV antibodies. Pre- and post-test counseling is provided, and referrals to service agencies are available by request or at the discretion of interviewers. The baseline and follow-up questionnaires collect data pertaining to experiences with accessing addiction services, both across SY’s lifetimes and during the previous 6 months [47].
For this study, we purposively recruited 22 ARYS cohort participants who had a history of injection drug use, and had reported at a biannual visit the cessation of injection drug use for at least one 6-month period, though participants may have continued to use non-injectable drugs. The ARYS cohort database was queried in January 2013 in order to identify eligible participants. Phone calls, emails, and social media messages were used to contact eligible participants. Youth who were interested in participating in the study (i.e., who were willing to speak about experiencing periods of injection cessation) had further study details explained to them by ARYS staff and provided informed consent prior to being enrolled in the study. Semi-structured interviews took place with enrolled participants in two waves between May 2013 and September 2015. A first wave of interviews with 13 participants occurred from May 2013 to August 2013 and was conducted by the third author (MH). These interviews focused on the social, structural, and environmental factors that shaped youth’s experiences with injection cessation. A second wave of interviews with nine participants occurred from June 2015 to September 2015 and was conducted by the first author (JB). These interviews were designed to further examine key themes (e.g., access to drug treatment services, experiences with MMT programs, housing availability) that emerged during the first wave of interviews and initial analysis of interview data.
All interviews took place at our frontline research office in the Downtown South, were audio-recorded, transcribed verbatim, and checked for accuracy. All identifying information was removed from transcripts. Semi-structured interviews lasted for 45–60 min, and sought to elicit discussion of participants’ perspectives regarding their experiences with achieving periods of injection cessation. The interview guide included questions about how SY’s drug use trajectories intersected with experiences of street-based homelessness and housing transitions, and access to various services and other kinds of supports (e.g., family and friends). We asked young people to describe transitions in routes of drug administration across time (e.g., from intranasal, oral or inhaled routes of administration to injection drug use, and vice versa), and about the ways that they reduced risks and harms in relation to their drug use across time. Finally, we probed for the different kinds of barriers and facilitators young people experienced when attempting to achieve periods of injection cessation.
The methodology employed in this study reflects an ethno-epidemiological approach, in which quantitative cohort data is utilized alongside qualitative findings from in-depth interviews and long-term ethnographic fieldwork. This “value added,” mixed-method approach [48] allows for a more robust exploration of the contextual factors surrounding drug use patterns than traditional epidemiological methods alone. It results in more nuanced, participant-centered, and experiential explorations of the production of particular events and health outcomes [49,50,51]. In what follows, we draw upon insights gained from previous qualitative research conducted by other authors (RM, WS), which examined experiences with addiction treatment programs among local people who use drugs [52, 53], as well as an ongoing program of ethnographic research with a subsample of ARYS participants conducted by another author (DF) [54, 55]. These broader qualitative and ethnographic research findings were used during analysis to triangulate the findings of our in-depth interviews (which are the focus of this paper) and to ensure the reliability of the analysis [48].
At the time of the interview, participants ranged in age from 20 to 31, with a mean average age of 26. Eight of the interview participants identified as women and 14 as men. The majority of interviewees were white, with three young people identifying as Indigenous. Taken as a whole, the participants of this study represent a highly marginalized subpopulation of “at risk youth” and most returned to injection drug use fairly quickly after their 6-month cessation. Along with drug use, many experienced mental health issues, disability, disease, homelessness, and unstable housing. Most had low levels of education and subsisted upon income assistance, disability benefits, and informal forms of income generation such as sex work and drug dealing. Participants’ accounts often contained references to difficult childhoods and a lack of familial/social supports. A number reported frequent encounters with police.
In order to analyze the data collected, an initial coding framework developed was generated that captured emergent themes (e.g., ‘addiction treatment programs,’ ‘family support,’ ‘housing,’ and ‘MMT programs’). The analysis and coding framework was then refined using insights gained through our previous qualitative and ethnographic research, as well as through consideration of how the risk environment framework could be meaningfully applied to our data [13, 56]. All study participants received a $30 honorarium for their participation in qualitative interviews. The study received ethical approval from the University of British Columbia Research Ethics Board.
Results
Participants’ experiences with achieving periods of injection cessation were diverse. While some described slowly reducing the frequency of injection drug use, others described quitting injecting “cold turkey.” Whether SY worked to slowly reduce injection drug use or quit all at once, for many young people periods of injection cessation were accomplished independent of engagement with addiction services, via a transition to a new route of administration and/or a new drug (e.g., from injection heroin to the smoking of heroin, or substitution with crystal methamphetamine or cannabis). For other SY, accessing various addiction services, including MMT programs, residential detoxification, and drug treatment programs, was a key pathway to injection cessation. Access to social support and stable housing was also critical for many SY as they attempted to transition away from injection drug use. Participants’ experiences with accessing addiction services, housing, and social support point to a number of important social, structural, and environmental barriers to injection cessation in our setting.
Accessing OAT: methadone maintenance therapy
A majority of participants indicated that the primary means through which they ceased injecting drugs, specifically opioids, was by accessing OAT, in particular, MMT. Getting on MMT was also identified by SY as essential to maintaining injection cessation over time. However, the cost of daily dispensing fees was cited by a number of youth as a barrier to accessing MMT. For example, one participant (who began smoking heroin at age 17, and injecting it at the age of 22) explained:
I always wanted to get on methadone ‘cause I had tried rehab many times and it just didn’t work for me – like I think the longest I’ve ever lasted was like twenty-two hours or something in a place – so I always wanted to get on methadone. I had a really hard time getting on it ‘cause I wasn’t on welfare and so you have to pay. (Participant #2, White woman, 29 years old)
At the time of the interview in British Columbia, the cost of MMT was only covered for individuals on income assistance, which this young woman was initially unable to access. Ultimately, this young woman’s father ended up paying the daily dispending fee, which finally allowed her to access to MMT at the age of 25. Having access to MMT, and later income assistance, she was able to cease injecting.
Accessing residential detox and drug treatment programs
The majority of participants expressed a similar view to that of the young women quoted above, namely, that residential drug treatment programs did not “work” for them or, youth suspected, many others:
Ninety-five percent of the people like in treatment centres that I’m seeing, are relapsing and– like this system is not working and it’s getting a lot of money. (Participant #17, White male, 30 years old)
Participants frequently described negative experiences while in abstinence-based residential detox and drug treatment programs, including, for example, overly restrictive rules and regulations (e.g., the requirement to attend daily 12-step meetings and group counseling sessions, and “one strike and you’re out” rules that meant expulsion from the program for any form of drug use). The residential detox and drug treatment programs available to young people in Vancouver vary dramatically in terms of quality and philosophies of care. While abstinence-based programs (usually informed by the 12-step model) were reported by a small number of participants to be beneficial in terms of facilitating short-term injection cessation, they were usually characterized as being insufficient to support long-term cessation of injecting. One participant noted that the 12-step program they attended worked initially but eventually did not facilitate their injection cessation:
I went to lots of [12-step] meetings. I don’t really go anymore but I went to a lot. I got a sponsor. I did the step work and it really helped in the beginning, it was a good stepping-stone. (Participant #4, White woman, 28 years old)
Consistent with the findings of our longitudinal ethnographic work, participants’ access to residential detox and drug treatment programs was limited by long waitlists, as well as experiences of aging out of youth-focused addiction services, which are capped at ages ranging from 18 to 24 years of age. One 23-year-old man described employing a combination of Suboxone (which was not readily available through, or covered by, pharmacare at the time of data collection) and his own methods (i.e., biking, yoga) to achieve and maintain injection cessation, because he was too old to access the harm reduction-informed youth detox he had benefited from previously:
Like you go there to detox but people are there to take care of you and it’s beautiful. And you’re able to go smoke, like whenever you ask can I go for a smoke and they brought you smokes and I love that place. It’s amazing for youth under 21. I wish there was a thing like that for uh [older people]. (Participant #15, White man, 23 years old)
Our long-term ethnographic research indicates that aging out of youth-specific services presents a particular problem for young people who are generally unwilling to access residential detox and drug treatment programs located in Vancouver’s DTES neighborhood, which are inclusive of all ages.
Achieving periods of injection cessation independent of addiction services engagement
Some participants appreciated the rules and structure that abstinence-based detox and drug treatment programs offered. However, a majority of study participants indicated that they eventually avoided abstinence-based detox and drug treatment programs as a result of what they characterized as restrictive policies (i.e., expulsion for drug use, missing curfews, house chores, meeting attendance, and noise complaints). These youth generally came to view injection cessation as something that they had to accomplish on their own, through what they referred to as “their own methods of harm reduction.” For many participants, periods of injection cessation were facilitated via different kinds of transitions in drug use. Some young people who quit injecting drugs continued to use non-injection illicit drugs. For example, a small number of youth transitioned from injecting to smoking crystal methamphetamine in an explicit attempt to reduce harms. Alternatively, several participants identified cannabis as means of assuaging the feelings of discomfort that accompany quitting injection drug use:
Being on drugs for such a long period of time is like, that’s how you’re normal […] and now when I stopped using, like, I’m still having a hard time adjusting, […] it’s really hard to deal with and that’s why I started smoking weed…. (Participant #11, Indigenous woman, 27 years old)
Accessing harm reduction-informed services
Participants also often emphasized the value of accessing harm reduction-informed services in aiding their eventual transition away from injecting. Harm reduction-informed services, including drop-in centers, shelters, and two local detox facilities, generally encourage youth to inject more safely (i.e., by providing sterile injecting paraphernalia and safer injecting education) or to take a short-term break from injecting, with the offer of additional support (e.g., residential drug treatment placements) if and when youth decide to transition away from injecting more permanently. In comparison to abstinence-based detox and drug rehabilitation programs, and in particular, those informed by the 12-step model, these service spaces were described by SY as less judgmental toward those who were gradually moving toward injection cessation as a means of reducing harms in their lives. One young woman compared her experience at the harm reduction-informed youth detox, which she described as “low key,” with an “absolutely terrible experience” she had at an abstinence-based, more medicalized detox, stating definitively, “I just don’t like medical detox”:
It’s cool that you can choose your own food. Like they’ll be like hey, you know are you getting hungry? Oh like, you want me to make you this or what do you want? They’ll take you to the park if you wanna like just be a kid and like play on the playground. Um, I dunno, they’re just cool. [….] Like there aren’t nurses running around me like here’s your meds [medication] rah rah rah, like it’s just… it’s better. (Participant #7, White woman, 20 years old)
The following participant similarly described a positive experience at Vancouver’s other harm-reduction informed detox (Onsite), which he accessed in order to meet the criteria (1 week of abstinence) for entrance into a longer-term treatment center:
I just slept most of the day, and kind of enjoyed little activities, and just eating regular food without having to stand in food lines, and did lots of fun activities, and enjoying some camaraderie there. (Participant #17, White male, 30 years old)
Both of Vancouver’s harm reduction informed detoxes are less rigid in enforcing abstinence, and instead of working with clients on a case-to-case basis, recognizing that hasty ejection from detox may precipitate increased instability, risk, and harm in individuals’ lives. In general, harm reduction-informed services often were felt to take a more holistic approach to supporting periods of injecting cessation by facilitating SY’s access to basic necessities and multiple supports including shelter, housing, work, clothing, showers, and food. These more “relaxed” and “respectful” service spaces (as participants often put it) were also often more conducive to the establishment of meaningful relationships with service staff; a valued source of social support for many SY.
Social support
Participants indicated that support from health and social service providers, as well as from family and friends, could be integral to achieving and maintaining injection cessation. As described earlier, one participant was only able to access MMT with the financial help of her father. Social support was also central to the experience of another young man, who connected his positive experience in a longer-term recovery house with the relationship he formed with a service provider:
The guy who was the worker that got me there would take me to movies and [we] became friends and you know, it was just a friend. You know? (Participant #16, White man, 30 years old)
One young woman, who was court ordered to remain abstinent for 14 months due to a criminal charge related to drug trafficking, resisted formal pressures to reside in a recovery house despite her fear of imprisonment, explaining that having a home and the support of a “loving family” were more useful in maintaining injection cessation than the addiction services available to her, which she characterized as overly restrictive (Participant #14, Indigenous woman, 29 years old).
Participants who achieved periods of injection cessation as a result of steady family support were the exception, however. The support of family members and even friends was generally scarce among study participants; most expressed that they had few people in their lives that they could rely upon. Obtaining adequate support from professionals could also be a challenge. One young man described his inability to find a family doctor after being “dropped” by his former doctor because she “had too many patients,” and expressed how his isolation was a barrier to maintaining injection cessation:
Ah, I’m somewhat isolated, I would say – of support. Like I don’t have a regular counsellor. I don’t have a lot of friends. I guess it’s just like maybe if I was looking at it from the outside, I would say I don’t have the strongest support network. (Participant #17, White man, 30 years old)
One Indigenous young man (participant #9, 29 years old) stressed the importance of receiving support via culturally appropriate, non-racist services that evidence respect for diverse Indigenous customs, values, and beliefs. Several participants (both women and men) emphasized the need for additional gender-sensitive supports, such as children friendly services.
Access to housing
SY understood stable housing to be key to their efforts to achieve and maintain injection cessation. One participant, for instance, noted that a combination of obtaining stable housing and work helped him to cease injecting heroin:
I mean it helps me still today, I’m so busy I have no time, I have no time to take it, I don’t have time to do it. [….] When I have time to myself I’m trying to, I found some new passion, um, you know I didn’t have that before, passions, because I didn’t have anything, like I couldn’t put anything anywhere. Now I have an apartment so I can put stuff in there. So if I want to go buy like a punching bag, I’ve got a place to put it. I got a yoga mat so I can do some yoga, you know. I’m able to go for a four or five hour bike ride. (Participant #15, White man, 23 years old)
When asked what services they thought might enable SY to achieve periods of injection cessation, many participants responded that they needed affordable, quality housing and access to other basic necessities such as food and education before they could even begin the process of transitioning away from injecting:
Affordable housing. I think that’s a really big one. And access to healthy food I think is a really big one too. ‘Cause most food banks and stuff like that just, it’s really terrible stuff. Like all processed and just gross. Um, [pause] and like just education I guess. Free education. (Participant #7, White woman, 20 years old)
Participants indicated that not only the quality but also the location of housing impacted their drug use. Specifically, they indicated that the ability to move further away from Vancouver’s inner city drug scene could be beneficial to achieving periods of injection cessation. For example, one young man explained why it was important to him to move away from Vancouver’s DTES:
‘Cause like the minute I go outside of my place all those people will be all messed up and on the street right? So like you gotta leave that stretch of area if you’re gonna, you know, try to get out of the drug scene. [….] I don’t even go to Hastings [Street] anymore [….] Like, I don’t even wanna go down there anymore. (Participant #20, White man, 21 years old)
Despite a desire to move out of the downtown core as a means of achieving and maintaining injection cessation, participants often lamented their inability to re-locate due to a lack of financial and social supports.
Discussion
Our findings point to the multiple contexts and supports that shape SY’s abilities to achieve and maintain periods of injection cessation, as well as the various barriers they face to reducing harm in their own lives. Participants spoke of the importance of housing, social support, harm-reduction informed services, and various addiction services to injection cessation. However, they also highlighted the strategies that they employed independently of service engagement, which primarily involved transitions in the route of drug use and forms of drug substitution that ranged from MMT to the use of cannabis.
Contrary to the findings of a study conducted with young PWID in San Francisco [19], participants in this study reported that the use of cannabis helped in achieving and maintaining periods of drug use cessation. Dynamics reported by our study participants are consistent, however, with more recent research in Canada and the USA, which point to cannabis substitution to be a potentially effective harm reduction strategy for PWID [57,58,59,60]. Participants also described OAT as a useful method for achieving injection cessation and stabilizing their lives. This is consistent with previous research which indicates that OAT allow individuals to reduce injection risks, in addition to treating opioid dependence [61,62,63,64]. Significantly, among PWID, methadone therapy has been shown to reduce risk of hepatitis C and HIV infection [64, 65].
Largely consistent with previous research, participants also emphasized a range of barriers to the cessation of injection drug use. Notably, many study participants experienced barriers to accessing OAT programs such as MMT, primarily because of the daily dispensing fee, which is a problem that has been well documented in existing literature [63, 66, 67]. There have been some recent changes to opioid substitution therapy in B.C. In 2015, Suboxone treatment expanded and is now covered by B.C.’s public drug plan [68, 69]. This is an important policy shift as risk of overdose is much lower with buprenorphine treatment as compared to methadone [70, 71]. Participants explained that family and social supports also had a positive impact on the initiation and continuation of OAT and other drug treatment programs, as has been demonstrated in previous research [72]. In general, increased family responsibility and social supports have been associated with the cessation of illicit drug use [73, 74], while family pressure has been indicated as a self-reported reason for injection cessation [75].
While participants accessed a range of services, harm reduction-informed services rather than abstinence-based ones were emphasized as productive in the facilitation of periods of injection cessation. This finding supports previous research showing that abstinence-based programs are often unsuccessful and can even be counter-productive [11]. People are significantly more vulnerable to overdose following release from residential abstinence-based detox and drug rehabilitation programs, or if expelled from OAT [76,77,78]. The more general barriers to addiction treatment described by participants, such as waitlists, age limitations, and restrictive abstinence-based and 12-step informed policies are consistent with previous studies on youth’s access to addiction services [41, 79,80,81,82]. An epidemiological study of predictors of injection cessation in San Francisco, for example, stressed addiction services targeted at young people as an important area of intervention. Such interventions need to take into consideration the fact that vulnerable and marginalized young people dealing with substance use may be less likely to approach service providers due to issues of trust and discrimination as well as a dearth of culturally appropriate and sex/gender sensitive services [41].
Our findings further highlight that housing is an important facilitator of periods of injection cessation among SY, and should therefore be a fundamental component of health and drug policies related to youth substance use. For marginalized people in Vancouver, and in particular youth, lack of housing has adverse health and social outcomes and negatively impacts the potential for injection cessation. Our findings resonate with an epidemiological study in Baltimore, which found that stable housing is associated with shorter time to injection cessation, and additional epidemiological studies in Montreal and Chennai (India) which found that homelessness impedes injection cessation [18, 20, 75]. Safe and affordable social housing is not only a human right—it is a crucial means of reducing the harms associated with substance use and can promote social inclusion [83,84,85,86,87,88]. In BC, research demonstrates that for youth who use drugs, appropriate low-threshold housing with support is lacking, yet essential to their well-being [41]. The injection-related risks faced by street-involved young people in Vancouver is often further exacerbated by their homelessness [27, 89]. In addition, prolonged presence in micro-risk environments as a result of the inability to exit particular local drug scenes or housing settings also increases harms related to injection drug use [8, 56, 85]. In our setting and others, residence in neighborhoods associated with deprivation and “disorder” have been found to have a negative impact on injection cessation [90, 91].
This study has several limitations. The methodological approach is subject to limited generalizability and social desirability bias. However, an ethno-epidemiological approach, which incorporates longitudinal ethnographic observations into the analysis of qualitative interview data, allows for a more comprehensive interpretation of this data [48, 92, 93]. Further, the research findings are situated within a unique setting (an urban center with a number of addiction, social and health services, and harm reduction initiatives). Our findings may not be reflective of the experiences of the larger injection drug using youth community either locally or nationally. For instance, not all provinces in Canada include harm reduction in their health strategies and previous research has found that younger PWID have been denied access to MMT based on age [94]. In addition, the underrepresentation of Indigenous participants in the study points to the need for further attention to barriers to injection cessation among this vulnerable population.
Conclusions
In conclusion, our findings highlight the broader social, structural, and environmental contexts that powerfully framed—or prevented—periods of injection cessation among highly marginalized SY. This study has implications for health and social policy. Namely, we argue that it is imperative to include the perspectives of young PWID in policy discussions and to reorient attention toward the socio-economic roots of poverty, drug policy, and related social and health harms [1, 95]. We further emphasize the need for a more comprehensive system of care for young PWID, with attention to facilitating better treatment access for young marginalized populations and developing youth oriented services attentive to diversity and youth perspectives. As well, increased consideration of the promotion of non-injection routes of drug administration, rather than more singular emphasis on abstinence, could play a significant role in the minimization of harms associated with injection drug use for young people. These final recommendations, however, will not be effective unless the underlying social structural factors that frame injection drug use among young PWID are also addressed.
Abbreviations
- ARYS:
-
At-Risk Youth Study
- B.C.:
-
British Columbia
- DTES:
-
Downtown Eastside
- HCV:
-
Hepatitis C
- HIV:
-
Human immunodeficiency virus
- MMT:
-
Methadone maintenance therapy
- OAT:
-
Opioid agonist therapies
- PWID:
-
People who inject drugs
- SY:
-
Street-involved young people who use drugs
References
Csete J, Kamarulzaman A, Kazatchkine M, Altice F, Balicki M, Buxton J, et al. Public health and international drug policy. The Lancet Commissions. 2016;387:1427–80.
Cook C, Phelan M, Sander G, Stone K, Murphy F. The case for a harm reduction decade: Progress, potential and paradigm shifts. Harm Reduction International Report. 2016. Available from: https://www.hri.global/files/2016/03/10/Report_The_Case_for_a_Harm_Reduction_Decade.pdf. Accessed 2 April 2016.
Kerr T, Marshall BD, Miller C, Shannon K, Zhang R, Montaner JS, et al. Injection drug use among street-involved youth in a Canadian setting. BMC Pub Health. 2009;3:171.
Roy E, Haley N, Pascale L, Cedras L, Weber AE, Claessens C, et al. HIV incidence among street youth in Montreal. Can AIDS. 2003;17:1071–5.
Strathdee SA, Hallett TB, Bobrova N, Rhodes T, Booth R, Abdool R, et al. HIV and risk environment for injecting drug users: the past, present, and future. Lancet. 2010;376:268–84.
Maher L. Don’t leave us this way: ethnography and injecting drug use in the age of AIDS. Int J Drug Policy. 2002;13:311–25.
Bourgois P, Prince B, Moss A. The everyday violence of hepatitis C among young women who inject drugs in San Francisco. Hum Organ. 2004;63:253–64.
Farmer P. Pathologies of power: health, human rights, and the new war on the poor. Berkeley, CA: University of California Press; 2003.
Bridge J. Route transition interventions: potential public health gains from reducing or preventing injecting. Int J Drug Policy. 2010;21:125–8.
Des Jarlais DC, Arasteh K, Perlis T, Hagan H, Heckathorn D, Mcknight C, et al. The transition from injection to non-injection drug use: long-term outcomes among heroin and cocaine users in New York City. Addiction. 2007;102:778–85.
Dolan K, Clement N, Rouen D, Rees V, Shearer J, Wodak A. Can drug injectors be encouraged to adopt non-injecting routes of administration (NIROA) for drugs? Drug Alcohol Rev. 2004;23:281–6.
Hunt N, Griffiths P, Southwell M, Stillwell G, Strang J. Preventing and curtailing injecting drug use: a review of opportunities for developing and delivering ‘route transition interventions’. Drug Alcohol Rev. 1999;18:441–51.
Rhodes T. The ‘risk environment’: a framework for understanding and reducing drug-related harm. Int J Drug Policy. 2002;13:85–94.
Rhodes T, Singer M, Bourgois P, Friedman SR, Strathdee SA. The social structural production of HIV risk among injection drug users. Soc Sci Med. 2005;61:1026–44.
Deren S, Kang SY, Colon HM, Robles RR. Predictors of injection drug use cessation among Puerto Rican drug injectors in New York and Puerto Rico. Am J Drug Alcohol Abuse. 2007;33:291–9.
Latkin CA, Knowlton AR, Hoover D, Mandell W. Drug network characteristics as a predictor of cessation of drug use among adult injection drug users: a prospective study. Am J Drug Alcohol Abuse. 1999;25:463–73.
Small W, Fast D, Krüsi A, Wood E, Kerr T. Social influences upon injection initiation among street-involved youth in Vancouver, Canada: A qualitative study. Subst Abuse Treat Prev Policy. 2009; 4: doi 10.1186/1747-597X-4-8.
Steensma C, Boivin JF, Blais L, Roy E. Cessation of injection drug use among street-based youth. J Urban Health. 2005;82:622–37.
Evans JL, Hahn JA, Lum PJ, Stein ES, Page K. Predictors of injection drug use cessation and relapse in a prospective cohort of young injection drug users in San Francisco, CA (UFO study). Drug Alcohol Depend. 2009;101:152–7.
Shah NG, Galai N, Celentano DD, Vlahov D, Strathdee SA. Longitudinal predictors of injection cessation and subsequent relapse among a cohort of injection drug users in Baltimore, MD, 1998–2000. Drug Alcohol Depend. 2006;83:147–56.
DeBeck K, Kerr T, Li K, Milloy MJ, Montaner J, Wood E. Incarceration and drug use patterns among a cohort of injection drug users. Addiction. 2009;104:69–76.
DeBeck K, Wood E, Montaner J, Kerr T. Canada’s new federal ‘National anti-Drug Strategy’: an informal audit of reported funding allocation. Int J Drug Policy. 2009;20:188–91.
McNeil R, Small W. ‘Safer environment interventions’: a qualitative synthesis of the experiences and perceptions of people who use drugs. Soc Sci Med. 2014;106:151–8.
Sherman SG, Hua W, Latkin CA. Individual and environmental factors related to quitting heroin injection. Subst Use Misuse. 2004;39:1199–214.
Krüsi A, Fast D, Small W, Wood E, Kerr T. Social and structural barriers to housing among street-involved youth who use illicit drugs. Health Soc Care Community. 2010;18:282–8.
Fast D, Small W, Wood E, Kerr T. Coming ‘down here’: Young people’s reflections on becoming entrenched in a local drug scene. Soc Sci Med. 2009;69:1204–10.
Boyd J, Fast D, Small W. Pathways to criminalization for street involved youth who use illicit substances. Crit Public Health. 2016;25:530–41.
Miller CL, Kerr T, Strathdee SA, Li K, Wood E. Factors associated with premature mortality among young injection drug users in Vancouver. Harm Red J. 2007;4:1.
Roy E, Haley N, Leclerc P, Sochanski B, Boudreau JF, et al. Mortality in a cohort of street youth in Montreal. JAMA. 2004;292:624–6.
BC Coroners Service. Illicit overdose deaths in BC: January 1, 2007- March 31, 2017. Burnaby April 19, 2017. Available from: http://www2.gov.bc.ca/assets/gov/public-safety-and-emergency-services/death-investigation/statistical/illicit-drug.pdf.
Egilson M. Preventing death after overdose: BC Coroners Service Child Death Review Panel. A Review of Overdose Deaths in Youth and Young Adults 2009–2013. Burnaby, BC: Office of the Chief Coroner, Ministry of Justice. 2016. Available from: http://www2.gov.bc.ca/assets/gov/public-safety-and-emergency-services/death-investigation/child-death-review-unit/reports-publications/overdose-death-youth-young-adult.pdf. Accessed 22 March 22, 2016.
BC Gov News. Provincial health officer declares public health emergency. News Release. 14 April 2016. Available from: https://news.gov.bc.ca/releases/2016HLTH0026-000568
BC Coroners Service. Illicit drug overdose deaths in B.C. January1, 2007–February 29, 2016. Burnaby, BC: Office of the Chief Coroner, Ministry of Justice. 2016. Available from: http://www2.gov.bc.ca/assets/gov/public-safety-and-emergency-services/death-investigation/statistical/illicit-drug.pdf.
Wood E, Kerr T. What do you do when you hit rock bottom? Responding to drugs in the city of Vancouver. Int J Drug Policy. 2006;17:55–60.
Fischer B, Murphy Y, Rudzinski K, MacPherson D. Illicit drug use and harms, and related interventions and policy in Canada: a narrative review of select key indicators and developments since 2000. Int J Drug Policy. 2016;27:23–35.
Bluthenthal RN, Jacobson JO, Robinson PL. Are racial disparities in alcohol treatment completion associated with racial differences in treatment modality entry? Comparison of outpatient treatment and residential treatment in Los Angeles County, 1998 to 2000. Alcohol Clin Exp Res. 2007;31:1920–6.
Cochran BN, Stewart AJ, Ginzler JA, Cauce AM. Challenges faced by homeless sexual minorities: comparison of gay, lesbian, bisexual, and transgender homeless adolescents with their heterosexual counterparts. Am J Public Health. 2002;92:773–7.
Guarino HM, Marsch LA, Campbell WS, Gargano SP, Haller DL, Solhkhah R. Methadone maintenance treatment for youth: experiences of clients, staff and parents. Subst Use Misuse. 2009;44:1979–89.
Rounds-Bryant JL, Kristiansen PL, Fairbank JA, Hubbard RL. Substance use, mental disorders, abuse, and crime: gender comparisons among a national sample of adolescent drug treatment clients. J Child Adolesc Subst Abuse. 1998;7:19–34.
Subramaniam GA, Fishman MJ, Woody G. Treatment of opioid-dependent adolescents and young adults with buprenorphine. Curr Psychiatry Rep. 2009;11:360–3.
Turpel-Lafond ME. A review of youth substance use services in B.C. Victoria, B.C.: Representative for Children and Youth. May 2016. Available from: https://www.rcybc.ca/sites/default/files/documents/pdf/reports_publications/rcy_reviewyouthsubstance-final.pdf. Accessed 4 June 2016.
Thomson M. Vancouver Homeless Count 2016. M. Thomson Consulting & City of Vancouver. 2016: p.24. Available from: http://vancouver.ca/files/cov/homeless-count-2016-report.pdf. Accessed 12 May 2017.
Covenant House. Statistics: a profile of Vancouver’s street youth. 2015. Available from: http://www.covenanthousebc.org/about/statistics. 22 Jan. 2016.
Feng C, DeBeck K, Kerr T, Mathias S, Montaner J, Wood E. Homelessness independently predicts injection drug use initiation among street-involved youth in a Canadian setting. J Adolesc Health. 2013;54:499–501.
Lloyd-Smith E, Kerr T, Zhang R, Montaner JS, Wood E. High prevalence of syringe sharing among street involved youth. Addict Res Theory. 2008;16:353–8.
Wood E, Stoltz JA, Montaner JSG, Kerr T. Evaluating methamphetamine use and risks of injection initiation among street youth: the ARYS study. Harm Red J. 2006;3:18.
Hadland SE, Kerr T, Li K, Montaner J, Wood E. Access to drug and alcohol treatment among a cohort of street-involved youth. Drug Alcohol Depend. 2009;101:1–7.
Lopez A, Bourgois P, Wenger L, Lorvick J, Martinez A, Kral A. Interdisciplinary mixed methods research with structurally vulnerable populations: case studies of injection drug users in San Francisco. Int J Drug Policy. 2013;24:101–9.
Bourgois P, Bruneau J. Needle exchange, HIV infection, and the politics of science: confronting Canada’s cocaine injection epidemic with participant observation. Med Anthropol. 2000;18:325–50.
Mayock P, Cronly J, Clatts M. The risk environment of heroin use initiation: young women, intimate partners, and “drug relationships.”. Subst Use Misuse. 2015;50:771–82.
Small W, Milloy MJ, McNeil R, Maher L, Kerr T. Plasma HIV-1 RNA viral load rebound among people who inject drugs receiving antiretroviral therapy (ART) in a Canadian setting: an ethno-epidemiological study. AIDS Res Ther. 2016;13:26.
Damon W, Small W, Anderson S, Maher L, Wood E, Kerr T, et al. ‘Crisis’ and ‘everyday’ initiators: a qualitative study of coercion and agency in the context of methadone maintenance treatment initiation. Drug Alcohol Rev. 2016: doi: 10.1111/dar.12411.
McNeil R, Kerr T, Anderson S, Maher L, Keewatin C, Milloy MJ, et al. Negotiating structural vulnerability following regulatory changes to a provincial methadone program in Vancouver, Canada: a qualitative study. Soc Sci Med. 2015;133:168–76.
Fast D, Kerr T, Wood E, Small W. The multiple truths about crystal meth among young people entrenched in an urban drug scene. Soc Sci Med. 2014;110:41–8.
Fast D, Small W, Krüsi A, Wood E, Kerr T. “I guess my own fancy screwed me over”: transitions in drug use and the context of choice among young people entrenched in an open drug scene. BMC Pub Health. 2010;10:126.
Rhodes T. Risk environments and drug harms: a social science for harm reduction approach. Int J Drug Policy. 2009;20:193–201.
Lau N, Sales P, Averill S, Murphy F, Sato S, Murphy S. A safer alternative: cannabis substitution as harm reduction. Drug Alcohol Rev. 2015;34:654–9.
Lucas P, Reiman A, Earleywine M, McGowan SK, Oleson M, Coward MP, et al. Cannabis as a substitute for alcohol and other drugs: a dispensary-based survey of substitution effect in Canadian medical cannabis patients. Addict Res Theory. 2013;21:435–42.
Lucas P, Walsh Z, Crosby K, Callaway R, Belle-Isle L, Kay R, et al. Substituting cannabis for prescription drugs, alcohol and other substances among medical cannabis patients: the impact of contextual factors. Drug Alcohol Rev. 2016;35:326–33.
Nunberg H, Kilmer B, Pacula R, Burgdorf J. An analysis of applicants presenting to a medical marijuana specialty practice in California. J Drug Policy Anal. 2011;4:1941–2851.
Gowing L, Farrell MF, Bornemann R, Sullivan LE, Ali R. Oral substitution treatment of injecting opioid users for prevention of HIV infection. Cochrane Database Syst Rev. 2011: CD004145.
Kellogg S, Melia D, Khuri E, Lin A, Ho A, Kreek MJ. Adolescent and young adult heroin patients. J Addict Dis. 2006;25:15–25.
Yang J, Oviedo-Joekes E, Christian KWM, Li K, Louie M, Schechter M, et al. The Cedar Project: methadone maintenance treatment among young Aboriginal people who use opioids in two Canadian cities. Drug Alcohol Rev. 2011;30:645–51.
MacArthur GJ, Minozzi S, Martin N, Vickerman P, Deren S, Bruneau J, et al. Opiate substitution treatment and HIV transmission in people who inject drugs: systematic review and meta-analysis. BMJ. 2012;345:e5945.
Nolan S, Dias Lima V, Fairbairn N, Kerr T, Montaner J, Grebely J, et al. The impact of methadone maintenance therapy on hepatitis C incidence among illicit drug users. Addict. 2014;109:2053–9.
Nyamathi A, Smith DM, Shoptaw S, Mutere M, Cohen A, Amrani I, et al. Perceptions of methadone maintained clients about barriers and facilitators to help-seeking behavior. Community Health Partnersh Res, Educ Action. 2007;1:301–9.
Parkes T, Reist D. British Columbia methadone maintenance treatment program: a qualitative systems review- summary report. 2010. Available from: www.vandu.org/documents/methadone_maintenance_in_bc_review_report_summary.pdf. Accessed 11 Feb. 2014.
BC Gov News. B.C. increases access to addiction treatment Suboxone. News Release. 13 Oct. 2015. Available from: https://news.gov.bc.ca/releases/2015HLTH0079-001698
Providence Health Care (PHC) & Vancouver Coastal Health (VCH). A Guideline for the clinical management of opioid addiction. 2015. Available from: http://www.bccsu.ca/wp-content/uploads/2016/10/opioid-addiction-guideline.pdf. Accessed 31 May 2016.
Bell JR, Butler B, Lawrance A, Batey R, Salmelainen P. Comparing overdose mortality associated with methadone and buprenorphine treatment. Drug Alcohol Depend. 2009;104:73–7.
Marteau D, McDonald R, Patel K. The relative risk of fatal poisoning by methadone or buprenorphine within the wider population of England and Wales. BMJ Open. 2015;5:e007629.
Lin C, Wu Z, Detels R. Family support, quality of life and concurrent substance use among methadone maintenance therapy clients in China. Public Health. 2011;125:269–74.
Galea S, Nandi A, Vlahov D. The social epidemiology of substance use. Epidemiol Rev. 2004;26:36–52.
Knight DK, Simpson DD. Influences of family and friends on client progress during drug abuse treatment. J Subst Abuse. 1996;8:417–29.
Mehta SH, Sudarshi D, Srikrishnan AK, Celentano DD, Vasudevan CK, Anand S, et al. Factors associated with injection cessation, relapse and initiation in a community-based cohort of injection drug users in Chennai. India Addict. 2011;107:349–58.
Cornish R, Macleod J, Strang J, Vickerman P, Hickman M. Risk of death during and after opiate substitution treatment in primary care: prospective observational study in UK General Practice Research Database. BMJ. 2010;341:c5475.
Strang J, McCambridge J, Best D, Beswick T, Bearn J, Rees S, Gossop M. Loss of tolerance and overdose mortality after inpatient opiate detoxification: follow up study. BMJ. 2003;326(7396):959–60.
WHO. Community management of opioid overdose. Geneva: World Health Organization, 2014. Available from: http://apps.who.int/iris/bitstream/10665/137462/1/9789241548816_eng.pdf?ua=1&ua=1. Accessed 26 March 2016.
DeBeck K, Kerr T, Nolan S, Dong H, Montaner J, Wood E. Inability to access addiction treatment predicts injection initiation among street-involved youth in a Canadian setting. Subst Abuse Treat Prev Policy. 2016;11:1.
Doweiko HE. Concepts of chemical dependency. 6th ed. Belmont, CA: Thomson Brooks/Cole; 2006.
Downey L, Rosenberg DB, Donovan DM. Gender, waitlists, and outcomes for public-sector drug treatment. J Subst Abuse Treat. 2003;25:19–28.
Pascoe RV, Rush B, Rotondi NK. Wait times for publicly funded addiction and problem gambling treatment agencies in Ontario. Can BMC Health Serv Res. 2013;13:483.
Cheng T, Wood E, Nguyen P, Kerr T, DeBeck K. Increases and decreases in drug use attributed to housing status among street-involved youth in a Canadian setting. Harm Reduct J. 2014;11:12.
Evans L, Strathdee S. A roof is not enough: unstable housing, vulnerability to HIV infection and the plight of the SRO. Int J Drug Policy. 2006;17:115–7.
Pauly B, Reist D, Belle-Isle L, Schactman C. Housing and harm reduction: what is the role of harm reduction in addressing homelessness. Int J Drug Policy. 2013;24:284–90.
Shannon K, Ishida T, Lai C, Tyndall M. The impact of unregulated single room occupancy hotels on the health status of illicit drug users in Vancouver. Int J Drug Policy. 2006;17:107–14.
Toronto shelter, support, and housing administration. What housing first means for people: results of streets to homes 2007 post occupancy research. 2007. Available from: http://www.homelesshub.ca/sites/default/files/txqjqfm0.pdf. Accessed 20 Feb 2015.
Zerger S. Housing: a fundamental component of drug policy. Int J Drug Policy. 2012;23:91–3.
Chesnay C, Bellot C, Sylvestre M. Taming disorderly people one ticket at a time: the penalization of homelessness in Ontario and British Columbia 1. Can J Criminol Crim Justice. 2013;3:161–85.
Genberg BL, Gange SJ, Go VF, Celentano DD, Kirk GD, Latkin CA, et al. The effects of neighbourhood deprivation and residential relocation on long-term injection cessation among injection drug users (IDUs) in Baltimore. Md Addict. 2011;106:1966–74.
Latkin CA, Williams CT, Wang J, Curry AD. Neighborhood social disorder as a determinant of drug injection behaviors: a structural equation modeling approach. Health Psychol. 2005;24:96–100.
Bourgois P. Anthropology and epidemiology on drugs: the challenges of cross-methodological and theoretical dialogue. Int J Drug Policy. 2002;13:259–69.
Creswell JW, Plano Clark VL. Designing and conducting mixed methods research. Thousand Oaks, CA: Sage; 2007.
Methadone Strategy Working Group. Countering the crisis: Ontario’s prescription for opioid dependence. Toronto: Centre for Addiction and Mental Health; 2004.
Room R, Reuter P. How well do international drug conventions protect public health? Lancet. 2012;379:84–91.
Acknowledgements
The authors thank the study participants for their contribution to the research, as well as current and past researchers and staff.
Funding
The study was supported by the Canadian Institutes of Health Research (CIHR) [MOP–102742] and the US National Institutes of Health [R01DA028532], [U01DA038886]. WS is supported by a Scholar Award from the Michael Smith Foundation for Health Research (MSFHR). RM is supported by a MSFHR Scholar Award and CIHR New Investigator Award. These institutions did not play a role in the design of the study; collection, analysis, and interpretation of data; and in writing the manuscript.
Availability of data and materials
Not applicable.
Authors’ contributions
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
All participants provided written informed consent and received a $30 honorarium for their participation. The study was undertaken with ethical approval granted by the Providence Healthcare/University of British Columbia Research Ethics Board.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Boyd, J., Fast, D., Hobbins, M. et al. Social-structural factors influencing periods of injection cessation among marginalized youth who inject drugs in Vancouver, Canada: an ethno-epidemiological study. Harm Reduct J 14, 31 (2017). https://doi.org/10.1186/s12954-017-0159-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12954-017-0159-9