
Abstract
Background
Allergic respiratory diseases are constantly increasing in prevalence. Allergen Immunotherapy (AIT) represent a valuable therapeutic tool as symptomatic and preventative approach, expecially in children. In Italy, primary care pediatricians (PCP) represent the first-line contact and interface for prescription, use and management of AIT. We attempted to evaluate the perception of AIT practice among PCP.
Methods
A questionnaire was built-up, based on literature, guidelines and with the contribution of pediatricians. The questionnaire, including 12 items, was e-mailed to 180 PCP, randomly chosen from mailing lists. The questionnaire explored the personal perception of AIT, the comparison between subcutaneous and sublingual AIT and the overall awareness about the treatment.
Results
130 questionnaires were eligible for analysis. There was a satisfactory knowledge of the characteristics of AIT, its aims and limits, although the positioning of the treatment in guidelines was insufficiently known. Overall, the prescription of AIT made by other specialists was accepted and agreed (78 %). The majority of pediatricians felt that a more intense divulgation and information about AIT would be needed (90 %).
Conclusion
AIT is in general well known and accepted among PCP, although a more intense divulgation effort is required.
Similar content being viewed by others


Background
The prevalence of allergic respiratory diseases (rhinitis and asthma) constantly increased in the second half of the last century. Nowadays, although the prevalence of asthma seemed to plateau, that of rhinitis is still increasing. This fact may be attributable to different factors, including the “westernization” of lifestyle, the reduction of infectious diseases, and the increased allergenic burden linked to climate changes [1, 2]. Concerning Italy, the SIDRIA survey [3], conducted in 1994–95 and 2002, confirmed the plateau of asthma prevalence (about 10 % in both children and adolescents), and the significant increase of rhinitis (from 6 to 9 % in children and from 14 to 17 % in adolescents). In this survey, no relevant difference could be seen in the geographical distribution of respiratory allergies, with a slightly higher occurrence of the symptom cough in large urban agglomerates with respect to rural areas.
In the pediatric age range, allergic diseases represent a special problem, with specific aspects, that include their possible evolution (allergic march) [4–6], the problems related to the long-term pharmacotherapy, the compliance (which is in charge of caregivers), the objective difficulties in correctly deliver inhaled drugs. In addition, the quality of life of the children themselves and of their parents (drug treatment, emergency unit visits, impaired school performance and absenteeism), is usually affected [7, 8]. Thus, an early and correct diagnosis and an adequate therapeutic management of allergic respiratory diseases in children are strongly desirable [9].
Many clinical trials and meta-analyses have convincingly demonstrated that allergen immunotherapy (AIT) is effective in reducing symptoms and drug consumption, with a consequent improvement of the overall quality of life. More importantly, there is evidence that AIT can modify the natural history of allergic disease, for instance preventing the onset of asthma in patients with allergic rhinitis and/or maintaining a long-lasting effect [10]. The introduction of the sublingual route of administration (SLIT) in clinical practice represented an important step forward, of particular relevance in the pediatric age [11]. In this case, the good safety profile (very low risk of severe adverse events), the convenience and the management at home, allowed to expand the indications. In fact, more and more often SLIT is prescribed to children below the age of 5 years [12, 13].
Pediatricians are the first-line specialists who afford the problems related to respiratory allergy, to the prescription and to management of AIT. In Italy, the figure of the “primary care” pediatrician, makes the situation even more peculiar, since those healthcare specialists remain a solid and constant contact with children and families. Based on these premises we performed a questionnaire-based survey among Italian primary care pediatricians to assess their knowledge and information about the use of AIT.
Methods
A 12-item questionnaire was built up, based on the current literature, Position Papers [14–16], expert opinions, and the contribution of numerous primary care pediatricians (Table 1). The questionnaire, involving prescription attitudes, follow-up of patients, awareness about the treatment, had multiple choice options. The questionnaire was e-mailed to primary care pediatricians, randomly chosen from the mailing lists of participants to meetings over the whole Italian territory. The study was observational and cross sectional, therefore only required notification to the local Ethic Committees, according to the Italian laws. The participating pediatricians were required to refer only to those patients for whom the diagnosis of respiratory allergy, and the prescription of AIT were clearly established, possibly made by pediatric allergists/pulmonologists.
Results
The questionnaire was e-mailed to 180 primary care pediatricians, of whom 140 responded. Out of the 140 returned questionnaires, 130 were eligible for analysis since correctly and completely filled. The respondent pediatrician had an age of 55 ± 8.3 years, and 50 of them were male. All of them were obviously employed in the primary care service. On average, each pediatrician was in charge of about 1,000 children (1050 ± 245). The pediatricians resulted to be distributed as follows: northern (31 %) central (24 %) and southern (46 %) Italy, with no difference in gender and age distribution among the three geographical regions. The results are reported in Table 1. As per responses, there was a satisfactory knowledge of the characteristics of AIT, its aims and limits. Overall, the prescription of AIT made by other specialists (pediatric allergist/pulmonologist) was accepted and agreed (78 %). Of note, the majority of pediatricians felt that a more intense divulgation and information about AIT would be needed (90 %). There was no difference in the distribution of the answers according to gender (not shown), and a comparative analysis according to age range could not be made due to the important skew towards older ages (80 % of respondents over 45 years of age and 94 % over 35 years). Also, no geographical-related difference in responses could be detected among the area of residency, as summarized in Table 2.
Discussion
As mentioned above, AIT is the only allergen-oriented therapy, and acts as a disease-modifying treatment. Thus, AIT can not only modify symptoms in the short-medium term period, but can change the progression of the disorder. The disease-modifying effect can be seen as the reduction of the risk of asthma onset in children with rhinitis, and as the persistence of the clinical benefit for several years after the discontinuation [10, 17–19]. These facts assume a special relevance in the pediatric age, when the plasticity and modulability of the immune system are maximal, and when the preventative effects can be reasonably expected.
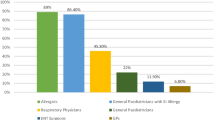
In Italy, children are followed-up by the institutional primary care pediatrician, an almost unique figure all over the world (the equivalent of the general practitioner for adults), who faces daily allergic diseases and their management as first-line referral. AIT is usually prescribed by pediatric allergists (a subspecialty in Italy), who diagnose the disease and chose the most appropriate AIT, then leaving it in the hands of the primary care pediatricians. In such a setting, we considered of primary importance to know which is the perception of and the attitude toward AIT within general pediatricians. This was explored by a simple questionnaire developed by a panel of experts, on the basis of the literature, and agreed with a representative number of primary care colleagues. According to the results, the overall knowledge on the specific argument seems to be satisfactory. Notably, about 50 % of pediatricians still believe that AIT is an add-on therapy to be used when pharmacotherapy fails. Another important aspect is that only one half of the interviewed pediatricians are aware of the fact that AIT is mentioned in the major guidelines. Finally, and probably according to the mentioned responses, the majority of primary care pediatrician agree on the fact that a more intense divulgation effort on the specific argument is worthwhile. The main limitation of this study stands in the questionnaire-based method, with the questionnaire prepared by a restricted group of experts. Nonetheless, it has to be considered that, to obtain a satisfactory response, the questionnaire itself had to be kept as simple and as short as possible. In addition, since no explanation or information on AIT was provided when the questionnaires were mailed, we can assume that the responses truly reflect the reality. Finally it is not possible to compare our results with other similar, since the primary care pediatircian is a professional figure that is present only in our Country (and very few others), and no survey in this sense has been attempted in the past.
Conclusion
As a general consideration, the results herein reported are overall in agreement with those described for Italian general practitioners and chest physicians, who were previously interviewed using similar questionnaires [20, 21]. This facts indirectly testifies that there is an increasing awareness about AIT among physicians, as repeatedly auspicated [22].
References
Bendiks M, Kopp MV. The relationship between advances in understanding the microbiome and the maturing hygiene hypothesis. Curr Allergy Asthma Rep. 2013;13:487–94.
Lombardi C, Fiocchi A, Raffetti E, Donato F, Canonica GW, Passalacqua G, et al. Cross-sectional comparison of the characteristics of respiratory allergy in immigrants and Italian children. Pediatr Allergy Immunol. 2014;25:473–80.
Galassi C, Forastiere F, Biggeri A, Gabellini C, De Sario M, Ciccone G, et al. SIDRIA second phase: objectives, study design and methods. Epidemiol Prev. 2005;29 suppl 1:24–31.
Ker J, Hartert TV. The atopic march: what’s the evidence? Ann Allergy Asthma Immunol. 2009;103:282–9.
Linneberg A. The allergic march in early childhood and beyond. Clin Exp Allergy. 2008;38:1419–21.
Burgess JA, Lowe AJ, Matheson MC, Varigos G, Abramson MJ, Dharmage SC. Does eczema lead to asthma? J Asthma. 2009;46:429–36.
Gentile D, Bartholow A, Valovirta E, Scadding G, Skoner D. Current and future directions in pediatric allergic rhinitis. J Allergy Clin Immunol Pract. 2013;1:214–26.
Borres MP. Allergic rhinitis: more than just a stuffy nose. Acta Paediatr. 2009;98:1088–92.
Nota del segretariato generale del Consiglio dell’Unione Europea-Bruxelles, nov 17 2011 (22.11) (OR. en) 16709/11 SAN 239
Passalacqua G. Specific immunotherapy: beyond the clinical scores. Ann Allergy Asthma Immunol. 2011;107:401–6.
Larenas-Linnemann D, Blaiss M, Van Bever HP, Compalati E, Baena-Cagnani CE. Pediatric sublingual immunotherapy efficacy: evidence analysis, 2009–2012. Ann Allergy Asthma Immunol. 2013;110:402–15.
Agostinis F, Foglia C, Landi M, Cottini M, Lombardi C, Canonica GW, et al. The safety of sublingual immunotherapy with one or multiple pollen allergens in children. Allergy. 2008;63:1637–9.
Pajno GB, Vita D, Caminiti L, Arrigo T, Lombardo F, Incorvaia C, et al. Children’s compliance with allergen immunotherapy according to administration routes. J Allergy Clin Immunol. 2005;116:1380–1.
World Health Organization Position Paper. Allergen immunotherapy : therapeutical vaccines for allergic diseases. Bousquet J, Lockey R, Malling HJ edts. Allergy. 1998;53 suppl 52:3–15. WHO.
Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA2LEN and AllerGen). Allergy. 2008;63 Suppl 86:8–160.
Canonica GW, Cox L, Pawankar R, Baena-Cagnani CE, Blaiss M, et al. Sublingual immunotherapy: World Allergy Organization position paper 2013 update. World Allergy Organ J. 2014;7(1):6. doi:10.1186/1939-4551-7-6.
Möller C, Dreborg S, Ferdousi HA, Halken S, Høst A, et al. Pollen immunotherapy reduces the development of asthma in children with seasonal rhinoconjunctivitis (the PAT-study). J Allergy Clin Immunol. 2002;109:251–6.
Novembre E, Galli E, Landi F, Caffarelli C, Pifferi M, De Marco E, et al. Coseasonal sublingual immunotherapy reduces the development of asthma in children with allergic rhinoconjunctivitis. J Allergy Clin Immunol. 2004;114:851–7.
Marogna M, Tomassetti D, Bernasconi A, Colombo F, Massolo A, Businco AD, et al. Preventive effects of sublingual immunotherapy in childhood: an open randomized controlled study. Ann Allergy Asthma Immunol. 2008;101:206–11.
Lombardi C, Canonica GW, Passalacqua G. The perception of allergen-specific immunotherapy among chest physicians: an Italian survey. Eur Ann Allergy Clin Immunol. 2014;46:132–6.
Lombardi C, Bettoncelli G, Canonica GW, Passalacqua G. The perception of allergen-specific immunotherapy among Italian general practitioners. Eur Ann Allergy Clin Immunol. 2014;46:83–6.
Canonica GW, Baena Cagnani CE, Compalati E, Bohle B, Bonici S, Bousquet J, et al. 100 years of immunotherapy: the Monaco charter. under the high patronage of His Serene Highness Prince Albert II of Monaco. Int Arch Allergy Immunol. 2013;160:346–9.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that thay have no competing interests.
Authors’ contributions
ML, PM, EP and CL did the clinical work. All the Authors equally contributed in collecting and analyzing the data and in drafting the MS. ML GWC and GP designed the study and prepared the final version of the MS. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Landi, M., Meglio, P., Praitano, E. et al. The perception of allergen-specific immunotherapy among pediatricians in the primary care setting. Clin Mol Allergy 13, 15 (2015). https://doi.org/10.1186/s12948-015-0021-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12948-015-0021-0