
Abstract
Background
Studies on the associations between lipid parameters and different hemostatic factors in men and women from the general population are scarce. It was therefore examined whether there are possible relationships between routinely measured serum lipids (total cholesterol, HDL-cholesterol, non-HDL-cholesterol, LDL-cholesterol, and triglycerides) and different hemostatic factors (activated partial thromboplastin time (aPTT), fibrinogen, factor VIII, antithrombin III (AT III), protein C, protein S, and D-dimer).
Methods
The analysis was based on data from the Cooperative Health Research in the Region of Augsburg (KORA)-Fit study, which included 805 participants (378 men, 427 women) with a mean age of 63.1 years. Sex-specific associations between serum lipids and coagulation factors were investigated using multivariable linear regression models.
Results
In men, total cholesterol was inversely related to aPTT but positively associated with protein C activity. HDL cholesterol was inversely related to aPTT and fibrinogen. LDL cholesterol, non-HDL cholesterol, and triglycerides showed a positive association with protein C and protein S activity.
In women, LDL-cholesterol, total cholesterol, and non-HDL-cholesterol were positively related to AT III concentrations and protein C and S activity. Additionally, non-HDL-cholesterol was positively associated with factor VIII activity. HDL cholesterol was inversely related to fibrinogen. Triglycerides showed a positive relationship with protein C activity.
Conclusions
There seem to be sex differences regarding various associations between blood lipid levels and hemostatic factors. Further studies are needed to address the possible impact of these associations on cardiovascular risk and the underlying mechanisms.
Similar content being viewed by others

Background
Dyslipidemia is a major risk factor for cardiovascular disease (CVD) [1]. Among others, elevated low-density lipoprotein cholesterol (LDL-c), decreased high-density lipoprotein cholesterol (HDL-c), and increased triglyceride (TG) levels in the blood are associated with an increased risk of coronary atherosclerosis [2, 3]. While LDL-c is considered the most important lipoprotein-based risk factor, recent epidemiological studies suggest that non-HDL-c may be superior to LDL-c in determining coronary heart disease (CHD) risk [4, 5].
A number of previous studies have examined the role of the hemostatic system in the manifestation of CVD [6,7,8] and have shown that systemic coagulation activity contributes to acute coronary events [9]. For example, associations between fibrinogen [10], Faktor VIII [11], and protein C and protein S [12] and incident CHD were found. Certain studies evaluated components of the blood coagulation system in subjects with familial combined hyperlipidemia, who have a substantially increased risk of CVD, and reported increased coagulation activity in these individuals [13]. Finally, other epidemiological studies have demonstrated a link between various coagulation factors and lipid parameters [8, 14].
Previous studies postulated that a hypercoagulable state was present in individuals with hypercholesterolemia [15]. It has been shown that blood lipids are associated with prothrombotic and endothelial-damaging properties [16]. Circulating lipids affect the vascular endothelium, platelets, and coagulation factors. They are associated with an alteration in the expression and/or function of thrombotic, fibrinolytic and rheological factors [16].
Data from large studies including men and women from the general population examining possible associations between different blood lipid parameters and a variety of coagulation factors are still scarce. Therefore, in the present study, sex-specific associations between LDL-c, HDL-c, non-HDL c, total cholesterol, and TG levels and the parameters activated partial thromboplastin time (aPTT), fibrinogen, D-dimers, antithrombin III (AT III), protein C, protein S, and factor VIII in the adult general population were investigated.
Methods
Study sample
The KORA (Cooperative Health Research in the Region of Augsburg, Germany) platform was established in 1996 and succeeded and advanced the MONICA study (Monitoring of trends and determinants in cardiovascular disease). The KORA cohort study consists of four cross-sectional baseline surveys (S1 1984/85, S2 1989/90, S3 1994/95 and S4 1999/2001, S1-S3 under the MONICA label [17]); since then, all study participants have been followed-up. In early 2018, a follow-up study called “KORA-Fit” started and was conducted in mid-2019. All living attendees of the KORA cohort born between 1945 and 1964 who agreed to be recontacted were invited for a new examination (n = 3059 or 64.4% of all appropriate participants).
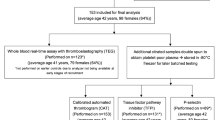
In the present analysis, a subgroup of all KORA-Fit study participants was considered, meaning participants who took part in the S4 baseline survey (n = 1394 eligible persons). Of those, 856 S4 participants (61.4%) also took part in the KORA-Fit examination. Overall, 805 participants (378 men, 427 women) with available data on hemostatic parameters could be included in the analysis.
The Ethics Committee of the Bavarian Chamber of Physicians gave its approval for the study (KORA-Fit EC No 17040). All study participants gave written informed consent, and the study was performed in accordance with the Declaration of Helsinki.
Data collection
The study participants were interviewed by certified and trained study nurses on education/socioeconomic status, lifestyle factors, and medication use. In addition, a standardized medical examination was undertaken that included fasting blood sampling. Height and weight were measured, and body mass index (BMI) was calculated as weight in kilograms divided by height in m2. Blood pressure was measured with an automated oscillometric device (HEM-705CP, Omron Corporation, Tokyo, Japan) after a five-minute rest while sitting. Education years up to 10 years were categorized as “low“, over 10 years of schooling/studying as “high “education levels. A history of diabetes was categorized as yes or no. A participant was defined as physically active if he/she participated in sports in summer and winter and for more than 1 h per week in at least one season [18, 19]. Alcohol intake was calculated in grams per day [18]. Smoking status was classified into smoker, ex smoker and never smoker [18, 20]. Detailed information on the data collection, examination processes, and variable definitions in the KORA studies is described in detail elsewhere [18].
Laboratory measurements
All hemostatic factors were measured in citrate plasma. During blood sampling, the patients were in an overnight fasting state. The samples were then processed and stored at − 80 °C until analysis. The parameter aPTT (reference value 26–36 sec) was determined photometrically (Pathromtin SL, Siemens Healthcare). AT III activity (ref. value 78–113%) was measured via a chromogenic activity assay (Innovance Antithrombin-Assay, Siemens Healthcare). Fibrinogen (ref. value 210–400 mg/dl) was quantified photometrically and turbidimetrically (Multifibren U, Siemens Healthcare). D-dimers (ref. value < 500 μg/L) were analyzed using a particle-enhanced immunoturbidimetric assay (Innovance D-Dimer Kit, Siemens Healthcare).
Protein C and S activity (ref. value for protein C 70–140%; ref. value for protein S 73–130% for men, 52–126% for women) were determined by photometry (Berichrom Protein C, Siemens Healthcare; Hemoclot Protein S). Factor VIII activity (ref. value 70–150%) was measured by photometry (coagulation factor VIII deficient plasma reagents used with Pathromtin SL reagents, Siemens Healthcare). All measurements, except for the protein S activity (CaoChrom analyzer (Wien, Austria)), were performed on a Siemens BCS-XP analyzer (Siemens, Eschborn, Germany).
After overnight fasting, serum blood samples were collected and kept at room temperature until centrifugation. Serum was separated after 30 minutes. Samples were assayed immediately at the laboratory of the University Hospital Großhadern (Ludwig-Maximilians Universität, München). Serum total cholesterol and HDL-c were measured enzymatically on a Cobas 8000 c702 Roche chemistry analyzer (Hoffmann-La Roche AG, Basel/Switzerland). The Friedewald formula was used for calculating LDL-c [21]. Non-HDL-c was calculated via subtraction of HDL-c from total cholesterol. Serum triglycerides were determined by an enzymatic color test (according to Trinder) (Hoffmann-La Roche AG Basel/Switzerland) on a Cobas 8000 c702 (Hoffmann-La Roche AG Basel/Switzerland).
Statistical analysis
Continuous variables were described by means ± standard deviations (SD) in the case of normal distribution. Nonnormally distributed variables were given as median and interquartile range (IQR). The Shapiro–Wilk test was used to check if the data were normally distributed. Means of normally distributed variables were compared by the two-sided t test. Median values (not normally distributed variables) were compared by the Mann–Whitney U test. Categorial variables were compared via Fisher’s exact test.
Multivariable linear regression models were used to investigate possible associations between the different serum lipid parameters (continuous variables) and aPTT, AT III, fibrinogen, D-dimer, protein C, protein S, and factor VIII. Participants taking anticoagulative medication were excluded from the analyses. The models were adjusted for the following confounders: BMI, age, sex (only in the total sample), education years, alcohol consumption, systolic blood pressure, smoking status, history of diabetes, and intake of lipid-lowering drugs. We performed additional analyses to account for clinical perspective and interpretation, using the lipid parameters in a binary way (abnormal vs. normal).
It was investigated whether the exposure-outcome associations (that is, lipid-coagulation factor associations) were modified by sex or age using formal tests for interaction (significance level 5%). The linearity assumption was tested by adding additional second-degree polynomial transformations of continuous covariates. Multicollinearity and heteroscedasticity were assessed by calculating the variance inflation factor and performing the Breusch–Pagan test, respectively. Finally, the assumption of normally distributed residuals was ensured by visual assessment of the respective Q-Q plots. P values < 0.05 were considered statistically significant. The statistical software IBM SPSS, version 28, was used for data analysis.
Results
Table 1 shows the sex-specific characteristics of the study sample. The mean age was the same for men and women (63.1 years). On average, men had a higher BMI (28.4 vs. 27.4) and were more often highly educated (68% vs. 60%) than women. Smoking status also differed between the sexes. While 65.6% of all men were smokers or ex-smokers, this was the case for only 50.8% of all women.
The aPTT values in men were higher than those in women (31.5 sec vs. 30.6 sec). Furthermore, protein C activity was higher in women (119.9% vs. 127.9%), while protein S activity was higher in men (137.1% vs. 120.9%). All other coagulation parameters showed no notable differences between males and females.
Total cholesterol, HDL cholesterol, LDL cholesterol, and triglycerides were different between the two sexes: total cholesterol levels in men were significantly lower than in women, as well as HDL-c and LDL-c. TGs were higher in men than in women.
In the whole population, LDL-c, total cholesterol, and non-HDL-c were positively associated with AT III, protein C and protein S activity. HDL-c was inversely related to aPTT and fibrinogen. Furthermore, there was a positive association between triglycerides and protein C and protein S activity (see Table 2).
Due to significant interactions with sex indicating different effect sizes for men and women in the multivariable linear regression models, the analyses were stratified by sex. In men, total cholesterol was inversely associated with aPTT and positively associated with protein C activity. HDL-c was inversely related to both aPTT and fibrinogen. LDL-c, non-HDL-c and TG values showed positive associations with protein C and protein S activity (see Table 3).
In women, total, LDL and non-HDL cholesterol were positively related to AT III concentrations as well as protein C and protein S activity. In addition, non-HDL-c was positively associated with factor VIII activity. For men, HDL-c was inversely related to fibrinogen. TG concentrations showed a positive association with protein C activity (see Table 4).
All findings were supported by regression models using the lipid parameters in a binary way (abnormal versus normal) (see Additional file 1, Tables 1, 2 and 3).
Discussion
The present study showed that commonly measured hemostatic factors were associated with several blood lipid markers in individuals from the general population. There were significant sex-specific differences; in particular, more notable associations, especially with non-HDL-c, could be observed in women. However, commonalities between the sexes could be found in the inverse relationship of HDL-c and fibrinogen and positive relationships of LDL-c as well as non-HDL-c with protein C.
Protein C and its cofactor protein S are vitamin K-dependent coagulation inhibitors and play an important role in fibrinolytic processes [22]. In both sexes, these two coagulation factors showed similar associations with total cholesterol, LDL-c, and non-HDL-c; TGs were associated with both coagulation inhibitors in men, but in women, they were only related to protein C. A positive correlation of protein C with LDL-c was also found in the ARIC Study [23], and in a Polish study, protein C activity was associated with hypercholesterolemia [24]. Women had higher protein C activity than men, and protein S activity was significantly higher in men. Protein C activity is known to change in women taking oral contraceptives or who are pregnant [25]. Since this was not the case in the present study, because the mean age of the women was 63.1 years, it could be assumed that in postmenopausal women, protein C activity might be higher compared to men. Similar to protein C and protein S, AT III also has antithrombotic properties and inhibits serine protease factors II, IX, X, XI, and XII [26]. In the present study, the AT III activity in women was significantly higher than that in men. Furthermore, in females, a significant association between total cholesterol, LDL-c and non-HDL-c and AT III was observed, but none of the lipid parameters were associated with AT III in men. This result is in accordance with findings from the ARIC study [27], which observed higher AT III concentrations in women than in men. Furthermore, in a study from Japan including hyperlipidemic and normolipidemic elderly individuals, in both groups, serum total cholesterol correlated positively with AT III activity [28]. In contrast, there was no notable association between LDL-c and AT III in the ARIC study [27]. A Polish study including a random sample of community-dwelling older individuals also did not find an association between AT III activity and total cholesterol and LDL-c [29]. In addition, total cholesterol was not associated with AT III in a study on 130 healthy adults aged 20–60 years from Poland [24].
Contrary to prior studies [27, 30, 31], fibrinogen values did not differ between men and women in the present investigation. A number of previous studies [30,31,32,33], but not all [34, 35], reported a positive association between fibrinogen and LDL-c. In the present study, no independent association between fibrinogen and LDL-c was observed, but an inverse relationship between fibrinogen and HDL-c in both sexes was found. This result agrees with findings from ARIC [8, 14] but could not be confirmed by other investigations [31, 32, 36]. D-dimer levels did not differ between males and females and showed no significant association with any of the different lipid parameters. In contrast, in the Dallas Heart Study, in linear regression analyses, D-dimer, a marker of fibrin formation and lysis, was significantly higher in females than in males even after multivariable adjustment for a number of covariables, including body composition [37].
In the present study, a significant relationship between factor VIII activity and non-HDL-c was observed in women. No other lipid parameters showed a relationship with factor VIII. Furthermore, no notable differences in factor VIII concentrations were found between the two sexes. This is in contrast to the ARIC study, where the mean levels of Factor VIII were higher in men than in women [23]. In addition, in ARIC in univariable analysis, factor VIII was negatively associated with HDL-c and positively associated with LDL-c [23]. In the third Glasgow MONICA Survey II [14], factor VIII correlated with cholesterol in women but not men. There are no prior studies on the association between non-HDL-c and hemostatic factors. Thus, the findings of the present study have to be confirmed by further investigations.
An inverse association between HDL-c and aPTT, a summary index for intrinsic and common pathways, was found in men but not in women in the present study. Furthermore, in males but not females, total cholesterol was inversely related to aPTT, which is a widely used routine screening test of the coagulation system. It could be shown that patients with hypercholesterolemia had shorter aPTT values than patients with lower cholesterol levels [38]. The results of the present study in men are consistent with this finding, but it is unclear why women do not show this relationship. Furthermore, contrary to this finding, no correlation between HDL-c and aPTT was observed in a prior study [39]. In contrast to the study of Chan et al. [40], where TGs were also related to aPTT, in the present study, such an association could not be observed.
As an underlying mechanism for the association between blood lipid levels and hemostasis factors, a previous study suggested that hypercholesterolemia may affect the regulation of blood coagulation via tissue factor pathway inhibitor (TFPI) [41]. TFPI, formerly also called lipoprotein-associated coagulation inhibitor [42] or extrinsic pathway inhibitor [43], is a protease inhibitor of the first steps of the extrinsic blood coagulation pathway. Increased TFPI activity was found in patients with hyperlipidemia [44], and there are positive correlations between plasma TFPI activity and total cholesterol [45] as well as LDL cholesterol levels [44]. In addition, studies have shown that hyperlipidemia may be associated with decreased activation of protein C, which in its activated form can inhibit several steps in the blood coagulation pathways.
Comparisons with other studies and what does the current work add to the existing knowledge
Prior studies observed possible effects of dyslipidemia on the coagulation system [23, 24, 27, 28, 30,31,32,33,34,35]. The present study found that sex is a moderator responsible for different effects in men and women regarding the relationships between lipid concentrations and coagulation factors.
Study strengths and limitations
The strengths of this study are the sample size, the availability of standardized measured laboratory data, information on medication intake, and standardized assessed cardiovascular risk factors. There are also certain limitations. The analysis was based on a follow-up study of a population-based study. Thus, it could be assumed that the participants are not representative of the initial population-based sample. Selection bias that may have affected the present results cannot be entirely excluded. This study included German subjects born between 1945 and 1964, so the results do not apply to other age groups and individuals of other ethnic origins.
Conclusions
There appear to be sex-specific differences regarding various associations between blood lipid levels and hemostatic factors in individuals from the general population. Therefore, in clinical practice, the role of lipid concentrations in the pathogenesis of venous thromboembolism (VTE) should not be neglected. Patients at high risk for developing venous thromboembolism could benefit from a reduction in lipid concentrations, e.g., by treatment with lipid-lowering drugs.
Availability of data and materials
The data that support the findings of this study are available from Helmholtz Zentrum München, but restrictions apply to the availability of these data, which are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of Helmholtz Zentrum München.
Abbreviations
- aPTT:
-
Activated partial thromboplastin time
- AT III:
-
Antithrombin III
- BMI:
-
Body mass index
- CHD:
-
Coronary heart disease
- CVD:
-
Cardiovascular disease
- HDL-c:
-
High-density lipoprotein cholesterol
- IQR:
-
Interquartile range
- KORA:
-
Cooperative Health Research in the Region of Augsburg, Germany
- LDL-c:
-
Low-density lipoprotein cholesterol
- Non-HDL-c:
-
Non-HDL cholesterol
- SD:
-
Standard deviation
- TG:
-
Triglycerides
- VTE:
-
Venous thromboembolism
References
Bays HE, Kulkarni A, German C, Satish P, Iluyomade A, Dudum R, et al. Ten things to know about ten cardiovascular disease risk factors – 2022. Am J Prev Cardiol. 2022;10:100342.
Klag MJ, Ford DE, Mead LA, He J, Whelton PK, Liang KY, et al. Serum cholesterol in young men and subsequent cardiovascular disease. N Engl J Med. 1993;328:313–8.
Anderson KM, Castelli WP, Levy D. Cholesterol and mortality. 30 years of follow-up from the Framingham study. JAMA. 1987;257:2176–80.
Carbayo Herencia JA, Simarro Rueda M, Palazon Bru A, Molina Escribano F, Ponce Garcia I, Artigao Rodenas LM, et al. Todos en nombre del Grupo de Enfermedades Vasculares de Albacete (GEVA). Evaluation of non-HDL cholesterol as a predictor of non-fatal cardiovascular events in a prospective population cohort. Clin Investig Arterioscler. 2018;30:64–71.
Nishizawa Y, Shoji T, Kakiya R, Tsujimoto Y, Tabata T, Ishimura E, et al. Non-high-density lipoprotein cholesterol (non-HDL-C) as a predictor of cardiovascular mortality in patients with end-stage renal disease. Kidney Int Suppl. 2003;84:S117–20.
Meade TW, Mellows S, Brozovic M, Miller GJ, Chakrabarti RR, North WR, et al. Haemostatic function and ischemic heart disease: principal results oft he Northwick Park heart study. Lancet. 1986;2:533–7.
Baker IA, Eastham R, Elwood PC, Etherington M, O’Brien JR, Sweetnam PM. Haemostatic factors associated with ischaemic heart disease in men aged 45 to 64 years. The Speedwell. Study Br Heart J. 1982;47:490–4.
Folsom AR, Conlan MG, Davis CED, Wu KK. For the atherosclerosis in communities (ARIC) study investigators. Relations between hemostasis variables and cardiovascular risk factors in middle-aged adults. Ann Epidemiol. 1992;2:481–94.
Maseri A, Fuster V. Is there a vulnerable plaque? Circulation. 2003;107:2068–71.
Song B, Shu Y, Xu YN, Fu P. Plasma fibrinogen level and risk of coronary heart disease among Chinese population: a systematic review and meta-analysis. Int J Clin Exp Med. 2015;8:13195–202.
Lowe G, Rumley A. The relevance of coagulation in cardiovascular disease: what do the biomarkers tell us? Thromb Haemost. 2014;112:860–7.
El-Hazmi MA. Hematological risk factors for coronary heart disease. Med Princ Pract. 2002;11(Suppl 2):56–62.
Georgieva AM, Cate HAT, Keulen ETP, van Oerle R, Govers-Riemslag JWP, Hamulyak K, et al. Prothrombotic markers in familial combined hyperlipidemia: evidence of endothelial cell activation and relation to metabolic syndrome. Atherosclerosis. 2004;175:345–51.
Woodward M, Lowe GDO, Rumley A, Tunstall-Pedoe H, Philippou H, Lane DA, et al. Epidemiology of coagulation factors, inhibitors and activation markers: the third Glasgow MONICA survey II. Relationships to cardiovascular risk factors and prevalent cardiovascular disease. Br J Haematol. 1997;97:785–97.
Wada H, Mori Y, Kaneko T, Wakita Y, Minamikawa K, Ohiwa M, et al. Hypercoagulable state in patients with hypercholesteriolemia: effects of pravastin. Clin Ther. 1992;14:829–34.
Poredos P, Jezovnik MK. Dyslipidemia, statins, and venous thromboembolism. Semin Thromb Hemost. 2011;37:897–902 Review.
Löwel H, Döring A, Schneider A, Heier M, Thorand B, Meisinger C, et al. The MONICA Augsburg surveys – basis for prospective cohort studies. Gesundheitswesen. 2005;67(Suppl 1):S13–8.
Meisinger C, Thorand B, Schneider A, Stieber J, Döring A, Löwel H. Sex differences in risk factors for incident type 2 diabetes mellitus: the MONICA Augsburg cohort study. Arch Intern Med. 2002;162:82–9.
Meisinger C, Löwel H, Thorand B, Döring A. Leisure time physical activity and the risk of type 2 diabetes in men and women from the general population. The MONICA/KORA Augsburg Cohort Study. Diabetologia. 2005;48:27–34.
Meisinger C, Döring A, Thorand B, Löwel H. Association of cigarette smoking and tar and nicotine intake with the development of type 2 diabetes mellitus in men and women from the general population: the MONICA/KORA Augsburg cohort study. Diabetologia. 2006;49:1770–6.
Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use oft he preparative ultracentrifuge. Clin Chem. 1972;18:499–502.
Hansen JB, Grimsgaard S, Huseby N, Sandset PM, Bonaa KH. Serum lipids and regulation of tissue factor-induced coagulation in middle-aged men. Thromb Res. 2001;102:3–13.
Conlan MG, Folsom AR, Finch A, Davis CE, Sorlie P, Wu KK. Correlation of plasma protein C levels with cardiovascular risk factors in middle-aged adults: the atherosclerosis risk in communities (ARIC) study. Thromb Haemost. 1993;70:762–7.
Koscielniak B, Wypasek E, Undas A. Determinants of elevated levels of natural anticoagulants in healthy subjects. Adv Clin Exp Med. 2015;24:791–800.
Trigg DE, Wood MG, Kouides PA, Kadir RA. Hormonal influences on hemostasis in women. Semin Thromb Hemost. 2011;37:077–86.
High KA. Antithrombin III, protein C, and protein S. Naturally occurring anticoagulant proteins. Arch Pathol Lab Med. 1988;112:28–36.
Folsom AR, Wu KK, Davis CE, Conlan MG, Sorlie PD, Szklo M. Population correlates of plasma fibrinogen and factor VII, putative cardiovascular risk factors. Atherosclerosis. 1991;91:191–205.
Kario K, Matsuo T. Lipid-related hemostatic abnormalities in the elderly: imbalance between coagulation and fibrinolysis. Atherosclerosis. 1993;103:131–8.
Kostka B, Para J, Drygas W, Kostka T. Antithrombin III activity in the elderly – association with cardiovascular disease risk factors. Przegl Lek. 2005;62(Suppl 3):35–8.
Lee AJ, Smith WCS, Lowe GDO, Tunstall-Pedoe H. Plasma fibrinogen and coronary risk factors. The Scottish heart health study. J Clin Epidemiol. 1990;43:913–9.
Balleisen L, Assmann G, Bailey J, Epping PH, Schulte H, van de Loo J. Epidemiological study on factor VII, factor VIII and fibrinogen in an industrial population: II. Baseline data on the relation to blood pressure, blood glucose, uric acid, and lipid fractions. Thromb Haemost. 1985;54:721.
Moller L, Kristensen TS. Plasma fibrinogen and ischemic heart disease risk factors. Arterioscler Thromb. 1991;11:344.
Korsan-Bengtsen K, Wilhelmsen L, Tibblin G. Blood coagulation and fibrinolysis in a random sample of 788 men 54 years old. II. Relations of the variables to “risk factors” for myocardial infarction. Thromb Diathes Haemorrh. 1972;28:99.
Kannel WB, Wolf PA, Castelli WP, D’Agostino RB. Fibrinogen and risk of cardiovascular disease. Thr Framingham Study. JAMA. 1987;258:1183.
Meade TW, Chakrabarti R, Haines AP, North WRS, Stirling Y. Characteristics affecting fibrinolytic activity and plasma fibrinogen concentrations. Br Med J. 1979;1:153.
Bonithon-Kopp C, Scarabin PY, Bara L, Castanier N, Jacqueson A, Roger M. Relationship between sex hormones and haemostatic factors in healthy middle-aged men. Atherosclerosis. 1988;71:71.
Lew J, Sanghavi M, Ayers CR, McGuire DK, Omland T, Atzler D, et al. Sex-based differences in cardiometabolic biomarkers. Circulation. 2017;135:544–55.
Chan P, Tomlinsoin B, Tsai CW, Pan WH, Lee YS. Thrombophilia in patients with hypercholesterolemia. Metabolism. 1996;45:966–99.
Kim JA, Kim JE, Song SH, Kim HK. Influence of blood lipids on global coagulation test results. Ann Lab Med. 2015;35:15–21.
Chan P, Huang TY, Shieh SM, Lin TS, Tsai CW. Thrombophilia in patients with hypertriglyceridemia. J Thromb Thrombolysis. 1997;4:425–9.
Kowaka T, Abumiya T, Kimura T, Harada-Shiba M, Koh H, Tsushima M, et al. Tissue factor pathway inhibitor activity in human plasma. Arterioscler Thromb Vasc Biol. 1995;15:504–10.
Wun TC, Kretzmer KK, Girard TJ, Miletich JP, Broze GJ. Cloning and characterization of a cDNA coding for the lipoprotein-associated coagulation inhibitor shows that it consists of three tandem Kunitz-type inhibitorydomains. J Biol Chem. 1988;263:6001–4.
Rao LVM, Rapaport SI. Studies of a mechanism inhibiting the initiation of the extrinsic pathway of coagulation. Blood. 1987;69:645–51.
Hansen JB, Huseby NE, Sandset PM, Svensson B, Lyngmo V, Nordoy A. Tissue factor pathway inhibitor and lipoproteins: evidence for association with and regulation by LDL in human plasma. Arterioscler Thromb. 1994;14:223–9.
Sandset PM, Larsen ML, Abildgaard U, Lindahl AK, Odegaard OR. Chromogenic substrate assay of extrinsic pathway inhibitor (EPI): levels in the normal population and relation to cholesterol. Blood Coagul Fibrinolysis. 1991;2:425–33.
Acknowledgments
The KORA study was initiated and financed by the Helmholtz Zentrum München – German Research Center for Environmental Health, which is funded by the German Federal Ministry of Education and Research (BMBF) and by the State of Bavaria. Data collection in the KORA study is done in cooperation with the University Hospital of Augsburg. Furthermore, KORA research was supported within the Munich Center of Health Sciences (MC-Health), Ludwig-Maximilians-Universität, as part of LMUinnovativ.
Funding
Open Access funding enabled and organized by Projekt DEAL. This research did not receive any specific funding.
Author information
Authors and Affiliations
Contributions
JVvF analyzed and interpreted the data and wrote the manuscript. DF and CM supervised the analysis and interpreted the data. JL and CM were responsible for the design of the study. AP and MH were responsible for the implementation and conduct of the KORA-Fit Study. DT was responsible for the measurement of the lipid parameters. All authors critically reviewed the manuscript and approved the final version to be published.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committees of the Bavarian Chamber of Physicians (KORA-Fit EC No 17040). The study was performed in accordance with the Declaration of Helsinki. All study participants gave written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table 1.
Results of the linear regression (ß value, 95% CI, p value) on the associations between categorized serum lipids (abnormal vs. normal) and coagulation parameters in both sexes (KORA-Fit). Table 2. Results of the linear regression (ß value, 95% CI, p value) on the associations between categorized serum lipids (abnormal vs. normal) and coagulation parameters in men (KORA-Fit). Table 3. Results of the linear regression (ß value, 95% CI, p value) on the associations between categorized serum lipids (abnormal vs. normal) and coagulation parameters in women (KORA-Fit).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
von Falckenstein, J.V., Freuer, D., Peters, A. et al. Sex-specific associations between serum lipids and hemostatic factors: the cross-sectional population-based KORA-fit study. Lipids Health Dis 21, 143 (2022). https://doi.org/10.1186/s12944-022-01757-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-022-01757-0