
Abstract
Background
Conicity index, body-shape index, lipid accumulation product (LAP), waist circumference (WC), triglyceride, triglyceride-glucose (TyG) index, hepatic steatosis index (HSI), waist-to-height ratio (WHtR), TyG index-related parameters (TyG-WHtR, TyG-BMI, TyG-WC), body mass index (BMI), visceral adiposity index, triglyceride to high-density lipoprotein cholesterol ratio and body roundness index have been reported as reliable markers of non-alcoholic fatty liver disease (NAFLD). However, there is debate about which of the above obesity and lipid-related indices has the best predictive performance for NAFLD risk.
Methods
This study included 6870 female and 7411 male subjects, and 15 obesity and lipid-related indices were measured and calculated. NAFLD was diagnosed by abdominal ultrasound. The area under the curve (AUC) of 15 obesity and lipid-related indices were calculated by receiver operating characteristic (ROC) analysis.
Results
Among the 15 obesity and lipid-related indices, the TyG index-related parameters had the strongest association with NAFLD. ROC analysis showed that except for ABSI, the other 14 parameters had high predictive value in identifying NAFLD, especially in female and young subjects. Most notably, TyG index-related parameters performed better than other parameters in predicting NAFLD in most populations. In the female population, the AUC of TyG-WC for predicting NAFLD was 0.9045, TyG-BMI was 0.9084, and TyG-WHtR was 0.9071. In the male population, the AUC of TyG-WC was 0.8356, TyG-BMI was 0.8428, and TyG-WHtR was 0.8372. In addition, BMI showed good NAFLD prediction performance in most subgroups (AUC>0.8).
Conclusions
Our data suggest that TyG index-related parameters, LAP, HSI, BMI, and WC appear to be good predictors of NAFLD. Of these parameters, TyG index-related parameters showed the best predictive potential.
Similar content being viewed by others

Background
Non-alcoholic fatty liver disease (NAFLD) is recognized as an important risk factor for peripheral vascular disease, diabetes, kidney disease, and cardio-cerebrovascular disease, and its most significant feature is hepatic steatosis [1,2,3]. In addition to hepatic steatosis, NAFLD also includes pathological changes such as nonalcoholic steatohepatitis and cirrhosis characterized by liver cell injury, fibrosis activation, and inflammation of lobular necrosis [3, 4]. NAFLD is not a benign, static disease, and without intervention, patients with hepatic steatosis will progress to liver fibrosis over time [5].
In recent decades, with changes in diet, the prevalence of obesity, and the increasing lack of physical exercise, the proportion of patients with NAFLD has increased rapidly [6]. According to the global survey report of NAFLD in 2016, the prevalence of NAFLD diagnosed by imaging exceeded 25%, including 31.79% in the Middle East, 30.45% in South America, 24.13% in North America, 27.37% in Asia, and 23.71% in Europe [7]. The increasing burden of NAFLD is a serious global public health challenge [7, 8].
However, at present, the gold standard for NAFLD diagnosis is still based on liver biopsy results [9]. This invasive examination method is extremely inconvenient for routine health surveillance and large-scale epidemiological investigation of the general population and runs counter to the Helsinki Declaration. Therefore, many studies have focused on identifying simple and effective alternatives for epidemiological investigations and extensive population health surveillance to facilitate early identification of patients most likely to develop NAFLD [10, 11]. In this context, a number of simple anthropometric indicators, biochemical indicators, and some combination of indicators, and even complex digital models have been developed to assess NAFLD risk. Among them, obesity and lipid-related indices are the most effective markers for predicting NAFLD and are widely used in epidemiological studies, including triglyceride (TG), conicity index (COI), visceral adiposity index (VAI), triglyceride-glucose (TyG) index, body roundness index (BRI), body mass index (BMI), hepatic steatosis index (HSI), waist circumference (WC), body-shape index (ABSI), waist-to-height ratio (WHtR), lipid accumulation product (LAP), triglyceride to high-density lipoprotein cholesterol (TG/HDL-C) ratio, and TyG index-related parameters (TyG-WHtR, TyG-BMI, TyG-WC) [12,13,14,15,16,17,18,19,20,21]. At present, there are very few comparative studies on the prediction of NAFLD by obesity and lipid-related indices. The conclusions of several existing studies are controversial, and do not include TyG index-related parameters [21,22,23]. According to some recent studies, TyG index-related parameters are promising new indicators for predicting NAFLD [14, 24]. It is critical to further compare TyG index-related parameters with other obesity and lipid-related indices and identify more useful biomarkers for predicting NAFLD. Therefore, the present study was designed to evaluate the best obesity and lipid-related indices for predicting NAFLD through an epidemiological survey of 14251 from the general population who underwent health screening.
Methods
Study design and data
The subjects of this study were from the NAGALA study, the design and implementation of which is described elsewhere [25]. In short, the NAGALA study, officially launched in 1994, is a population-based and ongoing cohort study of the general population who participated in a general health checkup at Murakami Memorial Hospital after the project was initiated. The NAGALA study aimed to assess NAFLD and diabetes by collating and analyzing medical data from the general population. The available data for research was shared by Fukui et al. with the Dryad database [26]. According to the terms of use of the database, different researchers can use the data for post-hoc analysis according to different research hypotheses, so that the data can play a greater role.
The present study was designed to further evaluate the most useful obesity and lipid-related indices for predicting NAFLD based on data from the large population in the NAGALA cohort. This study conducted a cross-sectional design according to the new research purpose, extracted the data of 20944 subjects who took part in the physical examination project from 2004 to 2015 in the NAGALA study, and set the following exclusion criteria according to the new research hypothesis: (a) Male subjects who had excessive alcohol intake during the baseline interview defined as consuming more than or equal to 210 g per week and female who consumed more than or equal to 140 g per week [27]. (b) Subjects diagnosed with alcoholic fatty liver, viral hepatitis, or diabetes at baseline. (c) Subjects with impaired fasting glucose at baseline visits. (d) Subjects taking drugs at the time of baseline examination. (e) Subjects with missing covariates. Finally, 14251 subjects who met the criteria were included in this study. Informed consent for the use of data was approved by subjects in previous studies [25], and the Murakami Memorial Hospital Research Ethics Committee authorized the NAGALA study. Since this study was a post-hoc analysis of the NAGALA study, there was no need to apply for ethical approval again. The whole study process follows the Declaration of Helsinki.
Data collection and measurement
As previously mentioned [25], the subjects' general clinical data and lifestyle factors were recorded using standardized self-completed questionnaires, including habit of exercise, sex, height, diastolic/systolic blood pressure (D/SBP), age, WC, weight, and smoking/drinking habits. The drinking status was divided into three categories by asking the subjects' weekly alcohol intake: no or little (<40 g/w), light or moderate (40–139 g/w and 140–209 g/w). The smoking status was divided into nonsmokers, former smokers, and current smokers at baseline. Habit of exercise were defined as subjects regularly participating in any type of exercise more than once a week. Hematological samples were collected in the morning after fasting for at least 8 hours. Gamma-glutamyl transferase (GGT), triglyceride (TG), fasting blood glucose (FPG), high-density lipoprotein cholesterol (HDL-C), alanine aminotransferase (ALT), hemoglobin A1c (HbA1c), total cholesterol (TC), and aspartate aminotransferase (AST) were analyzed and determined by an automatic analyzer according to the standard method.
The formulas for calculating obesity and lipid-related indices are shown in Fig. 1 [13,14,15,16,17,18,19,20,21].

Formulas for calculating obesity and lipid-related indices
Diagnosis of NAFLD
NAFLD diagnosis was based on the detection of hepatic steatosis by ultrasound while excluding drugs, viruses, or alcohol as the cause. Liver ultrasonography was performed by trained technicians, and experienced gastroenterologists examined the sonograms without knowing the subjects' clinical information and biochemical results. NAFLD diagnosis was based on the following four ultrasonic manifestations with a score of 0–6: liver brightness (0–4 points), hepatorenal echo contrast (0–4 points), vascular blurring (0–1 points), and deep attenuation (0–2 points). If the final score is greater than or equal to 2 points, a diagnosis was made [28].
Statistical analysis
Given the significant differences in body composition between males and females, all analyses were stratified according to sex. All data were analyzed using Empower (R) version 2.20 and R language version 3.4.3. Categorical variables were represented by numbers (%) and compared using the Pearson χ2 test. For continuous variables, the QQ plot and Shapiro–Wilk test were first used to check their distribution patterns. Continuous variables consistent with or approximately normal distribution were represented by the mean (standard deviation), while those with skewed distribution were represented by the median (interquartile range) and compared by nonparametric test or Student’s t-test. Multiple logistic regression models were established to calculate the odds ratio (OR) and corresponding 95% confidence intervals (CI) for NAFLD with different obesity and lipid-related indices. To allow direct comparison of OR values, 15 obesity and lipid-related indices were converted into Z-scores. The multivariate model adjusted for potential non-collinear confounding variables, such as GGT, age, drinking status, HbA1c, TC, smoking status, HDL-C, habit of exercise, and DBP (Supplementary Table 1). Additionally, to compare the predictive power of 15 obesity and lipid-related indices for NAFLD and determine the best threshold for each parameter, the ROC curve was used to analyze each parameter and find the point at which the sum of sensitivity + specificity was maximized to determine the best threshold for each parameter. Area under the curve (AUC) was interpreted according to the following criteria: <0.5, not useful; 0.5–0.7, poor; 0.7–0.9, good; and 0.9–1.0, excellent.
Results
Characteristics of the study subjects
The study included a total of 6870 female and 7411 male subjects, with mean ages of 43.27 and 44.78 years, respectively. Among these subjects, 478 females (3.35%) and 2029 males (14.24%) were diagnosed with NAFLD. Table 1 describes the general clinical characteristics, biochemical characteristics, and characteristics of obesity and lipid-related indices based on whether the study subjects were diagnosed with NAFLD. Some significant differences were observed between the groups with and without NAFLD. In both males and females, people with NAFLD had higher age, WHtR, LAP, AST, weight, BRI, BMI, TyG-WHtR, VAI, ALT/AST ratio, TyG index, HbA1c, TyG-BMI, ABSI, TG/HDL-C ratio, GGT, ALT, WC, TC, TG, FPG, S/DBP, HSI, TyG-WC, and COI. Additionally, among male subjects, there were also significant differences in physical exercise habits between NAFLD patients and healthy individuals, as NAFLD patients tended not to exercise.
Associations of 15 obesity and lipid-related indices with NAFLD
Table 2 shows the association between 15 obesity and lipid-related indices and NAFLD risk in males and females. As expected, 15 obesity and lipid-related indices were positively correlated with NAFLD before and after model adjustment. It is worth noting that NAFLD was strongly correlated with TyG-related parameters and HSI in both males and females, and TyG-WHtR was the most strongly correlated with NAFLD among all subjects (OR= 4.47 for men and OR = 5.56 for women, both P < 0.05). In addition, some anthropometric indicators, such as WC, BMI, and WHtR, were also strongly correlated with NAFLD in males. However, VAI, TG/HDL-C ratio, ABSI and TG were weakly correlated with NAFLD in the whole population.
Evaluate the accuracy of obesity and lipid-related indices in predicting NAFLD in the whole population
The accuracy of 15 obesity and lipid-related indices in predicting NAFLD in the whole population were first evaluated by ROC analysis. As shown in Table 3, the accuracy of the TyG index-related parameters, LAP, HSI, BMI, and WC in predicting NAFLD was relatively good. Among them, the AUC of TyG-BMI was the largest (0.8862), with a sensitivity of 0.8381, specificity of 0.7787, and best threshold of 189.6932.
Evaluate the accuracy of obesity and lipid-related indices in predicting NAFLD in different sexes
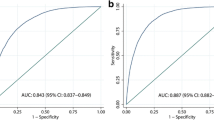
Figure 2 and Table 4 show the results of ROC analysis and the AUC of 15 obesity and lipid-related indices used to predict NAFLD in females and males. The AUCs of all 15 obesity and lipid-related indices were greater than 0.5, indicating that all have certain predictive values for NAFLD.

ROC curve analysis of NAFLD-related indicators in females and males. BMI: Body mass index; TyG-BMI: Triglyceride-glucose index-related body mass index; TyG-WHtR: Triglyceride-glucose index-related waist-to-height ratio; TyG-WC: triglyceride-glucose index-related waist circumference; HSI: hepatic steatosis index; LAP: lipid accumulation product; NAFLD: non-alcoholic fatty liver disease
Among females, the AUC of TyG-related parameters were the largest, all of which were more than 0.90, in which TyG-WHtR was 0.9071 (95% CI: 0.8954–0.9188), TyG-BMI was 0.9084 (95% CI: 0.8964–9204), and TyG-WC was 0.9045 (95% CI: 0.8926–0.9163). The best thresholds of TyG-WHtR, TyG-BMI, and TyG-WC for predicting NAFLD were 3.8078, 178.7047, and 595.3694, respectively. Additionally, BMI, WC, WHtR, HSI, LAP, and BRI also had a high predictive performance for NAFLD, and their AUCs were greater than 0.85.
In males, the AUC of WC, BMI, WHtR, TyG-related parameters, HSI, LAP, and BRI was larger, all exceeding 0.8, BMI was 0.8160, WC was 0.8102, WHtR was 0.8156, TyG-WC was 0.8356, TyG-BMI was 0.8428, TyG-WHtR was 0.8372, HSI was 0.8383, LAP was 8227, and BRI was 0.8156. TyG-BMI was the best marker for predicting male NAFLD, and its best threshold was 196.8688. In contrast, ABSI's performance in predicting NAFLD was mediocre in both males and females.
Evaluate the accuracy of obesity and lipid-related indices in predicting NAFLD in different sex and age groups
Table 5 and Table 6 show the AUCs of 15 obesity and lipid-related indices for predicting NAFLD in females and males at different ages. In the young female population (age 18–30 years), except ABSI and COI, the remaining 13 obesity and lipid-related markers had excellent performance in predicting NAFLD (all AUC>0.9), among which LAP was the best predictor in the young female population (AUC=0.9801). In the middle-aged female population (age 31–45 years), WC, BMI, WHtR, TyG-WC, HSI, TyG-BMI, LAP, TyG-WHtR, and BRI were all excellent predictors of NAFLD, among which the AUC of TyG-BMI was the largest (AUC=0.9436). However, in females over 45 years old, the accuracy of obesity and lipid-related indices in predicting NAFLD decreased. TyG-WHtR was the best marker for predicting NAFLD in middle-aged and elderly females (age 46–60 years: AUC=0.8541), and TyG-BMI was the best marker for predicting NAFLD in older females (age>60 years: AUC=0.8853).
In males, a trend similar to that of females was observed. Compared with young and middle-aged males, obesity and lipid-related indices were less accurate in predicting NAFLD in males over 45 years old. TyG-WHtR was the best predictor of NAFLD in young males (age 18–330 years: AUC=0.8861). TyG-BMI was the best predictor of NAFLD in males aged 31 to 60 years (AUC=0.8580 for males aged 31–45 years, AUC=0.8148 for males aged 46–60 years). However, in older males (age>60 years), HSI was the best marker for predicting NAFLD (AUC=0.8381).
Discussion
This study assessed the ability of 15 commonly used, non-invasive obesity and lipid-related indices to predict NAFLD risk in the general population. The accuracy of ABSI in predicting individual NAFLD risk was limited in both males and females, while the other 14 markers showed better predictive performance for NAFLD, especially in females. Of mention, although there were some differences in the predictive performance of the 15 obesity and lipid-related indices among different populations, TyG index-related parameters were superior to other parameters in predicting NAFLD in most populations. Therefore, TyG-related parameters may be the best choice for NAFLD risk screening indicators in the general population.
Past studies have shown that obesity, metabolic disorders, and environmental factors all contribute to the occurrence and development of NAFLD. However, with the rapid development of society, changes in lifestyle, dietary structure, and the prevalence of obesity, the prevalence of NAFLD is increasing rapidly, bringing a series of adverse consequences [6,7,8]. Therefore, it is an urgent task to screen vulnerable groups for NAFLD as soon as possible. Because liver biopsy-based tests are invasive, expensive, and time-consuming, noninvasive methods are being widely studied as alternative indicators [10, 11]. Simple measurements such as WC, BMI, WHtR, and blood lipids have an independent correlation with NAFLD [12, 16, 17]. These findings were verified in this study. Compared with WC, WHtR, and TG, BMI was a better predictor of NAFLD. In addition, it is worth mentioning that in this study, the AUC of BMI in most subgroups was greater than 0.8, which means that BMI had a good predictive performance in most populations. Although the incorporation of TyG significantly improves the predictive value of NAFLD in most subgroups, considering the simplicity and convenience of BMI measurement, it does not require additional laboratory measurements, so it should also be considered in the general population.
TyG index is a combination of FPG and TG. Previous studies reported that the index can be used as a substitute marker for IR in the clinic [29,30,31]. Additionally, it can effectively identify NAFLD and evaluate the risk of NAFLD in females [13, 32]. This finding was further verified in the present study. ROC analysis found that the AUC of TyG index for predicting NAFLD was 0.8186 in females and 0.7458 in males. Additionally, the TyG index has better predictive performance in the young population (age 18–30 years, AUC=0.9391 for females; AUC=0.8480 for males). TyG index-related parameters are the combined parameters of the TyG index with WC, BMI, and WHtR, which were first reported by Ko et al. [33]. They pointed out that TyG index-related parameters had the highest AUC value for predicting IR compared to visceral obesity indicators, lipid parameters, lipid ratios, and adipokines. Subsequent studies showed that TyG index-related parameters were used to predict non-obese, overweight, and obese people's NAFLD better than TyG alone [14, 24, 33]. This study expands the sample size from a previous study and found that TyG index-related parameters have excellent prediction performance in most populations.
TG/HDL-C is the ratio of TG and HDL-C. Similar to the TyG index, the TG/HDL-C ratio can distinguish IR from NAFLD, which has been widely popularized in the clinic [15, 34]. According to Ko et al., the TG/HDL-C ratio is a better predictor of IR than lipid markers and adipokines alone, but its AUC was lower than that of TyG-BMI, VAI, TyG index, LAP, and TyG-WC [32]. Similar results were found in predicting NAFLD in this study, which may be closely related to IR [1, 35].
HSI is a NAFLD prediction model developed by Lee et al [18]. It is a combination of liver enzymes and BMI, and was confirmed in a large number of studies to have excellent predictive performance in predicting NAFLD [36, 37]. According to a recent report by Lin et al., HSI has better prediction performance for NAFLD than BMI, WHtR, LAP, BRI, COI, VAI, TyG index, waist-hip ratio, body adiposity index (BAI) and abdominal volume index (AVI) [21]. However, it is not clear whether TyG index-related parameters are better than HSI and other obesity and lipid-related indices in predicting NAFLD. In this context, the predictive performance of 15 common obesity and lipid-related indices for NAFLD were compared in this study. The results showed that HSI did have better NAFLD identification ability than other parameters, but TyG index-related parameters were better predictors of NAFLD than HSI. In a follow-up study, the Procino team analyzed the predictive value of HSI, WC, fatty liver index, BMI, waist/height0.5, AVI, WHtR, and BRI for NAFLD. Their findings contradicted the research of Lin et al., who found that the best indicator of NAFLD screening was AVI, not HSI [22]. Additionally, in a recent study, Zhang et al. evaluated the predictive value of relative fat mass, WC, ABSI, WHtR, COI, ponderal index, BMI, and LAP for NAFLD in the elderly; their study showed that LAP was the best marker of these parameters for predicting NAFLD [23]. This study confirms the conclusion of Zhang et al., and in further analysis, it was found that LAP was superior to the TyG index, WHtR, ABSI, COI, BMI, TG/HDL-C ratio, WC, VAI, TG, and BRI in both males and females. Additionally, it is worth noting that LAP was the best predictor of NAFLD for young females (age 18–30 years, AUC=0.9801). Compared with these previous studies, this study considered more obesity and lipid-related indices, as well as TyG index-related parameters, which have been widely considered recently [14, 24]. In general, TyG index-related parameters may be the best choice for NAFLD risk screening in the general population, whether male or female, whether young, middle-aged or elderly. More importantly, the indicators that make up the TyG index-related parameters are clinically easy to obtain and affordable, which brings great convenience for the prevention and treatment of NAFLD.
In the correlation analysis, the researchers calculated the OR value and 95% CI of the corresponding NAFLD risk after Z-conversion of 15 obesity and lipid-related indices. The results of the study were similar to the results of the ROC analysis. Among the 15 parameters, TyG index-related parameters had the strongest correlation with NAFLD risk, both before and after model adjustment. Although many parameters in this study have a strong correlation with NAFLD and the accuracy of predicting NAFLD was good, the TyG index-related parameters were best.
In this study, the best thresholds of TyG index-related parameters in different sex and different age groups were calculated by ROC analysis, in which the best thresholds of TyG-WHtR, TyG-WC, and TyG-BMI were 3.8078, 595.3694, and 178.7047 in females, respectively and 4.0945, 699.2287, and 196.8688 in males, respectively. Two previous studies also provided data for reference; in the study by Huang et al., the best threshold for TyG-BMI to predict NAFLD in non-obese people was 183.8263 [24]. Khamseh's team reported that the best threshold for NAFLD corresponding to TyG-WC in overweight and obese individuals was 876 [14], which was significantly higher than the best threshold recommended in this study. In view of the obvious differences among the study subjects, only a brief description and report of these results are provided as a reference for subsequent studies.
Study strength and limitations
Several positive effects should be noted. First, the biggest advantage of this study is that of the 15 obesity and lipid-related indices, TyG index-related parameters had the highest accuracy for predicting NAFLD. Second, this study is based on data analysis of a large sample, and the conclusion can be regarded as relatively reliable. Finally, the study was stratified by sex and age to identify the best parameters and thresholds for predicting NAFLD for different populations. These results provide a reliable reference for precision treatment.
The study has some limitations. First, this study lacks general measurement information such as hip/neck circumference. To our knowledge, the new index combining the TyG index with hip/neck circumference was recently found to have high diagnostic value for IR [38]. IR is the main mediating factor in the pathogenesis of NAFLD [1], and the combination of the TyG index and hip/neck circumference may have excellent performance in the prediction of NAFLD. In addition, due to the lack of hip circumference, AVI and BAI cannot be calculated, so it was not possible to further evaluate the difference in NAFLD between AVI, BAI, and other obesity and lipid-related indices. Second, the diagnosis of NAFLD was made only on the basis of ultrasound. Although the current ultrasound diagnosis has high sensitivity and specificity, it is undeniable that nearly 30% of mild fatty liver may be missed [39], which means that the true prevalence rate of NAFLD in this study may be higher. Third, because the dataset analyzed comes from a public database, the dataset provided in the database cannot be updated, which lacks some parameters used to calculate the score of non-invasive fibrosis. Therefore, unfortunately, staging information on liver fibrosis cannot be provided in the current study. Fourth, the study used data from the Japanese population, so its conclusions may not apply to other ethnic groups. Finally, the research design may be a limitation. The cross-sectional design adopted in this study restricts us from explaining the causal correlation of these variables.
Conclusion
TyG index-related parameters may be the best choice for NAFLD risk screening in the general population. Considering that the calculation of the TyG index-related parameters is simple and convenient, it is suggested that the TyG index-related parameters should be included in the NAFLD risk assessment list as a marker of focus. The findings of this study provide more comprehensive and referential information for the prevention and treatment of NAFLD and add strong evidence for the non-invasive evaluation of NAFLD.
Availability of data and materials
The datasets that support the conclusions of this article can be found in the DRYAD repository.
Abbreviations
- NAFLD:
-
non-alcoholic fatty liver disease
- WHtR:
-
waist-to-height ratio
- WC:
-
waist circumference
- BMI:
-
Body mass index
- TG:
-
triglyceride
- TyG:
-
triglyceride-glucose
- TyG-WC:
-
triglyceride-glucose index-related waist circumference
- TyG-BMI:
-
triglyceride-glucose index-related body mass index
- TyG-WHtR:
-
triglyceride-glucose index-related waist-to-height ratio
- HSI:
-
hepatic steatosis index
- VAI:
-
visceral adiposity index
- LAP:
-
lipid accumulation product
- ABSI:
-
body-shape index
- BRI:
-
body roundness index
- COI:
-
conicity index
- ALT:
-
Alanine aminotransferase
- AST:
-
aspartate aminotransferase
- GGT:
-
gamma-glutamyl transferase
- HDL-C:
-
high-density lipoprotein cholesterol
- TC:
-
total cholesterol
- TG:
-
triglyceride
- HbA1c:
-
hemoglobin A1c
- FPG:
-
fasting blood glucose
- OR:
-
odds ratio
- CI:
-
confidence intervals
- ROC:
-
receiver operating characteristic curve
- AUC:
-
area under the curve
- TG/HDL-C:
-
triglyceride to high-density lipoprotein
- IR:
-
insulin resistance
- S/DBP:
-
systolic/diastolic blood pressure
References
Byrne CD, Targher G. NAFLD: a multisystem disease. J Hepatol. 2015;62:S47–64.
Long MT, Wang N, Larson MG, Mitchell GF, Palmisano J, Vasan RS, et al. Nonalcoholic fatty liver disease and vascular function: cross-sectional analysis in the Framingham heart study. Arterioscler Thromb Vasc Biol. 2015;35:1284–91.
Ipsen DH, Lykkesfeldt J, Tveden-Nyborg P. Molecular mechanisms of hepatic lipid accumulation in non-alcoholic fatty liver disease. Cell Mol Life Sci. 2018;75:3313–27.
Bedossa P. Pathology of non-alcoholic fatty liver disease. Liver Int. 2017;37:85–9.
McPherson S, Hardy T, Henderson E, Burt AD, Day CP, Anstee QM. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using paired biopsies: implications for prognosis and clinical management. J Hepatol. 2015;62:1148–55.
Fazel Y, Koenig AB, Sayiner M, Goodman ZD, Younossi ZM. Epidemiology and natural history of non-alcoholic fatty liver disease. Metabolism. 2016;65:1017–25.
Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84.
Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15:11–20.
Hashimoto E, Taniai M, Tokushige K. Characteristics and diagnosis of NAFLD/NASH. J Gastroenterol Hepatol. 2013;28:64–70.
Castera L, Friedrich-Rust M, Loomba R. Noninvasive Assessment of Liver Disease in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology. 2019;156:1264-1281.e4.
Zhou JH, Cai JJ, She ZG, Li HL. Noninvasive evaluation of nonalcoholic fatty liver disease: Current evidence and practice. World J Gastroenterol. 2019;25:1307–26.
Mansour-Ghanaei R, Mansour-Ghanaei F, Naghipour M, Joukar F, Atrkar-Roushan Z, Tabatabaii M, et al. The role of anthropometric indices in the prediction of non-alcoholic fatty liver disease in the PERSIAN Guilan Cohort study (PGCS). J Med Life. 2018;11:194–202.
Zheng R, Du Z, Wang M, Mao Y, Mao W. A longitudinal epidemiological study on the triglyceride and glucose index and the incident nonalcoholic fatty liver disease. Lipids Health Dis. 2018;17:262.
Khamseh ME, Malek M, Abbasi R, Taheri H, Lahouti M, Alaei-Shahmiri F. Triglyceride Glucose Index and Related Parameters (Triglyceride Glucose-Body Mass Index and Triglyceride Glucose-Waist Circumference) Identify Nonalcoholic Fatty Liver and Liver Fibrosis in Individuals with Overweight/Obesity. Metab Syndr Relat Disord. 2021;19:167–73.
Fan N, Peng L, Xia Z, Zhang L, Song Z, Wang Y, et al. Triglycerides to high-density lipoprotein cholesterol ratio as a surrogate for nonalcoholic fatty liver disease: a cross-sectional study. Lipids Health Dis. 2019;18:39.
Zou Y, Sheng G, Yu M, Xie G. The association between triglycerides and ectopic fat obesity: An inverted U-shaped curve. PLoS One. 2020;15:e0243068.
Sheng G, Xie Q, Wang R, Hu C, Zhong M, Zou Y. Waist-to-height ratio and non-alcoholic fatty liver disease in adults. BMC Gastroenterol. 2021;21:239.
Lee JH, Kim D, Kim HJ, Lee CH, Yang JI, Kim W, et al. Hepatic steatosis index: a simple screening tool reflecting nonalcoholic fatty liver disease. Dig Liver Dis. 2010;42:503–8.
Dai H, Wang W, Chen R, Chen Z, Lu Y, Yuan H. Lipid accumulation product is a powerful tool to predict non-alcoholic fatty liver disease in Chinese adults. Nutr Metab (Lond). 2017;14:49.
Okamura T, Hashimoto Y, Hamaguchi M, Obora A, Kojima T, Fukui M. The visceral adiposity index is a predictor of incident nonalcoholic fatty liver disease: A population-based longitudinal study. Clin Res Hepatol Gastroenterol. 2020;44:375–83.
Lin IT, Lee MY, Wang CW, Wu DW, Chen SC. Gender Differences in the Relationships among Metabolic Syndrome and Various Obesity-Related Indices with Nonalcoholic Fatty Liver Disease in a Taiwanese Population. Int J Environ Res Public Health. 2021;18:857.
Procino F, Misciagna G, Veronese N, Caruso MG, Chiloiro M, Cisternino AM, et al. Reducing NAFLD-screening time: A comparative study of eight diagnostic methods offering an alternative to ultrasound scans. Liver Int. 2019;39:187–96.
Zhang Y, Li B, Liu N, Wang P, He J. Evaluation of Different Anthropometric Indicators for Screening for Nonalcoholic Fatty Liver Disease in Elderly Individuals. Int J Endocrinol. 2021;2021:6678755.
Li Y, Zheng R, Li J, Feng S, Wang L, Huang Z. Association between triglyceride glucose-body mass index and non-alcoholic fatty liver disease in the non-obese Chinese population with normal blood lipid levels: a secondary analysis based on a prospective cohort study. Lipids Health Dis. 2020;19:229.
Okamura T, Hashimoto Y, Hamaguchi M, Obora A, Kojima T, Fukui M. Ectopic fat obesity presents the greatest risk for incident type 2 diabetes: a population-based longitudinal study. Int J Obes (Lond). 2019;43:139-148.
Okamura T, et al. Data from: Ectopic fat obesity presents the greatest risk for incident type 2 diabetes: a population-based longitudinal study. Dryad, Dataset. 2019. https://doi.org/10.5061/dryad.8q0p192.
Choi JH, Sohn W, Cho YK. The effect of moderate alcohol drinking in nonalcoholic fatty liver disease. Clin Mol Hepatol. 2020;26:662–9.
Byrne CD. Ectopic fat, insulin resistance and non-alcoholic fatty liver disease. Proc Nutr Soc. 2013;72:412–9.
Mohd Nor NS, Lee S, Bacha F, Tfayli H, Arslanian S. Triglyceride glucose index as a surrogate measure of insulin sensitivity in obese adolescents with normoglycemia, prediabetes, and type 2 diabetes mellitus: comparison with the hyperinsulinemic-euglycemic clamp. Pediatr Diabetes. 2016;17:458–65.
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, Martínez-Abundis E, Ramos-Zavala MG, Hernández-González SO, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95:3347–51.
Sánchez-García A, Rodríguez-Gutiérrez R, Mancillas-Adame L, González-Nava V, Díaz González-Colmenero A, Solis RC, et al. Diagnostic Accuracy of the Triglyceride and Glucose Index for Insulin Resistance: A Systematic Review. Int J Endocrinol. 2020;2020:4678526.
Kitae A, Hashimoto Y, Hamaguchi M, Obora A, Kojima T, Fukui M. The Triglyceride and Glucose Index Is a Predictor of Incident Nonalcoholic Fatty Liver Disease: A Population-Based Cohort Study. Can J Gastroenterol Hepatol. 2019;2019:5121574.
Er LK, Wu S, Chou HH, Hsu LA, Teng MS, Sun YC, et al. Triglyceride Glucose-Body Mass Index Is a Simple and Clinically Useful Surrogate Marker for Insulin Resistance in Nondiabetic Individuals. PLoS One. 2016;11:e0149731.
Uruska A, Zozulinska-Ziolkiewicz D, Niedzwiecki P, Pietrzak M, Wierusz-Wysocka B. TG/HDL-C ratio and visceral adiposity index may be useful in assessment of insulin resistance in adults with type 1 diabetes in clinical practice. J Clin Lipidol. 2018;12:734–40.
Watt MJ, Miotto PM, De Nardo W, Montgomery MK. The Liver as an Endocrine Organ-Linking NAFLD and Insulin Resistance. Endocr Rev. 2019;40:1367–93.
Ciardullo S, Muraca E, Perra S, Bianconi E, Zerbini F, Oltolini A, et al. Screening for non-alcoholic fatty liver disease in type 2 diabetes using non-invasive scores and association with diabetic complications. BMJ Open Diabetes Res Care. 2020;8:e000904.
Song E, Kim JA, Roh E, Yu JH, Kim NH, Yoo HJ, et al. Long Working Hours and Risk of Nonalcoholic Fatty Liver Disease: Korea National Health and Nutrition Examination Survey VII. Front Endocrinol (Lausanne). 2021;12:647459.
Mirr M, Skrypnik D, Bogdański P, Owecki M. Newly proposed insulin resistance indexes called TyG-NC and TyG-NHtR show efficacy in diagnosing the metabolic syndrome. J Endocrinol Invest. 2021.
Ferraioli G, Soares Monteiro LB. Ultrasound-based techniques for the diagnosis of liver steatosis. World J Gastroenterol. 2019;25:6053–62.
Acknowledgments
Special thanks to Fukui et al for sharing the available data from the NAGALA study
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Conceptualization and research design: GT-S and YZ; Supervision: GT-S and YZ; Project administration: GT-S, YZ, SL, MB-K, QY-X and NP; Writing-Original draft preparation: GT-S, YZ, SL, MB-K, QY-X and NP; Writing- Reviewing and Editing: GT-S, YZ, SL, MB-K, QY-X and NP; The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Murakami Memorial Hospital Research Ethics Committee authorized the NAGALA study. Since this study is a post-hoc analysis of the NAGALA study, there is no need to apply for ethical approval again.
The entire study process follows the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
No competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sheng, G., Lu, S., Xie, Q. et al. The usefulness of obesity and lipid-related indices to predict the presence of Non-alcoholic fatty liver disease. Lipids Health Dis 20, 134 (2021). https://doi.org/10.1186/s12944-021-01561-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-021-01561-2