
Abstract
Background
The present study was aimed to establish a prediction model for in-stent restenosis (ISR) in subjects who had undergone percutaneous coronary intervention (PCI) with drug-eluting stents (DESs).
Materials and methods
A retrospective cohort study was conducted. From September 2010 to September 2013, we included 968 subjects who had received coronary follow-up angiography after primary PCI. The logistic regression analysis, receiver operator characteristic (ROC) analysis, nomogram analysis, Hosmer–Lemeshow χ2 statistic, and calibration curve were applied to build and evaluate the prediction model.
Results
Fifty-six patients (5.79%) occurred ISR. The platelet distribution width (PDW), total cholesterol (TC), systolic blood pressure (SBP), low-density lipoprotein cholesterol (LDL-C), and lesion vessels had significant differences between ISR and non-ISR groups (all P < 0.05). And these variables were independently associated with ISR (all P < 0.05). Furthermore, they were identified as predictors (all AUC > 0.5 and P < 0.05) to establish a prediction model. The prediction model showed a good value of area under curve (AUC) (95%CI): 0.72 (0.64–0.80), and its optimized cut-off was 6.39 with 71% sensitivity and 65% specificity to predict ISR.
Conclusion
The incidence of ISR is 5.79% in CAD patients with DES implantation in the Xinjiang population, China. The prediction model based on PDW, SBP, TC, LDL-C, and lesion vessels was an effective model to predict ISR in CAD patients with DESs implantation.
Similar content being viewed by others

Background
Coronary artery disease (CAD) is a high mortality disease in modern society [1, 2], and it is commonly treated with percutaneous coronary intervention (PCI) [3]. However, the occurrence of in-stent restenosis (ISR) increases the risk of stent failure [4]. Although drug-eluting stents (DESs) are widely applied, ISR is still a crucial issue in the treatment of CAD after PCI [5]. Nowadays, the incidence of ISR remains approximately 10%, which may cause the recurrence of ischemic heart disease [4, 6]. Until now, the incidence of ISR in the Xinjiang population, China, was not reported. Additionally, clinic is still lacking an appropriate prediction model to predict ISR [7]. Establishing a novel prediction model for ISR will contribute to individual risk stratification and ISR prevention for CAD patients [8].
ISR has a distinct pathophysiological process that is not merely accelerated atherosclerosis [9]. ISR is usually caused by increased acute vessel injury and the promotion of neointimal hyperplasia [10]. Acute thrombotic occlusion is a high frequent cause of in-stent chronic total occlusion [11], which is implied that platelets are important in ISR. In previous reports, several risk factors were related to ISR, including diabetes, chronic renal insufficiency, bare-metal stents, small coronary artery vessels, a long stent length, and coronary bifurcation lesions [4, 12]. Recently, studies revealed that the increase of C-reactive protein, homocysteine, and stent numbers are risk factors for ISR [13,14,15]. However, the roles of platelet parameters in ISR were still less reported. Platelet activation is persistent and usually accompanied by morphological changes after PCI. Inhibition of platelet activation has effects on neointimal proliferation and restenosis [16, 17]. Developing a novel prediction model based on platelet parameters, clinical characteristics, lipid levels, and angiographic characteristicsand may contribute to risk stratification and disease prevention for ISR in CAD patients.
Therefore, this study is set out to reveal the incidence of ISR in the Xinjiang population, China, and explore a potential prediction model for ISR in CAD patients with DES implantation.
Materials and methods
Participants
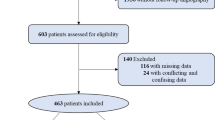
Nine hundred sixty-eight subjects who received PCI and coronary follow-up angiography from September 2010 to September 2013 were included. Inclusion criteria: 1) the subjects were diagnosed with CAD and had undergone PCI; 2) the patients had undergone follow-up angiography more than 6 months after PCI; 3) DESs were implanted; 4) the subjects were from the Han and Uyghur populations; 5) the subjects were aged over 18.
The exclusion criteria were as follows: 1) the patients had myocarditis, pericarditis, myocardiopathy, congenital heart disease, or other structural heart diseases; 2) the patients had other comorbidities, including immune system disease, infectious disease, tumors, or hematologic diseases.
Diagnostic criteria
ISR was defined as a restenosis degree > 50% based on coronary angiography, which included both the original site where the stent was placed and vascular segments adjacent to the stent at a 5-mm distance; if the restenosis degree was < 50%, the ISR was defined as non-ISR [18].
Data collection
Demographic information, biochemical parameters, clinical and angiographic characteristics were collected. Fasting blood samples collected from peripheral the vessel were obtained to test routine biochemical variables, including platelet parameters of plateletcrit (PCT), MPV, platelet count, platelet distribution width (PDW), lipid parameters of low-density lipoprotein cholesterol (LDL-C), triglyceride (TG), TC, and high-density lipoprotein-cholesterol (HDL-C). The blood samples were evaluated within 2 h. The specific data concerning angiography and the stents included the stenosis location, lesion vessels, the number of stents, stent parameters, and post-balloon dilatation.
Statistical analyses
To compare the difference between groups in continuous data, independent samples T-test was used between two groups, and one-way analysis of variance (ANOVA) and Student-Newman-Keuls (SNK) test were performed for more than three groups; the data were expressed as the means ± standard deviation (SD). For variables with an abnormal distribution, the Kruskal-Wallis H test was performed. A chi-squared test was used to compare categorical variables, and the data were expressed as percentages. Multivariate logistic regression analyses were conducted with forward stepwise selection, in which P-value levels for inclusion and exclusion criteria were set as 0.05 and 0.10, respectively. ROC analysis was performed for each variate associated with ISR, in which AUC > 0.5 and P < 0.05 were included in the prediction model. The Hosmer–Lemeshow χ2 statistic, calibration curve, and bootstrap for 1000 times were used to examine the prediction model. To further evaluate the discrimination of the model and optimized cut-off, the ROC analysis and Youden index were used. The internal validation was conducted by the bootstrap method. The total risk score for this prediction model was counted as the equation: Y = 0.1480*PDW + 0.1709*TC + 0.2639*LDL + 0.0121*SBP + 0.276*(lesion vessels), and the scales for each variable were assigned according to their corresponding beta-coefficient identified by multivariate logistic regression. Moreover, the risk score for each variable was conducted by nomogram analysis. A P-value < 0.05 was statistically significant. SPSS version 22.0 (SPSS Inc., Chicago, IL, USA) was used to perform statistical analyses in this study. The nomogram analysis and calibration curve were performed by R software version 4.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Clinical and angiographic characteristics between the ISR and non-ISR groups
Of 968 patients included in our study, 56 subjects (5.79%) had ISR after PCI for an average of 16.93 months. Most of the baseline characteristics between the two groups were similar, such as age, sex, blood glucose, current smoking, alcohol consumption, waist circumference, body mass index (BMI), post-balloon dilatation, balloon diameters, balloon lengths, stent diameters, and stent lengths (all P > 0.05). However, as Tables 1 and 2 shown, PDW, TC, HDL, LDL-C, SBP, myocardial infarction (MI), lesion vessels, and right coronary artery (RCA) stenosis showed significant differences between the groups (all P < 0.05).
Univariate analysis and multivariate analysis for potential predictors
The parameters of PDW, TC, LDL-C, SBP, MI, lesion vessels, and RCA stenosis were associated with ISR in CAD patients (all P < 0.05), and their ORs and 95% CIs were shown in Table 3. In addition, the elevated levels of PDW (OR 1.17; 95% CI; 1.05–1.31; P = 0.039), LDL-C (OR 1.34; 95% CI 1.02–1.76; P = 0.036), TC (OR 1.18; 95% CI; 1.01–1.39; P = 0.039), SBP (OR 1.01; 95% CI; 1.01–1.02; P = 0.014), lesion vessels (OR 1.32; 95% CI; 1.06–1.64; P = 0.012), and MI (OR 2.34; 95% CI; 1.32–4.15; P = 0.039) were still significantly associated with ISR after adjusting by TC, HDL, LDL-C, SBP, PDW, incidence of MI, lesion vessels, and RCA stenosis.
Identifying predictors in the prediction model for ISR
To identify potential predictors for ISR, the ROC analyses were conducted for each parameter which independently associated with ISR. At last, the SBP, PDW, TC, LDL-C, and lesion vessels were included in the prediction model, and their AUC and 95% CI were SBP [0.60 (0.51–0.69); P = 0.024], PDW [0.60 (0.53–0.67); P = 0.042], TC [0.63 (0.54–0.71); P = 0.005], and LDL-C [0.61(0.52–0.70); P = 0.046], lesion vessels [0.59 (0.52–0.66); P = 0.005], respectively (Table 4). To evaluate this prediction model, a Hosmer–Lemeshow goodness-of-fit test was conducted, which yielded P = 0.655, and a calibration curve was also displayed in Fig. 1A, indicating no deviation was observed between predicted and observed probability. An internal validation with 1000 times repetitions was performed, and demonstrated a good consistency. In addition, the AUC was 0.72(0.64–0.80) for the prediction model, P = 0.000, Fig. 1B.

Scoring and evaluating the prediction model. A nomogram was performed for the prediction model. The using instruction for the nomogram is that a line on the top labeled “Points” displays the corresponding score for the values of each variable; a line labeled “Total points”, representing an individual’s total points of all variables in the model, is corresponded to the line labeled “Risk” which indicates the risk of ISR for the individual. Abbreviations: LDL-C, low-density lipoprotein cholesterol; PDW, platelet distribution width; SBP, systolic blood pressure; TC, total cholesterol
Nomogram prediction for ISR
The parameters in the prediction model were used to calculate a probability of disease (POD) index which was calculated as the equation Y = 0.1480 ∗ PDW + 0.1709 ∗ TC + 0.2639 ∗ LDL + 0.0121 ∗ SBP + 0.276 ∗ (lesion vessels)A nomogram based on these variables was configured (Fig. 1C). The optimized cut-off for the POD index was 6.39, and its sensitivity and specificity were 71 and 65%, respectively. When the POD index > 6.39, subjects with a high risk of ISR, otherwise with low risk of ISR.
The association between the prediction model and ISR
As shown in Table 5, the POD index was divided as tertiles, compared with tertile 1 (T1), the OR and its 95%CI of ISR were 2.5 (95% CI: 1.02–6.11, P = 0.045) for tertile 2 (T2), and 4.95 (95% CI: 2.15–11.39, P = 0.000) for tertile 3 (T3).
Overview of the prediction model for ISR
As Fig. 2 shown, the overview of the prediction model was indicated, which ranking the predictors as risk scores and presenting actionable preventing methods for each variable.

Overview of the prediction model of ISR. The figure summarizes the content of the prediction model, including variables in the model, the lowest and highest risk score for each variable, and suggestions for risk factor control. Abbreviations: LDL, low-density lipoprotein cholesterol; PDW, platelet distribution width; SBP, systolic blood pressure; TC, total cholesterol
Discussion
An effective prediction model can provide useful references for disease prevention. Here, the incidence of ISR in CAD patients with DESs was revealed in the Xinjiang population, China. And a novel prediction model based on platelet parameters, and combined with clinical characteristics and angiographic results was established to predict ISR in patients with CAD and DESs implantation.
Platelet activation plays a crucial role in stent-thrombosis [19] which increased the risk of restenosis [11]. Some studies have explored the relationship between platelet parameter MPV and ISR, but conclusions were inconsistent. A study indicated that MPV is a predictor for ISR in Chinese subjects stented in the carotid artery [20]. While a European study showed that MPV was not a risk factor for ISR after stenting in Whites [21]. The differences may attribute to ethnic differences, for Asians have more prevalent diabetes mellitus, which tends to have higher MPV or clopidogrel resistance [22, 23]. Another platelet parameter PDW is an indicator that reflects the dispersion of the mean platelet volume (MPV), indicates platelet activation [24], and provides more information than MPV [25,26,27]. The raised PDW indicates an increasing platelet heterogeneity and the occurring of platelet size disparity. And PDW has been reported that associated with the severity and prognosis of CAD [28,29,30]. Instead of MPV, PDW is an effective predictor to predict ISR in the present study. And its potential mechanisms might be that platelet activation, indicated by elevated PDW, promotes secreting a plethora of chemokines after PCI, like, CXCL4, CXCL12, and CCL5 et al., which recruiting circulating neutrophils and lymphocytes to the place where vascular injured [31]. The process drives the low-grade inflammatory response and promoting the development of neointimal proliferation, and leads to restenosis progression [16, 17, 31, 32].
Raised circulating LDL-C levels play a vital role in atherosclerotic cardiovascular disease [33], and it affects the stenosis of coronary arteries by accelerating the progression of atherosclerosis [34]. Studies have been reported that elevated LDL-C is an independent predictor [15, 35], and comprised of it in prediction models for ISR might be effective [36]. TC is also an independent predictor for ISR in the present study. It has been indicated as an important component of prediction models for cardiovascular disease and recommended to be used to estimate total cardiovascular disease risks [37, 38].
Angiography examination is widely performed to diagnose CAD and to guide the PCI. In recent years, techniques of intravascular imaging detection, such as intravascular ultrasound (IVUS), are gradually applied in PCI. Many studies have revealed intravascular imaging detection has more advantages than angiography, displaying lesion with distinct characterization, and contributing to finding the etiology of ISR, furthermore, using it in PCI procedure decreases the major adverse cardiovascular events for ISR [39,40,41,42]. In this study, all PCI guidance or coronary artery examination was performed by the angiography, which may provide less information about lesion and miss some potential predictors. In further studies, establishing a prediction model combined with the lesion characters detected by intravascular imaging might be much valuable.
Comparisons with other studies and what does the current work add to the existing knowledge
The rates of ISR are varied from study to study in different patients or types of stents. The incidence of ISR is approximately 30% in patients implanted with bare-metal stenting [12]. The application of DESs has significantly reduced the incidence of ISR to 5–15%. While in subjects with diabetes or other comorbidities, the incidence is more than 20% although the DES is applied [25, 43, 44]. In line with previous studies, the incidence of ISR is 5.79% in the present study [4, 6, 14].
A recent study found that a prediction model including abnormal platelets could predict ISR [45]. And another study proved that PDW could predict ISR in patients with CAD and diabetes, which is similar to the present study but with different patients and small sample size [25]. Several prediction models have indicated that models combined with angiographic characteristics, like bifurcation lesion or ≥ 2 vessel-coronary diseases, have good predictive values for ISR [36, 45, 46]. The multivessel lesion has been regarded as a high-risk characteristic of cardiovascular disease. The present study showed that a prediction model comprised of lesion vessels was an independent predictor for ISR, which is similar to previous studies [45]. Beyond characteristics of vessel lesion, pre-procedural and intra-procedural operations of PCI may also influence outcomes of ISR, because various stenting strategies may have different extent impairments to vessels. Therefore, access sites of PCI might also affect the outcomes of ISR for it increasing incidences of adverse events of angiography [47].
Study strengths and limitations
Here, the present study revealed that the incidence of ISR was 5.79% in CAD patients with DES implantation in the Xinjiang population, China. A novel prediction model based on platelet parameters, and combined with clinical characteristics and angiographic results was effectively to predict ISR in patients with CAD and DESs implantation. Furthermore, a nomogram was provided to evaluate the risk of ISR, and an overview table was listed with potential treatment strategies for CAD patients in clinical practice. Despite these findings, some limitations in this study can not be neglected. First, the study had a retrospective design. Second, only the angiographic examination was applied, the intravascular imaging detections were not performed, which limited the detection of potential predictors and the identification of ISR. Third, the prediction model included the variable of vessel lesions detected by angiography, this might limit the applied range of the prediction model. Besides, this was a single-center study, lacking an external verification. Although an internal validation was conducted, the generalizability of the prediction model may decline.
Conclusion
In summary, the incidence of ISR is 5.79% in CAD patients with DES implantation in the Xinjiang population, China. The prediction model based on PDW, TC, LDL-C, SBP, and lesion vessels was an effective model to predict ISR, to conduct risk stratification, and prevent ISR in CAD patients with DESs implantation. In further studies, establishing a prediction model combined with more lesion characters detected by intravascular imaging might be much valuable.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ANOVA:
-
One-way analysis of variance
- BMI:
-
Body mass index
- AUC:
-
Area under curve
- DESs:
-
Drug-eluting stents
- HDL:
-
High-density lipoprotein cholesterol
- MPV:
-
Mean platelet volume
- PCI:
-
Percutaneous coronary intervention
- ISR:
-
In-stent restenosis
- LDL-C:
-
Low-density lipoprotein cholesterol
- ROC:
-
Receiver operator characteristic
- PDW:
-
Platelet distribution width
- POD:
-
Probability of disease
- PCT:
-
Plateletcrit
- SBP:
-
Systolic blood pressure
- IVUS:
-
Intravascular ultrasound
- MI:
-
Myocardial infarction
- TC:
-
Total cholesterol
- SD:
-
Standard deviation
- RCA:
-
Right coronary artery
- TG:
-
Triglyceride
- SNK:
-
Student-Newman-Keuls
- MI:
-
Myocardial infarction
- RCA:
-
Right coronary artery
- OCT:
-
optical coherence tomography
References
Lekshmi KM, Che HL, Cho CS, Park IK. Drug- and Gene-eluting Stents for Preventing Coronary Restenosis. Chonnam Med J. 2017;53:14–27. https://doi.org/10.4068/cmj.2017.53.1.14.
Timmis A, Townsend N, Gale CP, Torbica A, Lettino M, Petersen SE, et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur Heart J. 2020:41, 12–85. https://doi.org/10.1093/eurheartj/ehz859.
Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al. 2015 ACC/AHA/SCAI focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol. 2016;67:1235–50. https://doi.org/10.1016/j.jacc.2015.10.005.
Byrne RA, Joner M, Kastrati A. Stent thrombosis and restenosis: what have we learned and where are we going? The Andreas Gruntzig Lecture ESC 2014. Eur Heart J. 2015;36:3320–31. https://doi.org/10.1093/eurheartj/ehv511.
Stefanini GG, Holmes DR Jr. Drug-eluting coronary-artery stents. N Engl J Med. 2013;368:254–65. https://doi.org/10.1056/NEJMra1210816.
Windecker S, Serruys PW, Wandel S, Buszman P, Trznadel S, Linke A, et al. Biolimus-eluting stent with biodegradable polymer versus sirolimus-eluting stent with durable polymer for coronary revascularisation (LEADERS): a randomised non-inferiority trial. Lancet. 2008;372:1163–73. https://doi.org/10.1016/s0140-6736(08)61244-1.
Zhao SG, Xu JJ, Tao ZH, Jin L, Liu Q, Zheng WY, et al. CHA(2)DS(2)-Vasc score and CHA(2)DS(2)-Vasc-HS score are poor predictors of in-stent restenosis among patients with coronary drug-eluting stents. J Int Med Res. 2019;47:2533–44. https://doi.org/10.1177/0300060519841836.
Wang Z, Liu C, Fang H. Blood cell parameters and predicting coronary in-stent restenosis. Angiology. 2019;70(8):711–8. https://doi.org/10.1177/0003319719830495.
Costa MA, Simon DI. Molecular basis of restenosis and drug-eluting stents. Circulation. 2005;111:2257–73. https://doi.org/10.1161/01.cir.0000163587.36485.a7.
Farb A, Sangiorgi G, Carter AJ, Walley VM, Edwards WD, Schwartz RS, et al. Pathology of acute and chronic coronary stenting in humans. Circulation. 1999;99:44–52. https://doi.org/10.1161/01.cir.99.1.44.
Mori H, Lutter C, Yahagi K, Harari E, Kutys R, Fowler DR, et al. Pathology of Chronic Total Occlusion in Bare-Metal Versus Drug-Eluting Stents: Implications for Revascularization. JACC Cardiovasc Interv. 2017;10:367–78. https://doi.org/10.1016/j.jcin.2016.11.005.
Cassese S, Byrne RA, Tada T, Pinieck S, Joner M, Ibrahim T, et al. Incidence and predictors of restenosis after coronary stenting in 10 004 patients with surveillance angiography. Heart. 2014;100:153–9. https://doi.org/10.1136/heartjnl-2013-304933.
Tang L, Cui QW, Liu DP, Fu YY. The number of stents was an independent risk of stent restenosis in patients undergoing percutaneous coronary intervention. Medicine (Baltimore). 2019;98:e18312. https://doi.org/10.1097/md.0000000000018312.
Cheng G, Chang FJ, Wang Y, You PH, Chen HC, Han WQ, et al. Factors Influencing Stent Restenosis After Percutaneous Coronary Intervention in Patients with Coronary Heart Disease: A Clinical Trial Based on 1-Year Follow-Up. Med Sci Monit. 2019;25:240–7. https://doi.org/10.12659/msm.908692.
Wang JL, Qin Z, Wang ZJ, Shi DM, Liu YY, Zhao YX, et al. New predictors of in-stent restenosis in patients with diabetes mellitus undergoing percutaneous coronary intervention with drug-eluting stent. J Geriatr Cardiol. 2018;15:137–45. https://doi.org/10.11909/j.issn.1671-5411.2018.02.011.
Chandrasekar B, Tanguay JF. Platelets and restenosis. J Am Coll Cardiol. 2000;35:555–62. https://doi.org/10.1016/s0735-1097(99)00596-3.
Inoue T, Sohma R, Miyazaki T, Iwasaki Y, Yaguchi I, Morooka S. Comparison of activation process of platelets and neutrophils after coronary stent implantation versus balloon angioplasty for stable angina pectoris. Am J Cardiol. 2000;86:1057–62. https://doi.org/10.1016/s0002-9149(00)01159-0.
Hicks KA, Tcheng JE, Bozkurt B, Chaitman BR, Cutlip DE, Farb A, et al. 2014 ACC/AHA Key Data Elements and Definitions for Cardiovascular Endpoint Events in Clinical Trials: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Cardiovascular Endpoints Data Standards). Circulation. 2015;132:302–61. https://doi.org/10.1161/cir.0000000000000156.
Georgiadou P, Voudris V. Platelet activation and stent thrombosis. Hellenic J Cardiol. 2017;58:49–50. https://doi.org/10.1016/j.hjc.2017.03.013.
Dai Z, Gao J, Li S, Li R, Chen Z, Liang M, et al. Mean Platelet Volume as a Predictor for Restenosis After Carotid Angioplasty and Stenting. Stroke. 2018;49:872–6. https://doi.org/10.1161/strokeaha.117.019748.
Haidegger M, Kneihsl M, Niederkorn K, Deutschmann H, Augustin M, Wünsch G, et al. Mean Platelet Volume Does Not Predict Restenosis After Carotid Artery Stenting in Whites. Stroke. 2020;51:986–9. https://doi.org/10.1161/strokeaha.119.028180.
Coban E, Bostan F, Ozdogan M. The mean platelet volume in subjects with impaired fasting glucose. Platelets. 2006;17(1):67–9. https://doi.org/10.1080/09537100500220729.
Peng W, Shi X, Xu X, Lin Y. Both CYP2C19 and PON1 Q192R Genotypes Influence Platelet Response to Clopidogrel by Thrombelastography in Patients with Acute Coronary Syndrome. Cardiovasc Ther. 2019;2019:3470145. https://doi.org/10.1155/2019/3470145.
Rechcinski T, Jasinska A, Forys J, Krzeminska-Pakula M, Wierzbowska-Drabik K, Plewka M, et al. Prognostic value of platelet indices after acute myocardial infarction treated with primary percutaneous coronary intervention. Cardiol J. 2013;20:491–8. https://doi.org/10.5603/cj.2013.0134.
Hu CP, Du Y, Zhu Y, Shi C, Qin Z, Zhao YX. Platelet Distribution Width on Admission Predicts In-Stent Restenosis in Patients with Coronary Artery Disease and Type 2 Diabetes Mellitus Treated with Percutaneous Coronary Intervention. Chin Med J (Engl). 2018;131:757–63. https://doi.org/10.4103/0366-6999.228247.
Vagdatli E, Gounari E, Lazaridou E, Katsibourlia E, Tsikopoulou F, Labrianou I. Platelet distribution width: a simple, practical and specific marker of activation of coagulation. Hippokratia. 2010;14(1):28–32.
De Luca G, Venegoni L, Iorio S, Secco GG, Cassetti E, Verdoia M, et al. Platelet distribution width and the extent of coronary artery disease: results from a large prospective study. Platelets. 2010;21(7):508–14. https://doi.org/10.3109/09537104.2010.494743.
Bekler A, Ozkan MT, Tenekecioglu E, Gazi E, Yener AU, Temiz A, et al. Increased platelet distribution width is associated with severity of coronary artery disease in patients with acute coronary syndrome. Angiology. 2015;66(7):638–43. https://doi.org/10.1177/0003319714545779.
Liu R, Gao F, Huo J, Yi Q. Study on the relationship between mean platelet volume and platelet distribution width with coronary artery lesion in children with Kawasaki disease. Platelets. 2012;23(1):11–6. https://doi.org/10.3109/09537104.2011.586073.
Akin F, Ayca B, Kose N, Altun I, Avsar M, Celik O, et al. Relation of platelet indices to severity of coronary artery disease in patients undergoing primary percutaneous coronary intervention. Perfusion. 2016;31(3):216–22. https://doi.org/10.1177/0267659115594231.
Bakogiannis C, Sachse M, Stamatelopoulos K, Stellos K. Platelet-derived chemokines in inflammation and atherosclerosis. Cytokine. 2019;122:154157. https://doi.org/10.1016/j.cyto.2017.09.013.
Tanguay JF, Hammoud T, Geoffroy P, Merhi Y. Chronic platelet and neutrophil adhesion: a causal role for neointimal hyperplasia in in-stent restenosis. J Endovasc Ther. 2003;10(5):968–77. https://doi.org/10.1177/152660280301000521.
Ference BA, Ginsberg HN, Graham I, Ray KK, Packard CJ, Bruckert E, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38:2459–72. https://doi.org/10.1093/eurheartj/ehx144.
Lusis AJ. Atherosclerosis. Nature. 2000;407(6801):233–41. https://doi.org/10.1038/35025203.
Wu Y, Fu X. Comprehensive analysis of predictive factors for rapid angiographic stenotic progression and restenosis risk in coronary artery disease patients underwent percutaneous coronary intervention with drug-eluting stents implantation. J Clin Lab Anal. 2019;33:e22666. https://doi.org/10.1002/jcla.22666.
Zhao J, Wang X, Wang H, Zhao Y, Fu X. Occurrence and predictive factors of restenosis in coronary heart disease patients underwent sirolimus-eluting stent implantation. Ir J Med Sci. 2020;189:907–15. https://doi.org/10.1007/s11845-020-02176-9.
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS guidelines for the Management of Dyslipidaemias. Eur Heart J. 2016;37:2999–3058. https://doi.org/10.1093/eurheartj/ehw272.
Peters SA, Singhateh Y, Mackay D, Huxley RR, Woodward M. Total cholesterol as a risk factor for coronary heart disease and stroke in women compared with men: A systematic review and meta-analysis. Atherosclerosis. 2016;248:123–31. https://doi.org/10.1016/j.atherosclerosis.2016.03.016.
Ochijewicz D, Tomaniak M, Koltowski L, Rdzanek A, Pietrasik A, Kochman J. Intravascular imaging of coronary artery disease: recent progress and future directions. J Cardiovasc Med (Hagerstown). 2017;18:733–41. https://doi.org/10.2459/jcm.0000000000000552.
Giacoppo D, Gargiulo G, Aruta P, Capranzano P, Tamburino C, Capodanno D. Treatment strategies for coronary in-stent restenosis: systematic review and hierarchical Bayesian network meta-analysis of 24 randomised trials and 4880 patients. BMJ. 2015;351:h5392. https://doi.org/10.1136/bmj.h5392.
Shlofmitz E, Kuku KO, Waksman R, Garcia-Garcia HM. Intravascular ultrasound-guided drug-eluting stent implantation. Minerva Cardioangiol. 2019;67:306–17. https://doi.org/10.23736/s0026-4725.19.04895-3.
Shlofmitz E, Torguson R, Zhang C, Mintz GS, Dheendsa A, Khalid N, et al. Impact of intravascular ultrasound on Outcomes following PErcutaneous coronary interventioN for In-stent Restenosis (iOPEN-ISR study). Int J Cardiol. 2021. https://doi.org/10.1016/j.ijcard.2021.08.003.
Lee JY, Park DW, Kim YH, Yun SC, Kim WJ, Kang SJ, et al. Incidence, predictors, treatment, and long-term prognosis of patients with restenosis after drug-eluting stent implantation for unprotected left main coronary artery disease. J Am Coll Cardiol. 2011;57:1349–58. https://doi.org/10.1016/j.jacc.2010.10.041.
Gabbasov Z, Kozlov S, Melnikov I, Byazrova S, Saburova O, Prokofieva L, et al. Novel Biomarkers for Coronary Restenosis Occurrence After Drug-Eluting Stent Implantation in Patients With Diabetes Having Stable Coronary Artery Disease. Clin Appl Thromb Hemost. 2018;24:1308–14. https://doi.org/10.1177/1076029618771752.
Sampedro-Gómez J, Dorado-Díaz PI, Vicente-Palacios V, Sánchez-Puente A, Jiménez-Navarro M, San Roman JA, et al. Machine Learning to Predict Stent Restenosis Based on Daily Demographic, Clinical, and Angiographic Characteristics. Can J Cardiol. 2020;36:1624–32. https://doi.org/10.1016/j.cjca.2020.01.027.
Liang H, Cui Y, Bu H, Liu H, Yan P, Cui L, et al. Value of S100A12 in predicting in-stent restenosis in patients with coronary drug-eluting stent implantation. Exp Ther Med. 2020, 20:211–8. https://doi.org/10.3892/etm.2020.8721.
Gragnano F, Branca M, Frigoli E, Leonardi S, Vranckx P, Di Maio D, et al. Access-Site Crossover in Patients With Acute Coronary Syndrome Undergoing Invasive Management. JACC Cardiovasc Interv. 2021;14:361–73. https://doi.org/10.1016/j.jcin.2020.11.042.
Acknowledgements
We thank Shuo Pan and Shutao Zheng given advice on data collection and draft writing for this study.
Funding
This work was supported by the foundation of State Key Laboratory of Pathogenesis, Prevention and Treatment of High Incidence Diseases in Central Asia (Program No. SKL-HIDCA-2020-47), Training Program of National Science Foundation for Distinguished Young Scholar (No. xyd2021J004), National Natural Science Foundation of China (No. 81860072, U1903304), and the third Training Program of Tianshan Talents of Xinjiang Department of Human Resources and Social Security (No.37 [2021]).
Author information
Authors and Affiliations
Contributions
Y.T.M. and B.D.C. designed this study; X.C.C. and B.Z. collected data; Z.Y.F. and X.X. recruited subjects; F.L., X.M., and X.X. conducted statistical analyses; M.T.G., B.Z., and X.M.G contributed to the draft of the manuscript. The authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All the participants have signed informed consents and agreed to publication. The study has been approved by Medical Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (approval number: K202003–23). All procedures were conducted following the Declaration of Helsinki.
Competing interests
None competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gai, MT., Zhu, B., Chen, XC. et al. A prediction model based on platelet parameters, lipid levels, and angiographic characteristics to predict in-stent restenosis in coronary artery disease patients implanted with drug-eluting stents. Lipids Health Dis 20, 118 (2021). https://doi.org/10.1186/s12944-021-01553-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-021-01553-2