
Abstract
Background
Intermittent calorie restriction (ICR) is a novel method of dietary restriction for body weight control with the potential to improve obesity-related cardiometabolic markers, but the impact of this diet on subjects with hypertriglyceridemia (HTG) remains unknown.
Methods
Eighty-eight subjects with overweight or obesity and mild-to-moderate HTG were randomized to the continuous calorie restriction (CCR) group, or ICR group (a very low-calorie diet during 3 days of the week) for 8 weeks (44 patients in each group). Body composition, plasma lipids, glucose, insulin, adiponectin, and liver enzymes were measured at baseline and after 8 weeks. An intention-to-treat analysis was performed.
Results
The body weight decreased in both groups (4.07 ± 1.83 kg in the CCR group and 4.57 ± 2.21 kg in the ICR group) with no significant difference between the groups. There was no significant difference between the two groups in the reduced amount of fat mass, fat-free mass, and waist circumference. Both groups achieved a significant reduction in plasma triglycerides after 8 weeks (by 15.6 and 6.3% in ICR and CCR groups, respectively) with no difference between treatment groups. HOMA-IR improved significantly in ICR compared to the CCR group (P = 0.03). Plasma glucose, insulin, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, liver enzyme, and adiponectin were not different between the two groups.
Conclusions
The results of this short-term study suggest that three-days a week of the ICR is comparable to a CCR diet for the reduction of triglycerides level in patients with HTG and in the short-term it appears to be more effective than continuous dieting in improving insulin resistance. However, longer-term studies are needed to confirm these findings.
Trial registration
Trial registration number: NCT04143971.
Similar content being viewed by others


Background
Obesity is a major concern of global health due to the prevalence of obesity-related disorders, including diabetes and cardiovascular disease [1]. Hypertriglyceridemia (HTG) defined as fasting triglycerides (TGs) ≥150 mg/dL is highly prevalent in the adult population and the prevalence is increasing together with the increasing prevalence of obesity [2, 3]. Mild to moderate HTG is associated with several complications such as cardiovascular disease [3, 4] and pancreatitis [5]. In addition, HTG may play a role in the development of metabolic disturbances of glucose and has been suggested as an independent risk factor for developing impaired fasting glucose or diabetes mellitus [6, 7]. Considering the increased global prevalence of obesity [8], this may indicate a substantial healthcare burden associated with elevated triglycerides (TG) levels [2, 9].
Lifestyle changes including dietary therapy and weight loss could improve HTG [10]. Dietary calorie restriction is a cornerstone of the weight loss program. Continuous calorie restriction (CCR) has been the major form of dietary restriction to reduce weight. However, it may be difficult for some to maintain a constant calorie restriction to achieve weight loss. Intermittent calorie restriction (ICR) is an alternative method of dietary restriction for weight management that involves short periods of severe calorie restriction/fasting interspersed with normal daily caloric intake [11]. The efficacy of ICR for weight reduction is expected since it creates an overall decrease in energy intake.
In HTG, the elevated concentrations of triglyceride levels may lead to peripheral insulin resistance and islet beta-cell dysfunction [12]. Furthermore, obesity is associated with elevated serum free fatty acids which can contribute to insulin resistance in subjects with obesity [13]. The calorie restriction independent of its effect on weight loss could improve insulin sensitivity [14]. Therefore, the calorie restriction method used in the ICR, in which the calorie restriction is more severe on certain days of the week, may have an improved effect on hypertriglyceridemia and insulin resistance.
Previous studies had compared the effects of CCR to ICR on weight loss and cardiometabolic markers in subjects with overweight and obesity [11, 15]. However, currently, there is insufficient data regarding the impact of these diets in subjects with overweight and obesity and mild to moderate HTG. We hypothesized that an ICR diet would result in greater weight loss than a CCR diet in people with overweight and obesity and mild to moderate HTG, and since the calorie restriction in the ICR would be more severe than the CCR diet on some days of the week, the resulting metabolic effects, particularly on plasma TG and insulin concentrations, may also be different.
Methods
Study design and subjects
Subjects were recruited through advertisements placed on and around the Nutrition and Diet Therapy Clinic of Shahid-Beheshti University of Medical Sciences and via advertisements in print and broadcast media. Among individuals who responded to the advertisements, 88 participants were deemed eligible to participate after the body mass index (BMI) and plasma TG assessment. Individuals included were men and women with a BMI > 25 kg/m2, fasting plasma TG was between 150 and 400 mg/dL in a recent blood test (less than a month ago), who had not had a weight loss program in the previous 3 months and were not taking fibrates or omega-3 supplements, had no previous history of gallstones or cardiac arrhythmia. Exclusion criteria were unwillingness to continue participation, any change in medication regimen during follow up, chronic kidney disease stage 4 or 5, patients with diabetes who were taking insulin or taking insulin-stimulating drugs, currently smoking, and pregnancy. The experimental protocol was approved by the National Nutrition and Food Technology Research Institute and all volunteers gave written informed consent to participate in the trial. The protocol conducted in this trial was in compliance with the Helsinki Declaration and the trial has received ethical approval from the National Nutrition and Food Technology Research Institute Ethics Committee, and written informed consent was obtained from all participants. This clinical trial was registered at the clinical trial registration center (NCT04143971).
The study was a randomized, parallel-armed, comparison between CCR and ICR. Participants were stratified based on BMI (two strata: overweight 25.0–29.9 and obese ≥30.0). Subjects from each stratum were then randomly assigned 1:1 to either the CCR group (n = 44) or ICR group (n = 44) by the study dietitian according to the randomization schedule. The participants were randomly assigned to either the CCR group (n = 44) or ICR group (n = 44) following simple randomization procedures using an online-generated random number allocation sequence. The study was not blinded.
Dietary intervention
Subjects participated in the ICR or CCR protocol for 8 weeks. The CCR group was instructed to consume 70% of the estimated total energy expenditure. For this purpose, first weight maintenance calories were estimated by Mifflin St Jeor’s equation [16] multiplied by physical activity level. To estimate physical activity level, first the short form of the International Physical Activity Questionnaires [17] was completed for each participant and then they transformed to physical activity level (PAL) by using metabolic equivalents to PAL table [18]. The sum of activities value (∆ PAL value) was added to the value of 1.1 (thermic effect of food) and the resulting value was considered as the physical activity level of each participant. Then 30% of the estimated weight maintenance calories were subtracted and the remaining calories were distributed as ~ 52% from carbohydrate, ~ 18% from protein, and ~ 30% from fat. Then, the servings of each food group were determined, and by considering the number of each food group, several meal plans were given to subjects.
Participants of the ICR group consumed a diet that met 100% daily total energy expenditure for weight maintenance (estimated using the Mifflin equation multiplied by physical activity level) during the 4 days of the week, and for the other 3 days, they underwent a fast, consuming a very low-calorie diet (30% of daily calories requirement). A fasting day menu consists of 5–7 servings of meat and substitutes, 0–1 serving of whole grains, 0.5 serving of dairy products, 0–1 serving of fruits, and 5–6 servings of vegetables. Unsweetened tea and coffee were allowed (three servings/day). Participants of both groups also received a general multivitamin/mineral tablet three times during the week.
Dietary counseling sessions were held at weeks 0, 1, 4, and 6 of the study. The dietary counseling sessions were conducted individually for each participant by the study dietitian. For this purpose, the first session of dietary counseling of each participant lasted at least 45 min and the next sessions lasted 15 min. In each session, the participant was learned how to develop individualized meal plans by learning the macronutrient content of food groups and portion sizes. All participants received written dietary information including sample menus and portion advice. No food or meal replacements were provided and all foods were self-selected by participants.
The total weekly calorie of both groups had similar dietary calorie restrictions. A 70% energy restriction 3 days per week with 4 days per week eating at the normal calorie level to maintain weight is equal to a 30% daily energy restriction every day of the week.
The 24-h diet recalls were obtained by a dietitian three times at each of the three-time points (before week 0, at week 4, and week 8 of the study). Dietary data were analyzed by the Nutritionist software (version IV, San Bruno, USA). For the CCR group, the average intake of 3 diet recalls was calculated at each time point. For the ICR group, the diet recalls related to weeks 4 and week 8 were weighted as 3/7 fasting intake and 4/7 fed intake. All dietary information from the diet recalls was analyzed by a single trained operator. Participants were asked not to change their habitual physical activity during the study period.
Anthropometric measurements
Weight and height were measured during the screening, baseline, and post-intervention visits. The screening visit measurements confirmed BMI eligibility and were not used in the analysis.
Body weight was in light clothing using a balance beam scale (Seca Deutschland, Hamburg, Germany). Waist circumference was measured midway between the lower costal margin and super iliac crest by a flexible tape. Percentage body fat and fat-free mass were assessed after the weigh-in by using a bioelectrical impedance analyzer (X-contact 356; Jawon Medical Co, Seoul, South Korea).
Biochemical assays
Blood samples were collected into tubes (containing EDTA) after 12 h overnight fasting at the beginning and the end of the study. The platelet-free plasma was separated by centrifugation and stored at − 80 °C for later biochemical analysis. For participants in the ICR group, a final study visit was scheduled to take place the day after the normal-day diet. Plasma glucose, lipids, lipoproteins, and liver enzymes were analyzed with the colorimetry method via auto-analyzer Selectra ProXL (Vital Scientific, Spankeren, The Netherlands), using commercial kits (Pars Azmoon, Karaj, Iran). Commercially available enzyme-linked immunosorbent assay kits were used to measure plasma insulin (Monobind, Inc., Lake Forest, CA, USA) and adiponectin (Biolegend, San Diego, CA, USA) according to manufacturer’s protocol. Insulin resistance was calculated using the homeostasis model assessment of insulin resistance (HOMA-IR) [19].
Statistics
The study sample size was calculated using weight loss as the main outcome variable. By using mean and the standard deviation (SD) of body weight changes from a previous study [20], to detect an effect size of 0.59 with 80% power at the 5% level of significance, in each arm, 44 participants were needed.
All analyses were conducted using intention-to-treat. The baseline carry forward method was used to manage missing data. Data were analyzed using SPSS (version 23.0, SPSS Inc., Chicago, USA). Kolmogorov-Smirnov test was performed to check the normality of data and to permit parametric testing, non-normally distributed data were log-transformed. Differences between groups were assessed using independent t-tests or the χ 2 test. Between-groups differences were assessed with an ANCOVA test with post-treatment values as the dependent variable, and baseline values of each parameter as the covariate. To present more details, absolute change values from baseline were also analyzed with independent t-tests or non-parametric Manne Whitney U-test. However, since ANCOVA has the highest statistical power [21], the basis for significant differences between the two groups was considered based on the results of the analysis of covariance. Differences between baseline and post-intervention in each group were analyzed by the paired t-test. Dietary intake values were assessed with repeated-measures analysis of variance for the two factors with the group as a between-subjects factor. Correlations between changes in outcome variables were explored using Pearson’s or Spearman’s tests. Statistical significance was set at P < 0·05.
(two-tailed).
Results
Baseline characteristics
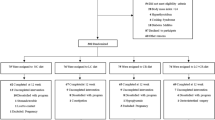
Of the 129 participants screened, 88 adults with HTG were randomly assigned to diet groups and 80 completed the study (Fig. 1). Baseline characteristics of all participants in the CCR and ICR groups are reported in Table 1. There were no differences between groups for age, weight, or medications. Eight participants in the CCR group and 11 in the ICR group were treated with statins. None of the participants were treated with oral estrogen and thiazide drugs before or during the study.

Flowchart of the study
Dietary intake
The dietary intake of participants is shown in Table 2. Participants of both groups ate slightly less than their prescribed goal. There was no between group difference in energy intake. Compared to the CCR group, carbohydrates intakes were significantly lower whereas protein and cholesterol intakes were significantly higher in the ICR group. Data from the dietary recall indicated that participants in the ICR group ate the types and quantities of foods that have been recommended in the fasting days.
Weight loss and body composition
Both groups lost significant weight between baseline and 8-week follow up (Table 3). Body weight decreased by 4.07 ± 1.83 kg in the CCR group and 4.57 ± 2.21 kg in the ICR group. The analysis showed that the mean weight reduction was not significant by treatment. Waist circumference, Fat mass, and fat-free mass decreased significantly within each group, but there were no significant differences between the groups.
Plasma cardiometabolic markers
Plasma lipid concentrations are displayed in Table 4. From baseline to 8-week, the TG level reduced in both groups (by 15.6 and 6.3% in ICR and CCR groups, respectively) with no significant difference between treatment groups. Total cholesterol and HDL-C concentrations decreased in the CCR group only (P < 0.05) but there was no significant difference between the two groups. LDL-C was not affected by either intervention. Non-HDL-C decreased in the CCR group while TG/HDL-C decreased in the ICR group with no difference between treatment groups.
There were also no significant differences in fasting plasma glucose between groups at week 8. In the ICR group, the plasma insulin levels decreased significantly from baseline, but the difference between groups was not statistically significant. Participants in the ICR group showed an improvement in HOMA-IR, and the treatment effects were significantly different from those in the CCR group. In addition, the insulin and HOMA-IR were analyzed by considering the baseline weight as well as baseline values of the variables as confounding factors, and no change was observed in the results (P = 0.07 and P = 0.25 for HOMA-IR and insulin levels, respectively).No changes in the plasma level of adiponectin occurred in either diet group. Plasma aspartate aminotransferase (AST) and alanine aminotransferase (ALT) were not different between groups.
The change values (baseline minus 8-week) of body weight were positively correlated with the corresponding changes in plasma TG (r = 0.35; P = 0.001) but not with insulin levels. The TG changes were correlated with the changes in insulin levels (r = 0.26; P = 0.015).
Discussion
The primary goal of this study was to determine whether subjects with overweight or obesity and mild-to-moderate HTG could benefit from intermittent dieting. The results of this trial demonstrated that three-days a week of the intermittent calorie restriction is comparable to a continuous energy restriction diet for the reduction of plasma TG level and appeared to be more effective than continuous dieting in improving a marker of insulin resistance in this group of participants with HTG.
A slightly greater weight loss was observed in ICR than the CCR diet after 8 weeks of treatment. However, this difference was not significant statistically and it was not also meaningful from the clinical point of view. Consistent with this finding, previous short-term (8–12 weeks) [20, 22, 23] or longer-term [24,25,26] studies that compared weight loss between the two types of daily and intermittent calorie restriction have not observed a statistically significant difference. It seems that the overall reduction in calorie intake appears to play a major role in weight loss and as long as overall energy restriction remains similar, ICR will result in comparable weight loss to CCR [27].
We observed no significant difference in plasma lipids and lipoproteins between the two groups. Consistent with our findings, a meta-analysis comparing ICR with CCR found no significant between-arms difference in blood lipid values [28]. Beneficial modulations in TG were observed by both diets. Reductions in plasma TG by ICR found in our study are consistent with those reported by several other investigators [25, 29, 30] but they differ from other reports of no change [31]. We also show that changes in plasma TG concentrations were correlated to changes in body weight. Therefore, the size of weight loss may have played a major role in the degree to which the plasma TG was altered. Thus, a slightly greater reduction in plasma TG in the ICR group may be related to their greater weight loss. However, the ICR group had lower carbohydrate intake as well and this may also have contributed to a slightly greater reduction in their plasma TG concentrations. Increases in dietary carbohydrates have been associated with an increase in TG concentration, particularly in overweight and obese subjects [32]. Regarding plasma HDL-C concentration, although no significant difference was found between groups at 8 weeks, the concentration decreased in the CCR group whereas it had no changes in the ICR group. However, it is unlikely this decrease is detrimental because no decrease was observed in the TC/HDL-C. TC/HDL-C has been suggested to be a cumulative marker of the metabolic abnormalities in individuals with high TG–low HDL-C levels [33].
Beneficial modulations in insulin and HOMA-IR (an insulin resistance marker) were observed by the ICR diet. Previous studies have reported either improvement [25, 34] in insulin resistance by ICR compared with CCR or no effect [17, 24, 35]. The effectiveness of the ICR diet may vary according to the study population. The result of the study by Gabel et al. demonstrated that in insulin-resistant participants, ICR produced more improvements in insulin resistance compared with CCR [34]. In contrast, Catenacci et al. noticed no difference in insulin sensitivity index after 8 weeks between ICR and CCR in metabolically healthy individuals with obesity [35]. Likewise, Trepanowski et al. reported no significant differences in fasting insulin or insulin resistance between the ICR and CCR in metabolically healthy obese adults [24]. In another study, individuals who participated in an 8-week ICR diet were divided into tertiles base on the on HOMA-IR [27]. They observed that ICR reduced insulin resistance (estimated by HOMA-IR) only in those that were in the highest tertile of HOMA-IR. In our study, changes in plasma TG concentrations were correlated to changes in insulin. HTG is associated with metabolic glucose disorders [6, 7] and the elevated concentrations of TG levels may lead to peripheral insulin resistance [12]. Subjects with overweight or obesity and HTG of the present study may have more insulin resistance than healthy individuals with overweight or obesity.
Despite a change in insulin resistance, plasma adiponectin levels were not different between ICR or CCR diet groups. This is consistent with the result of previous studies that have compared ICR to CCR [17, 36]. Adiponectin changes during calorie-restriction may have little relation to the amount of weight loss [37].
Study strengths and limitations
In the present study, the attrition rate was not high, with a dropout rate of only ∼9%. Furthermore, a well-trained dietitian collected the data through face-to-face interviews. However, the study also has a few limitations. First, the duration of the intervention was short and no maintenance phase was included in the study design. Longer trial durations may likely have more clearly shown differences in plasma TG and insulin between groups. Second, there was no run-in period before treatment and participants took their usual diet up to the start of the study. Third, the sample size was not powered to detect differences in cardiometabolic outcomes. In addition, although not statistically significant, at baseline the ICR group had a 6 kg lower body weight than CCR.
Conclusion
The main finding of our study is that ICR is an effective alternative diet strategy for the reduction of TG level in patients with mild to moderate HTG, and it may be partly superior to CCR for improving insulin resistance in the short-term. There is general agreement that lifestyle therapy, including a weight reduction program, is the cornerstone of treatment for mild-to-moderate HTG [38]. Based on results of the current study, ICR can be recommended for a short term in people with HTG who are reluctant to follow a continuous daily low-calorie diet. However, longer-term studies are needed to confirm these findings before ICR can be recommended more broadly.
Availability of data and materials
All data analyzed during this study are included in this published article.
Abbreviations
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- BMI:
-
Body mass index
- CCR:
-
Continuous calorie restriction
- HDL-C:
-
High-density lipoprotein cholesterol
- HOMA-IR:
-
Homeostasis model assessment of insulin resistance
- HTG:
-
Hypertriglyceridemia
- LDL-C:
-
Low-density lipoprotein cholesterol
- ICR:
-
Intermittent calorie restriction
References
Fava MC, Agius R, Fava S. Obesity and cardio-metabolic health. Br J Hosp Med (Lond). 2019;80:466–71.
Fan W, Philip S, Granowitz C, Toth PP, Wong ND. Prevalence of US Adults with Triglycerides >/= 150 mg/dl: NHANES 2007-2014. Cardiol Ther. 2020;9(1):207–13.
Nordestgaard BG. Triglyceride-rich lipoproteins and atherosclerotic cardiovascular disease: new insights from epidemiology, genetics, and biology. Circ Res. 2016;118:547–63.
Toth PP, Philip S, Hull M, Granowitz C. Elevated triglycerides (>/=150 mg/dL) and high triglycerides (200-499 mg/dL) are significant predictors of new heart failure diagnosis: a real-world analysis of high-risk statin-treated patients. Vasc Health Risk Manag. 2019;15:533–8.
Hansen SEJ, Madsen CM, Varbo A, Nordestgaard BG. Low-grade inflammation in the association between mild-to-moderate hypertriglyceridemia and risk of acute pancreatitis: a study of more than 115000 individuals from the general population. Clin Chem. 2019;65:321–32.
Guerrero-Romero F, Rodriguez-Moran M. Hypertriglyceridemia is associated with development of metabolic glucose disorders, irrespective of glucose and insulin levels: a 15-year follow-up study. Eur J Intern Med. 2014;25:265–9.
Kametani T, Koshida H, Nagaoka T, Miyakoshi H. Hypertriglyceridemia is an independent risk factor for development of impaired fasting glucose and diabetes mellitus: a 9-year longitudinal study in Japanese. Intern Med. 2002;41:516–21.
Jaacks LM, Vandevijvere S, Pan A, McGowan CJ, Wallace C, Imamura F, Mozaffarian D, Swinburn B, Ezzati M. The obesity transition: stages of the global epidemic. Lancet Diabetes Endocrinol. 2019;7:231–40.
Schwartz GG, Abt M, Bao W, DeMicco D, Kallend D, Miller M, Mundl H, Olsson AG. Fasting triglycerides predict recurrent ischemic events in patients with acute coronary syndrome treated with statins. J Am Coll Cardiol. 2015;65:2267–75.
Yamanaka M, Sakuma M, Matsushita A, Tanaka S, Yamamoto Y, Asai T, Arai H. The effects of long-term dietary therapy on patients with hypertriglyceridemia. J Atheroscler Thromb. 2019;26:39–49.
Harris L, Hamilton S, Azevedo LB, Olajide J, De Brun C, Waller G, Whittaker V, Sharp T, Lean M, Hankey C, Ells L. Intermittent fasting interventions for treatment of overweight and obesity in adults: a systematic review and meta-analysis. JBI Database System Rev Implement Rep. 2018;16:507–47.
Ma M, Liu H, Yu J, He S, Li P, Ma C, Zhang H, Xu L, Ping F, Li W, et al. Triglyceride is independently correlated with insulin resistance and islet beta cell function: a study in population with different glucose and lipid metabolism states. Lipids Health Dis. 2020;19:121.
Boden G. Obesity, insulin resistance and free fatty acids. Curr Opin Endocrinol Diabetes Obes. 2011;18:139–43.
Wing RR, Blair EH, Bononi P, Marcus MD, Watanabe R, Bergman RN. Caloric restriction per se is a significant factor in improvements in glycemic control and insulin sensitivity during weight loss in obese NIDDM patients. Diabetes Care. 1994;17:30–6.
Harris L, McGarty A, Hutchison L, Ells L, Hankey C. Short-term intermittent energy restriction interventions for weight management: a systematic review and meta-analysis. Obes Rev. 2018;19:1–13.
Mifflin MD, St Jeor ST, Hill LA, Scott BJ, Daugherty SA, Koh YO. A new predictive equation for resting energy expenditure in healthy individuals. Am J Clin Nutr. 1990;51:241–7.
Craig CL, Marshall AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF, Oja P. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–95.
Food and Nutrition Board IoMotNAo, Sciences. Dietary Reference Intake for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Washington, DC: National Academies Press; 2002.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28:412–9.
Keogh JB, Pedersen E, Petersen KS, Clifton PM. Effects of intermittent compared to continuous energy restriction on short-term weight loss and long-term weight loss maintenance. Clin Obes. 2014;4:150–6.
Vickers AJ. The use of percentage change from baseline as an outcome in a controlled trial is statistically inefficient: a simulation study. BMC Med Res Methodol. 2001;1:6.
Varady KA, Bhutani S, Klempel MC, Kroeger CM. Comparison of effects of diet versus exercise weight loss regimens on LDL and HDL particle size in obese adults. Lipids Health Dis. 2011;10:119.
Carter S, Clifton PM, Keogh JB. Effect of intermittent compared with continuous energy restricted diet on glycemic control in patients with type 2 diabetes: a randomized noninferiority trial. JAMA Netw Open. 2018;1:e180756.
Trepanowski JF, Kroeger CM, Barnosky A, Klempel MC, Bhutani S, Hoddy KK, Gabel K, Freels S, Rigdon J, Rood J, et al. Effect of alternate-day fasting on weight loss, weight maintenance, and Cardioprotection among metabolically healthy obese adults: a randomized clinical trial. JAMA Intern Med. 2017;177:930–8.
Harvie MN, Pegington M, Mattson MP, Frystyk J, Dillon B, Evans G, Cuzick J, Jebb SA, Martin B, Cutler RG, et al. The effects of intermittent or continuous energy restriction on weight loss and metabolic disease risk markers: a randomized trial in young overweight women. Int J Obes. 2011;35:714–27.
Headland ML, Clifton PM, Keogh JB. Effect of intermittent compared to continuous energy restriction on weight loss and weight maintenance after 12 months in healthy overweight or obese adults. Int J Obes. 2019;43:2028–36.
Davis CS, Clarke RE, Coulter SN, Rounsefell KN, Walker RE, Rauch CE, Huggins CE, Ryan L. Intermittent energy restriction and weight loss: a systematic review. Eur J Clin Nutr. 2016;70:292–9.
Cioffi I, Evangelista A, Ponzo V, Ciccone G, Soldati L, Santarpia L, Contaldo F, Pasanisi F, Ghigo E, Bo S. Intermittent versus continuous energy restriction on weight loss and cardiometabolic outcomes: a systematic review and meta-analysis of randomized controlled trials. J Transl Med. 2018;16:371.
Varady KA, Bhutani S, Klempel MC, Kroeger CM, Trepanowski JF, Haus JM, Hoddy KK, Calvo Y. Alternate day fasting for weight loss in normal weight and overweight subjects: a randomized controlled trial. Nutr J. 2013;12:146.
Cai H, Qin YL, Shi ZY, Chen JH, Zeng MJ, Zhou W, Chen RQ, Chen ZY. Effects of alternate-day fasting on body weight and dyslipidaemia in patients with non-alcoholic fatty liver disease: a randomised controlled trial. BMC Gastroenterol. 2019;19:219.
Bhutani S, Klempel MC, Kroeger CM, Trepanowski JF, Varady KA. Alternate day fasting and endurance exercise combine to reduce body weight and favorably alter plasma lipids in obese humans. Obesity (Silver Spring). 2013;21:1370–9.
Parks EJ. Effect of dietary carbohydrate on triglyceride metabolism in humans. J Nutr. 2001;131:2772S–4S.
Lemieux I, Lamarche B, Couillard C, Pascot A, Cantin B, Bergeron J, Dagenais GR, Despres JP. Total cholesterol/HDL cholesterol ratio vs LDL cholesterol/HDL cholesterol ratio as indices of ischemic heart disease risk in men: the Quebec cardiovascular study. Arch Intern Med. 2001;161:2685–92.
Gabel K, Kroeger CM, Trepanowski JF, Hoddy KK, Cienfuegos S, Kalam F, Varady KA. Differential effects of alternate-day fasting versus daily calorie restriction on insulin resistance. Obesity (Silver Spring). 2019;27:1443–50.
Catenacci VA, Pan Z, Ostendorf D, Brannon S, Gozansky WS, Mattson MP, Martin B, MacLean PS, Melanson EL, Troy Donahoo W. A randomized pilot study comparing zero-calorie alternate-day fasting to daily caloric restriction in adults with obesity. Obesity (Silver Spring). 2016;24:1874–83.
Trepanowski JF, Kroeger CM, Barnosky A, Klempel M, Bhutani S, Hoddy KK, Rood J, Ravussin E, Varady KA. Effects of alternate-day fasting or daily calorie restriction on body composition, fat distribution, and circulating adipokines: secondary analysis of a randomized controlled trial. Clin Nutr. 2018;37:1871–8.
Klempel MC, Varady KA. Reliability of leptin, but not adiponectin, as a biomarker for diet-induced weight loss in humans. Nutr Rev. 2011;69:145–54.
Berglund L, Brunzell JD, Goldberg AC, Goldberg IJ, Stalenhoef A. Treatment options for hypertriglyceridemia: from risk reduction to pancreatitis. Best Pract Res Clin Endocrinol Metab. 2014;28:423–37.
Acknowledgments
The authors would like to thank Elaheh Tajeddin for her assistance in laboratory measurements, and the participants who completed the trial.
Funding
This research is funded by a project grant supporting by the National Nutrition and Food Technology Research Institute, Shahid Beheshti University of Medical Science, Tehran, Iran.
Author information
Authors and Affiliations
Contributions
The research was designed by M.M. and J.N.; conducted by M.M.; data were analyzed by J.N; paper was written by J.N. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The procedures followed in this study were in accordance with the 1964 Helsinki Declaration and the study protocol was approved by the Ethical Committee of National Nutrition & Food Technology Research Institute, Tehran, Iran, and written informed consent were obtained from all patients.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Maroofi, M., Nasrollahzadeh, J. Effect of intermittent versus continuous calorie restriction on body weight and cardiometabolic risk markers in subjects with overweight or obesity and mild-to-moderate hypertriglyceridemia: a randomized trial. Lipids Health Dis 19, 216 (2020). https://doi.org/10.1186/s12944-020-01399-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-020-01399-0