
Abstract
The clinical responses observed following treatment with immune checkpoint inhibitors (ICIs) support immunotherapy as a potential anticancer treatment. However, a large proportion of patients cannot benefit from it due to resistance or relapse, which is most likely attributable to the multiple immunosuppressive cells in the tumor microenvironment (TME). Myeloid-derived suppressor cells (MDSCs), a heterogeneous array of pathologically activated immature cells, are a chief component of immunosuppressive networks. These cells potently suppress T-cell activity and thus contribute to the immune escape of malignant tumors. New findings indicate that targeting MDSCs might be an alternative and promising target for immunotherapy, reshaping the immunosuppressive microenvironment and enhancing the efficacy of cancer immunotherapy. In this review, we focus primarily on the classification and inhibitory function of MDSCs and the crosstalk between MDSCs and other myeloid cells. We also briefly summarize the latest approaches to therapies targeting MDSCs.
Similar content being viewed by others


Background
The tumor microenvironment (TME) releases multiple soluble factors that mediate normal myeloid differentiation and convert myeloid cells into immunosuppressive cells. This creates a tumor-promoting ‘macroenvironment’, which substantially limits the efficacy of cancer immunotherapy [1]. MDSCs are a cluster of cells with potent immunosuppressive effects widely distributed in the spleen and tumor tissues of tumor-bearing mice or the peripheral blood and tumor sites of cancer patients [2]. Under normal physiology, bone marrow cells differentiate from multipotent hematopoietic stem cells (HSCs) into diverse mature subsets, and macrophages, dendritic cells (DCs), and granulocytes are the terminally differentiated cells [3]. In contrast, in cancer conditions, the tumor microenvironment renders MDSCs incapable of differentiation, resulting in a population of immature heterogeneous cells [4]. Recent studies have increasingly emphasized that high concentrations of MDSCs are dramatically related to poor prognosis, cancer development and responses to immunotherapies in patients with breast, colorectal, and lung cancers and hematologic malignancies [5,6,7,8]. In the next section, we specifically discuss the classification and suppressive mechanisms of MDSCs. In addition, we emphasize the sophisticated crosstalk of MDSCs with bone marrow-derived cells and present clinically promising therapies targeting MDSCs.
Phenotypes and classifications of MDSCs
As early as 1978, it was found in tumor-bearing mice that coculture of activated T cells with bone marrow cells suppressed T cells [9]. Later, this group of cells with immunosuppressive function, which accumulated significantly in the peripheral blood of cancer patients, was renamed immature myeloid cells (IMCs) and myeloid suppressor cells (MSCs ) [10, 11]. To avoid confusion, Gabrilovich et al. proposed the term MDSCs, which more precisely reflects the origin and function of these cells [12]. First, they were characterized in mice by the coexpression of CD11b and Gr 1 [13]. Then, based on the different expression levels of Ly6G and Ly6C, two different epitopes binding to Gr1, MDSCs were identified as two distinguished subsets: polymorphonuclear- (PMN-) and monocytic- (M-) MDSCs [14].
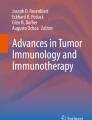
In mice, PMN-MDSCs are defined as CD11b+Ly6G+Ly6Clo, and M-MDSCs are defined as CD11b+Ly6G−Ly6Chi. Intriguingly, a recent study identified a new group of monocyte lineage precursors that differentiated into a substantial subset of PMN-MDSCs, and they were designated as monocyte-like precursors of granulocytes (MLPGs) [15]. In addition, several other markers have been associated with the MDSCs phenotype (Fig. 1). CD49d, a member of the integrin protein family, is only detected on M-MDSCs, not PMN-MDSCs. Haile et al. proposed that CD49d could substitute for Gr1 and, together with CD11b, better classify MDSCs [16].

The phenotypes of PMN-MDSCs and M-MDSCs. In mice, PMN-MDSCs are defined as CD11b+Ly6G+Ly6Clo, and M-MDSCs are defined as CD11b+Ly6G−Ly6Chi. Human PMN-MDSCs are defined as CD11b + CD14− CD15+ or CD11b+ CD14 - CD66b+, and human M-MDSCs are defined as CD11b+ CD14+ HLA-DR−/low CD15−. In addition, several other markers have been associated with the MDSCs phenotype, such as CD49d, LOX1 and IL-4Rα
MDSCs then received increasing attention in clinical practice. A number of studies have demonstrated that increased levels of MDSCs positively correlated with poor prognosis and clinical stage in patients with breast cancer, hepatocellular carcinoma, thyroid carcinoma, and non-small cell lung carcinoma (NSCLC ) [17,18,19,20]. MDSCs are of great value in predicting therapeutic effects in multiple solid tumors [21,22,23]. Human MDSCs lack typical markers of mature immune cells (Lin−, HLA-DR−) but express CD33, CD34, CD11b and IL-4Rα (CD124) [24, 25]. However, because human cells do not express Gr1, the phenotypes of human MDSCs remain controversial. Currently, human PMN-MDSCs are defined as CD11b + CD14− CD15+ CD66b+ and human M-MDSCs as CD11b+ CD14+ HLA-DR−/low CD15 − [14].
The majority of MDSCs are PMN-MDSCs, accounting for more than 75%, with M-MDSCs accounting for only 10–20 % [26]. Youn et al. examined the shared mechanism of MDSCs amplification in 10 diverse tumor models. Preferential expansion of PMN-MDSCs was shown in almost all tumor models, though the extent of amplification differed [27]. It is worth noting that M-MDSCs have a greater capacity for immunosuppression than PMN-MDSCs [27,28,29]. PMN-MDSCs preferentially use reactive oxygen species (ROS) and arginase I (ARG1) to mediate immunosuppression and are independent of inducible nitric oxide synthase (iNOS) [30], while M-MDSC-mediated inhibition mostly relies on nitric oxide (NO) and the suppressive cytokines IL-10 and TGF-β [4, 26] (Fig. 1). Importantly, MDSCs differentially drive immune suppression in a sex-specific manner. Male mice possessed elevated M-MDSCs in the tumor tissues, while females exhibited enhanced PMN-MDSCs in the peripheral circulation [31].
MDSCs phenotypes are similar to those of neutrophils and monocytes, making it a priority to identify MDSCs from other myeloid cells in peripheral blood (Table 1). PMN-MDSCs and neutrophils share mostly identical morphology and phenotype. However, PMN-MDSCs express M-CSFR and a CD244 molecule with higher ARG1 activity and lower phagocytic activity than neutrophils [32]. They can be separated by density gradients, with PMN-MDSCs in the low-density Ficoll gradient fraction of peripheral blood mononuclear cells (PBMCs) and neutrophils in the high-density fraction [33]. Additionally, one study indicated that LOX-1 could distinguish the population of human PMN-MDSCs from granulocytes, which is thought to be a marker of human PMN-MDSCs [34]. Since monocytes are CD14+CD15− HLA-DR+ and M-MDSCs are CD14+ HLA-DR−, human M-MDSCs can be isolated based on the presence of MHC class II molecules [33]. Table 2.
Although research on MDSCs has spanned for decades, key questions remain as to whether these cells are the precursors of well-established normal myeloid cells and whether there are other unidentified myeloid subpopulations of these cells [35].
Expansion and activation of MDSCs
The conflicting results described above have been reported in a few other studies. The amplification process of MDSCs is complex, and the exact process of how MDSCs are generated from bone marrow and eventually become a population of cells with immunosuppressive function has become a highlight of this field.
MDSCs are derived from HSCs, common myeloid progenitors (CMPs) and granulocyte-macrophage progenitors (GMPs ) [36]. GMPs then differentiate into granulocyte progenitors (GPs) and monocytic progenitors (MPs) in response to multiple tumor-induced growth factors, cytokines and other factors [37] (Fig. 2). Although the molecular mechanisms of MDSCs expansion have been intensively studied over the years, the exact details remain unclear. An increasingly large number of scholars favor the two-signal model, which suggests that the generation of MDSCs is a sequential but overlapping process induced by two different signal transduction pathways [38]. One pathway dominates the proliferation of MDSCs, whereas the second pathway contributes to MDSCs activation.

The origin of MDSCs. MDSCs are derived from HSCs, common myeloid progenitors (CMPs) and granulocyte–macrophage progenitors (GMPs). GMPs then differentiate into granulocyte progenitors (GPs) and monocytic progenitors (MPs). In response to multiple tumor-induced cytokines, MDSCs were developed through signaling pathways such as STAT3, IRF8 and C/EBPβ
MDSCs expansion
Previous studies have shown that the proliferation of MDSCs is mostly driven by tumor-derived growth factors, which include GM-CSF, G-CSF, M-CSF, VEGF and IL-6 [39] (Fig. 3). Under physiological conditions, GM-CSF promotes myelopoiesis, and G-CSF and M-CSF are both in charge of differentiation [40]. While it was known as early as 1999 that GM-CSF alone is capable of eliciting these inhibitory cells [41], the details of how GM-CSF triggers an increase in MDSCs remained poorly understood until a preclinical experiment indicated that GM-CSF amplified GMP and was the main factor promoting the CD11b+MDSCs immunosuppressive pathway [42]. Further studies revealed that GM-CSF predominantly invoked Gr-1 int/low MDSCs, while G-CSF drove the proliferation of Gr-1high MDSCs [42]. Another study demonstrated that G-CSF favored the production of MDSCs and whole-body amplification in a mouse breast cancer model [36]. VEGF severely impairs DC maturation and is responsible for the amplification of MDSCs [43]. IL-6 has been found to be positively correlated with peripheral blood MDSCs levels. Notably, all these experiments were conducted in vitro. Almand et al. measured the plasma concentrations of six cytokines, M-CSF, GM-CSF, IL-6, IL-10, TGF-β, and VEGF, in patients with head and neck squamous cell carcinoma (HNSCC), NSCLC, and breast cancer. They discovered that only elevated VEGF levels were statistically correlated with the expansion of MDSCs [44].

The mechanism of MDSCs expansion. The proliferation of MDSCs is mostly driven by GM-CSF, G-CSF, M-CSF, VEGF and IL-6. Additionally, several downstream factors are involved in regulating MDSCs expansion. Of particular interest is S100A9, STAT3, C/EBPβ and IRF8
The cytokines discussed above then trigger several transcription factors, mainly signal transducer and activator of transcription 3 (STAT3), C/EBPβ and IRF8 [26, 38].
STAT3
STAT3 was the first transcription factor found to be associated with MDSCs amplification in tumors. STAT3 upregulates the expression of the antiapoptotic genes Bcl-xL, c-myc and cyclin D to disrupt the normal differentiation of myeloid cells, thus augmenting the population of MDSCs [45, 46]. Additionally, STAT3 can directly bind to the ARG1 promoter to increase ARG1 expression and ROS production [47]. Previous studies have confirmed that the hyperactivation of the JAK–STAT3 pathway mediated the abnormal differentiation of DCs and thus increased the accumulation of MDSCs [48, 49]. In addition to upregulation, STAT3 downregulation caused by activated CD45 phosphatase was found in M-MDSCs, leading to a unique result of differentiation into TAMs [50]. In an inducible STAT3 knockout mouse model, multiple immune cell lineages showed enhanced antitumor activity when tested individually [51]. JSI-124, a selective JAK/STAT3 inhibitor, significantly reduced the presence of MDSCs and promoted their differentiation, suggesting that the inhibition of JAK/STAT3 signaling overcame the differentiation block [52]. However, the studies mentioned above utilized MDSCs in vitro or from cells isolated from lymphoid organs. Kumar et al. found that STAT3 activity of MDSCs is relatively lower in tumor sites than in the spleen and blood of patients [50]. Moreover, inhibition of STAT3 decreased splenic MDSCs, but no significant change in MDSCs was found in the tumor site [53]. Using a spontaneous medulloblastoma transgenic murine model, the prevalence of PMN-MDSCs was reduced after STAT3 disruption, but the number of M-MDSCs increased instead of decreased [54]. Therefore, the mechanistic details of how STAT3 impacts MDSCs in the TME require more intensive investigation.
In addition, several factors downstream of STAT3 may be engaged in regulating MDSCs expansion. Of particular interest is the proinflammatory protein S100A9 together with its dimerization partner S100A8, which is strongly upregulated in multiple tumors, including colon, breast, and prostate cancers [55]. S100A8/A9 directly binds to p47phox and p67phox, enhancing the activation of NOX2 and thus leading to increased ROS production to increase inhibitory functions [29]. S100A8/A9 was also shown to bind to a receptor located on the MDSCs membrane to promote MDSCs migration. After blocking the conjugation of S100A8/A9 to its receptor, the number of MDSCs in peripheral blood was found to be decreased [56]. Another experiment found no amplification of MDSCs in the peripheral blood or spleen of S100A9-deficient tumor-bearing mice, confirming previous findings [57]. In contrast, overexpression of S100A9 in mice resulted in the accumulation of MDSCs, and increased secretion of IL-10 and TGF-β [58]. Taken together, these experiments illustrate the vital role of S100A8/A9 in MDSCs amplification. However, the specific details remain to be explored more deeply.
C/EBPβ
CCAAT/enhancer-binding protein (C/EBP) β, a member of the C/EBP transcription factor family, is implicated in cell proliferation, differentiation and apoptosis [59, 60]. C/EBPβ has fundamental roles in myelopoiesis and emergency granulopoiesis, the level of which increases excessively at later stages of myeloid differentiation [61, 62]. IL-6-mediated C/EBPβ downregulates the expression of immunosuppressive genes such as ARG1, iNOS and NOX2, thus regulating MDSCs differentiation and function [63]. C/EBPβ has been reported to contribute to the generation of MDSCs in the bone marrow and spleen by activating microRNA-21 and microRNA-181b expression [64]. C/EBPβ is also closely associated with GM-CSF and G-CSF expression in myeloid cells and regulates the immunoregulatory activity of MDSCs [65, 66]. Moreover, Strauss et al. found that retinoic acid-related orphan receptor 1 (RORC1) orchestrated myelopoiesis by promoting C/EBPβ and PMN-MDSCs accumulation [67]. In contrast, C/EBPβ-deficient mice have decreased splenic CD11bhiMDSCs. Surprisingly, M-MDSCs were the most reduced population, indicating that the main vital impact of C/EBPβ is on the differentiation of M-MDSCs [68]. There is a consensus that C/EBPβ is indispensable for MDSCs proliferation. However, the exact stage at which C/EBPβ particularly affects MDSCs still needs to be addressed.
IRF8
Interferon regulatory factor-8 (IRF-8), also called interferon consensus sequence binding protein (ICSBP), is crucial for normal myelopoiesis. Mice with a null mutation of IRF-8 exhibit deregulated hematopoiesis, ultimately leading to chronic myelogenous leukemia [69]. Unexpectedly, a previous experiment demonstrated that IRF-8-deficient mice exhibited remarkable accumulation of MDSCs. In another study using both implantable and transgenic mouse models, IRF-8 was observed to play an integral role in the tumor-induced expansion of MDSCs [70]. In addition, IRF8 also functions as a negative regulator in human MDSCs of breast cancer patients. Downregulation of IRF-8 was demonstrated to induce PMN-MDSCs production. In vivo IRF-8 overexpression specifically attenuated MDSCs expansion and enhanced antitumor efficacy via the STAT3 and STAT5 signaling pathways [71, 72]. Notably, IRF-8 promotes monocyte and dendritic cell differentiation but limits granulocyte development [73]. A recent study demonstrated that IRF8 overexpression in vivo selectively led to GPs proliferation and PMN-MDSCs expansion without appreciable expansion of MPs and M-MDSCs [71].
MDSCs activation
Notably, MDSCs acquire immunosuppressive activity only after activation. The second signal governing MDSCs activation is primarily proinflammatory cytokines produced by the tumor stroma or activated T cells, including IFN-γ, IL-1β, IL-4, IL-13, and PGE2. The signaling pathways involved in MDSCs activation include STAT6, nuclear factor-κB (NF-κB) and STAT1 [29] (Fig. 4).

The mechanism of MDSCs activation. Notably, only after activation can MDSCs acquire immunosuppressive activity. MDSCs activation is primarily associated with IFN-γ, IL-1β, IL-4, IL-13, PGE2 and ER stress sensors. The signaling pathways involved in MDSCs activation include STAT6, nuclear factor-κB (NF-κB) and STAT1
IFN-γ is released by CD3/28-triggered activation of T cells, and due to the presence of IFN-γ, MDSCs become immune dysfunctional [74]. STAT1 is the most crucial downstream transcription factor of IFN-γ. Indeed, IFN-γ is strictly required for the activation and function of PMN-MDSCs, and is dependent on the STAT1 pathway or NO production. However, blocking IFN-γ only partially antagonizes the immune dysfunction of M-MDSCs [30]. IFN-γ and IL-13 were found to synergistically initiate immunosuppressive pathways of MDSCs. IFN-γ preferentially promotes iNOS expression, while IL-13 has a greater tendency to upregulate ARG1 [25]. Importantly, both enzymes are upregulated when IL-13 and IFN-γ are simultaneously or sequentially added. The inflammatory mediator IL-1β was shown to be a cytokine that induced the recruitment of MDSCs and, in particular, promoted the activation of MDSCs. Another study demonstrated that the PGE2 receptor expressed in MDSCs induced ARG1 expression, and using a COX2 inhibitor decreased the level of ARG1 in vitro and in vivo [75]. PGE2 is indispensable for the functionality of MDSCs. Indeed, blocking COX-2, an enzyme that catalytically synthesizes PGE2, potently revived the ability to suppress T-cell function mediated by MDSCs [76, 77]. Tumor-derived PGE2 has been shown to drive the suppressive phenotype of M-MDSCs through upregulation of NF-κB [78]. Moreover, PGE2 activated the Ras/Erk pathway and increased the level of TGF-β to activate the suppressive functions of MDSCs on NK cells [79].
Upregulation of genes associated with the ER stress response is a prominent feature of MDSCs. The ER stress response is highly conserved and serves to defend cells from a variety of emergency damages, such as hypoxia and infection [80]. MDSCs isolated from tumor-bearing mice and cancer patients were identified to upregulate downstream effectors of the ER stress response, especially C/EBP-homologous protein (CHOP ) [81]. Another study showed that CHOP deficiency impaired inhibitory activity in MDSCs and decreased the expression of IL-6, C/EBPβ, and pSTAT3. Additionally, exogenous IL-6 rescued MDSCs activity in Chop-deficient mice [82]. Consistent with these observations, the administration of ER stress inducers increased the expansion of MDSCs and their inhibitory function.
Recently, HMGB1 and PPARγ were found to exert an important role in the function of MDSCs [39]. HMGB1 released by MDSCs was reported to, by activating NF-κB, promote the differentiation of MDSCs, increase secretion of IL-10, and decrease the expression of L-selectin on circulating T cells, exerting immunosuppressive effects [83]. Overexpression of PPARγ led to the expansion of PMN-MDSCs with immunosuppressive activity, which was also associated with the NF-κB pathway [84].
Immunosuppressive mechanism of MDSCs
Previous studies have demonstrated that MDSCs specifically and effectively inhibit antigen-specific CD8+ T-cell function with decreased IFN-γ production, and this effect is dependent on the interaction between MDSCs and the T cells [85, 86]. Using immortalized murine CD11b + /Gr1 + cells, Bronte et al. found that MDSCs reduce the generation of T cells and suppress tumor immunity by triggering the apoptotic cascade of T cells [87]. They followed up their study by demonstrating that MDSCs halted the cell cycle of T cells, leading to apoptosis through proliferation blockade, rather than directly killing the cells [88]. Summarizing experimental murine models and clinical findings to date, MDSCs exert their T-cell suppression mainly through the high expression of ARG1, iNOS and ROS [89,90,91,92,93,94] (Fig. 5).

The mechanisms by which MDSCs inhibit T-cell antitumor immunity. MDSCs exert their T-cell suppression mainly via the high expression of ARG1 and iNOS and the production of ROS. In addition to biochemical metabolism, MDSCs also induce immunosuppression by upregulating PD-L1 expression and secretion of TGF-β
ARG1
Two arginine isozymes exist in mammals. ARG1, abundantly observed in the cytoplasm of hepatocytes, is an important element in the urea cycle. In comparison, ARG2 exists in mitochondria and is barely expressed in the liver [95]. MDSCs express high levels of ARG1, rather than ARG2, which is induced by Th2-type cytokines such as IL-4 and IL-13 [96]. ARG1 catalyzes the synthesis of urea and L-ornithine from L-arginine, the latter being an essential substrate for cell cycle processes. Therefore, extracellular L-arginine, an essential amino acid for T-cell activation, is substantially diminished [97]. Except in the case of T-cell anergy, L-arginine depletion decreases the expression of the CD3-associated ζ chain, suppressing T-cell proliferation [98,99,100]. Interestingly, one study demonstrated that MDSCs in the spleen downregulated the CD3-associated ζ chain of CD4+ T cells but not CD8+ T cells [101]. To investigate the mechanisms by which L-arginine deletion induces the inability of T cells to proliferate,Rodriguez et al. found that L-arginine starvation arrested the cell cycle from G1 to S phase by impairing the expression of cyclin D [102]. These data are consistent with the observation that MDSCs producing high ARG1 exist in patients with renal cell carcinoma and express lower levels of T-cell receptor (TCR) and CD3-associated ζ chain [103], indicating that ARG1 plays a critical role in immunosuppression of MDSCs both in mice and in patients. In addition, depletion of cystine and cysteine is also involved in the immunosuppressive effect of MDSCs. MDSCs importing cystine but not releasing cysteine restrict the levels of cysteine in the TME, thus limiting T-cell activation [104].
iNOS
There are three isoforms of nitric oxide synthase (NOS), neuronal NOS (nNOS), endothelial NOS (eNOS), and iNOS [105]. The first two isoforms are constitutively expressed. In contrast, iNOS is only expressed when stimulated and is highly associated with poor prognosis in malignant cancers [106]. iNOS competes for the same substrate as ARG1 and metabolizes L-arginine to citrulline and NO, which is a key messenger in tumor progression and T-cell activation [107, 108]. NO generated by MDSCs was found to abolish the IL-2 receptor signaling pathway and nitrate the TCR, resulting in immunosuppressive activity [109]. However, unlike ARG1 induced by Th2 cytokines, iNOS is induced by Th1 cytokines such as IFN-γ, TNF-α and IL-1 β [110]. This confirms the previous finding that blockade of IFN-γ eliminates the complete suppression of PMN-MDSCs and partial effect of M-MDSCs [30]. The intracellular signal transduction pathways involved are the NF-κB and JAK-STAT pathways [111]. Moreover, a new possible mechanism was proposed in which iNOS critically downregulated vascular E-selectin, impairing T-cell recruitment to tumors and antitumor immunity [112]. Similarly, the chemokine receptor CCR2 expressed by MDSCs and CCL2 produced by tumor cells have been implicated in a vital role in the recruitment of MDSCs into tumors [113]. iNOS+ MDSCs cause CCL2 nitration and inhibit T-cell migration.
Recent studies have revealed that the network of the two enzymes, ARG1 and iNOS, working together may be unique to MDSCs [114]. ARG1 overexpression led to a translational arrest of the mRNA for iNOS and reduced iNOS activity; while iNOS is overexpressed, ARG1 was in turn inhibited, and NO was further released in adjacent cells [114].
Reactive oxygen species (ROS)
Previous studies have provided multiple lines of evidence supporting the critical role of ROS in MDSCs immunosuppression [115, 116]. The ROS levels of MDSCs isolated from tumor-bearing mice were found to be significantly higher than those isolated from healthy mice. The main producer of increased ROS is NADPH oxidase (NOX2), which is composed of two membrane proteins and at least four cytosolic proteins, including p47phox and p67phox [117]. Several dramatically increased NOX2 subunits, directly regulated by STAT3, were found to result in ROS production [118]. The biochemical metabolisms of MDSCs produce ROS, including superoxide (O2−), hydrogen peroxide (H2O2), and peroxynitrite (ONOO−) [6]. H2O2 is a major contributor to this increased pool of ROS. Indeed, inhibiting ROS in MDSCs completely reversed MDSCs immunosuppression, suggesting that MDSCs suppress the CD8+ T-cell response via the production of ROS [119]. Moreover, H2O2 produced by MDSCs also had an impact on CD3-associated ζ chain expression and function [120]. ONOO− also causes DNA damage as well as nitration of various proteins, such as TCR, CD3 and CD8 [117].
In addition to the biochemical metabolisms discussed above, MDSCs also induce immunosuppression by upregulating PD-L1 expression and secretion of TGF-β. The percentage of PD-L1 expression is noticeably higher on tumor-infiltrating MDSCs than splenic MDSCs [121]. Another study demonstrated that tumor-derived PD-L1 expression was limited to M-MDSCs and that these cells directly eliminated CD8+ T cells in vitro [122]. Moreover, in the presence of MDSCs, the surface molecules of B cells are remodeled, with prominently increased PD-L1 expression, subsequently inducing T-cell dysfunction [123]. MDSCs were found to potently inhibit NK-cell cytotoxicity, which requires direct intercellular contact to suppress perforin production rather than granzyme B [124]. In orthotopic live tumor models, hepatic NK-cell cytotoxicity and secreted IFN-γ were remarkedly damaged. Furthermore, MDSCs induce NK-cell anergy via membrane-bound TGF-β [125]. However, Nausch et al. unexpectedly found that F4/80+MDSCs in mice could instead initiate NK cells and augment IFN-γ secretion [126].
The plasticity of MDSCs
Plasticity is a distinct characteristic of MDSCs (Fig. 6). In the last few years, three major cell populations have gained attention as major negative regulators of the immune response: tumor-associated macrophages (TAMs), MDSCs, and CD4+ regulatory T cells (Tregs) with the same immunoinhibitory functions that limit the effectiveness of ICI therapy [127,128,129,130,131,132]. MDSCs can influence the proliferation of Tregs, inhibiting T-cell activation. Tregs represent a group of special T cells that are divided into two main groups: natural Tregs and adapted Tregs. The former is produced in the thymus and is developmentally dependent on the expression of the forkhead box transcription factor (FOXP3). CD115+ F4/80+ MDSCs, cocultured with IFN-γ and IL-10, were shown to induce FOXP3+ Tregs in vivo [11].

The plasticity of MDSCs. MDSCs can induce Tregs and differentiate into TAMs, as well as mature DCs and M2 macrophages. Moreover, MDSCs were found to be derived from CAFs under the influence of IL-6 and turned into fibrocytes in the lung. MDSCs can also differentiate into osteoclasts and have a complex crosstalk with Th17 cells
TAMs are the second most well-described myeloid cell population negatively affecting immunotherapy. The relationship between TAMs and MDSCs has not been fully established, but TAMs may be partially derived from MDSCs [110]. Compared to TAMs, MDSCs exhibit high Gr1 expression and low F4/80 expression. After migration to a tumor site, MDSCs are capable of differentiating into TAMs, limiting the efficacy of the immune response by inducing T-cell apoptosis [133, 134]. MDSCs isolated from the spleen of tumor-bearing mice arrive at the tumor site and became F4/80+ TAMs, characterized by constitutive expression of ARG1 and iNOS [133]. A recent study found that HIF-1α was a key component of this differential process [135]. Hypoxia selectively increase the expression of PD-L1, an extremely important target in ICIs, in MDSCs via HIF-1α directly binding to the PD-L1 proximal promoter [121]. Moreover, recent reports suggested that significant downregulation of STAT3 is a major factor in regulating this kind of differentiation. Hypoxia-induced CD45 protein tyrosine phosphatases caused upregulation of HIF-1α and downregulation of STAT3, facilitating the differentiation of M-MDSCs into TAMs [50]. Another study indicated that circulating M-MDSCs were essential for TAMs accumulation [136]. Additionally, M-MDSCs can differentiate into mature macrophages and DC [137]. Ginderachter et al. demonstrated that M-MDSCs in the spleen could turn into M2 macrophages [138]. Inhibition of STAT3 in MDSCs facilitates their conversion to mature DCs [139].
It is well known that IL-17 is the key cytokine produced by Th17 cells [140]. One study found that MDSCs producing IL-1β, IL-6, and IL-23 promoted the differentiation of Th17 cells, which is critically NO-dependent [141]. Furthermore, innate γδT17 cells were demonstrated to be the major cellular source of IL-17, promoting the accumulation of MDSCs in human colorectal cancer [142].
Cancer-associated fibroblasts (CAFs) can polarize monocytes and convert them into MDSCs by increasing oxidative stress, with suppression of CD8+ T-cell activity and the production of IFN-γ. Furthermore, in the presence of a NOX2 inhibitor, CAF-induced MDSCs were found to attenuate ROS production and restore antitumor immunity [143]. Additionally, MDSCs have the ability to nonspontaneously differentiate into fibroblasts in the lung under the influence of CD4+ T cells [144]. Knockout of KLF4, a transcription factor that is crucial to monocyte differentiation and tumor development, decrease the generation of MDSCs and MDSC-derived fibrocytes in the lung, reducing pulmonary metastasis [145]. Indeed, these fibrocytes, mediating immune suppression via indoleamine oxidase (IDO) and Tregs expansion, have been described as a novel subset of cancer-induced MDSCs in patients with metastatic cancer [146, 147]. In addition, a study using a bone metastasis mouse model suggested that MDSCs are capable of differentiating into functional osteoclasts both in vivo and in vitro, mechanistically dependent on NO [148].
Harnessing MDSCs for therapy
MDSCs perform an essential function in tumor-associated immune suppression, which subsequently greatly limits the therapeutic effectiveness of cancer immunotherapy [149]. Therefore, how to eliminate these cells and reconstitute the immunosuppressive microenvironment has become a focus of research in this field. Current clinical therapies targeting MDSCs are mainly focused on four aspects: depleting MDSCs, differentiating MDSCs, inhibiting MDSCs immunosuppressive activity, and blocking MDSCs expansion or activation [150, 151] (Fig. 7).

The MDSC-targeting therapeutic strategies. Current clinical therapies targeting MDSCs are mainly focused on four aspects: depleting MDSCs, differentiating MDSCs, inhibiting MDSCs immunosuppressive activity, and blocking MDSCs expansion or activation
Depletion of MDSCs
Chemotherapy can eliminate immunosuppressive cells from the TME [152]. Gemcitabine and 5-fluorouracil selectively induced the apoptosis of MDSCs in the spleen and tumor site and enhanced the antigen-specific production of IFN-γ by intratumor CD8+ T cells [153]. Carboplatin and paclitaxel reduced the abnormally increased circulating MDSCs and fostered vigorous antitumor responses in advanced cervical cancer patients [154]. However, these agents are not specific to MDSCs and affect all rapidly proliferating cells, including effector T cells.
Gemtuzumab ozogamicin (GO) is a CD33-targeted antibody–drug conjugate (ADC) linked to calicheamicin, that specifically targets the membrane antigen CD33 and releases a derivative of the cytotoxic calicheamicin component after internalization, leading to tumor cell death [155, 156]. GO has been approved for the treatment of CD33+ acute myeloid leukemia and had an acceptable safety profile in multiple clinical trials [157,158,159]. Although human PMN-MDSCs and M-MDSCs are transcriptomically distinct, CD33 is a common target for MDSCs regardless of subtype. GO was found to increase the death of MDSCs, providing a clinically plausible approach to deplete MDSCs in cancer patients [160].
Differentiating MDSCs
MDSCs differentiation is regulated by complex signals, but the specific regulatory mechanisms are not well understood. All-trans retinoic acid (ATRA) was previously found to show potent activity on MDSCs [85]. In vivo administration of ATRA significantly decreased the presence of MDSCs by differentiating MDSCs into mature myeloid cells [161]. ATRA was also shown to abrogate MDSC-mediated immunosuppression [162, 163]. To determine the mechanism of this effect, Nefedova et al. found that ATRA specifically upregulated the gene expression of glutathione synthase (GSS) and glutathione (GSH) accumulation in MDSCs [116]. Indeed, inhibiting GSH synthesis blocked the effect of ATRA on MDSCs [116]. In preclinical models, ATRA was shown to remove MDSCs for improvement of efficacy of antiangiogenic therapies in breast cancer [164]. Ipilimumab, a fully humanized antibody targeting cytotoxic T-lymphocyte antigen-4 (CTLA-4), was the first approved therapy in advanced melanoma patients [165]. However, melanoma wields substantial immunosuppressive mechanisms, especially an increase in circulating MDSCs, limiting the efficacy of ipilimumab [166]. In a randomized phase II clinical trial, ipilimumab monotherapy or ipilimumab plus ATRA was used to treat patients with advanced melanoma. ATRA combined therapy was found to significantly reduce the frequency of circulating MDSCs with a safe profile (NCT02403778 ) [167]. However, the poor solubility and fast metabolism of ATRA limits its applications in cancer immunotherapy. HF1K16, a pegylated liposome formulation of ATRA with a great dose loading capacity and sustained drug release property, is under phase I clinical trial for its safety and tolerability (NCT05388487).
In addition, CpG oligonucleotides (ODNs), a Toll-like receptor 9 (TLR9) agonist, directly induces the activation of the immune response [168]. One study examined the effect of CpG ODN on MDSCs and found a decline in the frequency and inhibitory activity of M-MDSCs partly for inducing the differentiation of M-MDSCs into M1-like macrophages [169]. IFN-α stimulated by CpG is a key effector for the induction of MDSC maturation in vitro [170]. Notably, the codelivery of CpG ODN and TLR7/8 agonists more significantly reduced the frequency of M-MDSCs compared with monotherapy [171]. Another study showed that low concentrations of paclitaxel neither increased MDSCs apoptosis nor blocked MDSCs generation but stimulated MDSCs differentiation toward mature DCs [172].
Inhibition of MDSCs immunosuppression
Targeting the biochemical pathways of MDSCs, such as with ARG1, iNOS, COX2 and TGF-β inhibitors, is a good strategy to improve the effectiveness of various immunotherapies [173]. In several mouse tumor models, the phosphodiesterase-5 (PDE5) inhibitor sildenafil, tadalafil and vardenafil downregulates the expression of ARG1 and iNOS, reversing MDSC-induced immunosuppression and restoring antitumor immunity [173, 174]. Subsequently, sildenafil has also been shown to reduce MDSCs in a transgenic mouse melanoma model [175]. Moreover, multiple clinical trials have demonstrated that tadalafil reduces MDSCs concentrations and augments general and tumor-specific immunity in both HNSCC and metastatic melanoma patients [176,177,178].
Recently, the impact of histone deacetylase inhibitors (HADCi) on MDSCs has attracted a great deal of attention [179, 180]. A corrective analysis of a randomized, phase II trial in patients with breast cancer demonstrated that entinostat, a class I HADCi, decreased the frequency of circulating PMN-MDSCs and M-MDSCs [181]. A preclinical study showed that entinostat targeted MDSCs and increased the efficacy of ICIs in murine colorectal and breast cancers [182]. Entinostat reprogrammed tumor-infiltrating MDSCs by significantly inhibiting the expression of ARG1, iNOS and COX2 and suppressing the function of immunosuppressive MDSCs, thereby overcoming immune resistance [183, 184].
In addition, the COX2 inhibitor celecoxib blocks MDSCs suppressive function and delays tumor development by decreasing the expression of ARG1 [185]. Preclinical studies have shown that ARG inhibitors, which reverse the inhibition of T cells by blocking L-arginine depletion, reduce tumor growth in mouse models [186]. A phase I study (NCT02903914) was initiated to test the antitumor activity of ARG inhibitors alone or combined with anti-PD-1. IDO orchestrates immunosuppressive effects through recruitment and activation of MDSCs in a Treg-dependent manner. A selective IDO inhibitor was found in vivo to reverse tumor growth by decreasing the numbers of tumor-infiltrating MDSCs and abolishing their suppressive function [187].
Blockade of MDSCs accumulation
Given the essential role of STAT3 in MDSCs accumulation, blocking STAT3 is a promising approach for MDSC-targeted immunotherapy. AZD9150, an antisense oligonucleotide designed to downregulate the expression of STAT3 mRNA, shows potent antitumor activity in patients with lymphoma and NSCLC [188, 189]. Preclinical data have provided evidence that AZD9150 accompanied with PD-L1 antibody displayed enhanced the antitumor activity [190]. These data provide a rationale for testing this combination in the clinic. AZD9150 is now being investigated in several phase I/II clinical trials in combination with ICIs.
In addition, clinical trials with sunitinib, a tyrosine kinase inhibitor, revealed that it could target MDSCs by blocking VEGF, a promotor for MDSCs expansion described above. Sunitinib significantly reduced MDSCs in patients with renal cell carcinoma [191]. Moreover, sunitinib was found to abrogate highly increased MDSCs, enhancing the efficacy of stereotactic body radiotherapy (SBRT) in patients with oligometastases [192].
MDSCs are recruited into the TME via interactions between chemokines and chemokine receptors [193]. M-MDSCs are recruited via CXCR4-CXCL12, CXCR2-CXCL5/CXCL8, and CCR2-CCL2 signaling, whereas CXCR1-CXCL8, CXCR2-CXCL8, and CCR5-CCL5 axes contribute to the recruitment of PMN-MDSCs [194, 195]. Targeting these chemokine receptors may prevent the accumulation of MDSCs in the TME. Inhibition of CXCR2 has been shown to rescue MDSCs trafficking and enhance anti-PD-1 efficacy in murine glioblastoma and rhabdomyosarcoma [196, 197]. Moreover, CXCR4 blockade has been shown to synergize with anti-PD-1 therapy in several mouse models [198]. A phase IIa, open-label, two-cohort clinical trial was conducted to assess the safety, efficacy and immunobiological effects of BL-8040, a CXCR4 antagonist. Notably, the CXCR4 antagonist decreased the number of MDSCs [199].
Benefiting from the advent of quantitative tools, such as single-cell RNA sequencing (scRNA-seq) and high-dimensional cytometry, additional phenotypes and therapeutic targets of MDSCs have progressed considerably [200]. In a mouse model of melanoma, GCN2, an environmental sensor controlling transcription and translation, was shown to be required for the phenotypes and function of MDSCs, making it an attractive target for decreasing MDSCs [201]. Depletion of GCN2 increased the inflammatory pathway with the strongest impact on the IL-1β pathway [201]. Another study found that MDSCs drove glioblastoma growth in a sex-specific manner. M-MDSCs could be targeted with antiproliferative agents in males, whereas IL-1β inhibitors were identified as potential drug candidates to target PMN-MDSCs in females. Strikingly, anti-IL-1β treatment counteracted PMN-MDSC-mediated immunosuppression and potently prolonged the survival of female mice, further providing the rationale for clinical testing of IL-1β inhibitors in cancer patients [31]. Using scRNA-seq, Alshetaiwi et al. delineated the molecular features of MDSCs in a mouse model of breast cancer and identified CD84 and JAML as several novel surface markers for faithful MDSC detection [202]. CD84 is a member of the signaling lymphocytic activation molecule (SLAM) family of cell-surface immunoreceptors, broadly expressed on most immune cell subsets [203]. JAML is a member of the junctional adhesion molecule (JAM) family and is expressed on neutrophils and monocytes [204].
Although these emerging quantitative tools provide numerous of previously unappreciated insights into the targets and biology of MDSCs, there are potential limitations here [205]. One limitation is that scRNA-seq may lack the surface protein information, thereby leading to misnamed or misclassified MDSC subtypes.
Conclusion
The complexity of the tumor immune microenvironment has been gradually revealed by the combination of scRNA-seq and spatial omics [206, 207]. Not only the compositions and molecular features, but also the spatial architecture of immune components in the TME determine antitumor activity [208]. MDSCs, as a key component in the TME, are now recognized as an emerging target for anticancer immunotherapy, and their role in cancer development and treatment response is increasingly appreciated. However, due to ambiguous phenotypes, great heterogeneity and the complex network of origin and function, current therapeutic strategies targeting MDSCs are only partially effective [209]. There is a critical urgency to address the complexity and heterogeneity of MDSCs to develop novel clinical targets and strategies. In the coming years, it will be seen whether targeting MDSCs combined with ICIs may overcome the existing limitations of cancer immunotherapy.
Availability of data and materials
Not applicable.
Abbreviations
- MDSCs:
-
Myeloid-derived suppressor cells
- ICIs:
-
Immune checkpoint inhibitors
- TME:
-
Tumor microenvironment
- HSCs:
-
Hematopoietic stem cells
- DCs:
-
Dendritic cells
- IMCs:
-
Immature myeloid cells
- MSCs:
-
Myeloid suppressor cells
- PMN-MDSCs:
-
Polymorphic nuclei-MDSCs
- M-MDSCs:
-
Mononuclear-MDSCs
- MLPGs:
-
Monocyte-like precursors of granulocytes
- ARG1:
-
Arginase I
- iNOS:
-
Inducible nitric oxide synthase
- NO:
-
Nitric oxide
- ROS:
-
Reactive oxygen species
- PBMCs:
-
Peripheral blood mononuclear cells
- TCR:
-
T cell receptor
- NOX2:
-
NADPH oxidase
- O2− :
-
Superoxide
- H2O2 :
-
Hydrogen peroxide
- ONOO− :
-
Peroxynitrite
- CMPs:
-
Common myeloid progenitors
- GMPs:
-
Granulocyte–macrophage progenitors
- GPs:
-
Granulocyte progenitors
- MPs:
-
Monocytic progenitors
- STAT3:
-
Signal transducer and activator of transcription3
- Treg:
-
Regulatory T
- TAMs:
-
Tumor-associated macrophages
- FOXP3:
-
Forkhead box transcription factor
- CAFs:
-
Cancer-associated fibroblasts
- IDO:
-
Indoleamine oxidase
- ATRA:
-
All-trans retinoic acid
- HNSCC:
-
Head and neck squamous cell carcinoma
- NSCLC:
-
Non-small cell lung cancer
- PDE5:
-
Phosphodiesterase-5
- ADC:
-
Antibody–drug conjugate
- HADCi:
-
Histone deacetylase inhibitors
- CTLA-4:
-
Cytotoxic T-lymphocyte antigen-4
- scRNA-seq:
-
Single-cell RNA sequencing
References
Zhu S, Zhang T, Zheng L, Liu H, Song W, Liu D, et al. Combination strategies to maximize the benefits of cancer immunotherapy. J Hematol Oncol. 2021;14(1):156.
Ostrand-Rosenberg S, Sinha P. Myeloid-derived suppressor cells: linking inflammation and Cancer. J Immunol. 2009;182(8):4499–506.
Schulz C, Gomez Perdiguero E, Chorro L, Szabo-Rogers H, Cagnard N, Kierdorf K, et al. A lineage of myeloid cells independent of Myb and hematopoietic stem cells. Science. 2012;336(6077):86–90.
Gabrilovich DI, Ostrand-Rosenberg S, Bronte V. Coordinated regulation of myeloid cells by tumours. Nat Rev Immunol. 2012;12(4):253–68.
Solito S, Falisi E, Diaz-Montero CM, Doni A, Pinton L, Rosato A, et al. A human promyelocytic-like population is responsible for the immune suppression mediated by myeloid-derived suppressor cells. Blood. 2011;118(8):2254–65.
Yang Z, Guo J, Weng L, Tang W, Jin S, Ma W. Myeloid-derived suppressor cells-new and exciting players in lung cancer. J Hematol Oncol. 2020;13(1):10.
Yu S, Ren X, Li L. Myeloid-derived suppressor cells in hematologic malignancies: two sides of the same coin. Exp Hematol Oncol. 2022;11(1):43.
Hao Z, Li R, Wang Y, Li S, Hong Z, Han Z. Landscape of myeloid-derived suppressor cell in tumor immunotherapy. Biomark Res. 2021;9(1):77.
Bennett JA, Rao VS, Mitchell MS. Systemic bacillus Calmette-Guérin (BCG) activates natural suppressor cells. Proc Natl Acad Sci. 1978;75(10):5142–4.
Almand B, Clark JI, Nikitina E, van Beynen J, English NR, Knight SC, et al. Increased production of immature myeloid cells in Cancer patients: a mechanism of immunosuppression in Cancer. J Immunol. 2001;166(1):678–89.
Huang B, Pan PY, Li Q, Sato AI, Levy DE, Bromberg J, et al. Gr-1+CD115+ immature myeloid suppressor cells mediate the development of tumor-induced T regulatory cells and T-cell anergy in tumor-bearing host. Cancer Res. 2006;66(2):1123–31.
Gabrilovich DI, Bronte V, Chen S-H, Colombo MP, Ochoa A, Ostrand-Rosenberg S, et al. The terminology issue for myeloid-derived suppressor cells. Cancer Res. 2007;67(1):425.
Yang R, Cai Z, Zhang Y, Yutzy Iv WH, Roby KF, Roden RBS. CD80 in immune suppression by mouse ovarian carcinoma-associated gr-1 +CD11b + myeloid cells. Cancer Res. 2006;66(13):6807–15.
Bronte V, Brandau S, Chen SH, Colombo MP, Frey AB, Greten TF, et al. Recommendations for myeloid-derived suppressor cell nomenclature and characterization standards. Nat Commun. 2016;7:12150.
Mastio J, Condamine T, Dominguez G, Kossenkov AV, Donthireddy L, Veglia F, et al. Identification of monocyte-like precursors of granulocytes in cancer as a mechanism for accumulation of PMN-MDSCs. J Exp Med. 2019;216(9):2150–69.
Haile LA, Gamrekelashvili J, Manns MP, Korangy F, Greten TF. CD49d is a new marker for distinct myeloid-derived suppressor cell subpopulations in mice. J Immunol. 2010;185(1):203–10.
Arihara F, Mizukoshi E, Kitahara M, Takata Y, Arai K, Yamashita T, et al. Increase in CD14+HLA-DR −/low myeloid-derived suppressor cells in hepatocellular carcinoma patients and its impact on prognosis. Cancer Immunol Immunother. 2013;62(8):1421–30.
Diaz-Montero CM, Salem ML, Nishimura MI, Garrett-Mayer E, Cole DJ, Montero AJ. Increased circulating myeloid-derived suppressor cells correlate with clinical cancer stage, metastatic tumor burden, and doxorubicin-cyclophosphamide chemotherapy. Cancer Immunol Immunother. 2009;58(1):49–59.
Angell TE, Lechner MG, Smith AM, Martin SE, Groshen SG, Maceri DR, et al. Circulating myeloid-derived suppressor cells predict differentiated thyroid Cancer diagnosis and extent. Thyroid. 2016;26(3):381–9.
Huang A, Zhang B, Wang B, Zhang F, Fan KX, Guo YJ. Increased CD14(+)HLA-DR (−/low) myeloid-derived suppressor cells correlate with extrathoracic metastasis and poor response to chemotherapy in non-small cell lung cancer patients. Cancer Immunol Immunother. 2013;62(9):1439–51.
Tada K, Kitano S, Shoji H, Nishimura T, Shimada Y, Nagashima K, et al. Pretreatment immune status correlates with progression-free survival in chemotherapy-treated metastatic colorectal Cancer patients. Cancer Immunol Res. 2016;4(7):592–9.
Butterfield LH, Zhao F, Lee S, Tarhini AA, Margolin KA, White RL, et al. Immune correlates of GM-CSF and melanoma peptide vaccination in a randomized trial for the adjuvant therapy of resected high-risk melanoma (E4697). Clin Cancer Res. 2017;23(17):5034–43.
Davis RJ, Moore EC, Clavijo PE, Friedman J, Cash H, Chen Z, et al. Anti-PD-L1 efficacy can be enhanced by inhibition of myeloid-derived suppressor cells with a selective inhibitor of PI3Kδ/γ. Cancer Res. 2017;77(10):2607–19.
Mandruzzato S, Solito S, Falisi E, Francescato S, Chiarion-Sileni V, Mocellin S, et al. IL4Ralpha+ myeloid-derived suppressor cell expansion in cancer patients. J Immunol. 2009;182(10):6562–8.
Gallina G, Dolcetti L, Serafini P, De Santo C, Marigo I, Colombo MP, et al. Tumors induce a subset of inflammatory monocytes with immunosuppressive activity on CD8+ T cells. J Clin Invest. 2006;116(10):2777–90.
Condamine T, Mastio J, Gabrilovich DI. Transcriptional regulation of myeloid-derived suppressor cells. J Leukoc Biol. 2015;98(6):913–22.
Youn J-I, Nagaraj S, Collazo M, Gabrilovich DI. Subsets of myeloid-derived suppressor cells in tumor-bearing mice. J Immunol. 2008;181:5791–802.
Lee Y, Auh SL, Wang Y, Burnette B, Wang Y, Meng Y, et al. Therapeutic effects of ablative radiation on local tumor require CD8+ T cells: changing strategies for cancer treatment. Blood. 2009;114(3):589–95.
Gabrilovich DI, Nagaraj S. Myeloid-derived suppressor cells as regulators of the immune system. Nat Rev Immunol. 2009;9(3):162–74.
Movahedi K, Guilliams M, Van den Bossche J, Van den Bergh R, Gysemans C, Beschin A, et al. Identification of discrete tumor-induced myeloid-derived suppressor cell subpopulations with distinct T cell-suppressive activity. Blood. 2008;111(8):4233–44.
Bayik D, Zhou Y, Park C, Hong C, Vail D, Silver DJ, et al. Myeloid-derived suppressor cell subsets drive glioblastoma growth in a sex-specific manner. Cancer Discov. 2020;10(8):1210–25.
Youn J-I, Collazo M, Shalova IN, Biswas SK, Gabrilovich DI. Characterization of the nature of granulocytic myeloid-derived suppressor cells in tumor-bearing mice. J Leukoc Biol. 2012;91(1):167–81.
Veglia F, Perego M, Gabrilovich D. Myeloid-derived suppressor cells coming of age. Nat Immunol. 2018;19(2):108–19.
Condamine T, Dominguez GA, Youn JI, Kossenkov AV, Mony S, Alicea-Torres K, et al. Lectin-type oxidized LDL receptor-1 distinguishes population of human polymorphonuclear myeloid-derived suppressor cells in cancer patients. Sci Immunol. 2016;1(2):aaf8943. https://doi.org/10.1126/sciimmunol.aaf8943.
Qian B-Z, Pollard JW. Macrophage diversity enhances tumor progression and metastasis. Cell. 2010;141(1):39–51.
Casbon A-J, Reynaud D, Park C, Khuc E, Gan DD, Schepers K, et al. Invasive breast cancer reprograms early myeloid differentiation in the bone marrow to generate immunosuppressive neutrophils. Proc Natl Acad Sci. 2015;112(6):E566–75.
Yáñez A, Ng MY, Hassanzadeh-Kiabi N, Goodridge HS. IRF8 acts in lineage-committed rather than oligopotent progenitors to control neutrophil vs monocyte production. Blood. 2015;125(9):1452–9.
Condamine T, Gabrilovich DI. Molecular mechanisms regulating myeloid-derived suppressor cell differentiation and function. Trends Immunol. 2011;32(1):19–25.
Jin S, Yang Z, Hao X, Tang W, Ma W, Zong H. Roles of HMGB1 in regulating myeloid-derived suppressor cells in the tumor microenvironment. Biomark Res. 2020;8:21.
Becher B, Tugues S, Greter M. GM-CSF: from growth factor to central mediator of tissue inflammation. Immunity. 2016;45(5):963–73.
Bronte V, Chappell DB, Apolloni E, Cabrelle A, Wang M, Hwu P, et al. Unopposed production of granulocyte-macrophage colony-stimulating factor by tumors inhibits CD8+ T cell responses by dysregulating antigen-presenting cell maturation. J Immunol. 1999;162(10):5728–37.
Dolcetti L, Peranzoni E, Ugel S, Marigo I, Fernandez Gomez A, Mesa C, et al. Hierarchy of immunosuppressive strength among myeloid-derived suppressor cell subsets is determined by GM-CSF. Eur J Immunol. 2010;40(1):22–35.
Melani C, Chiodoni C, Forni G, Colombo MP. Myeloid cell expansion elicited by the progression of spontaneous mammary carcinomas in c-erbB-2 transgenic BALB/c mice suppresses immune reactivity. Blood. 2003;102(6):2138–45.
Almand B, Resser JR, Lindman B, Nadaf S, Clark JI, Kwon ED, et al. Clinical significance of defective dendritic cell differentiation in cancer. Clin Cancer Res. 2000;6(5):1755-66.
Yu H, Lee H, Herrmann A, Buettner R, Jove R. Revisiting STAT3 signalling in cancer: new and unexpected biological functions. Nat Rev Cancer. 2014;14(11):736–46.
Lee JK, Won C, Yi EH, Seok SH, Kim MH, Kim SJ, et al. Signal transducer and activator of transcription 3 (Stat3) contributes to T-cell homeostasis by regulating pro-survival Bcl-2 family genes. Immunology. 2013;140(3):288–300.
Vasquez-Dunddel D, Pan F, Zeng Q, Gorbounov M, Albesiano E, Fu J, et al. STAT3 regulates arginase-I in myeloid-derived suppressor cells from cancer patients. J Clin Invest. 2013;123(4):1580–9.
Nefedova Y, Huang M, Kusmartsev S, Bhattacharya R, Cheng P, Salup R, et al. Hyperactivation of STAT3 is involved in abnormal differentiation of dendritic cells in Cancer. J Immunol. 2004;172(1):464–74.
Xin H, Zhang C, Herrmann A, Du Y, Figlin R, Yu H. Sunitinib inhibition of Stat3 induces renal cell carcinoma tumor cell apoptosis and reduces immunosuppressive cells. Cancer Res. 2009;69(6):2506–13.
Kumar V, Cheng P, Condamine T, Mony S, Languino LR, McCaffrey JC, et al. CD45 phosphatase inhibits STAT3 transcription factor activity in myeloid cells and promotes tumor-associated macrophage differentiation. Immunity. 2016;44(2):303–15.
Kortylewski M, Kujawski M, Wang T, Wei S, Zhang S, Pilon-Thomas S, et al. Inhibiting Stat3 signaling in the hematopoietic system elicits multicomponent antitumor immunity. Nat Med. 2005;11(12):1314–21.
Nefedova Y, Nagaraj S, Rosenbauer A, Muro-Cacho C, Sebti SM, Gabrilovich DI. Regulation of dendritic cell differentiation and antitumor immune response in cancer by pharmacologic-selective inhibition of the janus-activated kinase 2/signal transducers and activators of transcription 3 pathway. Cancer Res. 2005;65(20):9525–35.
Ko JS, Rayman P, Ireland J, Swaidani S, Li G, Bunting KD, et al. Direct and differential suppression of myeloid-derived suppressor cell subsets by sunitinib is compartmentally constrained. Cancer Res. 2010;70(9):3526–36.
Abad C, Nobuta H, Li J, Kasai A, Yong WH, Waschek JA. Targeted STAT3 disruption in myeloid cells alters immunosuppressor cell abundance in a murine model of spontaneous medulloblastoma. J Leukoc Biol. 2014;95(2):357–67.
Laouedj M, Tardif MR, Gil L, Raquil MA, Lachhab A, Pelletier M, et al. S100A9 induces differentiation of acute myeloid leukemia cells through TLR4. Blood. 2017;129(14):1980–90.
Sinha P, Okoro C, Foell D, Freeze HH, Ostrand-Rosenberg S, Srikrishna G. Proinflammatory S100 proteins regulate the accumulation of myeloid-derived suppressor cells. J Immunol. 2008;181(7):4666–75.
Cheng P, Corzo CA, Luetteke N, Yu B, Nagaraj S, Bui MM, et al. Inhibition of dendritic cell differentiation and accumulation of myeloid-derived suppressor cells in cancer is regulated by S100A9 protein. J Exp Med. 2008;205(10):2235–49.
Chen X, Eksioglu EA, Zhou J, Zhang L, Djeu J, Fortenbery N, et al. Induction of myelodysplasia by myeloid-derived suppressor cells. J Clin Invest. 2013;123(11):4595–611.
Tamura A, Hirai H, Yokota A, Kamio N, Sato A, Shoji T, et al. C/EBPβ is required for survival of Ly6C(−) monocytes. Blood. 2017;130(16):1809–18.
Wang W, Xia X, Mao L, Wang S. The CCAAT/enhancer-binding protein family: its roles in MDSC expansion and function. Front Immunol. 1804;2019:10.
Hirai H, Zhang P, Dayaram T, Hetherington CJ, Mizuno S, Imanishi J, et al. C/EBPbeta is required for ‘emergency’ granulopoiesis. Nat Immunol. 2006;7(7):732–9.
Jones LC, Lin ML, Chen SS, Krug U, Hofmann WK, Lee S, et al. Expression of C/EBPbeta from the C/ebpalpha gene locus is sufficient for normal hematopoiesis in vivo. Blood. 2002;99(6):2032–6.
Gao Y, Sun W, Shang W, Li Y, Zhang D, Wang T, et al. Lnc-C/EBPβ negatively regulates the suppressive function of myeloid-derived suppressor cells. Cancer Immunol Res. 2018;6(11):1352–63.
Dai J, Kumbhare A, Youssef D, Yao ZQ, McCall CE, El Gazzar M. Expression of C/EBPβ in myeloid progenitors during sepsis promotes immunosuppression. Mol Immunol. 2017;91:165–72.
Akagi T, Saitoh T, O'Kelly J, Akira S, Gombart AF, Koeffler HP. Impaired response to GM-CSF and G-CSF, and enhanced apoptosis in C/EBPbeta-deficient hematopoietic cells. Blood. 2008;111(6):2999–3004.
Li W, Tanikawa T, Kryczek I, Xia H, Li G, Wu K, et al. Aerobic glycolysis controls myeloid-derived suppressor cells and tumor immunity via a specific CEBPB isoform in triple-negative breast Cancer. Cell Metab. 2018;28(1):87–103.e106.
Strauss L, Sangaletti S, Consonni FM, Szebeni G, Morlacchi S, Totaro MG, et al. RORC1 regulates tumor-promoting “emergency” Granulo-Monocytopoiesis. Cancer Cell. 2015;28(2):253–69.
Marigo I, Bosio E, Solito S, Mesa C, Fernandez A, Dolcetti L, et al. Tumor-induced tolerance and immune suppression depend on the C/EBPbeta transcription factor. Immunity. 2010;32(6):790–802.
Holtschke T, Löhler J, Kanno Y, Fehr T, Giese N, Rosenbauer F, et al. Immunodeficiency and chronic myelogenous leukemia-like syndrome in mice with a targeted mutation of the ICSBP gene. Cell. 1996;87(2):307–17.
Stewart TJ, Greeneltch KM, Reid JE, Liewehr DJ, Steinberg SM, Liu K, et al. Interferon regulatory factor-8 modulates the development of tumour-induced CD11b+gr-1+ myeloid cells. J Cell Mol Med. 2009;13(9b):3939–50.
Netherby CS, Messmer MN, Burkard-Mandel L, Colligan S, Miller A, Cortes Gomez E, et al. The granulocyte progenitor stage is a key target of IRF8-mediated regulation of myeloid-derived suppressor cell production. J Immunol. 2017;198(10):4129–39.
Waight JD, Netherby C, Hensen ML, Miller A, Hu Q, Liu S, et al. Myeloid-derived suppressor cell development is regulated by a STAT/IRF-8 axis. J Clin Invest. 2013;123(10):4464–78.
Xia X, Wang W, Yin K, Wang S. Interferon regulatory factor 8 governs myeloid cell development. Cytokine Growth Factor Rev. 2020;55:48–57.
Kusmartsev SA, Li Y, Chen SH. Gr-1+ myeloid cells derived from tumor-bearing mice inhibit primary T cell activation induced through CD3/CD28 costimulation. J Immunol. 2000;165(2):779–85.
Rodriguez PC, Hernandez CP, Quiceno D, Dubinett SM, Zabaleta J, Ochoa JB, et al. Arginase I in myeloid suppressor cells is induced by COX-2 in lung carcinoma. J Exp Med. 2005;202(7):931–9.
Mao Y, Poschke I, Wennerberg E, Pico de Coaña Y, Egyhazi Brage S, Schultz I, et al. Melanoma-educated CD14+ cells acquire a myeloid-derived suppressor cell phenotype through COX-2-dependent mechanisms. Cancer Res. 2013;73(13):3877–87.
Obermajer N, Muthuswamy R, Lesnock J, Edwards RP, Kalinski P. Positive feedback between PGE2 and COX2 redirects the differentiation of human dendritic cells toward stable myeloid-derived suppressor cells. Blood. 2011;118(20):5498–505.
Porta C, Consonni FM, Morlacchi S, Sangaletti S, Bleve A, Totaro MG, et al. Tumor-derived prostaglandin E2 promotes p50 NF-κB-dependent differentiation of Monocytic MDSCs. Cancer Res. 2020;80(13):2874–88.
Mao Y, Sarhan D, Steven A, Seliger B, Kiessling R, Lundqvist A. Inhibition of tumor-derived prostaglandin-e2 blocks the induction of myeloid-derived suppressor cells and recovers natural killer cell activity. Clin Cancer Res. 2014;20(15):4096–106.
Holcik M, Sonenberg N. Translational control in stress and apoptosis. Nat Rev Mol Cell Biol. 2005;6(4):318–27.
Condamine T, Kumar V, Ramachandran IR, Youn JI, Celis E, Finnberg N, et al. ER stress regulates myeloid-derived suppressor cell fate through TRAIL-R-mediated apoptosis. J Clin Invest. 2014;124(6):2626–39.
Thevenot PT, Sierra RA, Raber PL, Al-Khami AA, Trillo-Tinoco J, Zarreii P, et al. The stress-response sensor chop regulates the function and accumulation of myeloid-derived suppressor cells in tumors. Immunity. 2014;41(3):389–401.
Parker KH, Sinha P, Horn LA, Clements VK, Yang H, Li J, et al. HMGB1 enhances immune suppression by facilitating the differentiation and suppressive activity of myeloid-derived suppressor cells. Cancer Res. 2014;74(20):5723–33.
Wu L, Yan C, Czader M, Foreman O, Blum JS, Kapur R, et al. Inhibition of PPARγ in myeloid-lineage cells induces systemic inflammation, immunosuppression, and tumorigenesis. Blood. 2012;119(1):115–26.
Gabrilovich DI, Velders MP, Sotomayor EM, Kast WM. Mechanism of immune dysfunction in cancer mediated by immature Gr-1+ myeloid cells. J Immunol. 2001;166(9):5398–406.
Solito S, Bronte V, Mandruzzato S. Antigen specificity of immune suppression by myeloid-derived suppressor cells. J Leukoc Biol. 2011;90(1):31–6.
Apolloni E, Bronte V, Mazzoni A, Serafini P, Cabrelle A, Segal DM, et al. Immortalized myeloid suppressor cells trigger apoptosis in antigen-activated T lymphocytes. J Immunol. 2000;165(12):6723–30.
Mazzoni A, Bronte V, Visintin A, Spitzer JH, Apolloni E, Serafini P, et al. Myeloid suppressor lines inhibit T cell responses by an NO-dependent mechanism. J Immunol. 2002;168(2):689–95.
Marvel D, Gabrilovich DI. Myeloid-derived suppressor cells in the tumor microenvironment: expect the unexpected. J Clin Invest. 2015;125(9):3356–64.
Terabe M, Matsui S, Park JM, Mamura M, Noben-Trauth N, Donaldson DD, et al. Transforming growth factor-beta production and myeloid cells are an effector mechanism through which CD1d-restricted T cells block cytotoxic T lymphocyte-mediated tumor immunosurveillance: abrogation prevents tumor recurrence. J Exp Med. 2003;198(11):1741–52.
Li T, Liu T, Zhu W, Xie S, Zhao Z, Feng B, et al. Targeting MDSC for immune-checkpoint blockade in Cancer immunotherapy: current Progress and new prospects. Clin Med Insights Oncol. 2021;15:11795549211035540.
Grover A, Sanseviero E, Timosenko E, Gabrilovich DI. Myeloid-derived suppressor cells: a propitious road to clinic. Cancer Discov. 2021;11(11):2693–706.
Zhao H, Wu L, Yan G, Chen Y, Zhou M, Wu Y, et al. Inflammation and tumor progression: signaling pathways and targeted intervention. Signal Transduct Target Ther. 2021;6(1):263.
Wu J, Wang L, Xu J. The role of pyroptosis in modulating the tumor immune microenvironment. Biomark Res. 2022;10(1):45.
Wu G, Morris SM, Jr. Arginine metabolism: nitric oxide and beyond. Biochem J. 1998;336(1):1–17.
Bronte V, Serafini P, De Santo C, Marigo I, Tosello V, Mazzoni A, et al. IL-4-induced arginase 1 suppresses alloreactive T cells in tumor-bearing mice. J Immunol. 2003;170(1):270–8.
Rodriguez PC, Quiceno DG, Zabaleta J, Ortiz B, Zea AH, Piazuelo MB, et al. Arginase I production in the tumor microenvironment by mature myeloid cells inhibits T-cell receptor expression and antigen-specific T-cell responses. Cancer Res. 2004;64(16):5839–49.
Goh CC, Roggerson KM, Lee HC, Golden-Mason L, Rosen HR, Hahn YS. Hepatitis C virus-induced myeloid-derived suppressor cells suppress NK cell IFN-γ production by altering cellular metabolism via Arginase-1. J Immunol. 2016;196(5):2283–92.
Taheri F, Ochoa JB, Faghiri Z, Culotta K, Park HJ, Lan MS, et al. L-arginine regulates the expression of the T-cell receptor zeta chain (CD3zeta) in Jurkat cells. Clin Cancer Res. 2001;7(3 Suppl):958s–65s.
Rodriguez PC, Zea AH, DeSalvo J, Culotta KS, Zabaleta J, Quiceno DG, et al. L-arginine consumption by macrophages modulates the expression of CD3 zeta chain in T lymphocytes. J Immunol. 2003;171(3):1232–9.
Sinha P, Clements VK, Ostrand-Rosenberg S. Interleukin-13-regulated M2 macrophages in combination with myeloid suppressor cells block immune surveillance against metastasis. Cancer Res. 2005;65(24):11743–51.
Rodriguez PC, Quiceno DG, Ochoa AC. L-arginine availability regulates T-lymphocyte cell-cycle progression. Blood. 2007;109(4):1568–73.
Zea AH, Rodriguez PC, Atkins MB, Hernandez C, Signoretti S, Zabaleta J, et al. Arginase-producing myeloid suppressor cells in renal cell carcinoma patients: a mechanism of tumor evasion. Cancer Res. 2005;65(8):3044–8.
Srivastava MK, Sinha P, Clements VK, Rodriguez P, Ostrand-Rosenberg S. Myeloid-derived suppressor cells inhibit T-cell activation by depleting cystine and cysteine. Cancer Res. 2010;70(1):68–77.
Cinelli MA, Do HT, Miley GP, Silverman RB. Inducible nitric oxide synthase: regulation, structure, and inhibition. Med Res Rev. 2020;40(1):158–89.
Chung AW, Anand K, Anselme AC, Chan AA, Gupta N, Venta LA, et al. A phase 1/2 clinical trial of the nitric oxide synthase inhibitor L-NMMA and taxane for treating chemoresistant triple-negative breast cancer. Sci Transl Med. 2021;13(624):eabj5070.
García-Ortiz A, Serrador JM. Nitric oxide signaling in T cell-mediated immunity. Trends Mol Med. 2018;24(4):412–27.
Salimian Rizi B, Achreja A, Nagrath D. Nitric oxide: the forgotten child of tumor metabolism. Trends Cancer. 2017;3(9):659–72.
Xue Q, Yan Y, Zhang R, Xiong H. Regulation of iNOS on immune cells and its role in diseases. Int J Mol Sci. 2018;19(12):3805.
Sica A, Bronte V. Altered macrophage differentiation and immune dysfunction in tumor development. J Clin Invest. 2007;117(5):1155–66.
Vannini F, Kashfi K, Nath N. The dual role of iNOS in cancer. Redox Biol. 2015;6:334–43.
Gehad AE, Lichtman MK, Schmults CD, Teague JE, Calarese AW, Jiang Y, et al. Nitric oxide-producing myeloid-derived suppressor cells inhibit vascular E-selectin expression in human squamous cell carcinomas. J Invest Dermatol. 2012;132(11):2642–51.
Huang B, Lei Z, Zhao J, Gong W, Liu J, Chen Z, et al. CCL2/CCR2 pathway mediates recruitment of myeloid suppressor cells to cancers. Cancer Lett. 2007;252(1):86–92.
Bronte V, Zanovello P. Regulation of immune responses by L-arginine metabolism. Nat Rev Immunol. 2005;5(8):641–54.
Nagaraj S, Gupta K, Pisarev V, Kinarsky L, Sherman S, Kang L, et al. Altered recognition of antigen is a mechanism of CD8+ T cell tolerance in cancer. Nat Med. 2007;13(7):828–35.
Nefedova Y, Fishman M, Sherman S, Wang X, Beg AA, Gabrilovich DI. Mechanism of all-trans retinoic acid effect on tumor-associated myeloid-derived suppressor cells. Cancer Res. 2007;67(22):11021–8.
Cheung EC, Vousden KH. The role of ROS in tumour development and progression. Nat Rev Cancer. 2022;22(5):280–97.
Corzo CA, Cotter MJ, Cheng P, Cheng F, Kusmartsev S, Sotomayor E, et al. Mechanism regulating reactive oxygen species in tumor-induced myeloid-derived suppressor cells. J Immunol. 2009;182(9):5693–701.
Kusmartsev S, Nefedova Y, Yoder D, Gabrilovich DI. Antigen-specific inhibition of CD8+ T cell response by immature myeloid cells in cancer is mediated by reactive oxygen species. J Immunol. 2004;172(2):989–99.
Otsuji M, Kimura Y, Aoe T, Okamoto Y, Saito T. Oxidative stress by tumor-derived macrophages suppresses the expression of CD3 zeta chain of T-cell receptor complex and antigen-specific T-cell responses. Proc Natl Acad Sci U S A. 1996;93(23):13119–24.
Noman MZ, Desantis G, Janji B, Hasmim M, Karray S, Dessen P, et al. PD-L1 is a novel direct target of HIF-1α, and its blockade under hypoxia enhanced MDSC-mediated T cell activation. J Exp Med. 2014;211(5):781–90.
Prima V, Kaliberova LN, Kaliberov S, Curiel DT, Kusmartsev S. COX2/mPGES1/PGE2 pathway regulates PD-L1 expression in tumor-associated macrophages and myeloid-derived suppressor cells. Proc Natl Acad Sci U S A. 2017;114(5):1117–22.
Shen M, Wang J, Yu W, Zhang C, Liu M, Wang K, et al. A novel MDSC-induced PD-1(−)PD-L1(+) B-cell subset in breast tumor microenvironment possesses immuno-suppressive properties. Oncoimmunology. 2018;7(4):e1413520.
Liu C, Yu S, Kappes J, Wang J, Grizzle WE, Zinn KR, et al. Expansion of spleen myeloid suppressor cells represses NK cell cytotoxicity in tumor-bearing host. Blood. 2007;109(10):4336–42.
Li H, Han Y, Guo Q, Zhang M, Cao X. Cancer-expanded myeloid-derived suppressor cells induce anergy of NK cells through membrane-bound TGF-beta 1. J Immunol. 2009;182(1):240–9.
Nausch N, Galani IE, Schlecker E, Cerwenka A. Mononuclear myeloid-derived “suppressor” cells express RAE-1 and activate natural killer cells. Blood. 2008;112(10):4080–9.
Serafini P, Borrello I, Bronte V. Myeloid suppressor cells in cancer: recruitment, phenotype, properties, and mechanisms of immune suppression. Semin Cancer Biol. 2006;16(1):53–65.
Jenkins RW, Barbie DA, Flaherty KT. Mechanisms of resistance to immune checkpoint inhibitors. Br J Cancer. 2018;118(1):9–16.
Wang L, He T, Liu J, Tai J, Wang B, Chen Z, et al. Pan-cancer analysis reveals tumor-associated macrophage communication in the tumor microenvironment. Exp Hematol Oncol. 2021;10(1):31.
Qiu Y, Chen T, Hu R, Zhu R, Li C, Ruan Y, et al. Next frontier in tumor immunotherapy: macrophage-mediated immune evasion. Biomark Res. 2021;9(1):72.
Zhu S, Yi M, Wu Y, Dong B, Wu K. Roles of tumor-associated macrophages in tumor progression: implications on therapeutic strategies. Exp Hematol Oncol. 2021;10(1):60.
Liu F, Qin L, Liao Z, Song J, Yuan C, Liu Y, et al. Microenvironment characterization and multi-omics signatures related to prognosis and immunotherapy response of hepatocellular carcinoma. Exp Hematol Oncol. 2020;9:10.
Kusmartsev S, Gabrilovich DI. STAT1 signaling regulates tumor-associated macrophage-mediated T cell deletion. J Immunol. 2005;174(8):4880–91.
Franklin RA, Liao W, Sarkar A, Kim MV, Bivona MR, Liu K, et al. The cellular and molecular origin of tumor-associated macrophages. Science. 2014;344(6186):921–5.
Corzo CA, Condamine T, Lu L, Cotter MJ, Youn JI, Cheng P, et al. HIF-1α regulates function and differentiation of myeloid-derived suppressor cells in the tumor microenvironment. J Exp Med. 2010;207(11):2439–53.
Noy R, Pollard JW. Tumor-associated macrophages: from mechanisms to therapy. Immunity. 2014;41(1):49–61.
Bunt SK, Yang L, Sinha P, Clements VK, Leips J, Ostrand-Rosenberg S. Reduced inflammation in the tumor microenvironment delays the accumulation of myeloid-derived suppressor cells and limits tumor progression. Cancer Res. 2007;67(20):10019–26.
Van Ginderachter JA, Meerschaut S, Liu Y, Brys L, De Groeve K, Hassanzadeh Ghassabeh G, et al. Peroxisome proliferator-activated receptor gamma (PPARgamma) ligands reverse CTL suppression by alternatively activated (M2) macrophages in cancer. Blood. 2006;108(2):525–35.
Farren MR, Carlson LM, Netherby CS, Lindner I, Li PK, Gabrilovich DI, et al. Tumor-induced STAT3 signaling in myeloid cells impairs dendritic cell generation by decreasing PKCβII abundance. Sci Signal. 2014;7(313):ra16.
Miossec P, Kolls JK. Targeting IL-17 and TH17 cells in chronic inflammation. Nat Rev Drug Discov. 2012;11(10):763–76.
Obermajer N, Wong JL, Edwards RP, Chen K, Scott M, Khader S, et al. Induction and stability of human Th17 cells require endogenous NOS2 and cGMP-dependent NO signaling. J Exp Med. 2013;210(7):1433–45.
Wu P, Wu D, Ni C, Ye J, Chen W, Hu G, et al. γδT17 cells promote the accumulation and expansion of myeloid-derived suppressor cells in human colorectal cancer. Immunity. 2014;40(5):785–800.
Xiang H, Ramil CP, Hai J, Zhang C, Wang H, Watkins AA, et al. Cancer-associated fibroblasts promote immunosuppression by inducing ROS-generating Monocytic MDSCs in lung squamous cell carcinoma. Cancer Immunol Res. 2020;8(4):436–50.
Niedermeier M, Reich B, Rodriguez Gomez M, Denzel A, Schmidbauer K, Göbel N, et al. CD4+ T cells control the differentiation of Gr1+ monocytes into fibrocytes. Proc Natl Acad Sci U S A. 2009;106(42):17892–7.
Shi Y, Ou L, Han S, Li M, Pena MM, Pena EA, et al. Deficiency of Kruppel-like factor KLF4 in myeloid-derived suppressor cells inhibits tumor pulmonary metastasis in mice accompanied by decreased fibrocytes. Oncogenesis. 2014;3(11):e129.
Zhang H, Maric I, DiPrima MJ, Khan J, Orentas RJ, Kaplan RN, et al. Fibrocytes represent a novel MDSC subset circulating in patients with metastatic cancer. Blood. 2013;122(7):1105–13.
Zoso A, Mazza EM, Bicciato S, Mandruzzato S, Bronte V, Serafini P, et al. Human fibrocytic myeloid-derived suppressor cells express IDO and promote tolerance via Treg-cell expansion. Eur J Immunol. 2014;44(11):3307–19.
Sawant A, Deshane J, Jules J, Lee CM, Harris BA, Feng X, et al. Myeloid-derived suppressor cells function as novel osteoclast progenitors enhancing bone loss in breast cancer. Cancer Res. 2013;73(2):672–82.
Tumino N, Weber G, Besi F, Del Bufalo F, Bertaina V, Paci P, et al. Polymorphonuclear myeloid-derived suppressor cells impair the anti-tumor efficacy of GD2.CAR T-cells in patients with neuroblastoma. J Hematol Oncol. 2021;14(1):191.
Park JA, Wang L, Cheung NV. Modulating tumor infiltrating myeloid cells to enhance bispecific antibody-driven T cell infiltration and anti-tumor response. J Hematol Oncol. 2021;14(1):142.
Liu Y, Zhou X, Wang X. Targeting the tumor microenvironment in B-cell lymphoma: challenges and opportunities. J Hematol Oncol. 2021;14(1):125.
Rivera Vargas T, Apetoh L. Can immunogenic chemotherapies relieve Cancer cell resistance to immune checkpoint inhibitors? Front Immunol. 2019;10:1181.
Vincent J, Mignot G, Chalmin F, Ladoire S, Bruchard M, Chevriaux A, et al. 5-fluorouracil selectively kills tumor-associated myeloid-derived suppressor cells resulting in enhanced T cell-dependent antitumor immunity. Cancer Res. 2010;70(8):3052–61.
Welters MJ, van der Sluis TC, van Meir H, Loof NM, van Ham VJ, van Duikeren S, et al. Vaccination during myeloid cell depletion by cancer chemotherapy fosters robust T cell responses. Sci Transl Med. 2016;8(334):334ra352.
Jen EY, Ko CW, Lee JE, Del Valle PL, Aydanian A, Jewell C, et al. FDA approval: Gemtuzumab Ozogamicin for the treatment of adults with newly diagnosed CD33-positive acute myeloid leukemia. Clin Cancer Res. 2018;24(14):3242–6.
Fu Z, Li S, Han S, Shi C, Zhang Y. Antibody drug conjugate: the “biological missile” for targeted cancer therapy. Signal Transduct Target Ther. 2022;7(1):93.
Cortes JE, de Lima M, Dombret H, Estey EH, Giralt SA, Montesinos P, et al. Prevention, recognition, and management of adverse events associated with gemtuzumab ozogamicin use in acute myeloid leukemia. J Hematol Oncol. 2020;13(1):137.
Candoni A, Papayannidis C, Martinelli G, Simeone E, Gottardi M, Iacobucci I, et al. Flai (fludarabine, cytarabine, idarubicin) plus low-dose Gemtuzumab Ozogamicin as induction therapy in CD33-positive AML: final results and long term outcome of a phase II multicenter clinical trial. Am J Hematol. 2018;93(5):655–63.
Lambert J, Pautas C, Terré C, Raffoux E, Turlure P, Caillot D, et al. Gemtuzumab ozogamicin for de novo acute myeloid leukemia: final efficacy and safety updates from the open-label, phase III ALFA-0701 trial. Haematologica. 2019;104(1):113–9.
Fultang L, Panetti S, Ng M, Collins P, Graef S, Rizkalla N, et al. MDSC targeting with Gemtuzumab ozogamicin restores T cell immunity and immunotherapy against cancers. EBioMed. 2019;47:235–46.
Kusmartsev S, Cheng F, Yu B, Nefedova Y, Sotomayor E, Lush R, et al. All-trans-retinoic acid eliminates immature myeloid cells from tumor-bearing mice and improves the effect of vaccination. Cancer Res. 2003;63(15):4441–9.
Kusmartsev S, Su Z, Heiser A, Dannull J, Eruslanov E, Kübler H, et al. Reversal of myeloid cell-mediated immunosuppression in patients with metastatic renal cell carcinoma. Clin Cancer Res. 2008;14(24):8270–8.
Lee JM, Seo JH, Kim YJ, Kim YS, Ko HJ, Kang CY. The restoration of myeloid-derived suppressor cells as functional antigen-presenting cells by NKT cell help and all-trans-retinoic acid treatment. Int J Cancer. 2012;131(3):741–51.
Bauer R, Udonta F, Wroblewski M, Ben-Batalla I, Santos IM, Taverna F, et al. Blockade of myeloid-derived suppressor cell expansion with all-trans retinoic acid increases the efficacy of antiangiogenic therapy. Cancer Res. 2018;78(12):3220–32.
Korman AJ, Garrett-Thomson SC, Lonberg N. The foundations of immune checkpoint blockade and the ipilimumab approval decennial. Nat Rev Drug Discov. 2022;21(7):509–28.
Sade-Feldman M, Kanterman J, Klieger Y, Ish-Shalom E, Olga M, Saragovi A, et al. Clinical significance of circulating CD33+CD11b+HLA-DR- myeloid cells in patients with stage IV melanoma treated with Ipilimumab. Clin Cancer Res. 2016;22(23):5661–72.
Tobin RP, Jordan KR, Robinson WA, Davis D, Borges VF, Gonzalez R, et al. Targeting myeloid-derived suppressor cells using all-trans retinoic acid in melanoma patients treated with Ipilimumab. Int Immunopharmacol. 2018;63:282–91.
Vollmer J, Krieg AM. Immunotherapeutic applications of CpG oligodeoxynucleotide TLR9 agonists. Adv Drug Deliv Rev. 2009;61(3):195–204.
Shirota Y, Shirota H, Klinman DM. Intratumoral injection of CpG oligonucleotides induces the differentiation and reduces the immunosuppressive activity of myeloid-derived suppressor cells. J Immunol. 2012;188(4):1592–9.
Zoglmeier C, Bauer H, Noerenberg D, Wedekind G, Bittner P, Sandholzer N, et al. CpG blocks immunosuppression by myeloid-derived suppressor cells in tumor-bearing mice. Clin Cancer Res. 2011;17(7):1765–75.
Zhao BG, Vasilakos JP, Tross D, Smirnov D, Klinman DM. Combination therapy targeting toll like receptors 7, 8 and 9 eliminates large established tumors. J Immunother Cancer. 2014;2:12.
Michels T, Shurin GV, Naiditch H, Sevko A, Umansky V, Shurin MR. Paclitaxel promotes differentiation of myeloid-derived suppressor cells into dendritic cells in vitro in a TLR4-independent manner. J Immunotoxicol. 2012;9(3):292–300.
Yu SJ, Ma C, Heinrich B, Brown ZJ, Sandhu M, Zhang Q, et al. Targeting the crosstalk between cytokine-induced killer cells and myeloid-derived suppressor cells in hepatocellular carcinoma. J Hepatol. 2019;70(3):449–57.
Serafini P, Meckel K, Kelso M, Noonan K, Califano J, Koch W, et al. Phosphodiesterase-5 inhibition augments endogenous antitumor immunity by reducing myeloid-derived suppressor cell function. J Exp Med. 2006;203(12):2691–702.
Meyer C, Sevko A, Ramacher M, Bazhin AV, Falk CS, Osen W, et al. Chronic inflammation promotes myeloid-derived suppressor cell activation blocking antitumor immunity in transgenic mouse melanoma model. Proc Natl Acad Sci U S A. 2011;108(41):17111–6.
Califano JA, Khan Z, Noonan KA, Rudraraju L, Zhang Z, Wang H, et al. Tadalafil augments tumor specific immunity in patients with head and neck squamous cell carcinoma. Clin Cancer Res. 2015;21(1):30–8.
Weed DT, Vella JL, Reis IM, De la Fuente AC, Gomez C, Sargi Z, et al. Tadalafil reduces myeloid-derived suppressor cells and regulatory T cells and promotes tumor immunity in patients with head and neck squamous cell carcinoma. Clin Cancer Res. 2015;21(1):39–48.
Hassel JC, Jiang H, Bender C, Winkler J, Sevko A, Shevchenko I, et al. Tadalafil has biologic activity in human melanoma. Results of a pilot trial with Tadalafil in patients with metastatic melanoma (TaMe). Oncoimmunology. 2017;6(9):e1326440.
Shakespear MR, Halili MA, Irvine KM, Fairlie DP, Sweet MJ. Histone deacetylases as regulators of inflammation and immunity. Trends Immunol. 2011;32(7):335–43.
Cui Y, Cai J, Wang W, Wang S. Regulatory effects of histone deacetylase inhibitors on myeloid-derived suppressor cells. Front Immunol. 2021;12:690207.
Tomita Y, Lee MJ, Lee S, Tomita S, Chumsri S, Cruickshank S, et al. The interplay of epigenetic therapy and immunity in locally recurrent or metastatic estrogen receptor-positive breast cancer: correlative analysis of ENCORE 301, a randomized, placebo-controlled phase II trial of exemestane with or without entinostat. Oncoimmunology. 2016;5(11):e1219008.
Kim K, Skora AD, Li Z, Liu Q, Tam AJ, Blosser RL, et al. Eradication of metastatic mouse cancers resistant to immune checkpoint blockade by suppression of myeloid-derived cells. Proc Natl Acad Sci U S A. 2014;111(32):11774–9.
Orillion A, Hashimoto A, Damayanti N, Shen L, Adelaiye-Ogala R, Arisa S, et al. Entinostat neutralizes myeloid-derived suppressor cells and enhances the antitumor effect of PD-1 inhibition in murine models of lung and renal cell carcinoma. Clin Cancer Res. 2017;23(17):5187–201.
Christmas BJ, Rafie CI, Hopkins AC, Scott BA, Ma HS, Cruz KA, et al. Entinostat converts immune-resistant breast and pancreatic cancers into checkpoint-responsive tumors by reprogramming tumor-infiltrating MDSCs. Cancer Immunol Res. 2018;6(12):1561–77.
Fujita M, Kohanbash G, Fellows-Mayle W, Hamilton RL, Komohara Y, Decker SA, et al. COX-2 blockade suppresses gliomagenesis by inhibiting myeloid-derived suppressor cells. Cancer Res. 2011;71(7):2664–74.
Steggerda SM, Bennett MK, Chen J, Emberley E, Huang T, Janes JR, et al. Inhibition of arginase by CB-1158 blocks myeloid cell-mediated immune suppression in the tumor microenvironment. J Immunother Cancer. 2017;5(1):101.
Holmgaard RB, Zamarin D, Li Y, Gasmi B, Munn DH, Allison JP, et al. Tumor-expressed IDO recruits and activates MDSCs in a Treg-dependent manner. Cell Rep. 2015;13(2):412–24.
Shastri A, Choudhary G, Teixeira M, Gordon-Mitchell S, Ramachandra N, Bernard L, et al. Antisense STAT3 inhibitor decreases viability of myelodysplastic and leukemic stem cells. J Clin Invest. 2018;128(12):5479–88.
Hong D, Kurzrock R, Kim Y, Woessner R, Younes A, Nemunaitis J, et al. AZD9150, a next-generation antisense oligonucleotide inhibitor of STAT3 with early evidence of clinical activity in lymphoma and lung cancer. Sci Transl Med. 2015;7(314):314ra185.
Proia TA, Singh M, Woessner R, Carnevalli L, Bommakanti G, Magiera L, et al. STAT3 antisense oligonucleotide remodels the suppressive tumor microenvironment to enhance immune activation in combination with anti-PD-L1. Clin Cancer Res. 2020;26(23):6335–49.
Ko JS, Zea AH, Rini BI, Ireland JL, Elson P, Cohen P, et al. Sunitinib mediates reversal of myeloid-derived suppressor cell accumulation in renal cell carcinoma patients. Clin Cancer Res. 2009;15(6):2148–57.
Chen HM, Ma G, Gildener-Leapman N, Eisenstein S, Coakley BA, Ozao J, et al. Myeloid-derived suppressor cells as an immune parameter in patients with concurrent Sunitinib and stereotactic body radiotherapy. Clin Cancer Res. 2015;21(18):4073–85.
Nagarsheth N, Wicha MS, Zou W. Chemokines in the cancer microenvironment and their relevance in cancer immunotherapy. Nat Rev Immunol. 2017;17(9):559–72.
Ozga AJ, Chow MT, Luster AD. Chemokines and the immune response to cancer. Immunity. 2021;54(5):859–74.
Chang AL, Miska J, Wainwright DA, Dey M, Rivetta CV, Yu D, et al. CCL2 produced by the glioma microenvironment is essential for the recruitment of regulatory T cells and myeloid-derived suppressor cells. Cancer Res. 2016;76(19):5671–82.
Highfill SL, Cui Y, Giles AJ, Smith JP, Zhang H, Morse E, et al. Disruption of CXCR2-mediated MDSC tumor trafficking enhances anti-PD1 efficacy. Sci Transl Med. 2014;6(237):237ra267.
Flores-Toro JA, Luo D, Gopinath A, Sarkisian MR, Campbell JJ, Charo IF, et al. CCR2 inhibition reduces tumor myeloid cells and unmasks a checkpoint inhibitor effect to slow progression of resistant murine gliomas. Proc Natl Acad Sci U S A. 2020;117(2):1129–38.
D'Alterio C, Buoncervello M, Ieranò C, Napolitano M, Portella L, Rea G, et al. Targeting CXCR4 potentiates anti-PD-1 efficacy modifying the tumor microenvironment and inhibiting neoplastic PD-1. J Exp Clin Cancer Res. 2019;38(1):432.
Bockorny B, Semenisty V, Macarulla T, Borazanci E, Wolpin BM, Stemmer SM, et al. BL-8040, a CXCR4 antagonist, in combination with pembrolizumab and chemotherapy for pancreatic cancer: the COMBAT trial. Nat Med. 2020;26(6):878–85.
Hegde S, Leader AM, Merad M. MDSC: markers, development, states, and unaddressed complexity. Immunity. 2021;54(5):875–84.
Halaby MJ, Hezaveh K, Lamorte S, Ciudad MT, Kloetgen A, MacLeod BL, et al. GCN2 drives macrophage and MDSC function and immunosuppression in the tumor microenvironment. Sci Immunol. 2019;4(42):eaax8189. https://doi.org/10.1126/sciimmunol.aax8189.
Alshetaiwi H, Pervolarakis N, McIntyre LL, Ma D, Nguyen Q, Rath JA, et al. Defining the emergence of myeloid-derived suppressor cells in breast cancer using single-cell transcriptomics. Sci Immunol. 2020;5(44):eaay6017. https://doi.org/10.1126/sciimmunol.aay6017.
Cuenca M, Sintes J, Lányi Á, Engel P. CD84 cell surface signaling molecule: an emerging biomarker and target for cancer and autoimmune disorders. Clin Immunol. 2019;204:43–9.
Witherden DA, Verdino P, Rieder SE, Garijo O, Mills RE, Teyton L, et al. The junctional adhesion molecule JAML is a costimulatory receptor for epithelial gammadelta T cell activation. Science. 2010;329(5996):1205–10.
Ziegenhain C, Vieth B, Parekh S, Reinius B, Guillaumet-Adkins A, Smets M, et al. Comparative analysis of single-cell RNA sequencing methods. Mol Cell. 2017;65(4):631–643.e634.
Lei Y, Tang R, Xu J, Wang W, Zhang B, Liu J, et al. Applications of single-cell sequencing in cancer research: progress and perspectives. J Hematol Oncol. 2021;14(1):91.
Guo R, Lü M, Cao F, Wu G, Gao F, Pang H, et al. Single-cell map of diverse immune phenotypes in the acute myeloid leukemia microenvironment. Biomark Res. 2021;9(1):15.
Fu T, Dai LJ, Wu SY, Xiao Y, Ma D, Jiang YZ, et al. Spatial architecture of the immune microenvironment orchestrates tumor immunity and therapeutic response. J Hematol Oncol. 2021;14(1):98.
Li MO, Wolf N, Raulet DH, Akkari L, Pittet MJ, Rodriguez PC, et al. Innate immune cells in the tumor microenvironment. Cancer Cell. 2021;39(6):725–9.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Natural Science Foundation of China (No.82272794, 82073370, 81874120).
Author information
Authors and Affiliations
Contributions
YW drafted the manuscript and prepared the figs. MY and MN helped in collecting the related literatures and participated in discussion. KW and QM designed the review and revised the manuscript. All authors contributed to the article and approved the submitted version. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, Y., Yi, M., Niu, M. et al. Myeloid-derived suppressor cells: an emerging target for anticancer immunotherapy. Mol Cancer 21, 184 (2022). https://doi.org/10.1186/s12943-022-01657-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12943-022-01657-y