
Abstract
Background
Increasing evidence associates air pollution with thyroid dysfunction, whereas the potential relationship between exposure to ozone (O3) and Thyroid Nodules (TNs) is unclear.
Methods
This retrospective cohort study investigated the association between O3 exposure and TNs in Hunan province, enrolling 191,357 Chinese adults who lived in Hunan province from January 2009 to December 2019 and received voluntary medical examinations. Individual exposure levels to O3 from 2010 to 2019 were measured on account of participants’ residential addresses at the district level. Associations of O3 exposure with the risk of incidental TNs were assessed by restricted cubic splines and surveyed as odds ratios after adjusting for demographic factors.
Results
In total, 81,900 adults were newly diagnosed with TNs during the study period. Age-standardized TNs detection rate in Hunan province increased from 25.9 to 46.3% between 2010 and 2019, with the greatest annual percent change being 8.1 [95% CI, 7.3–8.8]. A similar trend has been found in all tumor sizes, ages, and both sexes. O3 exposure presented a statistically significant dose-dependent positive correlation (greater than 0.036 ppm) with TNs. Similarly, long-term exposure to high levels of O3 (1-year average O3 concentrations exceeding 0.0417 ppm) was found positively associated with increased TSH levels.
Conclusions
High-level O3 exposure in the long term was associated with an increase in TSH. Consequently, increased TSH was related to the increased risk of TNs. Being exposed to high-level O3 in the long term was related to the increased detection rates of TNs in Hunan province, which could be mediated by TSH.
Similar content being viewed by others


Background
Thyroid Nodules (TNs) present to be a kind of common clinical manifestation, occurring in 5% of the population, of which 7–15% turn out to be thyroid cancer [1]. In the United States, the morbidity of differentiated thyroid cancer tripled during the past 30 years [2]. Incremental evidence implicates so steady an increase that cannot be entirely ascribed to more sensitive diagnostic procedures and more intensive thyroid nodule screening [3], yet the reasons for the rapid increase of TNs remain elusive. Several environmental factors which show reliable candidates to stand for this increase have been observed, including improved iodine intake [4], exposure to various toxic compounds [5], nutritional deficiencies [6], eating habits, and comorbidities [7]. It has been reported that increased thyroid-stimulating hormone (TSH) or elevation within the normal range is relevant to an increased risk of malignancy in TNs [8]. Iodine deficiency, through regulating TSH levels, is a recognized risk factor for various thyroid diseases including TNs [4]. However, the fact that salt has been iodized all over China since 1996 has not stopped the incidence of thyroid cancer from markedly ascending, even in regions (including Hunan Province) with enough iodine intake [9, 10].
Air pollution is an unneglectable public health hazard [11]. Exposure to air pollutants, such as particulate matter (PM), Ozone (O3), nitrogen dioxide (NO2), and sulfur dioxide (SO2), has been proven to be related to public health and daily mortality worldwide [11, 12]. O3 is formed in the atmosphere through photochemical reactions, which lead to the action of ultraviolet light on precursor pollutants. A large body of literature links short-term O3 exposure to a wide range of cardiovascular diseases [13] and dry eye disease [14] but the relationship between long-term O3 exposure and some conditions is still poorly understood. Increasing evidence associates air pollution with thyroid dysfunction. Recent research has inspected the relationship between exposure to environmental and traffic-related air pollution and the thyroid function of pregnant women, which implied a strong link between ambient air pollution and thyroid dysfunction, both in pregnant women and newborns [15, 16]. Moreover, evidence indicates that short-term O3 exposure gives rise to a crucial decrease in circulating thyroid hormones and TSH in rats [17], as well as the threshold of goiter in several species of sharks [18]. Nevertheless, the correlation between ambient exposure to O3 and TNs has not been defined.
We hypothesized that high exposure to O3 is in connection with increased incidence of TNs and that abnormal thyroid function induced by O3 exposure may mediate and strengthen that association. To identify the associations between ambient exposure to O3 and TNs, we retrospectively analyzed 10 years of ambient O3 exposure in Hunan province as well as the age-adjusted TNs detection rate in 191,357 adults during the same period. We also examined and matched some risk factors for TNs, such as age, sex, BMI, triglycerides (TG), and total cholesterol (TC), which largely controlled potential confounding sociodemographic, behavioral, and clinical factors. This large sample study spanning ten years provides good insight into the effects of ambient O3 exposure on TNs.
Methods
Study population and data collection
We retrospectively collected voluntary medical examination records in the Health Management Center of Xiangya Hospital Central South University from January 2010 to December 2019. Xiangya Hospital Central South University is a top-ranked hospital with a good reputation in South-Central China, receiving patients from the whole Hunan province. Hunan Province is an area with rapid economic development, far from the ocean but with adequate iodine nutrition in South-Central China. We also obtained the measurement data of each air pollutant in every district.
This study was permitted by the Expert Committee of Xiangya Hospital Central South University in China (equivalent to an Institutional Review Board) and complied with the tenets of the Declaration of Helsinki. In this 10-year large research cohort, we recruited those (1) older than 18 years, (2) who were long-term residents (working and living more than 10 months per year) in Hunan province from January 2009 to December 2019, (3) who received voluntary medical examination including thyroid ultrasonography, (4) without a history of thyroid surgery or radiotherapy, (5) with no major chronic diseases as self-reported, (6) who had completed a questionnaire including demographic data and residential addresses before the physical examination.
TNs were diagnosed with high-resolution ultrasound and thyroid function was measured via serum concentrations of free T4, T3, and TSH. In the cases of repeated examinations, we used the last records for research. For those who were found with TNs in multiple physical examinations, we chose the first records with TNs diagnosis for research. Eventually, we analyzed the medical records of 191,357 subjects from 429,909 Chinese adults in the database. The flowchart for exclusion and analysis is shown in Fig. 1.

The flowchart for exclusion and analysis
The residence location of a participant was determined by the questionnaire. Residential locations were described in detail to a district of the city and even the neighborhoods within the district. Thyroid nodule screening has become a routine item of physical examination, with low cost and comprehensive coverage of urban and rural areas.
Air pollution exposures
Ambient air quality monitoring data from the China Air Quality Online Monitoring and Analysis Platform (https://www.aqistudy.cn/historydata/index.php) was used in this study. We downloaded O3 data (measured in ppm, parts per million) from 70 national ambient air quality monitoring stations in Hunan province. The distribution of national ambient air quality monitoring stations in each prefecture-level city is evenly covered. The district-level data used in our analysis is the average value obtained from actual measurements at each monitoring point in a given district.
Covariates
Participants were asked to fill in questionnaires to provide basic information before the medical examination, including gender, age, height, weight, residential address, and chronic diseases. Because Thyroid nodule is a multifactorial disease, we regarded reported risk factors as covariates, including demographic factors (gender, age, regions) and obesity. Body mass index (BMI) was calculated as the weight in kilograms divided by the square of the height in meters (kg/m2). Overweight was defined as BMI ≥25 kg/m2 according to the World Health Organization (WHO-BMI) definition. Previous studies showed that thyroid function was significantly associated with dyslipidemia and seasonal changes [19, 20]. Therefore, we added TC, TG, and season as covariates when TSH was analyzed in the restricted cubic splines.
Statistical analysis
This study applied R software (R 4.0.2) for data analysis, mainly using rms, ggplot2, and segmented packages. All tests were two-sided and P-values less than 0.05 deemed the corresponding result significant. For statistical description and comparison in the basic information, count data were indicated as frequencies (percentages), and the chi-square test was used for comparison between groups; those with normal distribution in the measurement data were indicated as mean (standard deviation, SD), and the student’s t-test was used for comparison between groups; those with non-normal distribution in the measurement data were indicated as median (interquartile range, IQR), and the Mann-Whitney U test was used for comparison among groups.
The crude detection rates of TNs were calculated in each stratum by age group (18–29, 30–39, 40–49, 50–59, 60–69, 70+ years old) and sex. Age-standardized rates by standard population were calculated using the age composition of the Hunan Province population according to the 6th census data released by the National Bureau of statistics. Mann-Kendall Trend Test was used to assess the changes in time series trends. We used the Joinpoint Regression Program (Version 4.9.0.0. March 2021; Statistical Research and Applications Branch, National Cancer Institute.) to get the APC (annual percent change) and AAPC (average annual percent change). Formulae are as shown (in 1–4). We employed a log-linear model {ln(y) = β0 + β1x} where y represents incidence, x represents the year of onset, and β1 is the regression coefficient. α is the statistical significance level (0.05). APCL(α) and APCU(α) are the lower and upper limit of the (1-α) confidence interval. d is the degree of freedom; s is the standard error of the regression coefficient (β1); td− 1 (1-α/2) is the q percentile of the t distribution with the degree of freedom of d; wi is the interval span width of each piecewise function (Number of years), and βi is the regression coefficient corresponding to each interval.
Based on the age-standardized rates and the O3 exposure data, a geostatistical map was made to visually show the relationship between the geographical distribution of TNs detection rates and the annual mean ozone concentration of each prefecture. Spatial distribution of the annual age-standardized detection rate of TNs and average O3 concentration for each prefectural city were generated by ArcGIS 10.2 (http://www.esri.com/arcgis/about-arcgis). To further confirm this relationship, we detected this link through Spearman correlation by rank, excluding the outliers.
To evaluate the exposure-response relationship between O3 exposure and TNs detection rate, each case was matched with the O3 exposure concentration at the corresponding time and location. A total of 191,357 cases were included after excluding patients without matched O3 concentration data. The restricted cubic spline function fitted for Logistic Regression Model (R package rms) was employed, with age, gender, BMI, and prefecture controlled as confounding factors. The degree of freedom (df) was selected by evaluating the model fit according to the Akaike Information Criterion (AIC), and the preferred number of knots was 5, all equally spaced. The lowest point of exposure-response (O3 = 0.036 ppm) was used as the reference point (i.e., OR = 1) to plot the relationship curve between O3 and the OR of suffering from TNs. Furthermore, we used the same method to perform a 2-year O3 concentration analysis.
Similarly, each case was matched to the O3 exposure concentration at the corresponding time (1-month, 6-month, and 12-month) and location to explore the correlation between O3 exposure levels and TSH levels. Cases without thyroid function test results or unmatched O3 concentration data were excluded from the analysis. 39,353 valid data cases were included in the TSH and 1-month O3 exposure relationship analysis. The relationships between 1-month, 6-month, and 12-month average O3 exposure concentrations and TSH levels were also studied using restricted cubic spline functions fitted for generalized linear models based on Gaussian distribution, with gender, age, BMI, cholesterol, triglycerides, and season adjusted as confounders. The preferred number of equally spaced nodes of 3 was selected according to AIC. Subgroup analysis was performed by gender. Finally, the fitted curves were plotted. From the exposure-response curve, O3 concentrations (O3 = 0.0365 ppm, 0.0445 ppm, 0.0417 ppm) corresponding to the extreme points were obtained by iterating the generalized linear models in 0.0001-unit increments.
The relationship between thyroid function and TNs is already well established [4] and to verify this correlation, we compared the status of thyroid function (based on TSH, free T4 (FT4), and free T3 (FT3) levels) between the TN group and a control group. 39,353 adults were tested for thyroid function.
Finally, to further test the hypothesis, we also analyzed the relationship between O3 exposure, TNs, and TSH levels. The threshold was obtained from the curve of 1-year average O3 exposure and TNs. According to the threshold, the cases were divided into two groups (higher O3 group and lower O3 group). On the other hand, we obtained the TSH cut-off value by the ROC curve of TSH-TNs, determined by the largest Youden index. Similarly, we performed a TSH dichotomy (higher TSH group and lower TSH group). The Mann-Whitney U test and the Chi-Square test were applied to examine the continuous variables and the dichotomous variables of TSH in the higher O3 group, respectively. Further, the mediation analysis was performed by Model 4 of PROCESS (Version 4.1, Written by Andrew F. Hayes). The model included ozone exposure as an independent variable, thyroid nodules as a dependent variable, and TSH as a mediating variable, adjusted by sex, age, and BMI. We selected 5000 as the number of bootstrap samples for percentile bootstrap confidence intervals. Direct and indirect effects of ozone on TNs are on a log-odds metric.
Results
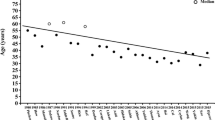
The baseline characteristics of the study participants are shown in Table 1 and supplemental Table 1. The mean (interquartile range, IQR) age of the participants (95,316 men and 96,041 women) was 44 (34–53) years old. The mean (IQR) levels of TG, O3 (1-year average exposure), and O3 (2-year average exposure) during the study period were 1.32 (0.93–1.99) mmol/L, 0.0408 (0.0392–0.0418) ppm, and 0.0410 (0.0390–0.0415) ppm, respectively. The mean (SD) levels of BMI and TC were 23.60 (3.34) and 5.08 (1.02) mmol/L. The detection rate of newly diagnosed TNs was 42.8% (81,900/191357) and was significantly related to age, sex, BMI, overweight, TG, TC, and the exposure level of O3 (P < 0.001). TNs were more likely to occur in adults of older age, female sex, who had higher BMI, TG or TC levels, and higher levels of O3 exposure.
From 2010 to 2019, the age-standardized TNs detection rate in Hunan province significantly increased (from 25.9 to 46.3%, APC, 8.1 [95% CI, 7.3–8.8]; P < 0.001), with small nodule (≤1 cm, APC, 10.0 [95% CI, 8.2–11.9]; P < 0.001), male (APC, 9.8 [95% CI, 9.0–10.6]; P < 0.001) and youth (< 50 years, AAPC, 8.9 [95% CI, 5.2–12.8]; P < 0.001) preponderance. In addition, detection rates of TNs significantly rose in all tumor sizes, ages, and both sexes (Fig. 2, Supplemental Tables 2–4, and Supplemental Figs. 1–4).

Trends in TNs Detection Rates, Stratified by Tumor Size, Age and Sex, 2010–2019
The grade distribution map showed that the yearly age-standardized detection rates of TNs of seven prefectural cities in Hunan province show a thyroid nodule detection rate of more than 40% (including Changde, Yueyang, Changsha, Loudi, Xiangtan, Shaoyang, Yongzhou), accounting for 50% of the total number of prefectural cities (Fig. 3). In addition, there is a spatial agglomeration of ambient O3 exposure in Hunan province according to the decade annual mean O3 concentration map, and the areas with the most severe pollution (O3 concentration of more than 0.412 ppm), such as Yueyang, Yiyang, Changde, Changsha, and Loudi are concentrated in the north-central areas of Hunan province, (Fig. 3B). The areas with high detection rates of TNs approximately overlap with the geographic regions where ozone exposure pollution is most severe. When all cities were included, the confirmatory ranking test revealed no significant connection (rs = 0.209, P = 0.494). Nonetheless, when Yongzhou, Yiyang, and Xiangtan were eliminated as outliers, annual mean ozone concentrations of cities were significantly positively connected with TN detection rates (rs = 0.64, P = 0.048). In other words, the TNs detection rates were closely related to the exposure levels of O3.

Spatial distribution of annual standardized detection rate of TNs and average O3 concentration for each prefectural city in Hunan province in Hunan province from 2010 to 2019
Further analysis of the relationship between O3 exposure and TNs showed that the ORs for incident TNs based on O3 exposure exhibited a statistically significant dose-dependent elevation (when the O3 levels were greater than 0.036 ppm), and the association remained robust even after adjusting for age, sex, BMI, and location (Fig. 4B). It should be noted that the absolute OR value was greater than 1, when O3 exposure concentration was greater than 0.0408 ppm, suggesting that O3 could be a risk factor for TNs.

Multivariable Regression Models for TSH Level and TNs with Restricted Cubic Splines
We observed a negative correlation between decreased TSH levels and short-term exposure to O3, such as 1-month average O3 concentrations exceeding 0.0365 ppm before diagnosis or 6-month average O3 concentrations exceeding 0.0445 ppm (supplemental Fig. 5A, B). Nonetheless, 1-year average O3 concentrations exceeding 0.0417 ppm were found positively associated with increased TSH levels (Fig. 4A). Accordingly, exposure to O3 in the long term was associated with an increase in TSH levels.
Of the 39,353 adults that were tested for thyroid function, 17,265 were diagnosed with TNs, and 22,088 were not. The results of our verification of the correlation between thyroid function and TNs showed that, although the results of almost all the thyroid functions were within the normal range, the mean (IQR) levels of TSH in individuals with TNs were prominently higher than in those without TNs (P = 0.007, 2.21 (1.47–3.3) vs. 2.19 (1.49–3.16)), and the mean (IQR) levels of FT3 levels in adults with TNs were observably lower than in those without TNs (P < 0.001, 4.52 (4.10–5.00) vs. 4.65 (4.18–5.15)), but no significant difference was found in FT4 levels between the two groups (Supplemental Table 1).
Further analyses of the relationship between O3 exposure, TSH level, and TNs are fully shown in Table 2. The TSH cut-off value was 3.2 mIU/L, obtained from the ROC curve of TSH-TNs. Based on the threshold values of O3 and TSH, all 191,357 Chinese adults were divided into two groups, respectively. The detection rates of TNs were significantly higher in the higher O3 group (P < 0.001) and the higher TSH group (P < 0.001). Meanwhile, TSH levels of adults with TNs were prominently higher than those without TNs in the higher O3 group (P = 0.006, 2.21 (1.47–3.3) vs. 2.18 (1.48–3.14)), which did not exist in the lower O3 group (P = 0.245). In the higher O3 group, the TNs detection rate of the higher TSH group was significantly higher than that of the lower TSH group (P < 0.001). The mediation analysis showed that the direct effect of ozone exposure on the dependent variable TN was 42.078 (33.516–50.639), accounting for 99.35% of the total effect. The indirect effect of ozone exposure on TNs through TSH level was 0.277 (0.0424–0.656), accounting for 0.65% of the total effect.
Discussion
Employing a cohort study, we examined the relationship between a time-varying 10-year mean O3 exposure and incidental TNs in Hunan province, an area with rapid economic development and adequate iodine nutrition in South-Central China. We found a statistically significant increase in TNs detection rates, which may be attributed to long-term, high-level O3 exposure mediated by TSH.
In recent decades, the prevalence of thyroid nodules (TNs) has steadily increased [21]. As people’s living standards have improved as a result of rapid economic growth, it has become easier for them to obtain medical examinations, thereby increasing the detection rate of TNs; more sensitive diagnostic procedures also have increased the detection of TNs by allowing the detection of smaller nodules [3]. However, incremental evidence implicates so steady an increase that cannot be entirely ascribed to more intensive thyroid nodule screening and more sensitive diagnostic procedures [3]. Several environmental factors which could lead to the increase have been observed, including iodine intake [4], toxic compounds [22], nutrition [6], obesity [23], and so on. Iodine is a trace element required for thyroid hormone synthesis and is an essential component of the thyroid cells’ functional microenvironment. Both iodine deficiency and excessive iodine may result in thyroid diseases such as thyroid nodules, hypothyroidism, and autoimmune diseases [4, 24,25,26]. As a country suffering from mild to moderate iodine deficiency, China implemented Universal Salt Iodization (USI) in 1996. By 2010, 28 provinces (including Hunan Province) had realized the goal of eliminating iodine-deficient disorders [27]. During the two decades of USI, the Chinese population has been consecutively exposed to three different stages of iodine nutritional status: excessive iodine intake (median urine iodine concentration, UIC ≥300 μg/L) from 1996 to 2001, more than adequate iodine intake (median UIC 200–299 μg/L) from 2002 to 2011, and adequate iodine intake (median UIC 100–199 μg/L) from 2012 to 2016 [27]. Iodine prophylaxis has played a key role in alleviating goiter and other iodine deficiency disorders and modulated the composition of thyroid disease [27]. It was reported that excessive iodine intake is positively associated with the risk of TNs [25, 26]. From the perspective of iodine nutrition level, excessive iodine intake may not be enough to explain the increase in TNs incidence, considering that the province’s iodine nutrition was not in an excessive iodine intake state during the period of this study. In our study, we found that long-term exposure to high levels of O3 would increase the risk of TNs.
To our knowledge, the present study is the first one investigating the correlation between the risk of incidental TNs and O3 concentration, which ultimately revealed an association between those two. Well-established evidence implied higher serum TSH concentrations would increase the likelihood of TNs and thyroid cancer [4]. Previously, four observational studies [15, 16, 28, 29] had particularly examined the relevance between air pollutants and thyroid function alteration of pregnant women and their newborns, which unveiled that PM2.5 and PM10 but not O3 were associated with the abnormal thyroid function, yet those results only explored the association at a short-term level. Of note, our findings confirmed that the relationship between O3 exposure and TSH level alteration was time-varying, namely short-term O3 exposure (1-month or 6-month) at high concentrations leads to the decline of TSH levels. In contrast, long-term exposure (1-year) to high levels of O3 leads to a rise in TSH levels. To date, the relationship between short-term O3 exposure and thyroid function has been presented in several studies [17, 30,31,32,33]. Consistent with our study, short-term O3 exposure has been associated with decreases in circulating TSH [17, 30,31,32,33]. Short-term O3 exposure was found to result in a remarkable reduction of circulating thyroid hormones and TSH in rats, which was interpreted as a possible adaptive mechanism to enhance the survival of rats during ozone exposure [17]. Huffman has observed the exacerbation of ozone effects in animals with hyperthyroidism [32]. Short-term O3 exposure has been reported to increase the levels of adrenal-derived circulating stress hormones and markedly decrease circulating TSH levels, indicating that short-term ozone exposure may function through the neuroendocrine axis, mediated by activation of central stress-response mechanisms [30, 34]. What’s more, this study was the first to establish the change of TSH through long-term O3 exposure (1-year) at high engagement. Perhaps, long-term ozone exposure induces thyroid inflammation, in which thyroid cells are destroyed. High TSH levels are required to promote the destruction-repair cycle of thyroid follicular epithelium cells to maintain thyroid homeostasis.
We agree with previous reports that increased TSH or elevation within the normal range is related to an increased risk of TNs. Our results show that long-term high ozone exposure is not only associated with elevated TSH but is also positively associated with thyroid nodule risk and this may be explained by higher serum TSH concentrations favoring the likelihood of TNs. The mediation analysis, together with the results of subgroup analyses, supports the idea that high ozone exposure, may play at least a partial role in thyroid nodule risk with TSH as a mediator. Considering these observations with our findings, we hypothesize that abnormal thyroid function can mediate the association between ozone exposure and TN incidence. However, multi-center studies and in-depth mechanistic research are required to confirm this.
Though our survey results revealed a long-term correlation between O3 exposure and TNs, the mechanism of that is still far from being fully understood and awaits further investigation. Hypothetically, the reaction of oxidative stress and remodeling of the microenvironment are tending to be the potential mechanisms since autoimmune processes may work on thyroid function for a more extended period [35]. Meanwhile, growing incidence implied that elevated TSH levels and thyroid autoimmunity were summarized as independent risk factors for thyroid cancer [36]. Such mechanisms have been identified in the pathological development of Hashimoto’s thyroiditis, which involved a shift from hyperthyroidism to hypothyroidism [37, 38]. Moreover, Hashimoto’s thyroiditis is an independent risk factor for incidental thyroid cancer [27].
Another explanation may lay in the long-term O3 exposure-induced Oxidative DNA damage. It is well-proven that the reactive oxygen species (ROS) that evade cellular defenses result in permanent or temporary damage to lipids, proteins, and nucleic acids [39]. Potassium bromate is a by-product of ozonation of high-bromide surface water to produce drinking water, as well as a rodent carcinogen that can produce tumors, including thyroid cancer [40, 41]. It has been established that potassium bromate renal carcinogenesis involves premutagenic base damage in DNA specially removed by base excision repair [42]. More direct evidence of the fact is a report describing the outbreak of goiter in a few species of sharks following the addition of ozone to a touch pool [18]. Four brown-banded bamboo sharks (Chiloscyllium punctatum) and 11 white-spotted bamboo sharks (Chiloscyllium plagiosum) housed in an aquarium with a high-level O3 exposure were diagnosed with hypothyroidism and multinodular goiter [18]. Yet, there is a lack of evidence that the development of TNs requires a latency period following exposure to O3, and further research is needed to access the optimal time lag between O3 exposure and the development of TNs.
As far as we know, our study is the first to explore the association between ozone exposure and thyroid nodules, and the first to verify the association between long-term ozone exposure and TSH, with a sufficiently large sample size but it inevitably has some limitations. The most obvious limitation is that the assessment of ozone exposure was not very accurate due to limited monitoring sites and the inability to apply a hybrid geophysical-statistical model. Due to some special factors, we can only obtain limited data from the public data of monitoring stations which may be clustered. In addition, the results of this study only partially reflect the detection rate of TNs in different regions of Hunan Province since the analysis depended on voluntary examination records and did not account for those who did not participate. We did not include diet (iodine intake) as a covariate in our analysis due to the lack of detailed data, instead, we assumed that iodine intake levels are balanced between groups since the iodine nutritional status of the Chinese population, in the period of this study, was almost in an adequate iodine intake state. Also, as the shapes of cities in Hunan province, such as Yiyang and Huaihua city, are irregular, even long and narrow, they may be closer to monitoring stations in nearby cities, creating the potential of producing inaccurate data.
Conclusions
High-level O3 exposure in the long term was associated with an increase in TSH. Consequently, increased TSH was related to the increased risk of TNs. Being exposed to high-level O3 in the long term was related to the increased detection rates of TNs in Hunan province, which could be mediated by TSH.
Abbreviations
- TNs:
-
Thyroid Nodules
- O3 :
-
Ozone
- TSH:
-
Thyroid-stimulating hormone
- PM:
-
Particulate matter
- NO2 :
-
Nitrogen dioxide
- SO2:
-
Sulfur dioxide
- TG:
-
Triglycerides
- TC:
-
Total cholesterol
- BMI:
-
Body mass index
- WHO:
-
World Health Organization
- SD:
-
Standard deviation
- IQR:
-
Interquartile range
- FT4:
-
Free thyroxine
- FT3:
-
Free triiodothyronine
- APC:
-
Annual percentage Change
- AAPC:
-
Average annual percentage change
- AIC:
-
Akaike information criterion
- ppm:
-
Parts per million
- ROS:
-
Reactive oxygen species
References
Burman KD, Wartofsky L. Clinical practice. Thyroid nodules. N Engl J Med. 2015;373(24):2347–56.
Lim H, Devesa SS, Sosa JA, Check D, Kitahara CM. Trends in thyroid cancer incidence and mortality in the United States, 1974-2013. JAMA. 2017;317(13):1338–48.
Wiltshire JJ, Drake TM, Uttley L, Balasubramanian SP. Systematic review of trends in the incidence rates of thyroid cancer. Thyroid. 2016;26(11):1541–52.
Laurberg P, Cerqueira C, Ovesen L, Rasmussen LB, Perrild H, Andersen S, et al. Iodine intake as a determinant of thyroid disorders in populations. Best Pract Res Clin Endocrinol Metab. 2010;24(1):13–27.
Zamora-Ros R, Cayssials V, Franceschi S, Kyro C, Weiderpass E, Hennings J, et al. Polyphenol intake and differentiated thyroid cancer risk in the European prospective investigation into cancer and nutrition (EPIC) cohort. Int J Cancer. 2020;146(7):1841–50.
Sangsefidi ZS, Ghafouri-Taleghani F, Zakavi SR, Norouzy A, Kashanifar R, Pourbaferani R, et al. Major dietary patterns and differentiated thyroid cancer. Clin Nutr ESPEN. 2019;33:195–201.
Barrea L, Gallo M, Ruggeri RM, Giacinto PD, Sesti F, Prinzi N, et al. Nutritional status and follicular-derived thyroid cancer: an update. Crit Rev Food Sci Nutr. 2021;61(1):25–59.
Haymart MR, Repplinger DJ, Leverson GE, Elson DF, Sippel RS, Jaume JC, et al. Higher serum thyroid stimulating hormone level in thyroid nodule patients is associated with greater risks of differentiated thyroid cancer and advanced tumor stage. J Clin Endocrinol Metab. 2008;93(3):809–14.
Teng W, Shan Z, Teng X, Guan H, Li Y, Teng D, et al. Effect of iodine intake on thyroid diseases in China. N Engl J Med. 2006;354(26):2783–93.
Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–32.
Liu C, Chen R, Sera F, Vicedo-Cabrera AM, Guo Y, Tong S, et al. Ambient particulate air pollution and daily mortality in 652 cities. N Engl J Med. 2019;381(8):705–15.
Friedrich MJ. Air pollution is greatest environmental threat to health. JAMA. 2018;319(11):1085.
Day DB, Xiang J, Mo J, Li F, Chung M, Gong J, et al. Association of Ozone Exposure with cardiorespiratory pathophysiologic mechanisms in healthy adults. JAMA Intern Med. 2017;177(9):1344–53.
Hwang SH, Choi YH, Paik HJ, Wee WR, Kim MK, Kim DH. Potential importance of ozone in the association between outdoor air pollution and dry eye disease in South Korea. JAMA Ophthalmol. 2016;134(5):503–10.
Howe CG, Eckel SP, Habre R, Girguis MS, Gao L, Lurmann FW, et al. Association of Prenatal Exposure to ambient and traffic-related air pollution with newborn thyroid function: findings from the Children's health study. JAMA Netw Open. 2018;1(5):e182172.
Ghassabian A, Pierotti L, Basterrechea M, Chatzi L, Estarlich M, Fernandez-Somoano A, et al. Association of Exposure to ambient air pollution with thyroid function during pregnancy. JAMA Netw Open. 2019;2(10):e1912902.
Clemons GK, Wei D. Effect of short-term ozone exposure on exogenous thyroxine levels in thyroidectomized and hypophysectomized rats. Toxicol Appl Pharmacol. 1984;74(1):86–90.
Morris AL, Stremme DW, Sheppard BJ, Walsh MT, Farina LL, Francis-Floyd R. The onset of goiter in several species of sharks following the addition of ozone to a touch pool. J Zoo Wildl Med. 2012;43(3):621–4.
Kotwal A, Cortes T, Genere N, Hamidi O, Jasim S, Newman CB, et al. Treatment of thyroid dysfunction and serum lipids: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2020;105(12):3683–94.
Wang D, Li D, Guo X, Yu S, Qiu L, Cheng X, et al. Effects of sex, age, sampling time, and season on thyroid-stimulating hormone concentrations: a retrospective study. Biochem Biophys Res Commun. 2018;506(3):450–4.
Kitahara CM, Sosa JA. The changing incidence of thyroid cancer. Nat Rev Endocrinol. 2016;12(11):646–53.
Benvenga S, Antonelli A, Vita R. Thyroid nodules and thyroid autoimmunity in the context of environmental pollution. Rev Endocr Metab Disord. 2015;16(4):319–40.
Bradley D. Obesity, thyroid nodularity, and thyroid cancer: epiphenomenon orcause? J Clin Endocrinol Metab. 2020;105(8):e3010–2.
Rayman MP. Multiple nutritional factors and thyroid disease, with particular reference to autoimmune thyroid disease. Proc Nutr Soc. 2019;78(1):34–44.
Wang Y, Wang J, Chen Z, Ma M, Lin C, He Q, et al. Analysis of the correlation between high iodized salt intake and the risk of thyroid nodules: a large retrospective study. BMC Cancer. 2021;21(1):1000.
Gao M, Chen W, Sun H, Fan L, Wang W, Du C, et al. Excessive iodine intake is associated with formation of thyroid nodules in pregnant Chinese women. Nutr Res. 2019;66:61–7.
Li Y, Teng D, Ba J, Chen B, Du J, He L, et al. Efficacy and safety of long-term universal salt iodization on thyroid disorders: epidemiological evidence from 31 provinces of mainland China. Thyroid. 2020;30(4):568–79.
Janssen BG, Saenen ND, Roels HA, Madhloum N, Gyselaers W, Lefebvre W, et al. Fetal thyroid function, birth weight, and in utero exposure to fine particle air pollution: a birth cohort study. Environ Health Perspect. 2017;125(4):699–705.
Zhao Y, Cao Z, Li H, Su X, Yang Y, Liu C, et al. Air pollution exposure in association with maternal thyroid function during early pregnancy. J Hazard Mater. 2019;367:188–93.
Henriquez AR, House JS, Snow SJ, Miller CN, Schladweiler MC, Fisher A, et al. Ozone-induced dysregulation of neuroendocrine axes requires adrenal-derived stress hormones. Toxicol Sci. 2019;172(1):38–50.
Huffman LJ, Beighley CM, Frazer DG, McKinney WG, Porter DW. Increased susceptibility of the lungs of hyperthyroid rats to oxidant injury: specificity of effects. Toxicology. 2006;225(2–3):119–27.
Huffman LJ, Judy DJ, Brumbaugh K, Frazer DG, Reynolds JS, McKinney WG, et al. Hyperthyroidism increases the risk of ozone-induced lung toxicity in rats. Toxicol Appl Pharmacol. 2001;173(1):18–26.
Clemons GK, Garcia JF. Changes in thyroid function after short-term ozone exposure in rats. J Environ Pathol Toxicol. 1980;4(1):359–69.
Henriquez AR, Snow SJ, Schladweiler MC, Miller CN, Dye JA, Ledbetter AD, et al. Beta-2 adrenergic and glucocorticoid receptor agonists modulate ozone-induced pulmonary protein leakage and inflammation in healthy and Adrenalectomized rats. Toxicol Sci. 2018;166(2):288–305.
Ferrari SM, Fallahi P, Elia G, Ragusa F, Ruffilli I, Paparo SR, et al. Thyroid autoimmune disorders and cancer. Semin Cancer Biol. 2020;64:135–46.
Boi F, Minerba L, Lai ML, Marziani B, Figus B, Spanu F, et al. Both thyroid autoimmunity and increased serum TSH are independent risk factors for malignancy in patients with thyroid nodules. J Endocrinol Investig. 2013;36(5):313–20.
Resende de Paiva C, Grønhøj C, Feldt-Rasmussen U, von Buchwald C. Association between Hashimoto’s thyroiditis and thyroid cancer in 64,628 patients. Front Oncol. 2017;7:53. https://doi.org/10.3389/fonc.2017.00053.
Ralli M, Angeletti D, Fiore M, D'Aguanno V, Lambiase A, Artico M, et al. Hashimoto's thyroiditis: an update on pathogenic mechanisms, diagnostic protocols, therapeutic strategies, and potential malignant transformation. Autoimmun Rev. 2020;19(10):102649.
Shibutani S, Takeshita M, Grollman AP. Insertion of specific bases during DNA synthesis past the oxidation-damaged base 8-oxodG. Nature. 1991;349(6308):431–4.
McDorman KS, Pachkowski BF, Nakamura J, Wolf DC, Swenberg JA. Oxidative DNA damage from potassium bromate exposure in long-Evans rats is not enhanced by a mixture of drinking water disinfection by-products. Chem Biol Interact. 2005;152(2–3):107–17.
Kurokawa Y, Maekawa A, Takahashi M, Hayashi Y. Toxicity and carcinogenicity of potassium bromate--a new renal carcinogen. Environ Health Perspect. 1990;87:309–35.
Shanmugavel V, Komala Santhi K, Kurup AH, Kalakandan S, Anandharaj A, Rawson A. Potassium bromate: effects on bread components, health, environment and method of analysis: a review. Food Chem. 2020;311:125964.
Acknowledgments
Not applicable.
Funding
This study was supported by the National Natural Science Foundation of China (grant numbers 81974423(S. Chang), 81902729(P. Huang)), the Key Research and Development Program of Hunan Province (grant number 2019SK2031(S. Chang)), the China Postdoctoral Science Foundation (grant number 2020 M672517(P. Huang), 2021 T140749(P. Huang)), the Natural Science Foundation of Hunan Province (2020JJ5904(P. Huang)), and the Xiangya Hospital Foundation for Young Scholars (grant number 2018Q01(P. Huang)).
The study funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
P. Huang and S. Chang had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: P. Huang, Q. He, S. Chang. Acquisition, analysis, or interpretation of data: HL. Tan, B. Wei, N. Tang, JJ. Chen, M. Liu, Q. Shi, M. Wu. Drafting of the manuscript: Q. He, Q. Shi. Critical revision of the manuscript for important intellectual content: P. Huang and S. Chang. Statistical analysis: Q. He. Obtained funding: P. Huang and S. Chang. Administrative, technical, or material support: S. Chang. Supervision: S. Chang. Additional contributions: Chuanzheng Sun, MD and Yao Lu, MD, Ph.D. (the Third Xiangya Hospital of Central South University) contributed insights to this work, for which they were not compensated. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplemental Table 1.
Basic characteristics of 39,353 patients with thyroid function. Supplemental Table 2. Age-standardized detection rates of TNs in Hunan Province from 2010 to 2019, stratified by tumor size, all age, both sexes. Supplemental Table 3. Age-standardized detection rates of TNs in Hunan Province from 2010 to 2019, stratified by age, all tumor sizes, both sexes. Supplemental Table 4. Age-standardized detection rates of TNs in Hunan Province from 2010 to 2019, stratified by sex, all tumor sizes, all ages. Supplemental Figure 1. Trends in TNs Detection Rates, Stratified by Sex, all ages, 2010–2019. Supplemental Figure 2. Trends in TNs Detection Rates, Stratified by age, all tumor sizes, 2010–2019. Supplemental Figure 3. Trends in Detection Rates of TNs with the maximum diameter > 1 cm, Stratified by age, 2010–2019. Supplemental Figure 4. Trends in Detection Rates of TNs with the maximum diameter ≤ 1 cm, Stratified by age, 2010–2019. Supplemental Figure 5. Multivariable Regression Models for TSH Level with Restricted Cubic Splines.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
He, Q., Wu, M., Shi, Q. et al. Association of Ozone Exposures with the risk of thyroid nodules in Hunan Province: a population-based cohort study. Environ Health 21, 65 (2022). https://doi.org/10.1186/s12940-022-00874-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12940-022-00874-8