
Abstract
Background
Short-term particulate air pollution exposure is associated with reduced heart rate variability (HRV), a risk factor for cardiovascular morbidity and mortality, in many studies. Associations with sub-chronic or long-term exposures, however, have been sparsely investigated. We evaluated the effect of fine particulate matter (PM2.5) and black carbon (BC) exposures on HRV in an elderly cohort: the Normative Aging Study.
Methods
We measured power in high frequency (HF) and low frequency (LF), standard deviation of normal-to-normal intervals (SDNN), and the LF:HF ratio among participants from the Greater Boston area. Residential BC exposures for 540 men (1161 study visits, 2000–2011) were estimated using a spatio-temporal land use regression model, and residential PM2.5 exposures for 475 men (992 visits, 2003–2011) were modeled using a hybrid satellite based and land-use model. We evaluated associations between moving averages of sub-chronic (3–84 day) and long-term (1 year) pollutant exposure estimates and HRV parameters using linear mixed models.
Results
One-standard deviation increases in sub-chronic, but not long-term, BC were associated with reduced HF, LF, and SDNN and an increased LF:HF ratio (e.g., 28 day BC: −2.3 % HF [95 % CI:−4.6, −0.02]). Sub-chronic and long-term PM2.5 showed evidence of relations to an increased LF and LF:HF ratio (e.g., 1 year PM: 21.0 % LF:HF [8.6, 34.8]), but not to HF or SDNN, though the effect estimates were very imprecise and mostly spanned the null.
Conclusions
We observed some evidence of a relation between longer-term BC and PM2.5 exposures and changes in HRV in an elderly cohort. While previous studies focused on short-term air pollution exposures, our results suggest that longer-term exposures may influence cardiac autonomic function.
Similar content being viewed by others
Background
Particulate air pollution exposure is associated with cardiovascular mortality and morbidity in a multitude of epidemiologic studies, including at levels at or below EPA standards [1, 2]. Pathways potentially mediating this association include induction of systemic inflammation [3, 4] and oxidative stress [5, 6], as well as changes in ion channel function in myocardial cells [7] or cardiac autonomic function [8–10].
Heart rate variability (HRV) is a marker of cardiac autonomic control, which reflects autonomic modulation of the rhythmic activity of the sinus node [11]. Reduced HRV is predictive of increased cardiovascular morbidity and mortality risk [12, 13]. Short-term particulate air pollution exposure is associated with reduced HRV in many epidemiologic studies, including a recent meta-analysis [14] and within the current study population [10, 15]. Associations are particularly pronounced among the elderly [16], among those with preexisting cardiovascular disease or diabetes [17], or among people with reduced antioxidative defenses [17, 18]. However, the association between exposure to sub-chronic or chronic air pollution exposure and HRV is unclear, although long-term exposure is known to have a stronger effect on cardiovascular mortality than acute exposure [19]. Also, many previous studies have used air pollution at a central site as the exposure metric, introducing potential exposure error.
Particulate matter is a complex mixture of particles and liquids, traffic and non-traffic components, and varies in composition across geographic regions [1]. Studies to date suggest that traffic-related particulate pollution may contribute significantly to cardiovascular outcomes [17, 20], including changes in HRV [19].
In the current study, we used address-specific estimates of exposure and evaluated whether sub-chronic (3–84 day) and long-term (1 year) exposure to ambient particulate matter <2.5 μm in aerodynamic diameter (PM2.5) or black carbon (BC), a marker for traffic related air pollution, would be associated with reduced HRV in a cohort of elderly men. In addition to examining the main effect of particulate air pollution on HRV, we also evaluated potential modification by oxidative stress allelic profile, hypertension, obesity and diabetes.
Methods
Study population
Our analysis included 540 men enrolled in the Veterans Administration Normative Aging Study (NAS) who had complete information regarding ambient BC concentrations, HRV measures, and all covariates of interest, and who underwent 1161 study visits between November 14, 2000 and August, 24, 2011. We also evaluated a largely overlapping group of 475 participants with complete information regarding PM2.5 concentrations and all covariates, who presented for 992 study visits between January 14, 2003 and December 21, 2011. The NAS is a prospective cohort study, described in detail previously [21]. Briefly, this closed cohort was established in 1963 and enrolled 2280 adult male volunteers, free of chronic medical conditions, who were living in the Greater Boston area. Detailed questionnaires and physical examinations were administered at all center-based study visits, occurring every 3–5 years. Loss to follow-up has been predominantly due to death or moving out of the study area.
There were 727 active NAS study participants during the time period of interest. Of these, 596 participants had complete information regarding sub-chronic or long-term residential BC exposures and HRV measures for one or more study visits, and 540 had complete information regarding PM2.5 exposures and HRV measurements. We excluded study participants with problematic heart rate measurements from the analysis (as described below, n = 56 for BC and n = 65 for PM2.5), which brought the final sample size to 540 for BC and 475 for PM2.5. Participants presented for 1–4 visits, with 65.6 % (n = 354) undergoing at least two study visits for BC and 65.1 % (n = 309) for PM2.5.
Physical examinations included measurement of height and weight, which was used to calculate body mass index (BMI, in kg/m2). Blood samples were collected to assess fasting blood glucose (FBG) levels. Smoking history was obtained via an American Thoracic Society questionnaire. Participants’ diabetes status was assessed based on a physician’s diagnosis of type 2 diabetes, and/or use or diabetes medication assessed during the physician interview. Similarly, hypertension was defined as a measured systolic blood pressure (SBP) of ≥140 mmHg, a measured diastolic blood pressure (DBP) of ≥90 mm Hg, or participant use of anti-hypertensive medication. SBP and DBP were measured by a physician, and mean arterial blood pressure (MAP) was defined as DBP + 1/3(SBP-DBP). Finally, room temperature was recorded at the time of electrocardiogram (ECG) measurement.
This study was approved by the Harvard School of Public Health and Veteran Administration institutional review boards, and all participants provided their written informed consent.
To summarize, all participants were administered questionnaires and were examined by a physician at each study visit. These examinations included measurement of heart rate variability, described below. Outdoor temperature and residential air pollution exposure estimates were also evaluated for several time periods preceding a participants’ study visit and are described below.
Heart rate variability
HRV was measured between 6:00 AM and 1:00 PM using a two-channel, five-lead ECG monitor (Trillium 30,000; Forest Medical, East Syracuse, NY), as described in detail previously [10, 22]. Briefly, participants rested for 5 min, and then remained seated during the ECG, which was recorded at a sampling rate of 256 Hz per channel for approximately 7 min. Heart rate and HRV measures were then calculated using PC-based software (Trillium 3000 PC Companion Software for MS Windows; Forest Medical, East Syracuse, NY) and reviewed by an experienced scanner to correct for any errors. The following HRV measures were computed: high-frequency power (HF; 0.15–0.4 Hz), low-frequency power (LF; 0.04–0.15 Hz), LF:HF ratio, and the standard deviation of normal-to-normal intervals (SDNN). HF is a marker of parasympathetic drive, LF is a marker of both sympathetic and para-sympathetic activity, and the LF:HF ratio reflects the balance of sympathetic and para-sympathetic systems and may also be influenced by baroreflexes. In contrast to the latter frequency domain measures, SDNN is a time domain measure that reflects the variability in N-N interval duration. As mentioned above, participants with problematic heart rate measurements (i.e., atrial fibrillation, atrial bigeminy/trigeminy, pacemakers, irregular rhythm, irregular sinus rhythm, frequent ventricular ectopic activity, ventricular bigeminy, multifocal atrial tachycardia, or a measurement time of less than 3.5 min) were excluded from our analysis.
Air pollution and weather
Daily BC exposures at participants’ residences in the greater Boston area was estimated using a validated spatio-temporal land-use regression model [23]. Daily BC predictions were obtained using estimates averaged from 148 monitoring sites, local meteorological conditions, land use variables (including traffic density), day of the week, and other factors [24]. Spatially-resolved daily residential PM2.5 exposures were also estimated at each residence using a validated hybrid exposure model, which incorporated satellite based aerosol optical depth (AOD) measurements as well as land-use and meteorological variables (i.e., outdoor temperature, elevation, visibility, wind speed, distance to major roads, percent of open space, traffic density, proximity to point emissions, and area emissions). More in depth details can be found in Kloog et al. [25].
For this study, we evaluated moving averages of pollutant exposure at 3, 7, 21, 14, 28, 56 and 84 days as well as 1 year prior to each study visit. Specifically, we calculated each participant’s average pollutant exposure level during a given number of a days before each study visit. We also calculated BC and PM2.5 levels 1 and 2 days prior to the study visits, for use in sensitivity analyses.
Our regression models accounted for both room temperature and outdoor temperature. Apparent temperature is defined as a person’s perceived outdoor temperature in °C ([26, 27], and calculated using the following formula: −2.653 + (0.994 * air temperature) + (0.0153 * dew-point temperature)). We calculated moving averages of apparent temperature, corresponding to 1–28 days before each study visit. Measured outdoor temperature was also averaged during the two months, three months, and one year preceding each study visit.
Oxidative stress genetic scores
Oxidative stress allelic profiles were calculated using a genetic score approach [28], in which genetic variants were selected using the least absolute shrinkage and selection operator (Lasso) based on their relation to 8-hydroxydeoxyguanosine levels (8-OhdG, a marker of oxidative DNA damage) [28]. The genetic variants used to calculate oxidative stress score were CAT (rs1001179, rs480575), GC (rs2282679), GCLM (rs3170633), HMOX1 (rs2071746, rs5995098), and NQO1 (rs1800566). Scores representing participants’ allelic profiles were constructed by summing these genetic variants, using the signs of the coefficients of the Lasso penalization [28].
Statistical analyses
We evaluated the association between one standard deviation (SD) increases in moving averages of BC and PM2.5 exposure estimates (3 days-1 year) and several HRV measures (HF, LF, LF:HF, and SDNN), using linear mixed models with random intercepts and a compound-symmetry covariance structure in a repeated measures study. The outcome of interest was percent change in HRV, which was calculated as [10(β*SD)-1]*100 %; 95 % confidence intervals (CIs) were calculated as [10[SD*(β±1.96*SE)]-1]*100 %, where SE is the standard error associated with the regression coefficient β [10]. Measures of HRV were log-transformed to improve normality and stabilize the variance.
All models controlled for potential confounders, which were identified following a thorough literature search: age, BMI, FBG, smoking history (current, former, or never), current use of anti-hypertensive medications (yes/no), room temperature at the time of ECG measurement, season (indicated using the sine and cosine of the date), MAP, and moving averages of outdoor temperature corresponding to the pollutant exposure measurement interval of interest (using both a linear and quadratic term).
Because of previous research indicating potentially susceptible subgroups [10, 15], we examined effect modification of the association between 28 day exposure to BC and HRV parameters by obesity (defined as BMI ≥ 30 kg/m2; yes/no), hypertension (yes/no), diabetes (yes/no) and oxidative stress allelic profile (high/low; dichotomized based on median score) using separated linear regression models. We also included multiplicative interaction terms in regression models to evaluate effect modification. We conducted all analyses using SAS versions 9.3 and 9.4.
Survivor bias
Because people who did not return for subsequent visits are likely to have been less healthy than those who did, this study, like all longitudinal cohorts, can suffer from a dynamic selection bias. To counteract this, we used inverse probability weighting. Specifically, we modeled the probability of returning for a visit based on variables available at previous visits, including HRV measures. The observations were given weights of one for the first visit, the inverse of the probability of returning for the second visit, and the product of the inverse of the probability of returning for the second visit times the inverse of the probability of returning for the third visit, and so on for subsequent visits.
Results
Participants’ characteristics at baseline visit are reported in Table 1. Briefly, at this initial examination, participants evaluated for the association between BC and HRV presented with a mean age of 73.6 years; most (71 %) were former or current smokers, 20 % were diabetic and 25 % had a BMI > 30 kg/m2. Participants evaluated for the association between PM2.5 and HRV presented with a mean age of 75.2 years; most (70 %) were former or current smokers, 21 % were diabetic and 26 % had a BMI > 30 kg/m2. We also present participants’ baseline HRV measures (HF, LF, SDNN, and the LF:HF ratio) in Table 1.
Pollutant concentrations across all study visits and averaging periods are reported in Table 2. For example, for a 28 day moving average of BC exposure, we observed a mean exposure level of 0.4 μg/m3 (SD: 0.2; 5th–95th percentiles: 0.2–0.8 μg/m3); for PM2.5, the corresponding values were 9.5 μg/m3 (SD: 2.5; 5th–95th percentiles: 5.8–14.2 μg/m3). For a 3 day moving average of BC exposure, we observed a mean exposure level of 0.4 μg/m3, with a standard deviation of 0.3. We report Spearman correlation coefficients between selected exposure measure durations (3, 14, 28 and 84 days, as well as 1 year) for both BC and PM2.5 in Additional file 1: Table S1. For BC, correlations between exposure measurement periods were fairly high, ranging from 0.65 to 0.97. For PM2.5, correlations were somewhat weaker, ranging from 0.25 to 0.87. The correlation between 28 day BC exposure and 1 year BC exposure was r = 0.76, and the corresponding correlation for PM2.5 was r = 0.53.
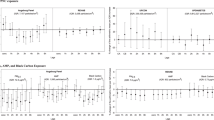
Associations between moving averages of BC and PM2.5 exposures and HRV parameters are presented in Table 3. We observed associations between increased sub-chronic BC exposure and decreased HF, LF, and SDNN, as well as an increased LF:HF ratio, though the confidence intervals were somewhat imprecise and in most cases spanned the null. This association was slightly stronger when evaluating 28-day and 56-day moving averages of exposure relative to other exposure durations, and was strongest for HF in comparison to other measures of HRV. For example, a 1 SD increase in BC measured during the preceding 28 days was associated with a 2.3 % decrease in HF (95 % CI: −4.6, −0.02), a 1 SD increase in 21 day BC exposure was associated with a 2.2 % decrease in HF (95 % CI: −4.4, 0.1), and a 1 SD increase in 7 day BC exposure was associated with a 1.9 % decrease in HF (95 % CI: −4.3, 0.6). A 1 SD increase in 28 day BC exposure was also associated with a 1.0 % decrease in LF (95 % CI: −3.0, 1.0), a 0.5 % decrease in SDNN (95 % CI: −1.5, 0.4), and a 1.3 % increase in the LF:HF ratio (95 % CI: −0.2, 2.8). When evaluating long-term BC exposures of 1 year prior to study visit, results showed a similar pattern but were attenuated greatly (Table 3). Moreover, when we included 28 day and 1 year BC exposure in the same model for HF, the magnitude of the association with 28 day BC increased, while the association with 1 year BC changed direction (data not shown). Similarly, effect estimates for 28 day BC were strengthened when adjusting for BC exposure 1 day before the visit (data not shown), indicating that short-term exposures are not dominating the observed association with sub-chronic BC.
We found some evidence of associations between increased short-term PM2.5 exposure estimates and decreases in HF, LF, and SDNN, as well as increased LF:HF ratio (our results for a 3 day moving average are reported in Table 3; data for 1 and 2 day averages are not shown), though the associated confidence intervals were very wide and many of the effect estimates were not statistically significant. In addition, the patterns of association we observed for shorter-term exposures were inconsistent when evaluating associations between modeled PM2.5 exposures reflecting 7 day to 1 year moving averages and HF and SDNN (Table 3). Associations between sub-chronic and long-term PM2.5 and both LF and the LF:HF ratio were consistently elevated and tended to be strongest for longer-term exposures. For example, the percent increase in the LF:HF ratio in relation to a 1 SD increase in PM2.5 was 13.1 % (95 % CI: −10.8, 43.5) for a 14 day moving average, 31.4 % (95 % CI: 5.9, 63.0) for a 28 day moving average, and 21.0 % (95 % CI: 8.6, 34.8) for a 1 year average. The corresponding increases for LF were 15.6 % (95 % CI: −16.2, 59.4), 22.4 % (95 % CI: −8.6, 64.1), and 23.6 % (95 % CI: 6.0, 44.1, respectively (Table 3).
Finally, associations between 28 day BC exposure estimates and HF stratified by obesity, hypertension, diabetes, and oxidative stress genetic score are reported in Table 4. We also examined interactions between 28 day BC and the aforementioned characteristics with respect to other HRV measures (data not shown). No multiplicative interaction terms rose to the level of statistical significance and confidence intervals were wide. Consistent with previous findings, however, the decrease in HRV in relation to BC exposure was greater among those with obesity or diabetes. For example, a 1 SD increase in BC exposure was associated with a 1.7 % decrease in HF (95 % CI: −4.5, 1.2) among men with BMI <30, and a 3.5 % decrease in HF among men with a BMI of 30 or greater (95 % CI: −7.4, 0.5) (Table 4). BC exposure was also associated with a greater increase in HF among those with a lower oxidative stress genetic score. We observed no consistent patterns for hypertension.
Discussion
We report positive associations between several measures of sub-chronic BC exposure, a marker of traffic pollution, and decreased HRV in a cohort of elderly men, although confidence intervals were wide and mostly spanned the null. These findings are consistent with many previous studies reporting associations between short-term particulate pollution exposure and decreased HRV [10, 14], which is predictive of increased cardiovascular morbidity and mortality [12, 13], but extend the literature to longer exposure measurement periods, and demonstrate somewhat larger effect sizes for those longer exposures. Longer-term exposures may be of most interest when assessing risk for adverse cardiovascular outcomes [19]. It is also notable that the observed associations reflect not only short-term spikes in particulate levels, but rather occur at particulate pollutant levels that are consistently at or below EPA standards. Our also extends the literature by using a sophisticated modeling approach, rather than fixed monitoring data, to predict individualized residential pollutant exposures during 3, 7, 14, 21, 28, 56 and 84 days and well as 1 year prior to each study visit [23, 25]. When evaluating BC exposures, we consistently found a larger effect size for HF, a marker of parasympathetic drive, than for LF. We also found some evidence of an increased LF:HF ratio. Recent research suggests the LF:HF ratio may be influenced primarily by parasympathetic output and baroreflex function [29, 30].
We observed attenuated associations between HF and 1-year BC exposure, which changed direction upon adjustment for 28-day BC exposure, suggesting the weak association observed between 1 year BC and HRV was explained by correlations with the shorter-term, sub-chronic exposures rather than by the long-term exposure. We did not observe a consistent pattern of associations between sub-chronic or long-term PM2.5 exposure and HF. While studies consistently report associations between short-term particulate pollution exposure and reduced HF, especially among the elderly or those with preexisting conditions [14, 16], very few have examined exposure periods of greater than a few days [31, 32]. Hence, although long-term PM exposure is known to have a stronger effect on cardiovascular mortality than acute exposure [19], the effects of long-term or sub-chronic particulate exposure on HF are unclear. Specifically, to our knowledge, only two studies have examined the association between long-term PM exposure (specifically, PM <10 μm in aerodynamic diameter [PM10] levels averaged over a 10 year period, among participants aged 50 and over) and HRV; they reported a null overall association between long-term PM10 and HRV, with reduced HRV observed among participants taking ACE inhibitors or with a particular pro-inflammatory polymorphism [31, 32]. Ours is also the first study to evaluate sub-chronic PM2.5 or BC exposure in relation to HRV. Further studies are necessary to clarify the effect of longer-term pollutant exposure on cardiac autonomic control.
We report discrepant findings for BC and PM2.5. The direction of results for modeled PM2.5 exposure 1, 2, or 3 days prior to the study visit are consistent with previous fixed monitoring studies from the NAS [10, 15] as well as with our findings for sub-chronic BC exposure. Air pollution was associated with decreased HF, LF, and SDNN as well as an increased LF:HF ratio in these studies. In our study, associations between longer-term PM2.5 levels and HF measures were inconsistent, and PM2.5 was related to an increase in LF, which is inconsistent with previous studies among elderly people, but is sometimes seen among younger subjects [33, 34]. We also observed a consistent, though imprecise, positive association between PM2.5 exposure and an increased LF:HF ratio, which was similar to our results for BC and was in general strongest for exposures measured over longer time periods.
Although BC is a component of PM, the source profiles of BC and PM2.5 differ. BC is a marker of traffic pollution, especially diesel exhaust and, in Boston, home heating oil [35], whereas these sources contribute to a minority of PM2.5 levels [36, 37]. The effects of different particle components or sources on health outcomes may vary, and emerging evidence suggests that traffic pollution may be especially important with regard to cardiovascular disease [38]. It should be noted that BC and PM2.5 estimates were derived from different exposure models; the differences in results for BC and PM2.5 and for shorter and longer-term PM2.5 do not have a clear biological basis and could also be due to a difference in modeling approach. We also note that that confidence intervals for the PM2.5 estimates were very wide, which increases the likelihood some of our results may be due to chance. While we cannot be sure of an underlying mechanism, one possible reason that we observed stronger associations for sub-chronic rather than long-term BC could be that HRV fluctuates based on a variety of short-term stimuli and this might overpower the effect of air pollution exposure over the course of a year, but not a shorter period of 1–2 months.
Potential mechanisms underlying possible associations between BC or PM2.5 and HRV include a particulate-induced increase in pulmonary oxidative stress, which can in turn induce proinflammatory cytokines [39], increase extracellular calcium influx [40], inactivate nitric oxide [41], and lead to greater parasympathetic than sympathetic nervous system withdrawal [19]. The result of these changes is an increased risk of cardiovascular morbidity and mortality, including ventricular arrhythmias and myocardial infarction [19].
We did not observe strong evidence of effect modification by obesity, hypertension, diabetes, or oxidative stress allelic profile, which may have been due to the low precision of stratified effect estimates. While not rising to the level of statistical significance, associations between BC exposure and HRV were somewhat stronger among men with obesity and diabetes, which is notable mainly because of similarity to previous findings [10, 15]. One explanation for these findings is that diabetes and obesity are themselves associated with reduced autonomic function [42–44], possibly rendering diabetics and those with a BMI over 30 kg/m2 more susceptible to the effects of particles on this same endpoint. We observed a stronger reduction in HF relative to BC exposure among men with lower oxidative stress genetic scores, which was unexpected. It should be noted that we did not have sufficient power to examine effect modification in an optimal way, and larger studies will be needed in the future in order to examine the possibility of susceptible subgroups more thoroughly, and to obtain more precise and stable effect estimates than we were able to calculate.
We acknowledge several limitations of our study. These include potential exposure misclassification of pollutant estimates, which could affect precision and potential bias effect size [45]. This possibility is standard to environmental epidemiology studies, and our use of sophisticated, spatially and temporally resolved models to estimate individualized residential pollutant exposures has likely reduced misclassification relative to fixed monitoring studies. The exposure model also did not account for indoor pollutant levels or residential indoor temperatures, and did not estimate the rate at which outdoor pollutants may penetrate indoors, though studies have shown that the contribution of outdoor air pollution to indoor pollutant levels [46, 47] and to monitored personal exposures, including in the Boston area [48], is fairly high.
Our study did not adjust for multiple comparisons. We chose to qualitatively examine the pattern of results instead. As we noted earlier, the confidence intervals associated with most of the observed effect estimates were wide, especially when evaluating PM2.5, and only a handful of effect estimates were statistically significant. Our findings are consistent with the greater literature on this subject, which adds plausibility to the pattern of associations we observed. Larger studies with greater statistical power will be needed to confirm and expand on our initial findings.
Ideally, we would have compared results for PM2.5 and BC estimated from the same exposure models. However, this was not possible in our study because PM2.5 levels were derived from AOD measurements, which do not capture the BC component of PM, and many of the BC measurements were obtained from ethylometers, which measured BC but not overall PM. Thus, we cannot rule out that differences in our findings for BC and fine PM could be due to differing modeling approaches.
The changes in HRV that we observed in this study do not rise to a level of clinical concern, but shifting the distribution of HRV measures may be of public health concern because of changes among ‘borderline’ individuals. Furthermore, PM2.5 levels in the Boston area are generally below EPA air quality standards, whereas other areas may have consistently higher pollutant levels which could affect HRV to a greater extent. Finally, part of our goal was to identify mechanisms mediating the association between particulate pollutant exposure and adverse cardiovascular outcomes, and these results, if confirmed, suggest that effects on HRV may be part of that pathway.
Our study population is comprised of elderly men, the vast majority of whom are retired, which is both a limitation and strength. Participants’ estimated residential exposures are likely to reflect the great majority of their total exposure burden, which is a strength in terms of exposure assessment, but results may not be generalizable to other (non-elderly, non-White, female) segments of the population. We examined this association within an elderly cohort because the elderly comprise a large, susceptible sub-population with respect to cardiovascular ailments and health effects of particle exposure. Finally, the sampling rate we used when measuring HRV is still clinically appropriate, but is lower that what is currently preferred for research purposes. This could lead to some non-differential measurement error and a consequent reduction in statistical power and bias towards the null.
Strengths of our study include access to a large, general population cohort with extensive and repeated information regarding pollutant exposures, potential confounders and effect modifiers, and HRV data from multiple study visits. While most air pollution studies examine short-term exposures, longer-term exposures may be of most interest when assessing risk for chronic disease and dysfunction. Hence, an additional strength of our study was the reconstruction of participants’ sub-chronic and long-term BC and PM2.5 exposures using comprehensive models. Our use of spatially resolved residential exposure measurements is another important strength, especially for BC, since traffic exposures can vary significantly within a small geographic distance [25].
Conclusions
In our study of particulate air pollution exposure and HRV, we report a pattern of associations between sub-chronic BC exposure estimates and decreased HF, LF, and SDNN, as well as increased LF:HF ratio. Although our limited statistical power led to wide confidence intervals that often spanned the null, our findings were similar to previous studies of short-term exposure in the NAS [10] and other study populations [14]. Long-term BC exposure was not linked to HRV after adjustment for sub-chronic exposure levels. We report discrepant findings for BC and PM2.5, as sub-chronic and long-term PM2.5 exposure estimates were associated with an increased LF and LF:HF ratio, but not other changes in HRV (HF or SDNN). HRV may mediate associations between particulate exposures and adverse cardiovascular outcomes, and assessing longer-term exposures is important to understanding effects of air pollution on chronic disease and dysfunction. Future high-powered studies should therefore further evaluate associations between sub-chronic or long-term pollutant exposures and HRV, including with respect to identifying potentially susceptible subpopulations.
Abbreviations
- 8-OhdG:
-
8-hydroxydeoxyguanosine
- AOD:
-
aerosol optical depth
- BC:
-
black carbon
- BMI:
-
body mass index
- CAT :
-
catalase
- DBP:
-
diastolic blood pressure
- ECG:
-
electrocardiogram
- FBG:
-
fasting blood glucose
- GC :
-
group-specific component
- GCLM :
-
glutamate-cysteine ligase, modifier subunit
- HF:
-
high frequency power
- HMOX1 :
-
heme oxygenase 1
- HRV:
-
heart rate variability
- LF:
-
low frequency power
- MAP:
-
mean arterial blood pressure
- NAS:
-
Normative Aging Study
- NQO1 :
-
NAD(P)H dehydrogenase, quinone 1
- PM10:
-
particulate matter <10 μm in aerodynamic diameter
- PM2.5:
-
particulate matter <2.5 μm in aerodynamic diameter
- SBP:
-
systolic blood pressure
- SD:
-
standard deviation
- SDNN:
-
standard deviation of normal-to-normal intervals
- SE:
-
standard error
References
Brook RD. Cardiovascular effects of air pollution. Clin Sci. 2008;115(6):175–87.
Miller KA, Siscovick DS, Sheppard L, Shepherd K, Sullivan JH, Anderson GL, et al. Long-term exposure to air pollution and incidence of cardiovascular events in women. N Engl J Med. 2007;356(5):457–8.
Dubowsky SD, Suh H, Schwartz J, Coull BA, Gold DR. Diabetes, obesity, and hypertension may enhance associations between air pollution and markers of systemic inflammation. Environ Health Perspect. 2006;114:992–8.
O’Neill MS, Veves A, Sarnat JA, Zanobetti A, Gold DR, Economides PA, et al. Air pollution and inflammation in type 2 diabetes: a mechanism of susceptibility. Occup Environ Med. 2007;64(6):373–9.
Kim JY, Mukherjee S, Ngo LC, Christiani DC. Urinary 8-hydroxy-2′-deoxyguanosine as a biomarker of oxidative DNA damage in workers exposed to fine particulates. Environ Health Perspect. 2004;112:666–71.
Nel A. Air pollution-related illness: effects of particles. Science. 2005;308(5723):804–6.
Utell MJ, Frampton MW, Zareba W, Devlin RB, Cascio WE. Cardiovascular effects associated with air pollution: potential mechanisms and methods of testing. Inhal Toxicol. 2002;14:1231–47.
Devlin RB, Ghio AJ, Kehrl H, Sanders G, Cascio W. Elderly humans exposed to concentrated air pollution particles have decreased heart rate variability. Eur Respir J Suppl. 2003;40:76s–80.
Gold DR, Litonjua A, Schwartz J, Lovett E, Larson A, Nearing B, et al. Ambient pollution and heart rate variability. Circulation. 2000;101:1267–73.
Park SK, O’Neill MS, Vokonas PS, Sparrow D, Schwartz J. Effects of air pollution on heart rate variability: the VA Normative Aging Study. Environ Health Perspect. 2005;113(3):304–9.
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: standards of measurement, physiological interpretation and clinical use. Circulation. 1996;93:1043–65.
Tsuji H, Larson MG, Venditti Jr FJ, Manders ES, Evans JC, Feldman CL, et al. Impact of reduced heart rate variability on risk for cardiac events. The Framingham Heart Study. Circulation. 1996;94(11):2850–5.
Nolan J, Batin PD, Andrews R, Lindsay SJ, Brooksby P, Mullen M, et al. Prospective study of heart rate variability and mortality in chronic heart failure: results of the United Kingdom heart failure evaluation and assessment of risk trial (UK-heart). Circulation. 1998;98(15):1510–6.
Pieters N, Plusquin M, Cox B, Kicinski M, Vangronsveld J, Nawrot TS. An epidemiological appraisal of the association between heart rate variability and particulate air pollution: a meta-analysis. Heart. 2012;98:1127–35.
Baja ES, Schwartz JD, Coull BA, Wellenius GA, Vokonas PS, Suh HH. Structural equation modeling of parasympathetic and sympathetic response to traffic air pollution in a repeated measures study. Environ Health. 2013;12(1):81.
Creason J, Neas L, Walsh D, Williams R, Sheldon L, Liao D, et al. Particulate matter and heart rate variability among elderly retirees: the Baltimore 1998 PM study. J Expo Anal Environ Epidemiol. 2001;11(2):116–22.
Schwartz J, Litonjua A, Suh H, Verrier M, Zanobetti A, Syring M, et al. Traffic-related pollution and heart rate variability in a panel of elderly subjects. Thorax. 2005;60(6):455–61.
Chahine T, Baccarelli A, Litonjua A, Wright RO, Suh H, Gold DR, et al. Particulate air pollution, oxidative stress genes, and heart rate variability in an elderly cohort. Environ Health Perspect. 2007;12:1617–22.
Brook RD, Rajagopalan S, Pope 3rd CA, Brook JR, Bhatnagar A, Diez-Roux AV, et al. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation. 2010;12:2331–78.
Laden F, Neas LM, Dockery DW, Schwartz J. Association of fine particulate matter from different sources with daily mortality in six U.S. cities. Environ Health Perspect. 2000;108:941–7.
Bell B, Rose C, Damon A. The Normative Aging Study: an interdisciplinary and longitudinal study of health and aging. Aging Hum Dev. 1972;3:4–17.
Pope III CA, Eatough DJ, Gold DR, Pang Y, Nielsen KR, Nath P, et al. Acute exposure to environmental tobacco smoke and heart rate variability. Environ Health Perspect. 2001;109:711–6.
Suglia SF, Gryparis A, Wright RO, Schwartz J, Wright RJ. Association of black carbon with cognition among children in a prospective birth cohort study. Am J Epidemiol. 2008;167:280–6.
Fang SC, Mehta AJ, Alexeeff SE, Gryparis A, Coull B, Vokonas P, et al. Residential black carbon exposure and circulating markers of systemic inflammation in elderly males: the Normative Aging Study. Environ Health Perspect. 2012;120(5):674–80.
Kloog I, Chudnovsky A, Just A, Nordio F, Koutrakis P, Coull B, et al. A new hybrid spatio temporal model for estimating daily multi-year PM2.5 concentrations across northeastern USA using high resolution aerosol optical depth data. Atmos Environ. 2014;95:581–90.
Kalkstein LS, Valimont KM. An evaluation of summer discomfort in the United States using a relative climatological index. Bull Am Meteorol Soc. 1986;7:842–8.
O’Neill MS, Zanobetti A, Schwartz J. Modifiers of the temperature and mortality association in seven US cities. Am J Epidemiol. 2003;157:1074–82.
Bind MA, Coull B, Suh H, Wright RO, Baccarelli A, Vokonas P, et al. A novel genetic score approach using instruments to investigate interactions between pathways and environment: application to air pollution. PLoS One. 2014;9(4), e96000.
Goldstein DS, Bentho O, Park MY, Sharabi Y. Low-frequency power of heart rate variability is not a measure of cardiac sympathetic tone but may be a measure of modulation of cardiac autonomic outflows by baroreflexes. Exp Physiol. 2011;96(12):1255–61.
Reyes del Paso GA, Langewitz W, Mulder LJ, van Roon A, Duschek S. The utility of low frequency heart rate variability as an index of sympathetic cardiac tone: a review with emphasis on a reanalysis of previous studies. Psychophysiology. 2013;50(5):477–87.
Adam M, Felber-Dietrich D, Schaffner E, Carballo D, Barthelemy JC, Gaspoz JM, et al. Long-term exposure to traffic-related PM(10) and decreased heart rate variability: is the association restricted to subjects taking ACE inhibitors? Environ Int. 2012;48:9–16.
Adam M, Imboden M, Boes E, Schaffner E, Kunzli N, Phuleria HC, et al. Modifying effect of a common polymorphism in the interleukin-6 promoter on the relationship between long-term exposure to traffic-related particulate matter and heart rate variability. PLoS One. 2014;9(8), e104978.
Link MS, Dockery DW. Air pollution and the triggering of cardiac arrhythmias. Curr Opin Cardiol. 2010;25(1):16–22.
Shields KN, Cavallari JM, Hunt MJ, Lazo M, Molina M, Molina L, et al. Traffic-related air pollution exposures and changes in heart rate variability in Mexico City: a panel study. Environ Health. 2013;12:7.
Grahame TJ, Klemm R, Schlesinger RB. Public health and components of particulate matter: the changing assessment of black carbon. J Air Waste Manag Assoc. 2014;64(6):620–60.
Keuken MP, Moerman M, Voogt M, Blom M, Weijers EP, Röckmann T, et al. Source contributions to PM2.5 and PM10 at an urban background and street location. Atmos Environ. 2013;71:26–35.
Thurston GD, Ito K, Lall R. A source apportionment of U.S. fine particulate matter air pollution. Atmos Environ. 2011;45(24):3924–36.
Adar SD, Kaufman JD. Cardiovascular disease and air pollutants: evaluating and improving epidemiological data implicating traffic exposure. Inhal Toxicol. 2007;19 Suppl 1:135–49.
Donaldson K, Stone V, Seaton A, MacNee W. Ambient particle inhalation and the cardiovascular system: potential mechanisms. Environ Health Perspect. 2001;109 Suppl 4:523–7.
Stone V, Tuinman M, Vamvakopoulos JE, Shaw J, Brown D, Petterson S, et al. Increased calcium influx in a monocytic cell line on exposure to ultrafine carbon black. Eur Respir J. 2000;15:297–303.
Thomas GD, Zhang W, Victor RG. Impaired modulation of sympathetic vasoconstriction in contracting skeletal muscle of rats with chronic myocardial infarctions: role of oxidative stress. Circ Res. 2001;88:816–23.
Burger AJ, Aronson D. Effect of diabetes mellitus on heart rate variability in patients with congestive heart failure. Pacing Clin Electrophysiol. 2001;24:53–9.
Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, Pi-Sunyer FX, et al. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation. 2006;113(6):898–918.
Singh JP, Larson MG, O’Donnell CJ, Wilson PF, Tsuji H, Lloyd-Jones DM, et al. Association of hyperglycemia with reduced heart rate variability (the Framingham Heart Study). Am J Cardiol. 2000;86:309–12.
Bergen S, Sheppard L, Sampson PD, Kim SY, Richards M, Vedal S, et al. A national prediction model for PM2.5 component exposures and measurement error-corrected health effect inference. Environ Health Perspect. 2013;121(9):1017–25.
Partti-Pellinen K, Marttila O, Ahonen A, Suominen O, Haahtela T. Penetration of nitrogen oxides and particles from outdoor into indoor air and removal of the pollutants through filtration of incoming air. Indoor Air. 2000;10(2):126–32.
Meng QY, Spector D, Colome S, Turpin B. Determinants of indoor and personal exposure to PM2.5 of indoor and outdoor origin during the RIOPA study. Atmost Environ. 2009;43(36):5750–8.
Sarnat JA, Brown KW, Schwartz J, Coull BA, Koutrakis P. Ambient gas concentrations and personal particulate matter exposures: implications for studying the health effects of particles. Epidemiology. 2005;16(3):385–95.
Acknowledgments
This work was supported by the US Environmental Protection Agency grants R832416 and RD 83479801 and by the National Institute of Environmental Health Sciences grants ES015172-01 and ES000002. The VA Normative Aging Study is supported by the Cooperative Studies Program/Epidemiology Research and Information Center of the U.S. Department of Veterans Affairs and is a component of the Massachusetts Veterans Epidemiology Research and Information Center, Boston, Massachusetts.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing financial or non-financial interests.
Authors’ contributions
IM was involved in designing and conducting statistical analyses, interpretation of results, drafting the manuscript, and review and approval of the manuscript. BC and IK were both involved in creating the study’s environmental exposure model and in the review and approval of the manuscript. PK was also involved in the creation of the study’s environmental exposure model and was involved in other aspects of data acquisition as well as review and approval of the manuscript. PV was involved in data acquisition and review and approval of the manuscript. JS was involved in the study conception, data acquisition, analysis, and interpretation, drafting of the manuscript, and review and approval of the manuscript. All authors read and approved the final manuscript.
Additional file
Additional file 1: Table S1.
Spearman correlation coefficients between selected exposure measurement intervals for BC and PM2.5a. BC: black carbon; PM2.5: particulate matter <2.5 μm in aerodynamic diameter a. Normative Aging Study (2000–2011). (DOC 39 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Mordukhovich, I., Coull, B., Kloog, I. et al. Exposure to sub-chronic and long-term particulate air pollution and heart rate variability in an elderly cohort: the Normative Aging Study. Environ Health 14, 87 (2015). https://doi.org/10.1186/s12940-015-0074-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12940-015-0074-z