
Abstract
Background
According to many conceptual frameworks, the first step in the monitoring cycle of health inequalities is the selection of relevant topics and indicators. However, some difficulties may arise during this selection process due to a high variety of contextual factors that may influence this step. In order to help accomplish this task successfully, a comprehensive review of the most common topics and indicators for measuring and monitoring health inequalities in countries/regions with similar socioeconomic and political status as Catalonia was performed.
Methods
We describe the processes and criteria used for selecting health indicators from reports, studies, and databases focusing on health inequalities. We also describe how they were grouped into well-known health topics. The topics were filtered and ranked by the number of indicators they accounted for.
Results
We found 691 indicators used in the study of health inequalities. The indicators were grouped into 120 topics, 34 of which were selected for having five indicators or more. Most commonly found topics in the list include “Life expectancy”, “Infant mortality”, “Obesity and overweight (BMI)”, “Mortality rate”, “Regular smokers/tobacco consumption”, “Self-perceived health”, “Unemployment”, “Mental well-being”, “Cardiovascular disease/hypertension”, “Socioeconomic status (SES)/material deprivation”.
Conclusions
A wide variety of indicators and topics for the study of health inequalities exist across different countries and organisations, although there are some clear commonalities. Reviewing the use of health indicators is a key step to know the current state of the study of health inequalities and may show how to lead the way in understanding how to overcome them.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Strong efforts to tackle health inequalities can be seen at international and national level since the 1980s. In early 2008, the World Health Organization’s (WHO) Global Commission on Social Determinants of Health called for action on the social determinants of health, the conditions in which persons are born, grow, work, live, and age, to “close the gap in a generation” [1]. In late 2008, the Spanish Public Health General Direction (Dirección General de Salud Pública) and the Foreign Health of Health Ministry and Social Policy (Sanidad Exterior del Ministerio de Sanidad y Política Social) requested the constitution of the Commission for the Reduction of Social and Health Inequalities (Comisión para Reducir las Desigualdades Sociales en Salud en España (CRDSS-E) [2]. The mission of CRDSS-E was to elaborate on a proposal of intervention measures to reduce health inequalities. The CRDSS-E published two documents: one analysing health inequalities in the Spanish context [3], and another describing some policy proposals to tackle them [4]. In 2011, a total of 125 countries, Spain being one of them, developed and signed the Rio Political Declaration on Social Determinants of Health [5]. The declaration recommended interventions from governments and international organisations [6].
At a regional level in Catalonia, tackling health inequalities is one of the main goals of both the Catalan Health Plan 2016–2020 (led by the Health Department of the Catalan Government) [7] and the Interdepartmental and Intersectorial Public Health Plan 2017–2020 (PINSAP) [8, 9]. During the past years, various reports and peer-reviewed papers about the health effects of the economic crisis on the population of Catalonia were published by the Catalan Health System Observatory [10,11,12,13,14,15,16,17].
Overall, much effort has been devoted to monitoring and tackling health inequalities at regional, national, and international levels. Even so, OECD countries continue to present large disparities in health, including, for example, significant differences in life expectancy between people with the highest and lowest levels of education [18]. The selection of topics represents the first step in monitoring health inequalities according to many conceptual frameworks and is highly relevant, as these topics will potentially limit the detection of health inequalities within the population, hence playing a key role in providing evidence for posterior decision-making [19, 20]. Yet some difficulties may arise during the selection of relevant topics, as well as their health indicators. A wide diversity of indicators for monitoring health inequalities have been used across different countries and organisations; this is due to the high variety of contextual factors that may have an influence on it, such as the study goals or the information resources available.
In order to help accomplish this task successfully, the objective of this study is to perform a systematic review of the most common topics and indicators used for measuring and monitoring health inequalities in the reports, projects, and databases of international, national, and regional governmental organizations.
The main purpose of this study is to provide a broad overview of health inequalities topics considered relevant by different public health organizations. Nevertheless, the focus of this review is on countries/regions with similar socioeconomic and political status to Catalonia. It may also be useful for other organizations who decide to study or monitor health inequalities to accomplish its very first step: topic selection. In addition, gaining some insights about which health issues are being prioritized, as well as which indicators were used, are considered secondary goals.
Material and methods
First, a bibliographic search was performed using PubMed, Google Scholar, and Google search engine with the terms “health inequalities”, “health observatories” and “health inequalities indicators”. Occasionally, names of concrete regions, countries, or organisations were added to these terms (i.e., “Andalucía health observatory” or “Canada health inequalities”). The search was performed from March to June of 2019. Once finished, a set of inclusion criteria was applied; studies included in the review had to:
-
1.
Include health inequalities indicators: All the reports that contained no health indicators were automatically discarded (i.e., policy frameworks [21]).
-
2.
Have been carried out by a governmental organisation or a related entity, whether at an international, national, or regional level: the reports not published by governmental (or government-related) organisations were discarded.
-
3.
Have a socioeconomic and political status similar (or highly related) to Catalonia: some reports were discarded due to significant differences in the socioeconomic profile of the countries they were studying in comparison to Catalonia or Spain.
Once the reports were selected, the authors performed a quality control check of the indicators shown in the reports and databases. The indicators had to match the basic anatomy of an indicator as a minimum requirement to be considered an indicator. This basic anatomy consists of containing data, i.e. the numerical data input; and containing good metadata, like a title and an explanation of how an indicator is defined and calculated [22]. In addition, the different reports found were classified according to the geo-political region they were studying: 1. international, 2. national, and 3. regional (Table 1).
After this selection process, the indicators were grouped into topics by semantic matching of their definition as well as by the area of knowledge there are intended to measure. Most of the topics were supported by references of relevant organisations like the WHO or the United Nations (UN) (see Table 2). Each topic was uniquely named in accordance with the area of knowledge that instruments were intended to measure. Indicators from different sources were often merged due to high similarities between them (most commonly, the only differences were stratifiers such as age, gender or region). Every topic had to be formed by at least five indicators in order to be considered relevant enough; the topics with less than five indicators were discarded.
The search was performed by the two researchers, and the results shared in order to agree on any discrepancies. All the data was organised in spreadsheets to identify common indicators, and then sorted by the amount of indicators they included. The names of the indicators in the spreadsheets were those given in the original reports or their metadata information.
Results
In total, 21 reports, projects, and databases were identified and classified into three categories: 1. international [8], 2. national [10], and 3. regional [3]. In the first category, international, all the projects selected were carried out or funded by the European Commission [23,24,25,26,27], the WHO [28, 29] or the World Bank [30]. In the following category, national, studies were conducted by health agencies or governments of countries such as Andorra [31], Australia [32], Canada [33, 34], England [35, 36], Scotland [37], Slovenia [38], Spain [39] or Portugal [40]. In the last category, regional, some reports published by Spanish regions were included (Andalucía [41], Barcelona [42], Valencia [43]). A total of 691 health indicators were identified (Table 1).
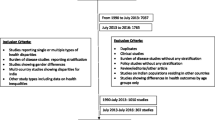
Following an iterative process of evaluation, we identified a core set of 120 candidate topics, of which 34 were finally selected (Fig. 1). Table 2 describes a complete list of 34 topics with the corresponding definition of each topic. The ten most commonly used were: “Life expectancy”, “Infant mortality”, “Obesity and overweight (BMI)”, “Mortality rate”, “Regular smokers/tobacco consumption”, “Self-perceived health”, “Unemployment”, “Mental well-being”, “Cardiovascular disease/hypertension”, “Socioeconomic status (SES)/material deprivation”. However, some topics that ranked below these were closely related with some of the most common topics; for example, “Perinatal, neonatal and stillbirths mortality” might be considered as a subtype of “Infant mortality”; and “Perceived mental health” is similar to both “Mental well-being” and “Self-perceived health”. Furthermore, some indicators may represent antithetically the same area of knowledge; that is the case for the indicators in the topic “Long-term limitations/chronic illnesses” and the indicator “Healthy Life Years (HLY)” [within the topic “Life expectancy”], where the former (long-term limitations or chronic illnesses) is used to determine the latter (the end of a healthy life condition). Nevertheless, the metadata of the health indicators within each topic was highly homogeneous: they all had similar definitions and methodology.

Flowchart of the processes undertaken to review the most common topics in the study of health inequalities
In general, the indicators within each topic were very similar. In fact, often the differences among them were related to the different stratifiers (such as sex, age or region) used for their calculation. For example, in the first topic “Life expectancy”, indicators have different variations: “Life expectancy at birth” [23,24,25, 27,28,29, 32, 33, 37, 40,41,42], “Life expectancy at birth by sex” [22, 24,25,26,27, 33, 34], “Life expectancy at a certain age” [25, 33, 35, 40], “Life expectancy by educational attainment level” [25], and “Life expectancy at birth by socioeconomic status” [25]. Complex measures of inequality, such as “Slope index of inequality (SII) for male and female life expectancy” [34] may be considered another (more advanced) variation.
Furthermore, in the case of a health outcomes or diagnostics (such as mortality or cancer) the concrete disease or cause may also play an important role in the heterogeneity found among the health indicators. Indicators are focused on different aspects, such as prevalence and incidence, mortality, preventive measures, or treatments. For example, for the topic “HIV”: “HIV incidence” [23, 26, 28, 33, 40], “Prevalence of HIV, male/female, by ages” [29, 39] and “AIDS-related mortality rate” [28, 39] are the most common, yet “Antiretroviral therapy (ART) coverage” [28] and “HIV test results for TB patients (positive results)” [28] can also be relevant.
The results of the study show that the most common topics are related to:
-
Mortality/life expectancy: “Life expectancy” [44, 45], “Infant mortality” [46] or “Mortality rate” [47] are widely used to study health inequalities.
-
Incidence/mortality rates of specific diseases: “Cardiovascular disease/hypertension”, “Cancer (incidence or mortality)” [48], “Diabetes/insulin resistance” [49], “HIV” [50], “Tuberculosis (TB)” [51] or “Respiratory diseases”.
-
Social determinants of health [52]:
-
◦ “Living and working conditions” where this could be studied at an individual level, was highly ranked: “Unemployment” [53] and “Primary studies/illiteracy”. Otherwise, these indicators were at the bottom of the list.
-
◦ This was similar for “Individual lifestyle factors and social and community networks” topics, which can also be studied at an individual level: “Obesity and overweight (BMI)” [54, 55], “Regular smokers/tobacco consumption” [56], “Alcohol consumption” [57], “Hazardous alcohol consumption”, “Physical activity” [58], and “Food consumption (vegetables, fruit, salt)”.
-
◦ Socioeconomic level: “Socioeconomic status (SES)/material deprivation” [59, 60].
-
◦ Healthcare system: “Healthcare resources” and “Policy and Legislation”.
-
Discussion
Main results of the study
The results of the study showed that the most common topics were related to mortality/life expectancy, incidence/mortality rates of specific diseases (i.e., TB or HIV), and social determinants of health, such as living and working conditions, and individual lifestyle factors and social and community networks, according to Dahlgren and Whitehead’s model of the social determinants of health [52]. The indicators that can be studied at an individual level tended to be highly ranked, in comparison to those that are studied at different levels (such as hospital or region), which tended to be at the bottom. Many methodological differences between indicators were due to stratifiers in their calculation.
Study selection criteria
To include health inequalities indicators was a fundamental requirement for any report in order to be included in the review. Hence, although some reports provided in-depth insights about tackling health inequalities (i.e., [21, 61]) they were not selected due to lack of health indicators monitoring.
In addition, to be carried out by a governmental or a government-related organisation was also an important requirement, as many academic and/or private institutions carry out studies and reviews of health inequalities, but their policy-making influence is limited. Their reports tend to be focused on concrete knowledge fields, such as gender influence [62], the effects of economic crises [63], or access to healthcare [64]; which are also relevant for the study of health inequalities but whose authorship does not fit the selection criteria, as the main interest of this paper is identifying the health inequalities indicators used by health agencies or similar government-related entities. The reports not produced by this kind of organisation were rejected.
Lastly, to have a socioeconomic and politic status similar or highly related to Catalonia criteria was intended to exclude reports whose health indicators were adapted to least developed/developing countries where, for example, access to treatments of diarrhea for infants may still be an issue [65]. Hence, some reports were discarded due to significant differences in the socioeconomic profile of the countries they are studying in comparison to Catalonia or Spain.
These criteria were applied to all the reports and studies found after an extensive search. The addition of country/region names in the search responded to the need of knowing how particular regions of interest were dealing with health inequalities. Interest in regions was mainly based on previous knowledge of concrete public health organizations studying those regions, as well as interest in looking for other organizations in charge of tackling health inequalities in regions similar to Catalonia. Nevertheless, as in any review, it is not possible to ensure that absolutely all the reports suitable for this study were found during the search, nor that they were selected after applying the selection criteria.
Grouping health indicators into topics
As stated above, the most frequent health indicators were grouped into topics according to the health domain they were measuring (with each indicator related to only one topic). For example, although “Percentage of 15-year-olds who were overweight in 2009–10, EU Member States by sex” [25] and “Obesity rate by body mass index (BMI) (sdg_02_10)” [23, 66] are different indicators per se, they are both intended to measure the same health issue and, hence, were grouped under the same topic “Obesity and overweight (BMI)” under the indicator name “Obesity and/or overweight (total, by sex, age, or educational level)”.
Most of the selected health indicators were taken from the official statistics of different countries or international organisations, whose development and methodology has been closely consolidated over many years and respond to international standards. In addition, most of these indicators are related to relevant knowledge areas for the study of health inequalities, such as lifestyle habits, deprivation, and mortality.
To prioritise the most relevant topics, all the groups with less than five health indicators were deleted. This meant that, unfortunately, interesting topics such as the “Years of potential life lost” [34, 36, 42], “Unmet health needs” [23, 26, 39] and “Passive smokers” [33, 34] were not taken into consideration. Nevertheless, this selection does not imply per se a periodic monitoring of the selected health indicators, as specific topics not present in this list may be studied according to ultimate needs.
Relevance of the most common topics
All the topics aim to measure and study the relation between determinants of health and health outcomes. Interestingly, three of the top five topics in the list (see Table 2) are related to mortality: life expectancy, infant mortality, and mortality rate. Life expectancy at birth is an indicator of mortality conditions and, by proxy, of health conditions [44]. Hence, life expectancy as well as other mortality-related topics are widely used in the study of health inequalities.
Living and working conditions, such as BMI or smoking, are also key factors in the study of health inequalities as both share a strong socioeconomic gradient [54, 56]. Therefore, as may be expected, they appeared among the top 10 positions in the list of topics (see Table 2). According to our review, the most common way to measure socioeconomic status is to analyse the unemployment rates and material deprivation level of the population.
In Spain, some regions use less common health indicators for studying health inequalities that may be interesting for particular knowledge areas. For example, the Valencian Observatory of Health uses the “Caregiver profile”, which they report to be mostly women, without primary studies, 57-years-old on average, and reporting bad self-perceived health. In addition, they also use “Reasons why contraceptive methods are not used by age and nationality of women” as well as a “Sexual-health information resources (school, parents, friends, etc.)”, which may help to understand possible sexual health inequalities [43]. In the Andalusian School of Public Health, the indicator “Psychosis and mental illnesses due to drugs or alcohol abuse” may be helpful to estimate various negative health outcomes of alcohol and substance abuse that the healthcare system will need to address [41]. Even so, more than a half of topics in Table 2 appear in their reports.
As may be expected, the health indicators used in other reports produced by the Catalan Health System Observatory, such as the “Community Health Indicators”, match the implicit measurement concept behind many of the topics: obesity and overweight, mortality by age (including infant), self-perceived health, and population with primary studies are some of them [67].
Health indicators
As can be seen in Table 3, health indicators were combined within each topic if stratifiers such as population sex, age, or region were the only difference in their calculation methodologies. Some indicators were also merged if they were formerly different in the way they expressed the same data (i.e., raw number, rate per 1000 or 100,000).
The health indicators within each topic often cover a different aspect relevant to health inequalities. For example, in the topic “Tuberculosis” [23, 29, 33, 34, 40, 42, 43] indicators about incidence, prevalence, or mortality can be observed. In addition, health indicators about treatment coverage or vaccination are also included in this topic. Overall, in most topics, indicators try to measure every relevant (and measurable) aspect of the topic.
Common stratifiers are sex, age, and studied region, something that is coherent with the determinants of health perspective and the focus on inequalities. However, the stratifiers found are highly heterogeneous and may also include socioeconomic status, educational level, or nationality/country of origin, among many others.
Research fitted to monitor health inequalities
This comprehensive review was carried out to help accomplish the first step in the process for tackling and monitoring health inequalities: selecting high-impact issues and health indicators [19, 20]. The next steps in the analysis will be to carefully take into account stratifiers such as area of residence, gender, age, and nationality. Lastly, after the identification of key health inequalities, decision-making stakeholders will need to play a role during the last steps: determining priorities of action and implementing changes. The time variable will play a key role in the monitoring, as it will indicate the possible health consequences of policy-making decisions [19, 20].
Conclusions
Reviewing the most common health indicators and topics used in the study of health inequalities may help research teams in different ways. First, having an overview of what is being done by their neighbouring countries or regions may highlight issues that should not be missed when selecting relevant health topics to study. Second, even if some topics might not ultimately be chosen as a priority of action, having a complete list of key issues will provide an overview of what is relevant in the study of health inequalities, as well as some interesting insights. Lastly, knowing what other research institutions are working on will promote potential collaborations between organizations, creating synergies and bonds that may lead to better understanding and monitoring of health inequalities.
At a regional level, these results are highly valuable for the first stages of health inequalities monitoring cycles in Catalonia. This study provided the basis for choosing health topics to study as well as helped gain insights about which indicators should be used. In addition, regions with similar socioeconomic status and goals in tackling health inequalities may benefit from this research. Similarly, at a national and international level these results may help organizations shift the focus towards undermined health inequalities topics or explore new areas of knowledge (yet unstudied or with a different perspective).
Availability of data and materials
No analysis of quantitative data was performed. Hence, data availability declaration is not applicable.
Abbreviations
- AIDS:
-
Acquired immune deficiency syndrome
- AMI:
-
Acute myocardial infarction
- BCG:
-
Bacillus Calmette-Guérin
- BMI:
-
Body mass index
- COPD:
-
Chronic obstructive pulmonary disease
- CRDSS-E:
-
Comisión para Reducir las Desigualdades Sociales en Salud en España
- CVD:
-
Cardiovascular disease
- ECHI:
-
European Core Health Indicators
- GHQ-12:
-
12-Item General Health Questionnaire
- GP:
-
General practitioner
- HI:
-
Health indicators
- HIV:
-
Human Immunodeficiency Virus
- HLY:
-
Healthy Life Years
- ICD9MC:
-
International Classification of Diseases, Clinical Modification
- IHR:
-
International Health Regulations
- NHS:
-
National Health Service
- PDF:
-
Portable document format
- PHAC:
-
Public Health Agency of Canada
- PINSAP:
-
Interdepartmental and Intersectorial Public Health Plan
- PTCA:
-
Percutaneous transluminal coronary angioplasty
- SDG:
-
Sustainable Development Goals
- SES:
-
Socioeconomic status
- SII:
-
Slope index of inequality
- TB:
-
Tuberculosis
- URL:
-
Uniform resource locator
- UN:
-
United Nations
- WHO:
-
World Health Organization
References
World health organization (WHO). Meeting report of the world conference on social determinants of health. Rio de Janeiro, 19-21. Geneva: WHO; 2011. p. 2012. http://www.who.int/sdhconference/resources/wcsdh_report/en/. Accessed 24 July 2019
Comisión para Reducir las Desigualdades Sociales en Salud en España. Propuesta de políticas e intervenciones para reducir las desigualdades sociales en salud en España. Gac Sanit. 2012:182–9.
Comisión para Reducir las Desigualdades Sociales en Salud en España. Análisis de situación para la elaboración de una propuesta de políticas e intervenciones para reducir las desigualdades sociales en salud en España. Madrid: Ministerio de Sanidad y Política Social; 2009. http://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/promocion/desigualdadSalud/docs/Analisis_reducir_desigualdes.pdf. Accessed 24 July 2019.
Comisión para Reducir las Desigualdades Sociales en Salud en España. Avanzando hacia la equidad: propuesta de políticas e intervenciones para reducir las desigualdades sociales en salud en España. Madrid: Ministerio de Sanidad y Política Social; 2010. http://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/promocion/desigualdadSalud/docs/Propuesta_Politicas_Reducir_Desigualdades.pdf. Accessed 24 July 2019.
World Health Organization (WHO). Rio political declaration on social determinants of health Rio de Janeiro, Brazil. Geneva: WHO; 2011. p. 2012. https://www.who.int/sdhconference/declaration/en/. Accessed 24 July 2019
Working Group for Monitoring Action on the Social Determinants of Health. Towards a global monitoring system for implementing the Rio Political Declaration on Social Determinants of Health: developing a core set of indicators for government action on the social determinants of health to improve health equity. Int J Equity Health. 2018;17(1):136.
Government of Catalonia. Health plan for Catalonia 2016–2020. Barcelona: Ministry of Health of Catalonia; 2016. http://salutweb.gencat.cat/web/.content/_departament/pla-de-salut/Pla-de-salut-2016-2020/documents/health-plan-catalonia_2016_2020.pdf. Accessed 24 July 2019
Comissió Interdepartamental de Salut. Pla interdepartamental i intersectorial de salut pública. Barcelona: Ministry of Health of Catalonia; 2017. http://salutpublica.gencat.cat/web/.content/minisite/aspcat/sobre_lagencia/pinsap/01Els_Plans/PINSAP_2017-2020/PINSAP_2017-2020-Complet.pdf. Accessed 24 July 2019
Cabezas-Peña C. Catalonia, Spain. Regions for Health Network (RHN). Geneva: WHO; 2018. http://www.euro.who.int/__data/assets/pdf_file/0004/373387/rhn-catalonia-eng.pdf. Accessed 24 July 2019
Observatori del Sistema Salut de Catalunya. Efectes de la crisi econòmica en la salut de la població de Catalunya. Barcelona: Agency for Health Quality and Assessment of Catalonia; 2014. http://observatorisalut.gencat.cat/web/.content/minisite/observatorisalut/contingutsadministratius/observatori_efectes_crisi_salut_document.pdf. Accessed 24 July 2019
Observatori del Sistema Salut de Catalunya. Efectes de la crisi econòmica en la salut de la població de Catalunya. Anàlisi territorial. Agency for Health Quality and Assessment of Catalonia: Barcelona; 2015. http://observatorisalut.gencat.cat/web/.content/minisite/observatorisalut/ossc_crisi_salut/Fitxers_crisi/Salut_crisi_informe_2015.pdf. Accessed 24 July 2019
Observatori del Sistema Salut de Catalunya. Desigualtats socioeconòmiques en la salut i la utilització de serveis sanitaris públics en la població de Catalunya. Agency for Health Quality and Assessment of Catalonia: Barcelona; 2017. http://observatorisalut.gencat.cat/web/.content/minisite/observatorisalut/ossc_crisi_salut/Fitxers_crisi/Salut_crisi_informe_2016.pdf. Accessed: 13 September 2019
Observatori del Sistema Salut de Catalunya. Central de Resultats: Efectes de la crisi econòmica en la població infantil de Catalunya. Barcelona: Agency for Health Quality and Assessment of Catalonia; 2014. http://observatorisalut.gencat.cat/web/.content/minisite/observatorisalut/contingutsadministratius/observatori_efectes_crisi_salut_monografic.pdf. Accessed 20 March 2020
Observatori del Sistema Salut de Catalunya. Central de Resultats: Evolució de la utilització de serveis i el consum de fàrmacs 2008–2015. Barcelona: Agency for Health Quality and Assessment of Catalonia; 2008. http://observatorisalut.gencat.cat/web/.content/minisite/observatorisalut/ossc_central_resultats/informes/fitxers_estatics/MONOGRAFIC_25_CRISI_EVOLUCIO_2008-2015.pdf. Accessed 20 Mar 2020
García-Altés A, Ruiz-Muñoz D, Colls C, Mias M, Martín BN. Socioeconomic inequalities in health and the use of healthcare services in Catalonia: analysis of the individual data of 7.5 million residents. J Epidemiol Community Health. 2018;72(10):871–9.
Ruiz-Muñoz D, Colls C, Mias M, Martín N, García-Altés A. Desigualtats socioeconòmiques en la salut i la utilització dels serveis sanitaris públics en la població de Catalunya. Ann Med. 2017;100:172–6 https://www.academia.cat/files/499-448-FITXER/provesievidencies1.pdf. Accessed 20 Mar 2020.
Genoveva B, Ruiz-Muñoz D, García-Altés A. Efectes de la crisi econòmica en la salut de la població de Catalunya: anàlisi territorial. Ann Med. 2016;99:126–31 https://www.academia.cat/files/499-386-FITXER/provesievidencies.pdf. Accessed 24 July 2019.
Health for Everyone?. OECD Health Policy Studies. Paris: OECD; 2019. https://www.oecd-ilibrary.org/social-issues-migration-health/health-for-everyone_3c8385d0-en. Accessed 9 Jan 2021.
World Health Organization (WHO). Handbook on health inequality monitoring with a special focus on low- and middle-income countries. Geneva: WHO; 2013.
UK Department of Health. Health equity audit: a self-assessment tool. London: Department of Health, 2004: 25. https://webarchive.nationalarchives.gov.uk/20120105214155/http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4070715. Accessed 13 Sept 2019.
WHO Regional Office for Europe. Health 2020: A European policy framework and strategy for the 21st century. Geneva: WHO; 2013:190. http:// www.euro.who.int/__data/assets/pdf_file/0011/199532/Health2020-Long.pdf. Accessed 24 July 2019.
Pencheon D. The good indicators guide: understanding how to use and choose indicators. Coventry: NHS Institute for Innovation and Improvement; 2017. https://www.england.nhs.uk/improvement-hub/publication/the-good-indicators-guide-understanding-how-to-use-and-choose-indicators. Accessed 25 Mar 2020
Eurostat. SDG 3. Good health and well-being. Luxembourg: European Commission. https://ec.europa.eu/eurostat/web/sdi/good-health-and-well-being. Accessed 8 Apr 2020.
ECHI-European Core Health Indicators. Luxembourg: European Commission. https://ec.europa.eu/health/indicators/echi/list_en#id3. Accessed 8 Apr 2020.
Marmot M. Health inequalities in the EU - final report of a consortium. Luxembourg: Publications Office of the European Union; 2013. [https://ec.europa.eu/health//sites/health/files/social_determinants/docs/healthinequalitiesineu_2013_en.pdf]. Accessed 8 Apr 2020
Social Protection Committee. Indicators Sub-group. Portfolio of EU social indicators for the monitoring of progress towards the EU objectives for social protection and social Inclusion. Luxembourg: Publications Office of the European Union; 2015. http://ec.europa.eu/social/BlobServlet?docId=14239&langId=en. Accessed 8 Apr 2020
I2sare project. Galicia, Spain profile. Regional Health Profiles in the European Union, 2010. www.sergas.es/Saude-publica/-I2SARE-Galicia. Accessed 8 Apr 2020.
World Health Organization (WHO). Data Management Tool. Copenhagen: WHO Regional Office for Europe. http://dmt.euro.who.int/classifications/tree/B#B02. Accessed 8 Apr 2020.
World Health Organization (WHO). 100 core health indicators (plus health-related SDGs). Geneva: WHO; 2018. www.who.int/healthinfo/indicators/100CoreHealthIndicators_2018_infogr.April 2020. Accessed 8 April 2020
The World Bank. Health. Data. Washington DC: The World Bank. https://data.worldbank.org/topic/health. Accessed 8 Apr 2020.
Observatori Social d'Andorra. Sant Julià de Lòria (Andorra): Centre d’Estudis Andorrans. Govern d'Andorra https://observatorisocial.ad/index.php. Accessed 8 Apr 2020.
Turrell G, Stanley L, de Looper M. Oldenburg B. Health inequalities in Australia: morbidity, health behaviours, risk factors and health services use (AIHW). Canberra; 2006. www.aihw.gov.au/getmedia/0cbc6c45-b97a-44f7-ad1f-2517a1f0378c/hiamhbrfhsu.pdf. Accessed 8 Apr 2020
Public Health Agency of Canada. Key Health Inequalities in Canada: A National Portrait. Ottawa: Government of Canada; 2018. http://www.canada.ca/en/public-health/services/publications/science-research-data/key-health-inequalities-canada-national-portrait-executive-summary.html. Accessed 8 Apr 2020
Canadian Institute of Health Information. Health Inequalities Data Tool. Ottawa: Government of Canada https://health-infobase.canada.ca/health-inequalities/data-tool/index. Accessed 8 Apr 2020.
Institute of Health Equity. Marmot indicators release 2017. London: Institute of Health Equity; 2017. http://www.instituteofhealthequity.org/about-our-work/marmot-indicators-release-2017. Accessed 8 Apr 2020
NHS England Analytical Services & the Equality and Health Inequalities Unit. England Analysis: NHS Outcome Framework Health Inequalities Indicators. London: NHS England; 2016. http://www.england.nhs.uk/wp-content/uploads/2017/07/nhs-outcome-framework-health-inequalities-indicators-2016-17.pdf. Accessed 8 Apr 2020
Scottish Government. Long-term monitoring of health inequalities. Scottish Government: Edinburgh; 2018. http://www.gov.scot/publications/long-term-monitoring-health-inequalities-december-2018-report. Accessed 8 Apr 2020
Buzeti T, Djomba JK, Blenkuš MG, Ivanuša M, Klanšček HJ, Kelšin N, et al. Health inequalities in Slovenia. Ljubljana: National Institute of Public Health; 2011. http://www.euro.who.int/__data/assets/pdf_file/0008/131759/Health_inequalities_in_Slovenia.pdf. Accessed 8 Apr 2020
Ministry of Health and Social Policy of Spain. Moving forward equity in health: monitoring social determinants of health and the reduction of health inequalities. Madrid: Ministry of Health and Social Policy of Spain; 2010. http://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/promocion/desigualdadSalud/PresidenciaUE_2010/conferenciaExpertos/docs/haciaLaEquidadEnSalud_en.pdf. Accessed 8 Apr 2020
Instituto Nacional de Estatística-Statistics Portugal. Indicadores Sociais 2011. Lisbon: Instituto Nacional de Estatística-Statistics Portugal; 2012. https://censos.ine.pt. Accessed 8 Apr 2020
García-Calvente MM, del Río LM, Marcos-Marcos J. Guía de indicadores para medir las desigualdades de género en salud y sus determinantes. Escuela Andaluza de Salud Pública. Junta de Andalucía: Granada; 2015. http://www.easp.es/project/guia-de-indicadores-para-medir-las-desigualdades-de-genero-en-salud-y-sus-determinantes. Accessed 8 Apr 2020
Malmusi D. Desigualtats en salut, respostes a nivell local: Polítiques per reduir les desigualtats en salut a la ciutat de Barcelona. Barcelona: Ajuntament de Barcelona; 2017. http://www.consorci.org/media/upload/arxius/coneixement/salut-publica/2017/D_%20Malmusi_Desigualtats_28-09-2017.pdf. Accessed 8 Apr 2020
Observatorio Valenciano de la Salud. Desigualdades en Salud en la Comunidad Valenciana. Valencia: Generalitat. Conselleria de Sanitat Universal i Salut Pública; 2018. http://www.sp.san.gva.es/DgspPortal/docs/20180301_Desigualdades_Salud_OVS2018.pdf. Accessed 8 Apr 2020
United Natios (UN). Life expectancy at birth. New York: UN. http://www.un.org/esa/sustdev/natlinfo/indicators/methodology_sheets/health/life_expectancy.pdf. Accessed 19 Mar 2020.
Shryock HS, Siegel JS, Stockwell EG. The methods and materials of demography. San Diego: Academic Press; 1976.
Global Health Observatory (GHO) data. Infant mortality. Geneva: World Health Organization (WHO); 2018. http://www.who.int/gho/child_health/mortality/neonatal_infant/en/. Accessed 8 Apr 2020
Porta M, editor. A dictionary of epidemiology, sixth edition. Oxford: Oxford University Press; 2016. http://www.oxfordreference.com/view/10.1093/acref/9780199976720.001.0001/acref-9780199976720. Accessed 8 Apr 2020
World Health Organization (WHO). Cancer. Geneva: WHO. http://www.who.int/health-topics/cancer#tab=tab_1. Accessed 7 Apr 2020.
World Health Organization (WHO). Diabetes. Geneva: WHO. http://www.who.int/health-topics/diabetes#tab=tab_1. Accessed 7 Apr 2020.
World Health Organization (WHO). HIV/AIDS. Geneva: WHO. http://www.who.int/health-topics/hiv-aids#tab=tab_1. Accessed 7 Apr 2020.
World Health Organization (WHO). Tuberculosis. Geneva: WHO. http://www.who.int/health-topics/tuberculosis#tab=tab_1. Accessed 7 Apr 2020.
Bambra C, Gibson M, Sowden A, Wright K, Whitehead M, Petticrew M. Tackling the wider social determinants of health and health inequalities: evidence from systematic reviews. J Epidemiol Community Health. 2010;64(4):284–91.
Organisation for Economic Co-operation and Development (OECD). OECD Glossary of Statistical Terms-Unemployed–ILO Definition. Paris: OECD; 2003. https://stats.oecd.org/glossary/detail.asp? ID=2791. Accessed 7 Apr 2020
Pigeyre M, Rousseaux J, Trouiller P, Dumont J, Goumidi L, Bonte D, et al. How obesity relates to socio-economic status: identification of eating behavior mediators. Int J Obes. 2016;40(11):1794–801.
World Health Organization (WHO). Obesity and overweight. Geneva: WHO. http://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 7 Apr 2020
WHO, Tobacco and inequities Guidance for addressing inequities in tobacco-related harm Written by: Belinda Loring. 2014.
World Health Organization (WHO). Harmful use of alcohol. Geneva: WHO. http://www.who.int/health-topics/alcohol#tab=tab_1. Accessed 7 Apr 2020.
World Health Organization (WHO). Physical activity. Geneva: WHO. http://www.who.int/news-room/fact-sheets/detail/physical-activity. Accessed 7 Apr 2020.
American Psychological Association (APA). Socioeconomic Status. Washinton DC. http://www.apa.org/topics/socioeconomic-status/. Accessed 6 Apr 2020.
Eurostat. Glossary: Material deprivation - Statistics Explained. Luxembourg: European Commission. https://ec.europa.eu/eurostat/statistics-explained/index.php/Glossary:Material_deprivation. Accessed 6 Apr 2020.
Solar O, Irwin A. A conceptual framework for action on the social determinants of health. Social Determinants of Health Discussion Paper 2. Geneva: World Health Organization (WHO); 2010. p. 79.
Salcedo N, Saez M, Bragulat B, Saurina C. Does the effect of gender modify the relationship between deprivation and mortality? BMC Public Health. 2012;12:574.
Regidor E, Barrio G, Bravo MJ, de la Fuente L. Has health in Spain been declining since the economic crisis? J Epidemiol Community Health. 2014;68(3):280–2.
Consulting Services Limited ICF. Towards a fairer and more effective measurement of access to healthcare across the EU final. London: ICF; 2018. https://ec.europa.eu/health/sites/health/files/cross_border_care/docs/2018_measurement_accesstohealthcare_frep_en.pdf. Accessed 6 Apr 2020
Ebinger JO, Hamso B, Gerner F, Lim A, Plecas A. Europe and Central Asia region. New York: World Bank; 2008. https://elibrary.worldbank.org/doi/abs/10.1596/25984. Accessed 6 Apr 2020
Eurostat. Eurostat - Tables, Graphs and Maps Interface (TGM) table. Luxembourg: European Commission; 2018. https://ec.europa.eu/eurostat/tgm/table.do?tab=table&init=1&language=en&pcode=sdg_02_10&plugin=1. Accessed 28 Feb 2020
Catalan Healthcare System Observatory. Indicadors de salut comunitària. Barcelona: Agència de Qualitat i Avaluació Sanitàries de Catalunya. Departament de Salut; 2017. http://observatorisalut.gencat.cat/ca/observatori-desigualtats-salut/indicadors_comunitaria/. Accessed 25 Mar 2020
Acknowledgements
We thank Neus Carrilero-Carrió (Agència de Qualitat i Avaluació Sanitàries de Catalunya (AQuAS), Barcelona, Spain) for support in reviewing drafts and assistance with writing.
Funding
All the activities performed were funded by the Agència de Qualitat i Avaluació Sanitàries de Catalunya (AQuAS) and CIBER de Epidemiología y Salud Pública (CIBERESP).
Author information
Authors and Affiliations
Contributions
SA performed the main bibliographic review as well as the selection and organisation of health indicators and topics. AGA supervised the whole process, contributed to the conceptualisation of the paper and provided extensive comments and improvements to the drafts. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Albert-Ballestar, S., García-Altés, A. Measuring health inequalities: a systematic review of widely used indicators and topics. Int J Equity Health 20, 73 (2021). https://doi.org/10.1186/s12939-021-01397-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12939-021-01397-3