
Abstract
Background
It is suggested that supplementation with milk protein (MP) has the potential to ameliorate the glycemic profile; however, the exact impact and certainty of the findings have yet to be evaluated. This systematic review and dose–response meta-analysis of randomized controlled trials (RCTs) assessed the impact of MP supplementation on the glycemic parameters in adults.
Methods
A systematic search was carried out among online databases to determine eligible RCTs published up to November 2022. A random-effects model was performed for the meta-analysis.
Results
A total of 36 RCTs with 1851 participants were included in the pooled analysis. It was displayed that supplementation with MP effectively reduced levels of fasting blood glucose (FBG) (weighted mean difference (WMD): -1.83 mg/dL, 95% CI: -3.28, -0.38; P = 0.013), fasting insulin (WMD: -1.06 uU/mL, 95% CI: -1.76, -0.36; P = 0.003), and homeostasis model assessment of insulin resistance (HOMA-IR) (WMD: -0.27, 95% CI: -0.40, -0.14; P < 0.001) while making no remarkable changes in serum hemoglobin A1c (HbA1c) values (WMD: 0.01%, 95% CI: -0.14, 0.16; P = 0.891). However, there was a significant decline in serum levels of HbA1c among participants with normal baseline body mass index (BMI) based on sub-group analyses. In addition, HOMA-IR values were significantly lower in the MP supplement-treated group than their untreated counterparts in short- and long-term supplementation (≤ 8 and > 8 weeks) with high or moderate doses (≥ 60 or 30–60 g/d) of MP or whey protein (WP). Serum FBG levels were considerably reduced upon short-term administration of a low daily dose of WP (< 30 g). Furthermore, the levels of serum fasting insulin were remarkably decreased during long-term supplementation with high or moderate daily doses of WP.
Conclusion
The findings of this study suggest that supplementation with MP may improve glycemic control in adults by reducing the values of fasting insulin, FBG, and HOMA-IR. Additional trials with longer durations are required to confirm these findings.
Similar content being viewed by others

Introduction
The increasing prevalence and burden of type 2 diabetes mellitus (T2DM) and hyperglycemia (very high blood sugar) is a major global health concern [1, 2]. A high blood glucose (HBG) level is a common problem for diabetic patients [2]. Long-term exposure to HBG is the primary causal factor in the pathogenesis of diabetic complications [3]. Hyperglycemia is caused by reduced glucose utilization, increased glucose production, and decreased insulin secretion [4]. It is a potential target to enhance clinical outcomes in hospitalized patients with acute disease, even without overt diabetes [5]. It has been suggested that each 1 mg/ dL increment in fasting glucose concentration may increase the risk of developing diabetes by 9% [6].
Hyperglycemia causes a lot of changes in vascular tissue that could lead to accelerated atherosclerosis [3]. In addition, HBG raises the risk of developing cardiovascular diseases (CVDs) in diabetic and non-diabetic individuals [7]. Furthermore, HBG can be diagnosed in hospitalized patients, even those without diabetes [8]. It can change innate immune responses to infection, leading to poor outcomes in these patients [8]. Therefore, it is essential to monitor blood glucose levels, normalize hyperglycemia, and prevent hyperglycemia-induced complications [9].
Consumption of food products that contain digestible carbohydrates (CHO) can cause postprandial HBG and glycemic responses [10]. A healthy eating pattern is one of the key components of HBG management [11,12,13,14]. Cow milk is a food item necessary for a balanced diet and contains several essential micro- and macronutrients [15]. Lactose is the major carbohydrate with a low glycemic index (GI) in dairy products and a disaccharide of glucose and galactose [10]. The lower GI of dairy products has been linked to their matrix for controlling gastric emptying and the presence of lactose [16, 17]. It was reported that the addition of dairy products to high-carbohydrate meals may reduce postprandial blood glucose levels and have a favorable impact on glycemic profile [18]. It decreases post-meal glycemia when consumed during or before an ad libitum meal [19]. In addition, it may deliver comparatively high levels of CHO with limited glycemic responses [10]. However, glycemic reactions following the consumption of milk products are uncertain and controversial [10].
Bovine milk is a major source of high-quality proteins with various nutritional, physiological, and functional benefits [20]. Milk proteins (MP) have health-promoting effects such as digestion and absorption of nutrients, stimulation of the immune system, and prebiotic effects [21, 22]. They may have hypotensive, anticancer, satiating, anti-inflammatory, antimicrobial, antioxidant, and insulinotropic properties [21, 23], as well as the potential to increase muscle protein synthesis [24]. Casein and whey are the main proteins in dairy products that account for 80% and 20% of the amino acids (AAs) in milk, respectively [25]. They are two of the most common types of protein available on the market with different absorption rates and bioavailability [26]. Whey protein (WP) is rapidly digested, whereas casein protein (CP) is classified as a high-quality protein source [23] with slow digestion and absorption [27] that provides all essential AAs to humans, except cysteine [28]. In contrast, WP has a higher proportion of valine, isoleucine, and leucine (essential AAs that are identified as branched-chain amino acids (BCAAs)) than CP [29]. However, non-essential AAs are more abundant in CP [29].
It has been found that proteins are useful in triggering insulin secretion in T2DM patients [30]. The evidence suggests that MP enhances the postprandial insulin response and reduces the postprandial blood glucose response in healthy individuals [31,32,33] and T2DM patients [1, 34, 35]. The precise mechanisms by which protein of milk lowers the levels of postprandial glucose remain to be determined [36]. The hypothesis is that the AAs and bioactive peptides in MP may lead to delayed gastric emptying, increased incretin and insulin response, and a decrease in postprandial glucose levels [36].
A limited number of reviews and meta-analyses have explored the effects of WP supplementation or dairy products on glycemic control, but they focused only on patients with T2DM [36,37,38,39]. The effects of MP supplements on the glycemic profile of different types of consumers were not well investigated and the outcomes of the studies were controversial or inclusive. In addition, meta-analyses of observational studies have higher risks of bias and heterogeneity compared to randomized controlled trials (RCTs) [40]. The main problems in observational studies are confounders and selection bias, but they are prevented in RCTs by blinding and randomization [41]. Therefore, the aim of this systematic review and meta-analysis of RCTs was to assess the impacts of supplementation with MP on glycemic parameters.
Methods
This systematic review and meta-analysis were performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework [42]. The study protocol was registered in the international prospective register of systematic reviews (PROSPERO) (CRD42023424242).
Search strategy
One reviewer implemented a search strategy to determine relevant RCTs published up to December 2022 in various databases (Medline/ PubMed, Web of Science, and Scopus). The language and period of publications were unrestricted. Google Translate was used to translate articles that were not written in English. The search strategy was focused on four key elements in trials with parallel or crossover design; they were population (adult), exposure/intervention (MP supplement), comparator/control (no intervention or placebo), and outcomes (levels of fasting blood glucose (FBG), hemoglobin A1c (HbA1c), homeostasis model assessment of insulin resistance (HOMA-IR), and fasting insulin). The subsequent medical subject headings (MeSH) and non-MESH were used in the search strategy: (("milk" OR "milk protein" OR "milk protein supplement" OR "milk protein supplementation" OR "whey" OR "casein" OR "whey supplement" OR "whey supplementation" OR "casein supplement" OR "casein supplementation" OR "milk protein concentration" OR "MPC") AND ("glucose tolerance" OR "insulin resistance" OR "FBG" OR "fasting blood glucose" OR "HbA1c" OR "hemoglobin A1c" OR "HOMA-IR" OR "homeostatic model assessment" OR "Insulin" OR "fasting blood sugar" OR "FBS") AND ("Intervention" OR "Intervention Study" OR "Intervention Studies" OR "controlled trial" OR "randomized" OR "randomised" OR "random" OR "randomly" OR "placebo" OR "clinical trial" OR "Trial" OR "randomized controlled trial" OR "randomized clinical trial" OR "RCT" OR "blinded" OR "double-blind" OR "double blinded" OR "trial" OR "clinical trial" OR "trials" OR "Pragmatic Clinical Trial" OR "Cross-Over Studies" OR "Cross-Over" OR "Cross-Over Study" OR "parallel" OR "parallel study" OR "parallel trial")).
Study selection criteria
Identified records were exported to the Endnote reference management software. Two reviewers (SM and SD) independently assessed the studies and determined appropriate RCTs based on the inclusion criteria. They discussed any disagreements or resolved them through negotiation with a third investigator (DAL). This systematic review and meta-analysis included all RCTs (with crossover or parallel design) that looked at the effect of MP administration on serum levels of HbA1c, fasting insulin, HOMA-IR, and FBG in MP supplement-treated individuals compared with their untreated counterparts.
Eligible RCTs enrolled adult individuals and had a cross-over or parallel design, as well as a placebo or control group. They had a pre-post design with a duration longer than two weeks. In addition, the RCTs had sufficient data on the values of HOMA-IR, fasting insulin, HbA1c, and FBG in the MP-treated and placebo groups at the end of each study and baseline. The trials evaluated the impact of supplementation with MP on the glycemic parameters in participants. Furthermore, the MP supplement was not administered as a multi-component supplement in the MP-treated and placebo groups. Moreover, RCTs with one of the following criteria were excluded: non-placebo-controlled or uncontrolled trials; studies that included individuals under 18 years of age or pregnant women; RCTs with < 2 weeks in duration; non-RCTs or observational studies; trials with inadequate data on selected outcomes at follow-up or baseline assessments.
Data extraction
Two independent researchers (SM and HSO) extracted data from eligible full-text articles to determine the required information; disagreements were resolved through discussion. The extracted data were related to study characteristics (sample size, publication year, trial duration and setting, study design, dose of MP supplement, type of placebo or control group, and first author’s name), and participants’ demographics (mean body mass index (BMI), age, and gender). In addition, pre- and post-assessments of selected outcomes (HOMA-IR, FBG, HbA1c, and fasting insulin) were collected at the endpoints and baseline of the study.
Risk of bias assessment
Two independent researchers (SM and NA) appraised the quality of the trials based on the modified Cochrane risk of bias (RoB 2) tool [43]. It identified possible causes of bias including attrition bias, performance bias, allocation bias, reporting bias, and detection bias. The RoB for each domain was deemed high, unclear, and low [43].
Certainty assessment
The certainty of the evidence was assessed by applying the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach, which categorizes the quality of evidence as moderate, very low, low, and high [44].
Statistical analysis
Meta-analysis was performed by applying the STATA statistical software (version 17). The effects of MP administration on the glycemic parameters were measured as a 95% confidence interval (CI) and weighted mean differences (WMDs) for total changes of trial outcomes from baseline to endpoints in the MP-treated and untreated groups. The outcome measures were presented as standard deviation (SD) and mean. The effect sizes were determined by the mean differences. The following formula was applied to calculate SD changes from pre-to post-intervention: SD change = √ (SD2 baseline + SD2 final)– (2 × R correlation coefficient × SD baseline × SD final) [45]. The random-effects model was employed to calculate the pooled WMDs [46]. The heterogeneity among RCTs was evaluated by applying the I2 statistic [47] and Cochrane’s Q test. The I2 values 25–50%, < 25%, 50–75%, and > 75%, were considered as moderate, low, high, and very high heterogeneity between RCTs, respectively [48].
Sub-group analyses were applied to identify the possible sources of heterogeneity among the included RCTs. The analysis was based on baseline serum levels of the outcomes (HbA1c, fasting insulin, HOMA-IR, and FBG), trial duration (> 8 weeks vs. ≤ 8 weeks), the dose of MP supplement (≥ 60 g/d vs. 30–60 g/d vs. < 30 g/d), protein supplementation type (WP vs. CP vs. MP), gender (male vs. both female and male vs. female), and baseline BMI of participants (overweight (25–29.9 kg/m2) vs. obese(> 30 kg/m2) vs. normal (18.5–24.9 kg/m2)). Leave-one-out sensitivity analyses were utilized to determine the effect of each study on the overall analysis. In addition, funnel plots, Egger's [49], and Begg's tests [50] were employed to determine probable publication bias. In addition, a P-value less than 0.05 was reported as statistically significant. The fractional polynomial model was used to find the possible non-linear impacts of the dose of MP supplement (g/d) and the trial duration (weeks). In addition, meta-regression was performed to evaluate a dose–response slope for a potential linear relationship between effect sizes, trial length, and dose of MP supplement [51].
Results
Study selection
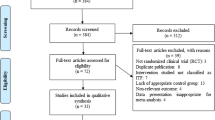
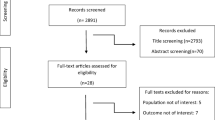
A primary search among multi-databases yielded 15,632 records. After excluding 5238 duplicate studies, 10,394 records were screened, and 10,287 citations were excluded based on their titles and abstracts. Full texts of 107 articles were assessed, and 36 eligible RCTs that met the inclusion criteria were analyzed in this study. A flowchart of the study selection and screening process is illustrated in Supplemental Fig. 1.
Study characteristics
The present systematic review and meta-analysis included 36 trials. Characteristics of the included RCTs are presented in Table 1. Thirty-four RCTs had parallel designs [52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85], while two were cross-over trials [86, 87]. The total number of participants in all trials was 1851 (MP supplement-treated group, n = 975; controls, n = 992), with mean age and BMI ranging from 18 to 85 years and 20 to 37 kg/m2, respectively. The sample sizes ranged from 16 to 171 participants. Twenty RCTs [52,53,54,55,56,57,58, 62, 63, 66, 70, 71, 74,75,76, 79, 80, 82, 83, 87] used a mixed-sex sample, while seven and nine studies had a women-only sample [64, 68, 69, 77, 78, 81, 86] or a men-only sample [59,60,61, 65, 67, 72, 73, 84, 85], respectively.
The trials enrolled patients with pre-or mild hypertension [52, 79], amyotrophic lateral sclerosis (ALS) [55], metabolic syndrome [58], after bariatric surgery (> 24 months) [69], hypoalbuminemia on peritoneal dialysis [70], T2DM [73, 76], and sarcopenic elderly men [67]. In addition, the RCTs were carried out among participants with overweight or obesity [53, 54, 56, 60, 61, 64,65,66, 75, 78, 80, 84], visceral fat [57], or abdominal obesity [83], and post-menopausal women [68] with overweight [86] or obesity [81]. The studies also included older women with sarcopenic obesity [77], futsal players [85], nursing home residents [62], elderly adults [63, 71, 82], and healthy individuals [59, 72, 74] with mildly elevated blood pressure (BP) [36].
The articles were published between 2007 and 2022. The RCTs were performed in Germany [52, 58], Australia [53, 56, 86], Netherlands [54], Brazil [55, 69, 77, 78], Japan [57], Portugal [85], Sweden [59, 84], and Iran [60, 61, 65, 81]. The settings of studies were also Finland [62], the Czech Republic [63], the United States(US) [64, 66, 68, 72, 74, 80, 82], the United Kingdom(UK) [87], Canada [67], Israel [70], Norway [71], New Zealand [73], Denmark [75, 83], Italy [76], and China [79]. The length of the trials was between 3 and 72 weeks and the doses of MP, WP, or CP supplements ranged from 3.5 to 90 g per day. The risk of bias evaluation among 36 RCTs is displayed in Supplemental Table 1.
The GRADE evaluation of the overall certainty of the evidence for the measured outcomes is summarized in Supplemental Table 2. The HbA1c outcome was downgraded to low quality due to serious limitations in inconsistency and imprecision. High certainty of evidence was allocated to fasting insulin outcome. In addition, moderate quality evidence was considered for FBG and HOMA-IR outcomes because of a very serious risk of inconsistency or serious limitations in publication bias and inconsistency, respectively.
Effect of supplementation with milk protein on serum FBG
Thirty-four RCTs (42 trial arms) [52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67, 69, 71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87] with 1731 participants (MP-treated group, n = 919; placebo group, n = 928) were included in this meta-analysis. The pooled analysis displayed that MP supplementation effectively reduced serum concentrations of FBG in the MP supplement-treated group compared with their untreated counterparts (WMD: -1.83 mg/dL, 95% CI: -3.28, -0.38; P = 0.01). In addition, there was considerable heterogeneity between trials (I2 = 88.3%, P < 0.001) (Fig. 1). Sub-group analyses explored that serum FBG levels were considerably reduced upon short-term administration (≤ 8 weeks) of a low daily dose of WP (< 30 g) among female participants with normal or overweight BMI and higher baseline FBG (> 100 mg/dL) (Table 2).

Forest plot for the effect of supplementation with milk protein on fasting blood glucose (FBG) (mg/dL). Horizontal lines represent 95% confidence intervals (CIs). Diamonds represent pooled estimates from random-effects analysis. The effect column comprises weighted mean differences (WMDs) and 95% CIs
Effect of supplementation with milk protein on fasting insulin
The effect of MP administration on serum fasting insulin values was evaluated in 20 RCTs [52,53,54, 57,58,59, 62, 64, 66, 67, 75,76,77,78, 80, 81, 83, 84, 86, 87] that involved 1100 participants (603 cases and 613 controls). A pooled analysis of 24 effect sizes indicated that the level of serum fasting insulin was considerably lower in the MP-treated group than in the control group (WMD: -1.06 uU/mL, 95% CI: -1.76, -0.36; P = 0.003). There was significant heterogeneity among RCTs (I2 = 50.1%, P = 0.003) (Fig. 2). Subgroup analyses depicted similar outcomes based on long-term supplementation with high or moderate daily doses of WP (≥ 60 or 30–60 g) among participants of both sexes (Table 2).

Forest plot for the effect of supplementation with milk protein on fasting insulin (uU/mL). Horizontal lines represent 95% confidence intervals (CIs). Diamonds represent pooled estimates from random-effects analysis. The effect column comprises weighted mean differences (WMDs) and 95% CIs
Effect of supplementation with milk protein on serum HbA1c
The meta-analysis of five studies (6 arms) [54, 57, 58, 70, 76] with 432 participants explored no significant changes in serum concentrations of HbA1c in the MP supplement-treated group compared to the untreated group (WMD: 0.01%, 95% CI: -0.14, 0.16; P = 0.89) with a high degree of heterogeneity between studies (I2 = 82%, P < 0.001) (Fig. 3). However, there was a substantial decline in serum levels of HbA1c among participants with normal baseline BMI based on sub-analyses (Table 2).

Forest plot for the effect of supplementation with milk protein on hemoglobin A1c (HbA1c) (%). Horizontal lines represent 95% confidence intervals (CIs). Diamonds represent pooled estimates from random-effects analysis. The effect column comprises weighted mean differences (WMDs) and 95% CIs
Effect of supplementation with milk protein on HOMA-IR
Seventeen trials [52, 54, 58, 59, 64, 66, 68, 69, 73, 76,77,78, 80, 81, 83, 84, 87] with 20 effect sizes and 940 participants revealed the impact of MP supplementation on HOMA-IR values. The meta-analysis displayed that the mean value of HOMA-IR was considerably lower in the experimental group than in the controls (WMD: -0.27, 95% CI: -0.40, -0.14; P < 0. 00.1) (Fig. 4). In addition, substantial heterogeneity was found between trials (I2 = 49.9%, P = 0.006). Subgroup analysis indicated that HOMA-IR values were significantly lower in the MP supplement-treated group than their untreated counterparts in short- and long-term supplementation (≤ 8 and > 8 weeks) with high or moderate doses (≥ 60 or 30–60 g/d) of MP or WP; similar outcomes were detected in subgroups including participants of both sexes with a normal or obese baseline BMI, and high or low baseline HOMA-IR values (> 2 or < 2) (Table 2).

Forest plot for the effect of supplementation with milk protein on homeostasis model assessment of insulin resistance (HOMA-IR). Horizontal lines represent 95% confidence intervals (CIs). Diamonds represent pooled estimates from random-effects analysis. The effect column comprises weighted mean differences (WMDs) and 95% CIs
Publication bias
Visual inspection of the funnel plots displayed different degrees of asymmetry for all assessed outcomes (Supplemental Fig. 2). There was no publication bias for FBG, HbA1c, or fasting insulin outcomes based on Begg’s and Egger's tests. However, there was publication bias for the HOMA-IR outcome (P = 0.033) according to Egger's test.
Linear and non-linear dose–response relations
There was no linear (Supplemental Figs. 5 and 6) or non-linear (Supplemental Figs. 3 and 4) relationship between changes in trial duration or doses of MP supplement and serum HbA1c values based on the dose–response assessment. There was a substantial non-linear association between changes in the duration of the intervention and serum levels of FBG (P = 0.005; Supplemental Fig. 4A) and fasting insulin (P = 0.03, Supplemental Fig. 4B), as well as between doses of MP supplements and changes in HOMA-IR values (P = 0.02; Supplemental Fig. 3D).
Sensitivity analysis
Excluding any specific study did not affect the evaluated outcomes (values of fasting insulin, HOMA-IR, HbA1c, and FBG) based on sensitivity analysis.
Discussion
This dose–response meta-analysis of 36 RCTs evaluated the impact of MP administration on the glycemic parameters in adults. It was indicated that supplementation with milk protein effectively reduced the levels of HOMA-IR, fasting insulin, and FBG while making no remarkable changes in serum HbA1c values. However, there was a significant decline in serum levels of HbA1c among participants with normal baseline BMI based on sub-analyses.
A subgroup analysis revealed that HOMA-IR values were significantly lower in the MP supplement-treated group than their untreated counterparts in short- and long-term supplementation (≤ 8 and > 8 weeks) with high or moderate doses (≥ 60 or 30–60 g/d) of MP or WP; similar outcomes were detected in subgroups among participants of both sexes with a normal or obese baseline BMI, and high or low baseline HOMA-IR values (> 2 or < 2). In addition, it explored that serum FBG levels were considerably reduced upon short-term administration (≤ 8 weeks) of a low daily dose of WP (< 30 g) among female participants with normal or overweight BMI, and higher baseline FBG (> 100 mg/dL). Furthermore, the levels of serum fasting insulin were remarkably decreased during long-term supplementation with high or moderate daily doses of WP among participants of both sexes. The dose–response assessment showed a significant non-linear relationship between changes in the intervention duration and serum concentrations of FBG and fasting insulin, as well as between doses of MP supplements and changes in HOMA-IR values.
This meta-analysis suggests that supplementation with MP could significantly ameliorate some glycemic parameters (fasting insulin, HOMA-IR, and FBG) of adults. However, the improvements were relatively small and might not be clinically significant. The minimum clinically important difference (MCID) for FBG and HA1C is between ≥ 14 and ≥ 0.5% mg/dL, respectively [88, 89]. The hypoglycemic effects of MP supplements are lower than MCID, which means that the impact is clinically insignificant.
A meta-analysis of 22 RCTs indicated that WP administration significantly decreased the values of HOMA-IR, HBA1c, and fasting insulin in patients with metabolic syndrome, but did not have any impact on FBG levels [90]. A systematic review of 58 RCTs explored that WP exerts a significant impact on glycemic control primarily by stimulating incretins and insulin secretion, suppressing appetite, and slowing down gastric emptying [39]. In addition, a comprehensive review of the literature stated the positive impacts of WP supplementation on improving postprandial glycemic control in the short term based on a few studies [91]. Another meta-analysis of five RCTs revealed that premeal WP supplementation is beneficial to ameliorate postprandial glycemia in patients with well-controlled or mild T2DM without significant adverse effects [37]. Some observational studies have reported a negative correlation between milk consumption and hyperglycemia [92, 93]. A prospective study displayed that a higher intake of dairy products was related to a lower 9-year incidence of hyperglycemia [92]. Another prospective cohort study among 15,512 adults in China (median follow-up of 9 years) declared that dairy consumption such as liquid milk and milk powder, was inversely associated with reduced diabetes risk [93]. However, most previous interventional trials failed to highlight the findings from observational studies regarding supplementation with MP.
It has been revealed that the insulinotropic impact of MP is related to certain AAs, in particular BCAAs [94]. Leucine induces glutamate dehydrogenase activity in β-cells that leads to an enhancement in Krebs cycle activity and insulin production [95]. In addition, WP as a fast digestible protein and a remarkable source of BCAAs promotes the circulation and release of insulin that may reduce postprandial hyperglycemia [90]. Bioactive peptides also induce the release of incretin hormones including glucagon‐like peptide‐1 (GLP‐1) and glucose-dependent insulinotropic polypeptide (GIP) that play a significant role in the enhancement of insulin resistance [96].
The maintenance of glucose levels involves a complex interaction between insulin-sensitive peripheral tissues and pancreatic β-cells [97]. The AAs are vital nutrients that may induce a diversity of indirect and direct impacts at the organismal and cellular levels [97]. However, there is a debate regarding the optimal amount of dietary protein for T2DM patients [97, 98]. It has been proposed that excessive amounts of AAs may reduce insulin-stimulated glucose uptake and increase insulin resistance [97]. A meta-analysis of eight RCTs explored that the consumption of proteins, particularly animal proteins, may be associated with an increased risk of T2DM [99].
The current study demonstrated a considerable reduction in serum FBG levels in RCTs that were short-term interventions with low-dose WP administration. Previous studies have revealed that the short-term effects of WP supplementation were equivalent to insulin therapy or sulfonylurea for the treatment of hyperglycemia in T2DM patients [28, 100, 101]. These promising results have only been displayed in short-term clinical trials. Therefore, short-term epidemiological and clinical evidence suggests that dairy proteins may ameliorate hyperglycemia. Although the outcomes of the present study proposed that the insulin-lowering effects of MP supplements are more efficient at higher doses and long-term interventions, further long-term RCTs are essential to confirm the proper efficacy, safety, and dosage of consistent consumption of MP supplements.
There were several strengths in the present systematic review and meta-analysis. This study is the first dose–response meta-analysis to evaluate the impact of supplementation with MP on the glycemic profile of adults. There was no restricted search period for selecting all eligible RCTs in a systematic search. In addition, a considerable number of studies were included in the analysis. Most of the RCTs in this meta-analysis had good or fair quality. Several limitations to the outcomes of this study should be considered. Dietary protein and carbohydrate intakes of participants were not reported in the majority of studies. The included RCTs in this meta-analysis had different control or non-intervened groups. Furthermore, there was considerable heterogeneity between trials related to each outcome. Therefore, a pre-defined subgroup analysis was employed to identify the cause of heterogeneity based on several variables, including supplement dose, intervention length, baseline BMI, baseline glycemic status, and gender of participants.
In conclusion, supplementation with MP may ameliorate the glycemic profile in adults by reducing the values of HOMA-IR, FBG, and fasting insulin. However, glycemic changes following MP administration were lower than MCID; therefore, its hypoglycemic effects were minor and may not reach clinical importance. Additional RCTs with longer durations are expected to confirm these findings.
Availability of data and materials
The datasets analyzed during the current study are presented in the manuscript.
Abbreviations
- RCT:
-
Randomized controlled trial
- FBG:
-
Fasting blood glucose
- HbA1c:
-
Hemoglobin A1c
- HOMA-IR:
-
Homeostasis model assessment of insulin resistance
- T2DM:
-
Type 2 diabetes mellitus
- HBG:
-
High blood glucose
- CVDs:
-
Cardiovascular diseases
- CHO:
-
Carbohydrates
- GI:
-
Glycemic index
- WP:
-
Whey protein
- CP:
-
Casein Protein
- MP:
-
Milk Protein
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- MeSH:
-
Medical subject headings
- RoB:
-
Risk of bias
- WMD:
-
Weighted mean difference
- SD:
-
Standard deviation
- CI:
-
Confidence interval
- ALS:
-
Amyotrophic lateral sclerosis
- GRADE:
-
Grading of recommendations assessment, development, and evaluation
- MCID:
-
Minimum clinically important difference
- BMI:
-
Body mass index
- PROSPPERO:
-
International prospective register of systematic reviews
References
Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al KJ. Epidemiology of type 2 diabetes–global burden of disease and forecasted trends. J Epidemiol Global Health. 2020;10(1):107.
Korytkowski M, McDonnell ME, Umpierrez GE, Zonszein J. Patient guide to managing hyperglycemia (high blood sugar) in the hospital. J Clin Endocrinol Metab. 2012;97(1):27A–A28.
Aronson D. Hyperglycemia and the pathobiology of diabetic complications. Cardiovascular Diabetology: Clinical, Metabolic Inflammat Facets. 2008;45:1–16.
Giugliano D, Ceriello A, Esposito K. Glucose metabolism and hyperglycemia. Am J Clin Nutr. 2008;87(1):217S–S222.
Lemkes BA, Hermanides J, DeVries JH, Holleman F, Meijers JC, Hoekstra JB. Hyperglycemia: a prothrombotic factor? J Thromb Haemost. 2010;8(8):1663–9.
Munekawa C, Okada H, Hamaguchi M, Habu M, Kurogi K, Murata H, et al. Fasting plasma glucose level in the range of 90–99 mg/dL and the risk of the onset of type 2 diabetes: Population-based Panasonic cohort study 2. J Diabetes Investig. 2022;13(3):453–9.
Sarwar N, Aspelund T, Eiriksdottir G, Gobin R, Seshasai SRK, Forouhi NG, et al. Markers of dysglycaemia and risk of coronary heart disease in people without diabetes: Reykjavik prospective study and systematic review. PLoS Med. 2010;7(5):e1000278.
Jafar N, Edriss H, Nugent K. The effect of short-term hyperglycemia on the innate immune system. Am J Med Sci. 2016;351(2):201–11.
Jeon H-Y, Lee A-J, Ha K-S. Polymer-based delivery of peptide drugs to treat diabetes: normalizing hyperglycemia and preventing diabetic complications. BioChip J. 2022;16(2):111–27.
Shkembi B, Huppertz TJF. Glycemic Responses of Milk and Plant-Based Drinks: Food Matrix Effects. Foods. 2023;12(3):453.
Evert AB, Boucher JL, Cypress M, Dunbar SA, Franz MJ, Mayer-Davis EJ, et al. Nutrition therapy recommendations for the management of adults with diabetes. Diabetes Care. 2014;37(1):S120–43.
Asbaghi O, Ashtary-Larky D, Bagheri R, Moosavian SP, Olyaei HP, Nazarian B, et al. Folic acid supplementation improves glycemic control for diabetes prevention and management: a systematic review and dose-response meta-analysis of randomized controlled trials. Nutrients. 2021;13(7):2355.
Asbaghi O, Fouladvand F, Gonzalez MJ, Ashtary-Larky D, Choghakhori R, Abbasnezhad AJD, et al. Effect of green tea on glycemic control in patients with type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes Metab Syndr Clin Res Rev. 2021;15(1):23–31.
Nosratabadi S, Ashtary-Larky D, Hoseini F, Namkhah Z, Mohammadi S, Salamat S, et al. The effects of vitamin C supplementation on glycemic control in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab Syndr Clin Res Rev. 2023;17(8):102824.
Marangoni F, Pellegrino L, Verduci E, Ghiselli A, Bernabei R, Calvani R, et al. Cow’s milk consumption and health: a health professional’s guide. J Am Coll Nutr. 2019;38(3):197–208.
Huppertz T, Vasiljevic T. Understanding and improving the functional and nutritional properties of milk. Cambridge: Burleigh Dodds Science Publishing Limited; 2022. https://doi.org/10.1111/1471-0307.12870.
Romero-Velarde E, Delgado-Franco D, García-Gutiérrez M, Gurrola-Díaz C, Larrosa-Haro A, Montijo-Barrios E, et al. The importance of lactose in the human diet: Outcomes of a Mexican consensus meeting. Nutrients. 2019;11(11):2737.
Leary M, Tanaka H. Role of fluid milk in attenuating postprandial hyperglycemia and hypertriglyceridemia. Nutrients. 2020;12(12):3806.
Panahi S, El Khoury D, Kubant R, Akhavan T, Luhovyy BL, Goff HD, et al. Mechanism of action of whole milk and its components on glycemic control in healthy young men. 2014;25(11):1124-31.
Davoodi SH, Shahbazi R, Esmaeili S, Sohrabvandi S, Mortazavian A, Jazayeri S, et al. Health-related aspects of milk proteins. Iran J Pharm Res. 2016;15(3):573–91.
Nongonierma AB, FitzGerald RJ. Bioactive properties of milk proteins in humans: a review. Peptides. 2015;73:20–34.
Raikos V, Dassios T. Health-promoting properties of bioactive peptides derived from milk proteins in infant food: a review. Dairy Scie Technol. 2014;94:91–101.
Frid AH, Nilsson M, Holst JJ, Björck IM. Effect of whey on blood glucose and insulin responses to composite breakfast and lunch meals in type 2 diabetic subjects–. Am J Clin Nutr. 2005;82(1):69–75.
Horstman AM, Huppertz T. Milk proteins: Processing, gastric coagulation, amino acid availability and muscle protein synthesis. Crit Rev Food Sci Nutr. 2022;1–16. https://doi.org/10.1080/10408398.2022.2078782.
Pal S, Radavelli-Bagatini S, Hagger M, Ellis V. Comparative effects of whey and casein proteins on satiety in overweight and obese individuals: a randomized controlled trial. Eur J Clin Nutr. 2014;68(9):980–6.
Wilborn CD, Taylor LW, Outlaw J, Williams L, Campbell B, Foster CA, et al. The effects of pre-and post-exercise whey vs. casein protein consumption on body composition and performance measures in collegiate female athletes. J Sports Sci Med. 2013;12(1):74–9.
Kumar KS, Yatoo MI, Mohapatra RK, Dhama K. Major health effects of casein and whey proteins present in cow milk: a narrative review. Indian Vet J. 2021;98(11):09–19.
McGregor RA, Poppitt SD. Milk protein for improved metabolic health: a review of the evidence. Nutr Metab. 2013;10(1):1–13.
Hall W, Millward D, Long S, Morgan L. Casein and whey exert different effects on plasma amino acid profiles, gastrointestinal hormone secretion and appetite. Br J Nutr. 2003;89(2):239–48.
van Loon LJ, Kruijshoop M, Menheere PP, Wagenmakers AJ, Saris WH, Keizer HA. Amino acid ingestion strongly enhances insulin secretion in patients with long-term type 2 diabetes. Diabetes Care. 2003;26(3):625–30.
Petersen BL, Ward LS, Bastian ED, Jenkins AL, Campbell J, Vuksan V. A whey protein supplement decreases post-prandial glycemia. Nutr J. 2009;8:1–5.
Gunnerud U, Östman E, Björck I. Effects of whey proteins on glycaemia and insulinaemia to an oral glucose load in healthy adults; a dose–response study. Eur J Clin Nutr. 2013;67(7):749–53.
Akhavan T, Luhovyy BL, Panahi S, Kubant R, Brown PH, Anderson GH. Mechanism of action of pre-meal consumption of whey protein on glycemic control in young adults. J Nutr Biochem. 2014;25(1):36–43.
Almario RU, Buchan WM, Rocke DM, Karakas SE. Glucose-lowering effect of whey protein depends upon clinical characteristics of patients with type 2 diabetes. BMJ Open Diabetes Res Care. 2017;5(1):e000420.
King DG, Walker M, Campbell MD, Breen L, Stevenson EJ, West DJ. A small dose of whey protein co-ingested with mixed-macronutrient breakfast and lunch meals improves postprandial glycemia and suppresses appetite in men with type 2 diabetes: a randomized controlled trial. Am J Clin Nutr. 2018;107(4):550–7.
Hidayat K, Du X, Shi BM. Milk in the prevention and management of type 2 diabetes: the potential role of milk proteins. Diabetes Metab Res Rev. 2019;35(8):e3187.
Chiang S-W, Liu H-W, Loh E-W, Tam K-W, Wang J-Y, Huang W-L, et al. Whey protein supplementation improves postprandial glycemia in persons with type 2 diabetes mellitus: A systematic review and meta-analysis of randomized controlled trials. Nutr Res. 2022;104:44–54.
Pasin G, Comerford KB. Dairy foods and dairy proteins in the management of type 2 diabetes: a systematic review of the clinical evidence. Adv Nutr. 2015;6(3):245–59.
Nouri M, Gargari BP, Tajfar P, Tarighat-Esfanjani A. A systematic review of whey protein supplementation effects on human glycemic control: A mechanistic insight. Diabetes Metab Syndr. 2022;16(7):102540.
Metelli S, Chaimani A. Challenges in meta-analyses with observational studies. BMJ Ment Health. 2020;23(2):83–7.
Mariani AW, Pego-Fernandes PM. Observational studies: why are they so important? Sao Paulo Med J. 2014;132(1):1–2.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906.
Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. https://doi.org/10.1136/bmj.l4898.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–6.
Borenstein M, Hedges LV, Higgins JP, Rothstein HR. Introduction to meta-analysis. Hoboken: Wiley; 2009. https://doi.org/10.1002/9780470743386.
DerSimonian R, Laird N. Meta-analysis in clinical trials Control Clin Trials. Control Clin Trials. 1986;7(3):177–88.
Borenstein M, Hedges LV, Higgins JP, Rothstein HR. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synthesis Methods. 2010;1(2):97–111.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
Begg CB, Berlin JA. Publication bias: a problem in interpreting medical data. J R Stat Soc A Stat Soc. 1988;1MP supplementation on the glycemic parameters51(3):419–45.
Mitchell MN. Interpreting and visualizing regression models using Stata. College Station: Stata Press; 2012. https://doi.org/10.1111/1475-4932.12023.
Lee YM, Skurk T, Hennig M, Hauner H. Effect of a milk drink supplemented with whey peptides on blood pressure in patients with mild hypertension. Eur J Nutr. 2007;46(1):21–7.
Keogh JB, Clifton P. The effect of meal replacements high in glycomacropeptide on weight loss and markers of cardiovascular disease risk. Am J Clin Nutr. 2008;87(6):1602–5.
Claessens M, van Baak MA, Monsheimer S, Saris WH. The effect of a low-fat, high-protein or high-carbohydrate ad libitum diet on weight loss maintenance and metabolic risk factors. Int J Obes (Lond). 2009;33(3):296–304.
Silva LB, Mourão LF, Silva AA, Lima NM, Almeida SR, Franca MC Jr, et al. Effect of nutritional supplementation with milk whey proteins in amyotrophic lateral sclerosis patients. Arq Neuropsiquiatr. 2010;68(2):263–8.
Pal S, Ellis V, Dhaliwal S. Effects of whey protein isolate on body composition, lipids, insulin and glucose in overweight and obese individuals. Br J Nutr. 2010;104(5):716–23.
Takahira M, Noda K, Fukushima M, Zhang B, Mitsutake R, Uehara Y, et al. Randomized, double-blind, controlled, comparative trial of formula food containing soy protein vs milk protein in visceral fat obesity FLAVO study. Circ J. 2011;75(9):2235–43.
Gouni-Berthold I, Schulte DM, Krone W, Lapointe JF, Lemieux P, Predel HG, et al. The whey fermentation product malleable protein matrix decreases TAG concentrations in patients with the metabolic syndrome: a randomised placebo-controlled trial. Br J Nutr. 2012;107(11):1694–706.
Hambre D, Vergara M, Lood Y, Bachrach-Lindström M, Lindström T, Nystrom FH. A randomized trial of protein supplementation compared with extra fast food on the effects of resistance training to increase metabolism. Scand J Clin Lab Invest. 2012;72(6):471–8.
Sheikholeslami VD, Ahmadi Kani GF. Changes in antioxidant status and cardiovascular risk factors of overweight young men after six weeks supplementation of whey protein isolate and resistance training. Appetite. 2012;59(3):673–8.
Ahmadi Kani GF, Sheikholeslami-Vatani D. The Effects of whey protein isolate supplementation and resistance training on cardiovascular risk factors in overweight young men. J Isfahan Medical School. 2012;30:289–301.
Björkman M, Finne-Soveri H, Tilvis R. Whey protein supplementation in nursing home residents A randomized controlled trial. Europ Geriatric Medicine. 2012;3:161–6.
Rambousková J, Procházka B, Binder M, Anděl M. Vliv podávání tekutého mléčného nutričního doplňku se zvýšeným obsahem syrovátkových bílkovin na nutriční stav seniorů. Vnitřní lékařství. 2014;60(7–8):556–61.
Piccolo BD, Comerford KB, Karakas SE, Knotts TA, Fiehn O, Adams SH. Whey protein supplementation does not alter plasma branched-chained amino acid profiles but results in unique metabolomics patterns in obese women enrolled in an 8-week weight loss trial. J Nutr. 2015;145(4):691–700.
Tahavorgar A, Vafa MR, Shidfar F, Gohari M, Heydari I. Beneficial Effects of Whey Protein Preloads on some Cardiovascular Diseases Risk Factors of Overweight and Obese Men are Stronger than Soy Protein Preloads – A Randomized Clinical Trial. J Nutr Intermed Metab. 2015;2(3–4):69–75.
Arciero PJ, Edmonds RC, Bunsawat K, Gentile CL, Ketcham C, Darin C, et al. Protein-Pacing from Food or Supplementation Improves Physical Performance in Overweight Men and Women: The PRISE 2 Study. Nutrients. 2016;8(5):288.
Maltais ML, Ladouceur JP, Dionne IJ. The effect of resistance training and different sources of Postexercise protein supplementation on muscle mass and physical capacity in Sarcopenic elderly men. J Strength Cond Res. 2016;30(6):1680–7.
Stojkovic V, Simpson CA, Sullivan RR, Cusano AM, Kerstetter JE, Kenny AM, et al. The Effect of Dietary Glycemic Properties on Markers of Inflammation, Insulin Resistance, and Body Composition in Postmenopausal American Women: An Ancillary Study from a Multicenter Protein Supplementation Trial. Nutrients. 2017;9(5):484.
Lopes Gomes D, Moehlecke M, Silva F, Dutra E, Schaan B, Carvalho K. Whey Protein Supplementation Enhances Body Fat and Weight Loss in Women Long After Bariatric Surgery: a Randomized Controlled Trial. Obes Surg. 2017;27(2):424–31.
Hassan K, Hassan F. Does whey protein supplementation affect blood pressure in hypoalbuminemic peritoneal dialysis patients? Ther Clin Risk Manag. 2017;13:989–97.
Ottestad I, Løvstad AT, Gjevestad GO, Hamarsland H, ŠaltytėBenth J, Andersen LF, et al. Intake of a Protein-Enriched Milk and Effects on Muscle Mass and Strength. A 12-Week Randomized Placebo Controlled Trial among Community-Dwelling Older Adults. J Nutr Health Aging. 2017;21(10):1160–9.
Lockwood C, Roberts M, Dalbo V, Smith-Ryan A, Kendall K, Moon J, et al. Effects of hydrolyzed whey versus other whey protein supplements on the physiological response to 8 weeks of resistance exercise in college-aged males. J Am Coll Nutr. 2016;36:1–12.
Gaffney KA, Lucero A, Stoner L, Faulkner J, Whitfield P, Krebs J, et al. Nil whey protein effect on glycemic control after intense mixed-mode training in type 2 diabetes. Med Sci Sports Exerc. 2018;50(1):11–7.
Sharp MH, Lowery RP, Shields KA, Lane JR, Gray JL, Partl JM, et al. The effects of beef, chicken, or whey protein after workout on body composition and muscle performance. J Strength Cond Res. 2018;32(8):2233–42.
Larsen AE, Bibby BM, Hansen M. Effect of a Whey Protein Supplement on Preservation of Fat Free Mass in Overweight and Obese Individuals on an Energy Restricted Very Low Caloric Diet. Nutrients. 2018;10(12):1918.
Derosa G, D’Angelo A, Maffioli P. Change of some oxidative stress parameters after supplementation with whey protein isolate in patients with type 2 diabetes. Nutrition. 2020;73:110700.
Nabuco HCG, Tomeleri CM, Fernandes RR, Sugihara Junior P, Cavalcante EF, Cunha PM, et al. Effect of whey protein supplementation combined with resistance training on body composition, muscular strength, functional capacity, and plasma-metabolism biomarkers in older women with sarcopenic obesity: A randomized, double-blind, placebo-controlled trial. Clin Nutr ESPEN. 2019;32:88–95.
Giglio BM, Schincaglia RM, da Silva AS, Fazani ICS, Monteiro PA, Mota JF, et al. Whey Protein Supplementation Compared to Collagen Increases Blood Nesfatin Concentrations and Decreases Android Fat in Overweight Women: A Randomized Double-Blind Study. Nutrients. 2019;11(9).
Yang J, Wang HP, Tong X, Li ZN, Xu JY, Zhou L, et al. Effect of whey protein on blood pressure in pre- and mildly hypertensive adults: a randomized controlled study. Food Sci Nutr. 2019;7(5):1857–64.
Hudson JL, Zhou J, Kim JE, Campbell WW. Incorporating Milk Protein Isolate into an Energy-Restricted Western-Style Eating Pattern Augments Improvements in Blood Pressure and Triglycerides, but Not Body Composition Changes in Adults Classified as Overweight or Obese: A Randomized Controlled Trial. Nutrients. 2020;12(3):851.
Haidari F, Aghamohammadi V, Mohammadshahi M, Ahmadi-Angali K, Asghari-Jafarabadi M. Whey protein supplementation reducing fasting levels of anandamide and 2-AG without weight loss in pre-menopausal women with obesity on a weight-loss diet. Trials. 2020;21(1):657.
Lefferts WK, Augustine JA, Spartano NL, Hughes WE, Babcock MC, Heenan BK, et al. Effects of Whey Protein Supplementation on Aortic Stiffness, Cerebral Blood Flow, and Cognitive Function in Community-Dwelling Older Adults: Findings from the ANCHORS A-WHEY Clinical Trial. Nutrients. 2020;12(4):1054.
Fuglsang-Nielsen R, Rakvaag E, Langdahl B, Knudsen KEB, Hartmann B, Holst JJ, et al. Effects of whey protein and dietary fiber intake on insulin sensitivity, body composition, energy expenditure, blood pressure, and appetite in subjects with abdominal obesity. Eur J Clin Nutr. 2021;75(4):611–9.
Pettersson S, Edin F, Hjelte C, Scheinost D, Wagner S, Ekblom B, et al. Six Weeks of Aerobic Exercise in Untrained Men With Overweight/Obesity Improved Training Adaptations, Performance and Body Composition Independent of Oat/Potato or Milk Based Protein-Carbohydrate Drink Supplementation. Front Nutr. 2021;8:617344.
Teixeira FJ, Matias CN, Faleiro J, Giro R, Pires J, Figueiredo H, et al. A Novel Plant-Based Protein Has Similar Effects Compared to Whey Protein on Body Composition, Strength, Power, and Aerobic Performance in Professional and Semi-Professional Futsal Players. Front Nutr. 2022;9:934438.
Pal S, Ellis V, Ho S. Acute effects of whey protein isolate on cardiovascular risk factors in overweight, post-menopausal women. Atherosclerosis. 2010;212(1):339–44.
Fekete ÁA, Giromini C, Chatzidiakou Y, Givens DI, Lovegrove JA. Whey protein lowers blood pressure and improves endothelial function and lipid biomarkers in adults with prehypertension and mild hypertension: results from the chronic Whey2Go randomized controlled trial. Am J Clin Nutr. 2016;104(6):1534–44.
Lenters-Westra E, Schindhelm R, Bilo H, Groenier K, Slingerland RJNJM. Differences in interpretation of haemoglobin A1c values among diabetes care professionals. Neth J Med. 2014;72(9):462–6.
Chan LSJAjoph. Minimal clinically important difference (MCID)—adding meaning to statistical inference. Am J Public Health. 2013;103(11):e24–25.
Amirani E, Milajerdi A, Reiner Ž, Mirzaei H, Mansournia MA, Asemi Z. Effects of whey protein on glycemic control and serum lipoproteins in patients with metabolic syndrome and related conditions: A systematic review and meta-analysis of randomized controlled clinical trials. Lipids Health Dis. 2020;19:1–18.
Giglio BM, Lobo PC, Pimentel GD. Effects of whey protein supplementation on adiposity, body weight and glycemic parameters: A synthesis of evidence. Nutr Metab Cardiovasc Dis. 2022;33(2):258–74.
Fumeron F, Lamri A, Abi Khalil C, Jaziri R, Porchay-Baldérelli I, Lantieri O, et al. Dairy consumption and the incidence of hyperglycemia and the metabolic syndrome: results from a French prospective study. Data Epidemiol Study Insulin Resistance Syndrome (DESIR). 2011;34(4):813–7.
Yang Y, Na X, Xi Y, Xi M, Yang H, Li Z, et al. Association between dairy consumption and the risk of diabetes: A prospective cohort study from the China Health and Nutrition Survey. Front Nutr. 2022;9:997636.
Lesgards J-F. Benefits of whey proteins on type 2 diabetes mellitus parameters and prevention of cardiovascular diseases. Nutrients. 2023;15(5):1294.
Tome D. Protein, amino acids and the control of food intake. Br J Nutr. 2004;92(S1):S27–30.
Adams RL, Broughton KS. Insulinotropic effects of whey: mechanisms of action, recent clinical trials, and clinical applications. Ann Nutr Metab. 2016;69(1):56–63.
Ancu O, Mickute M, Guess ND, Hurren NM, Burd NA, Mackenzie RW. Does high dietary protein intake contribute to the increased risk of developing prediabetes and type 2 diabetes? Appl Physiol Nutr Metab. 2021;46(1):1–9.
Hamdy O, Horton ES. Protein content in diabetes nutrition plan. Curr DiabRep. 2011;11:111–9.
Zhao L-G, Zhang Q-L, Liu X-L, Wu H, Zheng J-L, Xiang Y-B. Dietary protein intake and risk of type 2 diabetes: a dose–response meta-analysis of prospective studies. Eur J Nutr. 2019;58:1351–67.
Ma J, Stevens JE, Cukier K, Maddox AF, Wishart JM, Jones KL, et al. Effects of a protein preload on gastric emptying, glycemia, and gut hormones after a carbohydrate meal in diet-controlled type 2 diabetes. 2009;32(9):1600–2.
Jakubowicz D, Froy O, Ahrén B, Boaz M, Landau Z, Bar-Dayan Y, et al. Incretin, insulinotropic and glucose-lowering effects of whey protein pre-load in type 2 diabetes: a randomised clinical trial. Diabetologia. 2014;57(9):1807–11.
Funding
There was no specific funding for this research.
Author information
Authors and Affiliations
Contributions
DAL, SM, and OA prepared the study protocol. SM, SD, HSO, and NA contributed to the extraction, search of the data, and screening. OA conducted data analysis. SM and DAL provided the first draft of the manuscript. The last version of the manuscript has been read and accepted by all authors.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Supplemental Table 1. Risk of bias assessment for included RCTs in the meta-analysis. Supplemental Table 2. GRADE assessment. Supplemental Fig. 1. Flow diagram of study selection. Supplemental Fig. 2. Funnel plots for the effect of supplementation with milk protein on (A) fasting blood glucose (FBG) (B) fasting insulin (C) hemoglobin A1c(HbA1c), and (D) homeostasis model assessment of insulin resistance (HOMA-IR). Supplemental Fig. 3. Non-linear dose-response association between dose (gr/day) of supplementation with milk protein and absolute mean differences in (A) fasting blood glucose (FBG) (B) fasting insulin (C) hemoglobin A1c(HbA1c), and (D) homeostasis model assessment of insulin resistance (HOMA-IR). The 95% CI (confidence interval) is demonstrated in the shaded parts. Supplemental Fig. 4. Non-linear association between duration of the supplementation with milk protein (weeks) and absolute mean differences in (A) fasting blood glucose (FBG) (B) fasting insulin (C) hemoglobin A1c(HbA1c), and (D) homeostasis model assessment of insulin resistance (HOMA-IR). The 95% CI (confidence interval) is depicted in the shaded parts. Supplemental Fig. 5. Linear dose-response association between dose (gr/day) of supplementation with milk protein and absolute mean differences in (A) fasting blood glucose (FBG) (B) fasting insulin (C) hemoglobin A1c(HbA1c), and (D) homeostasis model assessment of insulin resistance (HOMA-IR). Supplemental Fig. 6. Linear association between duration of the supplementation with milk protein (weeks) and absolute mean differences in (A) fasting blood glucose (FBG) (B) fasting insulin (C) hemoglobin A1c (HbA1c), and (D) homeostasis model assessment of insulin resistance (HOMA-IR).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mohammadi, S., Asbaghi, O., Dolatshahi, S. et al. Effects of supplementation with milk protein on glycemic parameters: a GRADE-assessed systematic review and dose–response meta-analysis. Nutr J 22, 49 (2023). https://doi.org/10.1186/s12937-023-00878-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-023-00878-1