
Abstract
Background
Fruit, vegetable, and fruit juice intake is associated with the risk of gestational diabetes mellitus (GDM). However, the conclusion is limited and conflicted. The purpose of this systematic review and meta-analysis is to investigate the association between fruit, vegetable, and fruit juice consumption and the risk of GDM.
Methods
To find relevant studies, we searched PubMed, The Cochrane Library, Web of Science, Embase, ScienceDirect, PsycINFO, CINAHL, Ovid, EBSCO, CBM, CNKI, Wanfang Data, and VIP for the report on prospective cohort studies published from inception to April 8, 2022. Summary relative risks (RR) and 95% confidence intervals (Cis) were estimated using a random-effects model.
Results
A total of 12 studies with 32,794 participants were included in the meta-analysis. Total fruit consumption was associated with a lower risk of GDM (RR = 0.92, 95% CI = 0.86–0.99). Whereas an increasing the consumption of vegetable, including all vegetable (RR = 0.95, 95% CI = 0.87–1.03), starchy vegetable (RR = 1.01, 95% CI = 0.82–1.26), and fruit juice (RR = 0.97, 95% CI = 0.91–1.04) was not associated with a reduction in the risk of GDM. In a dose‒response analysis of eight studies, a 3% reduction in risk of GDM for a 100 g/d increase in fruit consumption (RR = 0.97, 95% CI = 0.96–0.99).
Conclusions
The findings suggest that higher fruit consumption may reduce the risk of GDM, with a 3% reduction in the risk of GDM for every 100 g/d increase in fruit intake. Higher-quality prospective studies or randomized clinical trials are required to validate the effect of different variations of fruits, vegetables, and fruit juice consumption on the risk of GDM.
Similar content being viewed by others


Introduction
Gestational diabetes mellitus (GDM) is an endocrine disorder in which abnormal blood glucose first occurs or is detected during pregnancy [1]. The International Diabetes Federation (IDF) estimates that 16.7% of women aged 10–49 years currently have GDM [2]. GDM is also linked to an increased risk of both short and long-term adverse pregnancy outcomes, including large birth weight, baby-obstructed labour, and type 2 diabetes mellitus (T2DM) in both mother and offspring [3]. The increased prevalence and adverse outcomes of GDM have caused a serious societal, economic, and health burden on both the population and individuals.
There is growing interest in the function of dietary behaviour and patterns in the development of chronic diseases [4, 5]. Fruit and vegetable consumption have been linked with a reduced incidence of cardiovascular diseases, metabolic syndrome, and type 2 diabetes [6, 7]. Fruit juices have become part of the daily diet and this is another important form of fruit intake. Many people try to supplement their daily fruit intake by drinking fruit juice. Drinking fruit juice may be an easy and effective way to reach your goal of 5 servings of fruit per day [8]. In another study, pregnant women reported a preference for drinking homemade fruit juice, and they believed the juice had more nutrients, such as vitamins and minerals, compared to whole fruit [9].The intake of fruits, vegetables, and fruit juices could explain some of the beneficial effects of the individual components and nutrients in the daily diet [10, 11]. Fruits and vegetables have anti-inflammatory properties and are rich in antioxidants, dietary fibre, and healthful phytochemicals [12, 13]. These compounds could improve insulin sensitivity by reducing pancreatic β cell apoptosis, muscular inflammation, and oxidative stress [14, 15].
The World Health Organization (WHO) suggests that consuming more than 400 g of different fruits and vegetables per day may reduce the incidence of diabetes [16]. Consumption of different types and amounts of fruits and vegetables could provide different levels of diabetes protection [17]. Evidence indicates that the Mediterranean diet (i.e.,vegetables and fruit-rich foods) could significantly reduce the development of GDM [18, 19]. Compared with a red-meat diet, vegetable and fruit-rich dietary patterns were linked to a reduced occurrence of impaired fasting glucose [20]. Consumption of fruit or green leafy vegetables is related to reduced risk of GDM [21, 22]. However, when compared to other cruciferous vegetables, legumes, or whole-grain foods, higher levels of potato consumption before pregnancy were found to be associated with a higher risk of GDM [23]. There is only one systematic review that indicated that fruit intake before pregnancy is associated with the risk of GDM, but this review did not assess the effects of vegetable or fruit juices on the incidence of GDM [24]. Therefore, based on the inconsistency among studies and to solve the limitations of the current review, we conducted a systematic review and meta-analysis to assess the effect of fruit, vegetable, and fruit juice intake on the risk of GDM and to assist in the exploration of dietary intervention strategies.
Methods
Search strategy
We conducted and reported this systematic review according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) 2020 statement (see online supplementary materials, Table S1). A comprehensive literature search was conducted in the following databases: PubMed, The Cochrane Library, Web of Science, Embase, Scopus, Ovid, EBSCO, Wanfang Data, CNKI, and VIP. There were no specified language restrictions. The database search was conducted from the database inception dates to April 8, 2022. During the retrieval process, MeSH terms were used as follows: “pregnancy or pregnant* or gestation*” and “vegetables or vegetable or fruits or fruit or vegetable juices or juice, vegetable or juices, vegetable or vegetable juice or fruit juices or juices, fruit”, and “diabetes, gestational or diabetes, pregnancy-induced or diabetes, pregnancy-induced or pregnancy-induced diabetes or gestational diabetes or diabetes mellitus, gestational or gestational diabetes mellitus” (see online supplementary materials, Table S2). References of original publications as well as previous meta-analyses or reviews were also manually reviewed.
Study selection and inclusion and exclusion criteria
Duplicate articles were removed in EndNoteX9. Two reviewers (Liao and Zheng) screened titles and abstracts to determine eligibility. Disagreements were adjudicated by a third reviewer (Jiang). Based on the title and abstract screening, the full-text articles of all the eligible studies were reviewed by Liao and Zheng.
Inclusion and exclusion criteria
The criteria of the included and excluded studies were guided by the PECOs. The following criteria were used to determine which studies to include in the meta-analysis. (1) Participants: eligibility criteria were restricted to pregnant adult women (18 years old and above); (2) Exposures: the intake of fruit, vegetables, and fruit juice was the exposure; (3) Outcomes: the GDM criteria included the following two methods: incident cases defined by self-reported clinical diagnosis of GDM or by meeting the criteria of either a fasting blood glucose concentration of 92 mg/dL, a 1-hour blood glucose concentration of 180 mg/dL, or a 2-hour blood glucose concentration of 153 mg/dL after a glucose tolerance test. (4) Study design: cohort studies. Studies that do not report relative risk and 95% confidence intervals for the relationship between fruit, vegetable, or/and fruit juice consumption and GDM risk were excluded.
Data extraction
The researchers extracted authors, year of publication, country/location, follow-up period, number of participants, number of GDM cases, age, pre-BMI, exposure (fruit/all vegetables/ starchy vegetable/fruit juice), assessment of GDM, exposure assessment, quality assessment score, and adjustments. The information was extracted by Liao and Zheng and any disagreements were solved through discussion with Jiang. When studies reported multivariate models, we included the highest exposure of the adjusted variables in the risk estimates.
Quality assessment
Evaluation of cohort studies was performed using the Newcastle‒Ottawa Scale (NOS) [25]. There are three categories and a maximum of nine points: (1) selection of populations; (2) comparability of the two groups; and (3) assessment of outcome. Studies with different points were divided into high quality (7–9 points), moderate quality (5–6 points), and poor quality (0–4 points). The quality of each study was assessed by Liao and Zheng, and any inconsistencies were discussed with Jiang. Studies was not excluded from the meta-analysis based on quality assessment scores.
Statistical analysis
STATA software version 16 was used for statistical analyses. For the meta-analysis, we used the study-specific relative risk (RR) and 95% confidence interval (Cis) for the highest versus lowest category of fruit, vegetables, and fruit juice intake with a random-effects model analysis. Statistical significance was defined as a two-tailed P value less than 0.05. The I2 (P < 0.1) and Q statistics were used to assess heterogeneity between studies. I2 values of 25%, 50%, and 75% represent low, moderate, and high heterogeneity, respectively. To investigate sources of heterogeneity, we conducted subgroup analyses by the period of dietary assessment (prepregnancy/first trimester/second trimester), location (Asia/Non-Asia), total number of participants (≥ 2000/<2000), number of GDM (≥ 500/<500), pre-BMI (< 25/≥25 kg/m2), parity-adjusted (yes/no), family history of diabetes-adjusted (yes/no), physical activity-adjusted (yes/no), smoking-adjusted (yes/no), alcohol-adjusted (yes/no). We assessed the stability of the study results by the trim and fill method in a sensitivity analysis or by excluding studies at a high risk of bias. Begg’s test and Egger’s test or funnel plot asymmetry were used to examine publication bias.
In the dose‒response analysis, we used generalized least squares to calculate study-specific slopes and 95% confidence intervals [26]. Statistical significance was defined as a P value of 0.05. For each category, the mean or median fruit, vegetable, and fruit juice intake were assigned to the appropriate RR for the individual study. We used the midpoint between the highest and lowest bounds in each category when the data on average consumption were not available. In an open category, if only the value of the highest category or the lowest category is known, we assume that the lowest bound is zero and the highest category bound is 1.5 times the lowest category [27, 28]. When the study used the number of servings to express the intake of vegetables and fruits, we normalized it to one serving equal to106 grams [29].

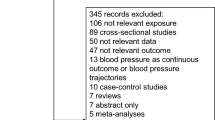
PRISMA flow chart of study selection

Forest plot of fruit, vegetable, fruit juice intake, and risk of GDM.

Dose-response analyses of fruit intake and risk of GDM.
Results
Study characteristics
The study selection process is shown in Fig. 1. In total, 701 articles were retrieved from 10 database searches. The eligibility of 320 articles was determined after removing duplicate publications. There were 51 studies eligible for full-text review, and 12 studies met the inclusion criteria. The study characteristics are summarized in Table 1. The studies were all cohort studies. The 12 studies were published between 2012 and 2021 and were conducted in eight countries, one was conducted in America [30], one in Australia [31], five in China [9, 32,33,34,35], one in Canada [36], two in Iran [37, 38], one in Iceland [39], and one in Malaysia [40]. Recruiting or follow-up periods ranged from one to 12 years. Two of these studies were from large cohort studies with longer recruitment times, resulting in the longer overall follow-up of the studies, and their study data results are only a portion of the large cohort studies [30, 36]. The period of dietary investigation for all the studies included three periods, four studies before pregnancy [30, 31, 37, 38], three studies in the first trimester [34,35,36], and five studies in the second trimester [9, 32, 33, 39, 40]. Eight studies provided information on fruit intake [9, 30,31,32,33, 35, 36, 38]. A total of seven studies reported on vegetable intake, of which four reported on all vegetables (including starchy vegetables and other vegetables) [31, 36, 38, 39], and three only reported on starchy vegetables [9, 34, 37]. Four studies reported on fruit juice intake [9, 30, 31, 40]. For the quality assessment, nine studies had a score of 6, indicating moderate quality [9, 30, 32,33,34,35, 37,38,39], and three studies had a score of 7, indicating high quality [31, 36, 40].
Fruit consumption and risk of GDM
A total of eight studies involving 2,809 GDM outcomes and 28,604 participants reported an association between fruit consumption and GDM [9, 30,31,32,33, 35, 36, 38]. Summarizing all eight comparisons with a random effects model, fruit intake was inversely associated with the risk of GDM (RR = 0.92; 95% CI: 0.86–0.99). Participants in the highest intake quartile had an 8% lower risk of developing GDM than those in the lowest intake quartile. There was low heterogeneity among studies (P = 0.14, I2 = 36.0%) (Fig. 2; Table 2). Fruit intake increased by 100 g per day was linked to a 3% lower risk of GDM in a dose‒response meta-analysis (RR = 0.97, 95% CI: 0.96–0.99) (Fig. 3).
Vegetable consumption and risk of GDM
A total of seven studies involving 2,132 GDM outcomes and 13,212 participants reported a link between vegetable consumption and GDM risk [9, 31, 34, 36,37,38,39]. The results indicated that there was no relationship between the intake of various types of vegetables and the risk of developing GDM. Four of these studies investigated the intake of all vegetables (including starchy vegetables and other vegetables) (RR = 0.95; 95% CI: 0.87–1.03) [31, 36, 38, 39] and three studies determined the intake of starchy vegetables (RR = 1.01; 95% CI: 0.82–1.26) [9, 34, 37] (Fig. 2; Table 2). Studies showed significant heterogeneity (all vegetables: P = 0.23, I2 = 61.3%; starchy vegetables: P = 0.90, I2 = 63.7%) (Fig. 2; Table 2). No correlation between the incidence of GDM and a 100 g/day increase in all vegetable intake (RR = 1.00, 95% CI: 0.99-1.00) and starchy vegetable intake (RR = 0.97, 95% CI: 0.93–1.01) was detected in dose‒response study (see online supplementary materials, Figure S1, S2).
Fruit juice consumption and risk of GDM
In four studies, 1,598 people with GDM outcomes and 23,177 participants showed an association between fruit juice intake and the risk of GDM [9, 30, 31, 40]. No relationship was identified between fruit juice intake and the risk of developing GDM (RR = 0.97; 95% CI: 0.91–1.04). Low heterogeneity was detected among studies (P = 0.23, I2 = 29.8%) (Fig. 2; Table 2). There was no linear relationship between each 100 ml/day increase in fruit juice consumption and the risk of GDM based on a dose‒response analysis (RR = 1.01, 95% CI: 0.97–1.08; see online supplementary materials, Figure S3).
Subgroup analysis and sensitivity analysis
Table 3 summarizes the results of the subgroup analysis according to several research characteristics. Subgroup analyses according to country/location (Asia/non-Asia) and parity-adjusted (yes/no) reduced the heterogeneity of the association between the consumption of fruit and GDM. We also assessed the period of dietary assessment (prepregnancy/first trimester/second trimester), the total number of participants (≥ 2000/<2000), the number of GDM patients (≥ 500/<500), pre-BMI (< 25/≥25 kg/m2), and adjustment factors such as parity (yes/no), family history of diabetes-adjusted (yes/no), physical activity (yes/no), smoking status (yes/no), and alcohol consumption (yes/no). Although statistically nonsignificant, some of the subgroups changed the effect size dramatically, such as the period of dietary assessment (prepregnancy), pre-BMI (≥ 25 kg/m2), and parity-adjusted (yes). As a result of the sensitivity analysis, the summary RRs for fruit, vegetable, and juice intake and GDM are as follows. Fruit intake: ranged from 0.92 (95% CI: 0.86–0.99) to 0.92 (95% CI: 0.85–0.98); all vegetable intake: ranged from 0.96 (95% CI: 0.90–1.03) to 0.98 (95% CI: 0.90–1.06); starchy vegetable intake: ranged from 0.78 (95% CI: 0.32–1.90) to 1.04 (95% CI: 0.97–1.13); fruit juice intake ranged from 0.97 (95% CI: 0.91–1.04) to 0.96 (95% CI: 0.90–1.03). Associations did not change considerably from the summary results (see online supplementary materials, Figure S4-S6).
Publication bias
Based on the funnel plot, Begg’s tests (see online supplementary materials, Figure S6-S8), and Egger tests, no significant publication bias was found (fruit: PBegg= 0.216 and PEgger=0.191; all vegetable: PBegg=0.174 and PEgger=0.060; starchy vegetable: PBegg=0.602 and PEgger=0.622; fruit juice: PBegg=0.497 and PEgger=0.874) (Table 2).
Discussion
The risk of GDM was inversely related to fruit consumption in this meta-analysis of 12 cohort studies, but no association was found between vegetables, fruit juices, and GDM. Moreover, a dose‒response analysis found that every 100 g of fruit per day reduced the risk of GDM by 3%. These findings offer support for the positive effects of moderate fruit intake on human health.
Studies have shown that fruit can reduce diabetes risk [41]. In regard to the relationship between diabetes and fruit consumption, there may be variations between different types of fruit. Rine et al. found that total fruit (apples, pears, blueberries, and grapes) and fruit combined with vegetables were related to a reduced risk of T2DM [42]. However, Wu-Qing Huang et al. found excessive intake (419 g/d) of tropical and citrus fruits, and fruits with a moderate or high glycaemic index (GI) increased the risk of GDM. The recommended intake of fruit during pregnancy is 200–400 g in China [32]. Studies have shown that most people currently fall short of the recommended daily intake of fruit [43, 44]. The average intake of fruit in this review was 220 g per day, which met the recommended intake. Thus, different fruit intakes could explain the inconsistent results of these studies. There are polyphenols, and antioxidant compounds in fruit, such as carotenoids and vitamins C and E. These compounds alleviate oxidative stress in cells that interfere with glucose uptake and prevent the development of abnormal glucose tolerance [45]. The fibre in fruits and vegetables can delay the absorption of carbohydrates from food and prevent a rapid rise in blood sugar [46]. The high fructose content of fruits is associated with impaired function of pancreatic β-cells and decreased insulin sensitivity [47,48,49]. The beneficial effects of fruits are determined not only by the effectiveness of specific micronutrients, but also by the combined action of many plant compounds. The high fructose content of fruits can be counteracted by the beneficial effects of fibre and other antioxidants [32]. Therefore, future studies can investigate the relationship between fruit intake and GDM risk through different types of fruit with different glycaemic indexs.
We found that vegetable intake and fruit juice were not significantly linked to the risk of GDM in this meta-analysis. Studies have reported that a diet pattern rich in vegetables and soy products can reduce the risk of GDM. For every one-quarter increase in vegetable pattern score, the risk of GDM was reduced by 3% [50]. Increased vegetable consumption may increase dietary fibre consumption and reduce fat intake, and is associated with a reduced risk of GDM [50, 51]. In this study, no association was found between the consumption of all vegetables (including starchy vegetables and other vegetables) or starchy vegetables and the risk of developing GDM. However, the study by Li et al. suggested that the total prepregnancy consumption of starchy vegetables, such as potatoes, was positively related to the risk of developing GDM [34]. Potatoes and other starchy vegetables are good quality carbohydrates and can be used as a substitute for a staple food [52]. The excessive intake of starchy vegetables can lead to a rapid rise in blood glucose after meals, which can damage pancreatic β-cells and increase the risk of GDM in the long term [53, 54]. Studies have shown that the risk of GDM increased by 8% for each additional serving of baked and boiled potatoes and French fries consumed [23]. The nutrients and biological effects of different types and cooking methods of vegetables play different roles in regulating blood glucose and insulin concentrations [55]. There is still a need for more research to assess the association with the risk of GDM based on the intake of some specific vegetables such as starchy and non-starchy vegetables, and leafy vegetables and legumes.
The fibre in the fruit juice is decreased and the sugar content are increased due to the commercial manufacturing process [56]. The study by Imamura et al. found that the consumption of artificially made sweet drinks and fruit juices was positively associated with the development of diabetes. [57]. Compared to pure fruit juice, fruit juice with added sugar increases the incidence of T2DM [58]. In addition, dietary guidelines in the United States indicate that consuming 75–224 ml of juice per day does not increase the risk of T2DM, cardiovascular and other diseases. In contrast, some short-term studies have found regular consumption of juice to be beneficial for cardiovascular health and blood pressure control [59]. Excess sugar in sweetened fruit juices can add to the body’s burden of regulating blood sugar, leading to a glycaemic load. The inconsistencies and bias between studies may be because most studies did not differentiate between pure fruit juice and sugar-sweetened juice [8]. In addition, compared to eating whole fruit, fruit juices can lead to overconsumption of fruit due to the lack of crude fibre, which has a satiating effect [60].
These results need to be interpreted with caution due to the lack of analysis of different types of fruits, vegetables, and juices. In the future, the relationship between fruits, vegetables, and juices needs to be further investigated by different subtypes.
Strengths and limitations
To interpret the findings appropriately, it is important to acknowledge this study’s limitations. Owing to a limited number of included studies and low reported intakes of certain fruits, vegetables, and fruit juices, this study did not carry out a specific analysis of the impact of specific fruits, vegetables, and fruit juices on the risk of GDM. Furthermore, the description of the cooking method and fruit juice and whether sugar was added not specified. Although subgroup analyses were performed to adjust for confounding factors that may influence the occurrence of GDM, residual confounding factors such as the history of endocrine disease and mode of conception may still be present. The majority of studies used a food frequency scale (FFQ) and dietary records to estimate dietary intake. Dietary assessments based on FFQ may have recall bias and do not provide a detailed record of daily changes in food intake. The FFQ can reflect food intake over time. The dietary record provides a more objective picture of eating habits and detailed food preparation methods, mitigating interindividual differences but requiring a more detailed record and a higher level of compliance [61, 62]. Indeed, some health-related outcomes with GDM were poorly covered, and owing notably to rough estimates of the degree of fruit and vegetable processing, many associations were not reviewed systematically.
Conclusion
Based on the results of this meta-analysis, fruit consumption appears to be associated with a reduced risk of GDM, whereas vegetable and fruit juice consumption was not associated with the incidence of GDM. According to the results of dose response analyses, increasing fruit consumption by 100 g per day reduced the risk of GDM by 3%. This suggests that people can reduce their risk of GDM by consuming moderate amounts of fresh fruit every day. Therefore, more high-quality, large-sample studies are needed to further investigate the relationship between different varieties of fruits, vegetables, and juices and the risk of GDM.
Data Availability
Not applicable.
References
Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(1):81–90. https://doi.org/10.2337/dc14-S081.
International Diabetes Federation. IDF Diabetes Atlas. 10th ed. Belgium, Brussels: International Diabetes Federation; 2021.
Mulla WR, Henry TQ, Homko CJ. Gestational diabetes screening after HAPO: has anything changed? Curr Diab Rep. 2010;10(3):224–8. https://doi.org/10.1007/s11892-010-0109-3.
Tian Y, Su L, Wang J, Duan X, Jiang X. Fruit and vegetable consumption and risk of the metabolic syndrome: a meta-analysis. Public Health Nutr. 2018;21(4):756–65. https://doi.org/10.1017/s136898001700310x.
Lee M, Lim M, Kim J. Fruit and vegetable consumption and the metabolic syndrome: a systematic review and dose-response meta-analysis. Br J Nutr. 2019;122(7):723–33. https://doi.org/10.1017/s000711451900165x.
Lamb MJ, Griffin SJ, Sharp SJ, Cooper AJ. Fruit and vegetable intake and cardiovascular risk factors in people with newly diagnosed type 2 diabetes. Eur J Clin Nutr. 2017;71(1):115–21. https://doi.org/10.1038/ejcn.2016.180.
Arnotti K, Bamber M. Fruit and Vegetable Consumption in overweight or obese individuals: a Meta-analysis. West J Nurs Res. 2020;42(4):306–14. https://doi.org/10.1177/0193945919858699.
Benton D, Young HA. Role of fruit juice in achieving the 5-a-day recommendation for fruit and vegetable intake. Nutr Rev. 2019;77(11):829–43. https://doi.org/10.1093/nutrit/nuz031.
Li H, Xie S, Zhang X, Xia Y, Zhang Y, Wang L. Mid-pregnancy consumption of fruit, vegetable and fruit juice and the risk of gestational diabetes mellitus: a correlation study. Clin Nutr ESPEN. 2021;46(1):505–9. https://doi.org/10.1016/j.clnesp.2021.08.033.
O’Neil CE, Nicklas TA, Rampersaud GC, Fulgoni VL 3. 100% orange juice consumption is associated with better diet quality, improved nutrient adequacy, decreased risk for obesity, and improved biomarkers of health in adults: National Health and Nutrition Examination Survey, 2003–2006. Nutr J. 2012;11(1):1–10. https://doi.org/10.1186/1475-2891-11-107.
Hosseini B, Berthon BS, Saedisomeolia A, Starkey MR, Collison A, Wark PAB, et al. Effects of fruit and vegetable consumption on inflammatory biomarkers and immune cell populations: a systematic literature review and meta-analysis. Am J Clin Nutr. 2018;108(1):136–55. https://doi.org/10.1093/ajcn/nqy082.
Agha-Jaffar R, Oliver N, Johnston D, Robinson S. Gestational diabetes mellitus: does an effective prevention strategy exist? Nat reviews Endocrinol. 2016;12(9):533–46. https://doi.org/10.1038/nrendo.2016.88.
Saghafian F, Malmir H, Saneei P, Keshteli AH, Hosseinzadeh-Attar MJ, Afshar H, et al. Consumption of fruit and vegetables in relation with psychological disorders in iranian adults. Eur J Nutr. 2018;57(6):2295–306. https://doi.org/10.1007/s00394-018-1652-y.
Vinayagam R, Xu B. Antidiabetic properties of dietary flavonoids: a cellular mechanism review. Nutr metabolism. 2015;12(1):1–20. https://doi.org/10.1186/s12986-015-0057-7.
Kawser Hossain M, Abdal Dayem A, Han J, Yin Y, Kim K, Kumar Saha S, et al. Molecular Mechanisms of the Anti-Obesity and Anti-Diabetic Properties of Flavonoids. Int J Mol Sci. 2016;17(4):569–71. https://doi.org/10.3390/ijms17040569.
Li M, Fan Y, Zhang X, Hou W, Tang Z. Fruit and vegetable intake and risk of type 2 diabetes mellitus: meta-analysis of prospective cohort studies. BMJ Open. 2014;4(11):1–9. https://doi.org/10.1136/bmjopen-2014-005497.
Muraki I, Imamura F, Manson JE, Hu FB, Willett WC, van Dam RM, et al. Fruit consumption and risk of type 2 diabetes: results from three prospective longitudinal cohort studies. BMJ. 2013;347(1):1–15. https://doi.org/10.1136/bmj.f5001.
Olmedo-Requena R, Gómez-Fernández J, Amezcua-Prieto C, Mozas-Moreno J, Khan KS, Jiménez-Moleón JJ. Pre-Pregnancy Adherence to the Mediterranean Diet and Gestational Diabetes Mellitus: a case-control study. Nutrients. 2019;11(5):1–11. https://doi.org/10.3390/nu11051003.
Hassani Zadeh S, Boffetta P, Hosseinzadeh M. Dietary patterns and risk of gestational diabetes mellitus: a systematic review and meta-analysis of cohort studies. Clin Nutr ESPEN. 2020;36(1):1–9. https://doi.org/10.1016/j.clnesp.2020.02.009.
Zhang M, Zhu Y, Li P, Chang H, Wang X, Liu W, et al. Associations between dietary patterns and impaired fasting glucose in chinese men: a cross-sectional study. Nutrients. 2015;7(9):8072–89. https://doi.org/10.3390/nu7095382.
Alperet DJ, Butler LM, Koh WP, Yuan JM, van Dam RM. Influence of temperate, subtropical, and tropical fruit consumption on risk of type 2 diabetes in an asian population. Am J Clin Nutr. 2017;105(3):736–45. https://doi.org/10.3945/ajcn.116.147090.
Chen GC, Koh WP, Yuan JM, Qin LQ, van Dam RM. Green leafy and cruciferous vegetable consumption and risk of type 2 diabetes: results from the Singapore Chinese Health Study and meta-analysis. Br J Nutr. 2018;119(9):1057–67. https://doi.org/10.1017/s0007114518000119.
Bao W, Tobias DK, Hu FB, Chavarro JE, Zhang C. Pre-pregnancy potato consumption and risk of gestational diabetes mellitus: prospective cohort study. BMJ. 2016;352(1):1–8. https://doi.org/10.1136/bmj.h6898.
Mohammadi T, Irandoost P, Roshanravan N, Khamechi SP, Milajerdi A, Larijani B, et al. Is there any association between fruit consumption and the risk of gestational diabetes mellitus? A systematic review and meta-analysis. Complement Ther Med. 2020;54(1):1–7. https://doi.org/10.1016/j.ctim.2020.102445.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5. https://doi.org/10.1007/s10654-010-9491-z.
Orsini N, Li R, Wolk A, Khudyakov P, Spiegelman D. Meta-analysis for linear and nonlinear dose-response relations: examples, an evaluation of approximations, and software. Am J Epidemiol. 2012;175(1):66–73. https://doi.org/10.1093/aje/kwr265.
Aune D, Lau R, Chan DS, Vieira R, Greenwood DC, Kampman E, et al. Nonlinear reduction in risk for colorectal cancer by fruit and vegetable intake based on meta-analysis of prospective studies. Gastroenterology. 2011;141(1):106–18. https://doi.org/10.1053/j.gastro.2011.04.013.
Zhao W, Tang H, Yang X, Luo X, Wang X, Shao C, et al. Fish Consumption and Stroke Risk: a Meta-analysis of prospective cohort studies. J stroke Cerebrovasc diseases: official J Natl Stroke Association. 2019;28(3):604–11. https://doi.org/10.1016/j.jstrokecerebrovasdis.2018.10.036.
Dauchet L, Amouyel P, Hercberg S, Dallongeville J. Fruit and vegetable consumption and risk of coronary heart disease: a meta-analysis of cohort studies. J Nutr. 2006;136(10):2588–93. https://doi.org/10.1093/jn/136.10.2588.
Chen L, Hu FB, Yeung E, Tobias DK, Willett WC, Zhang C. Prepregnancy consumption of fruits and fruit juices and the risk of gestational diabetes mellitus: a prospective cohort study. Diabetes Care. 2012;35(5):1079–82. https://doi.org/10.2337/dc11-2105.
Looman M, Schoenaker D, Soedamah-Muthu SS, Geelen A, Feskens EJM, Mishra GD. Pre-pregnancy dietary carbohydrate quantity and quality, and risk of developing gestational diabetes: the australian Longitudinal Study on Women’s Health. Br J Nutr. 2018;120(4):435–44. https://doi.org/10.1017/s0007114518001277.
Huang WQ, Lu Y, Xu M, Huang J, Su YX, Zhang CX. Excessive fruit consumption during the second trimester is associated with increased likelihood of gestational diabetes mellitus: a prospective study. Sci Rep. 2017;7(1):1–11. https://doi.org/10.1038/srep43620.
Zhou X, Chen R, Zhong C, Wu J, Li X, Li Q, et al. Fresh fruit intake in pregnancy and association with gestational diabetes mellitus: a prospective cohort study. Nutrition. 2019;60(1):129–35. https://doi.org/10.1016/j.nut.2018.09.022.
Li F, Sun H, Dong HL, Zhang YQ, Pang XX, Cai CJ, et al. Starchy vegetable intake in the first trimester is associated with a higher risk of gestational diabetes mellitus: a prospective population-based study. J maternal-fetal neonatal Med. 2021;35(25):1–8. https://doi.org/10.1080/14767058.2021.1924144.
Sun H, Dong H, Zhang Y, Lan X, Pang X, Cai C, et al. Specific fruit but not total fruit intake during early pregnancy is inversely associated with gestational diabetes mellitus risk: a prospective cohort study. Public Health Nutr. 2021;24(13):4054–63. https://doi.org/10.1017/s1368980021001920.
Mercier R, Perron J, Weisnagel SJ, Robitaille J. Associations between fruit and vegetable intake and abnormal glucose tolerance among women with prior gestational diabetes mellitus. Eur J Nutr. 2019;58(2):689–96. https://doi.org/10.1007/s00394-018-1669-2.
Goshtasebi A, Hosseinpour-Niazi S, Mirmiran P, Lamyian M, Moghaddam Banaem L, Azizi F. Pre-pregnancy consumption of starchy vegetables and legumes and risk of gestational diabetes mellitus among tehranian women. Diabetes Res Clin Pract. 2018;139(1):131–8. https://doi.org/10.1016/j.diabres.2018.02.033.
Mirmiran P, Hosseinpour-Niazi S, Moghaddam-Banaem L, Lamyian M, Goshtasebi A, Azizi F. Inverse relation between fruit and vegetable intake and the risk of gestational diabetes mellitus. Int J Vitam Nutr Res. 2019;89(1–2):37–44. https://doi.org/10.1024/0300-9831/a000475.
Tryggvadottir EA, Medek H, Birgisdottir BE, Geirsson RT, Gunnarsdottir I. Association between healthy maternal dietary pattern and risk for gestational diabetes mellitus. Eur J Clin Nutr. 2016;70(2):237–42. https://doi.org/10.1038/ejcn.2015.145.
Yong HY, Mohd Shariff Z, Mohd Yusof BN, Rejali Z, Tee YYS, Bindels J, et al. Beverage Intake and the risk of gestational diabetes Mellitus: the SECOST. Nutrients. 2021;13(7):1–11. https://doi.org/10.3390/nu13072208.
Schwingshackl L, Hoffmann G, Lampousi AM, Knüppel S, Iqbal K, Schwedhelm C, et al. Food groups and risk of type 2 diabetes mellitus: a systematic review and meta-analysis of prospective studies. Eur J Epidemiol. 2017;31(5):363–75. https://doi.org/10.1007/s10654-017-0246-y.
Halvorsen RE, Elvestad M, Molin M, Aune D. Fruit and vegetable consumption and the risk of type 2 diabetes: a systematic review and dose-response meta-analysis of prospective studies. BMJ Nutr Prev health. 2021;4(2):519–31. https://doi.org/10.1136/bmjnph-2020-000218.
Li Y, Zhang D, Pagán JA. Social norms and the consumption of fruits and vegetables across New York City neighborhoods. J urban health: Bull New York Acad Med. 2016;93(2):244–55. https://doi.org/10.1007/s11524-016-0028-y.
Aune D, Giovannucci E, Boffetta P, Fadnes LT, Keum N, Norat T, et al. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. Int J Epidemiol. 2017;46(3):1029–56. https://doi.org/10.1093/ije/dyw319.
Khalil A, Gaudreau P, Cherki M, Wagner R, Tessier DM, Fulop T, et al. Antioxidant-rich food intakes and their association with blood total antioxidant status and vitamin C and E levels in community-dwelling seniors from the Quebec longitudinal study NuAge. Exp Gerontol. 2011;46(6):475–81. https://doi.org/10.1016/j.exger.2011.02.002.
Steinberg GR, Schertzer JD. AMPK promotes macrophage fatty acid oxidative metabolism to mitigate inflammation: implications for diabetes and cardiovascular disease. Immunol Cell Biol. 2014;92(4):340–5. https://doi.org/10.1038/icb.2014.11.
Jayaprakasam B, Vareed SK, Olson LK, Nair MG. Insulin secretion by bioactive anthocyanins and anthocyanidins present in fruits. J Agric Food Chem. 2005;53(1):28–31. https://doi.org/10.1021/jf049018+.
Johnson RJ, Segal MS, Sautin Y, Nakagawa T, Feig DI, Kang DH, et al. Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease. Am J Clin Nutr. 2007;86(4):899–906. https://doi.org/10.1093/ajcn/86.4.899.
Lai HT, Threapleton DE, Day AJ, Williamson G, Cade JE, Burley VJ. Fruit intake and cardiovascular disease mortality in the UK Women’s Cohort Study. Eur J Epidemiol. 2015;30(9):1035–48. https://doi.org/10.1007/s10654-015-0050-5.
Chen Q, Wu W, Yang H, Zhang P, Feng Y, Wang K, et al. A Vegetable Dietary Pattern is Associated with lowered risk of gestational diabetes Mellitus in Chinese Women. Diabetes & metabolism journal. 2020;44(6):887–96. https://doi.org/10.4093/dmj.2019.0138.
Galisteo M, Duarte J, Zarzuelo A. Effects of dietary fibers on disturbances clustered in the metabolic syndrome. J Nutr Biochem. 2008;19(2):71–84. https://doi.org/10.1016/j.jnutbio.2007.02.009.
Wang SS, Lay S, Yu HN, Shen SR, Dietary Guidelines for Chinese Residents. (2016): comments and comparisons. Journal of Zhejiang University Science B. 2016;17(9):649–656. https://doi.org/10.1631/jzus.B1600341.
Ceriello A, Esposito K, Piconi L, Ihnat MA, Thorpe JE, Testa R, et al. Oscillating glucose is more deleterious to endothelial function and oxidative stress than mean glucose in normal and type 2 diabetic patients. Diabetes. 2008;57(5):1349–54. https://doi.org/10.2337/db08-0063.
Riccardi G, Rivellese AA, Giacco R. Role of glycemic index and glycemic load in the healthy state, in prediabetes, and diabetes. Am J Clin Nutr. 2008;87(1):269–74. https://doi.org/10.1093/ajcn/87.1.269S.
Park S, Ham JO, Lee BK. Effects of total vitamin A, vitamin C, and fruit intake on risk for metabolic syndrome in korean women and men. Nutrition. 2015;31(1):111–8. https://doi.org/10.1016/j.nut.2014.05.011.
Mendez R, Grissom M. Disorders of childhood growth and development: childhood obesity. FP essentials. 2013;410(1):20–4.
Imamura F, O’Connor L, Ye Z, Mursu J, Hayashino Y, Bhupathiraju SN, et al. Consumption of sugar-sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: systematic review, meta-analysis, and estimation of population attributable fraction. BMJ. 2015;351(1):1–12. https://doi.org/10.1136/bmj.h3576.
Xi B, Li S, Liu Z, Tian H, Yin X, Huai P, et al. Intake of fruit juice and incidence of type 2 diabetes: a systematic review and meta-analysis. PLoS ONE. 2014;9(3):1–6. https://doi.org/10.1371/journal.pone.0093471.
Ruxton CHS, Myers M. Fruit Juices: are they helpful or harmful? An evidence review. Nutrients. 2021;13(6):1–14. https://doi.org/10.3390/nu13061815.
Ho K, Ferruzzi MG, Wightman JD. Potential health benefits of (poly)phenols derived from fruit and 100% fruit juice. Nutr Rev. 2020;78(2):145–74. https://doi.org/10.1093/nutrit/nuz041.
Mertens E, Kuijsten A, Geleijnse JM, Boshuizen HC, Feskens EJM, Van’t Veer P. FFQ versus repeated 24-h recalls for estimating diet-related environmental impact. Nutr J. 2019;18(1):1–12. https://doi.org/10.1186/s12937-018-0425-z.
Xue Y, Yang K, Wang B, Liu C, Mao Z, Yu S, et al. Reproducibility and validity of an FFQ in the Henan Rural Cohort Study. Public Health Nutr. 2020;23(1):34–40. https://doi.org/10.1017/s1368980019002416.
Acknowledgements
We give our thanks for the support from all the authors. All authors reviewed the manuscript and approved the final manuscript.
Funding
This work was supported by Joint funds project for science and technology innovation in Fujian (2020Y9133) and Hospital Fund from Fujian Maternity and Child Health Hospital (YCXH22-20).
Author information
Authors and Affiliations
Contributions
Yan-Ping Liao: study design and conduct, data collection and analysis, manuscript drafting and manuscript revision.Qing-Xiang Zheng: study design, data interpretation and manuscript revision.Xiu-Min Jiang: study design, data interpretation, and manuscript revision.Xiao-Qian Chen: data collection and manuscript revision.Xiao-Xia Gao: data collection.Yu-Qing Pan: data collection.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent for publication
All authors gave their consent for publication.
Ethical approval and Consent to participate
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liao, YP., Zheng, QX., Jiang, XM. et al. Fruit, vegetable, and fruit juice consumption and risk of gestational diabetes mellitus: a systematic review and meta-analysis. Nutr J 22, 27 (2023). https://doi.org/10.1186/s12937-023-00855-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-023-00855-8