
Abstract
Background
Food and nutrition literacy is a key factor in shaping healthy dietary behaviors and may result in decreasing decrease the prevalence of overweight. Empirical research on food and nutrition literacy and its outcomes is limited, especially among children and adolescents. Thus, this study investigates the link between Food and Nutrition Literacy (FNLIT) with eating behaviors, academic performance, and overweight in 10–12 years old students in Tehran, Iran.
Methods
This study was performed through two phases: 1) Proposing a conceptual model of the relationship between FNLIT and its determinants and outcomes, based on the existing evidence and previous models, and 2) Testing the proposed FNLIT model through a cross-sectional study on 803 primary school students (419 boys and 384 girls, from 34 public and 10 private primary schools), aged 10–12 years using structural equation modeling. Demographic, socio-economic, and household food security characteristics were collected by interviewing the students and their mothers/caregivers using a questionnaire. FNLIT was measured by a self-administered, locally designed, and validated questionnaire.
Results
The fit indices suggested a reasonably adequate fit of the data to the hypothesized model (χ2/df = 2.03, p < 0.001, goodness of fit index (GFI) = 0.90, adjusted goodness of fit index (AGFI) = 0.88, comparative fit index (CFI) = 0.91, incremental fit index (IFI) = 0.91, root mean square error of approximation (RMSEA) = 0.04, standardized root mean residual (SRMR) = 0.06). SES was directly and positively related to FNLIT and its subscale in students. FNLIT score had a positive direct (non-mediated) relationship with healthy eating behavior and academic performance. This pattern was strongly reversed in unhealthy eating behavior. There was a full mediation relationship between FNLIT and overweight/obesity via healthy eating behaviors. SES predicted academic performance partially through the mediating effect of Food Label Literacy (FLL). The results indicated that despite the direct relationship between SES and academic performance, an indirect but negative relationship existed with food insecurity.
The finding also revealed the fully mediating role of Food Choice Literacy (FCL) in the relationship between demographic factors and healthy eating behaviors. Our study also found that Interactive Food and Nutrition Literacy (IFNL) protected unhealthy eating behaviors, and FCL predicted healthy eating behaviors in children.
Conclusion
Our study draws attention to FNLIT, especially the skills domain, including IFNL, FCL, and FLL, as the most important determinant of healthy eating behavior, academic performance, and weight status in school-age children reduces social inequalities in children’s development.
To ensure an adequate level of FNLIT, educators should assess and plan to enhance food literacy skills in children and adolescents.
Similar content being viewed by others

Introduction
Factors contributing to poor dietary habits are complex, and improving eating behavior requires an interdisciplinary approach that acknowledges the social context [1]. Among the different factors affecting eating behaviors, food literacy has recently been considered a key factor in improving diet quality, health, and well-being [2]. Food literacy is a construct that affects an individual’s ability to assess food and nutrition information, comprehend food labels, perform food safety precautions, use healthy cooking methods, apply dietary recommendations and make healthy food choices [3,4,5]. It may be a key factor in shaping dietary behaviors, specifically in children and adolescents [6, 7]. Healthy eating behaviors are essential in maintaining physical health and promoting optimal learning and school achievement [8]. Food literacy may contribute to a person’s ability to feed themselves (and others) in a nutrition-promoting way [9]. Enhancing food literacy to decrease nutrition-related disease burden is a growing international role for public health practitioners. However, assessing the impact of food literacy programming and the link between food literacy and health outcomes is hindered by the lack of validated measurement tools [10].
Doustmohammadian et al. developed a validated FNLIT questionnaire that measures the key functional, interactive, and critical elements of FNLIT in 10–12 years old students [11]. Guided by Nutbeam’s hierarchical model of health literacy [12], food and nutrition literacy in children is consisted of cognitive domains, including Understanding Food and Nutrition Information (UFNI) and Nutritional Health Knowledge (NHK) and skill domain including Functional Food and Nutrition Literacy (FFNL), Interactive Food and Nutrition Literacy (IFNL) and Critical Food and Nutrition Literacy (CFNL).
Childhood is a unique life stage through which decision-making skills are developed. Food and nutrition literacy programs are ideal for this stage because they focus on building capacity to operationalize healthy decisions [13]. There have been few studies on food and nutrition literacy improvement among adolescents [7]. Several conceptual models targeting the adult population have been suggested that improving food literacy might influence eating behavior and well-being [5, 14].
However, empirical research on food and nutrition literacy and its outcomes is limited [6, 15]. Thus, any relationship between food literacy/nutrition literacy and eating behaviors, food insecurity, academic achievement, or other health outcomes targeting children needs to be clarified to inform stakeholders involved in intervention design and curriculum content in this age group. Structural equation modeling (SEM) is a set of linear simultaneous equations considered an appropriate statistical technique for identifying the direct and indirect (through mediators) relationship between potential and observed variables [16, 17]. In SEM, individual differences and errors are also taken into account, which provides a more in-depth insight into the assessment of FNLIT, its determinants, and outcomes [18]. To date, no studies have used the SEM approach in this field. Therefore, the current study aimed to investigate the association between Food and Nutrition Literacy (FNLIT) components and eating behaviors, academic achievement, and weight status using the statistical approach of structural equation modeling (SEM), in elementary school children in Tehran, Iran.
Conceptual framework
The conceptual framework of the study was proposed based on a review of prior evidence and previously described conceptual models on food/nutrition literacy (Fig. 1).

Proposed model of the relationship between FNLIT and its determinants and outcomes in 10–12 years old students. Arrows starting from the same determinant factors are in the same color
Linking food literacy/nutrition literacy to socio-demographic factors [19, 20], food security [21,22,23], weight status [24], and academic achievement [25] have been established in previous studies. The direct relationship between food or nutrition literacy and eating behaviors has been observed across several studies [6, 26, 27]. Chang et al. [28] theorized consumer capacities in the field of nutrition as factors that affect individuals’ food security and determined using a nutritional panel as a viable plan to reduce food insecurity. In addition, other studies focused on food literacy abstracted food security as a food literacy outcome [5, 6, 29,30,31,32,33,34]. They believed that the achievement of food literacy ensures access to a healthy diet. According to studies, food security is strongly related with children’s health and could affect anthropometrical indices [35, 36]. Other researchers have assessed the relationship between food insecurity, academic achievement, and anthropometric status in elementary school children [35]. On the other hand, Magulod et al. [37] reported anthropometric status and dietary behavior as determinants of academic achievement. The existing literature highlighted a moderate association between food consumption and behaviors on school performance among children [38].
Several proposed conceptual models or frameworks attempted to describe the relationship between food literacy, individual determinants, and outcomes related to health [5, 39,40,41,42,43,44,45,46]. Although food literacy has been presented as an essential factor for healthy food choices and a powerful resource to improve individual and public health, Vidgen and Gallegos (2014) found an indirect link between food literacy and healthy nutrition. They believe that food security and the ability to prepare food can enhance food choice and pleasure, stimulating healthy eating behavior [5]. In most conceptual frameworks, the authors have particularly focused on the sociocultural as well as environmental factors [5, 39,40,41,42,43,44].
Methods
Study design
This study used a population-based cross-sectional design, proposing a hypothesized model for explaining the relationship between FNLIT and its determinants and outcomes. Model fitness was addressed by testing the hypothesized conceptual model.
Settings and sample
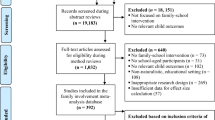
The study was performed from November 2015 to May 2017 in Tehran, the capital of Iran. The sampling frame can be seen in Fig. 2. The total eligible participants included 186,761 primary school children in the designated districts. Since there was no prior knowledge on the low FNLIT prevalence in primary school children to be estimated/examined for FNLIT, the P-value was 50% to obtain the highest P*(1-P) value for estimating the largest sample size. The sample size was determined to be at least 768 using the following formula, and 900 students were invited to increase statistical power further.

Study sampling frame
Finally, 803 students aged 10 to 12 years completed the survey (response rate = 89.2%, power = 88%). Time constraints were the main reason for non-participation. According to the general office of education in Tehran, there are three socioeconomic levels in 19-educational-districts of Tehran, namely affluent (north), semi-affluent (center), and deprived (south). A list of primary schools within the boundary of the mentioned districts provided by education department was used to start sampling. The students were selected through a three-stage cluster random sampling technique. Initially, according to the population density of the districts, nine districts (three from each socio-economic level) were selected. In the second stage, private and public schools were randomly allocated in each district with a probability proportional to the target sample size of each school. Finally, the students were randomly chosen from the fifth and sixth grades (aged 10–12 years) of the selected schools, and the ultimate participants were chosen from 34 public and 10 private primary schools. The excluded subjects’ characteristics did not differ significantly from those in the study.
Measurements
Food and nutrition literacy assessments
A valid self-administered questionnaire was applied to measure food and nutrition literacy in 10–12 years old students (details of its development and validation are explained elsewhere [11]). It was a 46-item questionnaire and included the cognitive and skill domains. Two sub-scales of Understanding Food and Nutrition Information (UFNI, 10 items) and Nutritional Health Knowledge (NHK, 5 items) were identified in the cognitive domain. The skill domain consisted of four sub-scales, including Functional Food and Nutrition Literacy (FFNL), Interactive Food and Nutrition Literacy (IFNL), Food Choice Literacy (FCL), and Critical Food and Nutrition Literacy (CFNL), encompassing ten, seven, six and four items each, respectively. Finally, Food Label Literacy (FLL) was evaluated by four dichotomous questions. Based on the characterized scores of low (≤51), medium (> 51- < 74), and high (≥74), the FNLIT score ranged between 25.8 and 96.8 [19].
Assessment of eating behavior
The research team developed the eating behavior questionnaire based on the previous questionnaires [8]. For qualitative content validity, a panel of six experts (three nutritionists, one health education and health promotion, one sociologist, and one social medicine) examined the initial questionnaire. Items were modified based on the experts’ comments. Then it was pretested on 30 students (15 boys and 15 girls) to assess the questions’ content and clarity, and the unclear items were reworded. Using the questionnaire, interviewers asked about the frequency of eating sweets and salty snacks, fast foods, energy-free beverages (water, coffee, tea), energy-containing beverages (soft drinks, juices), and meals during the previous week. The regularity of mealtime was evaluated according to frequency intake of breakfast, lunch, and dinner during the past 7-day and divided into four groups, including every day a week; 3–6 times a week; 1–2 times a week; and never. Consumption frequency of snacks was measured by a four-response scale: more than or equal to three times a day, twice a day, once a day, and never. The frequency of drinking water in a day was reported as four groups of ≥5 cups a day, 3–4 cups a day, 1–2 cups a day, and zero cup a day. The students were also questioned about the frequency of having drinks (e.g., tea/coffee/hot cacao, soft drinks, and fruit juices), fast foods (e.g., sausage/hamburger, pizza, fried potato, and restaurant foods/fast foods), and snacks (e.g., sweet and salty snacks) over the last 7 days. The possible responses included: ≥5 times a week, 3–4 times a week, 1–2 times a week, and never.
Food security status
The status of household food security was measured by the valid USDA’s Household Food Security Survey Module, which assessed the ability of the households to obtain and conserve food during the previous 12-month. The survey module was translated into Farsi and validated in the Iranian context [47, 48]. The USDA module consisted of 10 questions for households without and 18 questions for households with children and was completed face-to-face or by telephone with mothers. Based on the scale, the households were classified into four categories of food secure (FS) (raw score ranged between 0 and 2); food insecure (FI) without hunger (raw score ranged between 3 and 7); and food insecure (FI) with moderate hunger (raw score ranged between 8 and 12); food insecure with severe hunger (raw score ranged between 13 and 18). Due to the low prevalence of FI with moderate and severe hunger, they were pooled as one.
Academic achievement
The students’ teachers completed the author-designed questionnaire on academic achievement. Since children’s final grades were not available at the study time, this pretested, self-administered questionnaire was developed and used based on the teachers’ evaluations of the student’s achievement in class and with regard to the grades for mid-term assignments. The validity and consistency of the quantitative academic achievement were assessed using two evaluation approaches, including qualitative and quantitative. The teachers (n = 152) from 43 girls’ and boys’ primary schools assessed their students in math, reading, spelling, composition, science, and social-science using two scoring scales, including a quantitative scale of 0 to 20 points according to the grades attained in class and qualitative scale of 1 (very good) to 7 (very weak) points according to the teachers’ assessment of the student. The teachers were instructed to fill out the questionnaire.
Study covariates
Several baseline covariates, including age, birth order, family size, ethnicity, parental age, parental education, father’s job position, mother’s employment status, other income source(s) of family members, house ownership status, and receiving financial support were considered based on the available evidence [8, 49,50,51]. Anthropometric measurements were taken, and age-and sex- standardized BMIz-score was calculated based on World Health Organization Child Growth Standards (WHO AnthroPlus, 2007) [52]. The weight status of students was reported as thin (BMIz-score < −2SD), normal (BMIz-score ≥ −2SD and ≤ 1SD), overweight (BMIz-score > 1SD and ≤ 2SD) and obese (BMIz-score > 2SD). All participants (students and their parents) signed a written informed consent before the study.
The demographic and socioeconomic status were evaluated by a structured questionnaire through interviews with children and verified by their parents and/or caregivers after that. Parents completed the food security (FS) questionnaire through face-to-face interviews. Telephone interviews were conducted for those who could not attend schools (because of child care needs, illness, work constraints, etc.).
Statistical analysis
the Kolmogorov–Smirnov test was used to assess the normal distribution of data. Categorical variables were presented as frequencies and percentages and compared using by χ2 test. In the current study, the hypothesized model of direct and indirect associations among observed and latent variables was identified and evaluated through the following steps:
-
1.
Exploratory Factor Analysis (EFA)
EFA was used to explore two latent constructs of healthy and unhealthy eating behaviors. Principal Component Analysis (PCA) with orthogonal Varimax rotation was applied to estimate factor loadings influencing observed variables. Items with an absolute loading of 0.30 remained in the structural model of healthy and unhealthy eating behaviors.
-
2.
Confirmatory Factor Analysis (CFA)
The CFA method was applied to verify the measurement model of academic achievement and healthy and unhealthy eating behaviors by testing the association among the observed variables and their underlying latent construct (s).
-
3.
Structural equation modeling (SEM)
SEM was used to examine the multidirectional relationships and causal dependencies between a number of endogenous and exogenous variables of interest [53]. SEM also allows the construction of latent variables, which are not measured directly and estimated from measured variables [53]. The latent variables were demographic, socio-economic status, healthy and unhealthy eating behaviors, and academic achievement in the current study. Measurable variables were FNLIT, BMIzscore, and food insecurity. We calculated standardized regression weights, standardized total effects, direct and indirect effects. Model fit measures were used to assess how well the proposed model captured the covariance between all the model items or measures. Goodness-of-fit to ensure that the proposed model can adequately explain the data was assessed by several model fit indices including χ2, the ratio of the χ2 to degrees of freedom (CMIN/DF), goodness of fit index (GFI), Adjusted Goodness of Fit Index (AGFI), the Comparative Fit Index (CFI), the incremental fit index (IFI), the Root Mean Square Error of Approximation (RMSEA) and Standardised Root Mean Residual (SRMR). CFI > 0.90, RMSEA and SRMR≤0.10, and CMIN/DF < 4.0 are considered to represent an appropriate model fit to the data. For GFI, AGFI, and NFI, which range from 0 to 1.0, values > 0.90 show an appropriate model fit to the data [54]. Statistical significance of the direct effects, indirect effects, and total effects were evaluated using a bootstrapping procedure. The number of bootstrapping was set at 2000 times.
Statistical analyses were performed using SPSS 21.0 (SPSS Inc., Chicago, Illinois, and the United States) and AMOS 21.0 [55]. All P-values were two-tailed, and P-values < 0.05 were considered statistically significant.
Results
Demographic and socio-economic characteristics of the study participants
A total of 803 students (419 boys and 384 girls) participated in the study. The mean age of students was 11.28 ± 0.65 years.
Girls and boys significantly differed in some demographic and socio-economic characteristics, including father’s education (p < 0.001), father’s job position (p < 0.001), and house ownership status (P = 0.005). Father illiteracy/low literacy (up to 5 years of education) was significantly more frequent in boys (15.5%) as compared to girls (5.5%). However, among boys, a higher proportion (21.6%) had fathers with higher-ranking job positions (employee/clerks) compared to girls (13.9%) (p < 0.001) and compared to girls (29%), a significantly higher proportion of the families of boys (36%) were tenants. Details on the background characteristics of the participants were described in Table 1.
FNLIT status of the study participants
FNLIT level of the participants is shown in Fig. S1. Approximately 11.6% of students were categorized as having low FNLIT, while almost 25% had low scores in FNLIT skill domain, and the majority scored moderate to high in cognitive domain (97.4%). Among subscales of FNLIT skill domain, a high proportion of students had low scores in critical FNLIT (42.2%) and food label literacy (81.1%). However, they scored better in food choice literacy (only 7.8% scored low).
Confirmatory factor analysis
The fit indices for CFAs used to develop the constructs of eating behaviors (χ2/df = 2.65, GFI = 0.95, AGFI = 0.93, CFI = 0.90, IFI = 0.90, RMSEA = 0.05) and academic achievement (χ2/df = 3.91, RMSEA = 0.07, GFI = 0.98, AGFI = 0.95, CFI = 0.99, IFI = 0.99, RMSEA = 0.07), socio economic factor (χ2/df = 2.17, p = 0.007, GFI = 0.98, AGFI = 0.96, CFI = 0.96, IFI = 0.96, RMSEA = 0.04) and demographic factor (χ2/df = 1.77, p = 0.06, GFI = 0.99, AGFI = 0.97, CFI = 0.99, IFI = 0.99, RMSEA = 0.03) had acceptable fit to the data. All components were significantly related to their latent variables (p < 0.001). Mother education and mother age explained a higher proportion of the variance of the socio economic and demographic factors, respectively. Reading mark, the frequency of eating lunch per week and the frequency of sausage/hamburger explained a higher proportion of the variance of academic achievement, unhealthy and healthy eating behaviors, respectively (Fig. 3).

Results of Confirmatory Factor Analysis (CFA). Ellipses: latent variables; boxes: observed variables. All coefficients are standardized and have a p.value < 0.001. Fit indices of measurement model of Socio-economic status: χ2/df = 2.17, p = .007, GFI = .98, AGFI = .96, CFI = .96, IFI = .96, RMSEA = .04. Fit indices of measurement model of Demographic status: χ2/df = 1.77, p = .06, GFI = .99, AGFI = .98, CFI = .99, IFI = .99, RMSEA = .03. Fit indices of measurement model of Eating behaviors: χ2/df = 3.24, p < .0001, GFI = .95, AGFI = .92, CFI = .89, IFI = .89, RMSEA = .05. Fit indices of measurement model of School achievement: χ2/df = 3.91, p < .0001, GFI = .98, AGFI = .95, CFI = .99, IFI = .99, RMSEA = .07
Structure equation modeling
The proposed FNLIT model was tested after controlling for the possible confounding impact of the background variables (Figs. 4 and 5). The fit indices suggested a reasonably adequate data fit for the hypothesized model. The standardized regression weights (β) from the structural equation model are shown in Models 1 and 2. When the direct and indirect effects of FNLIT on dietary habits were examined (Model 1, Table 2), FNLIT score had a positive direct (non-mediated) relationship with healthy eating behavior (β = 0.13, P = 0.005) and academic achievement (β = 0.23 P < 0.001). This pattern was strongly reversed in unhealthy eating behavior (β = − 0.30, P < 0.001). Socioeconomic status (SES), including mother’s job and education, school status (governmental), and the family size, was directly related to FNLIT score and overweight/obese in students (β = 0.13, P = 0.006; β = 0.14, P = 0.007 respectively), while also had direct (β = 0.30, P < 0.001) and indirect (food insecurity mediated) relationship with academic achievement (β = − 0.40, P < 0.001); β = − 0.12, P = 0.008 respectively). There was a full mediation relationship between FNLIT and overweight/obese via healthy eating behaviors. FNLIT indirectly through healthy eating behavior, had a negative effect on overweight/obese (of FNLIT on healthy eating behaviors, β = − 0.13, p < 0.01; of healthy eating behaviors on overweight/obese, β = −-0.10, p < 0.05) (Fig. 4, Table 2).

Linking FNLIT status to its determinants and related outcomes (Model 1). Note: Statistically non-significant associations are not shown. FNLIT, Food and Nutrition Literacy; χ2, Chi square; df, degree of freedom; GFI, goodness fit index; AGFI, adjusted goodness of fit index; CFI, Comparative Fit Index; IFI, Incremental Fit Index; RMSEA, root mean square error of approximation.; SRMR, Standardized Root Mean Square Residual. χ2/df = 2.03, p < 0.001, GFI = .90, AGFI = .88, CFI = .91, IFI = .91, RMSEA = .04, SRMR = .06

Linking FNLIT’s subscales to its determinants and related outcomes (Model 2). Note: Statistically non-significant associations are not shown. Abbreviations: Cognitive subscales including: UFNI, Understanding Food and Nutrition Literacy; NHK, Nutritional Health Knowledge; Skill subscales including; FFNL, Functional Food and Nutrition Literacy IFNL, Interactive Food and Nutrition Literacy; FCL, Food Choice Literacy; CFNL, Critical Food and Nutrition Literacy; FLL, Food Label Literacy., χ2, Chi square; df, degree of freedom; GFI, goodness fit index; AGFI, adjusted goodness of fit index; CFI, Comparative Fit Index; IFI, Incremental Fit Index; RMSEA, root mean square error of approximation.; SRMR, Standardized Root Mean Square Residual. χ2/df = 1.93, p < 0.001, GFI = .89, AGFI = .87, CFI = .91, IFI = .91, RMSEA = .04, SRMR = .06. *P < .05
Model 2 demonstrated the linking of FNLIT’s subscales to its determinants and related outcomes (Fig. 5). Mother’s job and education, school status (governmental schools), and family size were the socio-economic determinants of “Understanding Food and Nutrition Information” (β = 0.10, P < 0.05), “Food Choice Literacy” (β = 0.10, P < 0.01), and “Food Label Literacy” (β = 0.19, P < 0.01). SES predicted academic achievement partially through the mediating effect of “Food Label Literacy” (of SES on “Food Label Literacy”, β = 0.19, P < 0.01; of “Food Label Literacy” on academic achievement, β = 0.11, P < 0.05). The results indicated, despite the direct relationship between SES and academic achievement (β = 0.25, P < 0.001), an indirect but negative relationship existed through food insecurity (of SES on food insecurity, β = − 0.42, P < 0.001; of food insecurity on academic achievement, β = − 0.10, P < 0.05). Demographic factors negatively affected unhealthy eating behaviors (β = − 0.29, P = 0.001) and BMIZ-score (β = − 0.25, P = 0.003).
Demographic factors, including mother’s age, ethnicity (fars), ethnicity (tork), grade, and gender, were the most important determinants of “Critical Food and Nutrition Literacy” (β = − 0.17, P = 0.01), FCL (β = 0.16, P = 0.02), unhealthy eating behaviors (β = − 0.29, P = 0.001), and BMI Z-score (β = − 0.25, P = 0.003). The finding also revealed the fully mediating role of “Food Choice Literacy” in the relationship between demographic factors and healthy eating behaviors (of demographic factors on “Food Choice Literacy”, β = 0.16, P = 0.02; of “Food Choice Literacy” on healthy eating behaviors, β = 0.13, P = 0.02). In our study, we also found that “Interactive Food and Nutrition Literacy” protected unhealthy eating behaviors (β = − 0.43, P < 0.001), and “Food Choice Literacy” predicted healthy eating behaviors (β = 0.13, P = 0.02) in children.
The fit indices suggested a reasonably adequate fit of the FNLIT’s subscale model (Fig. 5).
Discussion
In the current study, the proposed FNLIT conceptual model was tested to describe the determinants and outcomes of FNLIT in primary school children.
Socio-economic determinants of the outcomes of FNLIT, eating behaviors, academic achievement, and overweight
Small family size, private schooling, mothers’ education, and occupation were the most important socio-economic determinants acting as the predictive factors of FNLIT and its subscales scores, including UFNI, FCL, and FLL. This finding is aligned with Sørensen et al., (2012) study, which reported the overall relationship between socio-economic status (parental education and occupation) and different forms of literacy (i.e., health literacy) in childhood and youth [56].
The evidence shows that family socio-demographic factors strongly influence children’s food literacy [57]. Parents, especially mothers, are important agents in the promotion of health, behavior, and abilities of their children; they create food environments and play a key role in structuring their children’s first experiences with food and eating through their own beliefs, food practices, perspectives, eating attitudes, knowledge, and understanding of the benefits of food and nutrients on health (1). The literature suggests that well-educated parents have a skill set that includes the ability to develop and facilitate children’s food and nutrition skills, for example, improving the critical thinking about media to defend from the persuasive influences of food advertisements (food and nutrition critical skills), opportunities to make food selections independently, such as by selecting a healthy snack at a convenience store after school using reading and understanding of food labels (food choice skills and food label literacy), obtain, interpret and apply of nutrition information (2, 3). The children of well-educated parents may better obtain, process, interpret and apply information that shapes their knowledge and attitudes about nutrition [58]. Parents can be role models for accessing and interpreting food and nutrition information and teaching children how to critically analyze the credibility and validity of information sources and media channels [59]. However, socioeconomic status has different impacts on food behavior and skills. Several studies have shown that communities with low socioeconomic status have more likely to make unhealthy food choices [60]. High socioeconomic status has also been linked with increased fruit and vegetables, dairy products, and other healthy foods among children and adolescents [58]. Families with a higher level of education may also promote greater investment in their children’s health. On the other hand, Larson et al. (2006) showed that greater involvement of children in food and nutrition skills/food literacy (food preparation and food shopping skill) is related to low socioeconomic status [24].
In addition to the significant direct effect of family SES on academic achievement, family SES indirectly affects academic achievement through FNLIT. The finding of several meta-analysis reviews [61, 62] revealed that parents’ location in the socioeconomic structure substantially impacts students’ academic achievement. Family SES sets the stage for students’ academic achievement by directly providing resources at home and indirectly providing the social capital necessary to succeed in school.
The current research has documented that those children with a low family size, educated and employed mothers, and children in the private schools had a higher probability of being overweight/obese. On the other hand, SES indirectly impacted overweight/obesity through FNLIT and healthy eating behaviors (negatively).
Based on the results, the effect of SES on academic achievement was mediated by food insecurity. Several studies have reported low SES and its connection to food insecurity as a key risk factor for unfavorable academic achievement [63,64,65]. Food insecurity has been associated with poor psychosocial outcomes, mental health, cognitive development, and compromised dietary intake, potentially resulting in malnutrition and, subsequently, low academic achievement [38, 64, 66].
Our results suggest that although SES is a condition that is difficult to change, helping children develop the cognitive and skill domain of FNLIT may improve their weight status and academic achievement and reduce social inequalities in child education and health.
The impact of socio-demographic characteristics on children’s skills (FCL and CFNL) can be explained that parents are more involved in daily food-related decisions and activities, including meal planning, grocery shopping, and cooking, that can create environments to influence the nutritional skills of children [67, 68]. Consistent with our results, models that focus specifically on children and young people emphasize the family’s demographic factors. The younger the child is, the more likely he/she is to rely on their parents' economic and social support [57, 69].
Link between FNLIT, eating behaviors, academic achievement, and overweight
The relationship between healthy eating behaviors and overweight/obesity reduction has been shown in several studies [70, 71]. According to studies, by placing children at the center of food production, cooking food, selling food, and sharing food with their community, food literacy programs are helping to develop their food and nutrition skills to understand food and the benefits of a healthy diet. It will lead to a positive shift in healthy eating behaviors and may affect obesity trends [7, 72]. The current study also showed that FNLIT, especially in skills domain, is the essential determinant of healthy eating behavior. Regarding the association between FNLIT and eating behaviors, our findings are in line with interventional [73, 74] and correlational studies [75,76,77] as well as systematic review [6].
Previous studies found that high food literacy/nutrition literacy is associated with the frequency of main meal consumption [78], preference for healthy foods, lower intake of fast food and packaged or processed snacks among school-age children and adolescents in developed and developing countries [79, 80]. The limited awareness of FNLIT, functional, interactive, and food label literacy can create barriers to consuming a diverse and nutrient adequate diet [81]. Chung et al. (2017) stated that the unhealthy eating behaviors and lower quality of diet are related to the lack of food and nutrition knowledge, why and how food labeling information is read, and how healthy foods are prepared and safely saved to avoid food poisoning [26]. These are the so-called food and nutrition literacy concepts [5, 51].
Researches indicated that building food literacy in children through school gardens contributes to increased academic achievement, engagement, and self-confidence [82]. This relationship can be explained from two perspectives. First, FNLIT can reduce barriers to healthy eating and may influence adolescents’ dietary intake [6]. On the other hand, some studies confirm the association between eating behaviors and academic achievement in school-age children [83, 84]. Unhealthy eating patterns likely affect the intake of protein, vitamins, and minerals in both a quantitative and qualitative sense, jointly leading to metabolic consequences, which influence academic achievement negatively.
Adequacy of food choice literacy and food label literacy in children improves their ability to understand information about food items and food groups, read food labels, control their portions, and make informed decisions and healthy eating behaviors [9]. On the other hand, students with high critical skills are more involved in questioning and thinking critically to advance the various teaching fields [10]. These findings are consistent with our results on the mediating effect of food label literacy and food choice skills in promoting children’s eating behaviors.
The large study sample provided sufficient power to probe relatively small effects. In addition, this study enables us to minimize the confounding effects of other factors on the relations between FNLIT to eating behavior, academic achievement, and overweight/obesity by considering numerous covariates and their interactions using standardized regression analyses. To the best of our knowledge, the present study is the first to investigate the direct and indirect link between FNLIT, eating behaviors, academic achievement, and overweight in children. However, several limitations merit consideration. First, it is impossible to establish causal association due to the cross- sectional research design. However, SEM does let us evaluate the dose-response of the interrelationships of the variables. Second, our study population was not representative of the Iranian school population, meaning that our results may not be generalizable to the wider population of Iranian school children. The third is the memory bias that may occur when a self-reported dietary assessment method such as dietary recalls is applied. Furthermore, the impact of unmeasured confounders cannot be excluded entirely.
Future research with longitudinal design will be needed to elucidate the mechanisms involved in this relationship. Moreover, interventions to determine the relationship between change in food and nutrition literacy scores for before and after outcome variables are necessary.
Conclusion
This research positions FNLIT within a conceptual model of its determinants and outcomes in primary school children and proposes an evaluation framework to guide investment and practice. These are critical foundations to further works in this field. The study results highlight groups within the school population who are at adequate levels of FNLIT, including having mothers with high-education levels, employed mothers, small family sizes, and children with private schooling children. These results serve as a general reminder that children (and their families) have highly varying educational needs that school educators and policymakers should consider new strategies based on this. In addition, our study draws attention to FNLIT, especially the skills domain, including IFNL, FCL, and FLL, as the essential determinant of healthy eating behavior, academic achievement, and weight status in school-age children and may reduce social inequalities in children’s development.
To ensure an adequate level of FNLIT, educators should assess and plan to enhance the food literacy skills of children and adolescents. Without a complete understanding of food, nutrition, and health, children and adolescents cannot gear up to improve their eating habits and diet quality. The current findings suggest that interventions targeting FNLIT improvement may effectively improve children’s eating behaviors, school academic achievement, and weight status. Stakeholders, including the government, food manufacturers, health providers, educators, and the food industry, should also play their roles to achieve a more significant reach and impact on the community.
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- FNLIT:
-
Food and nutrition literacy
- UFNI:
-
Food and nutrition information
- NHK:
-
Nutritional health knowledge
- FFNL:
-
Functional food and nutrition literacy
- IFNL:
-
Interactive food and nutrition literacy
- CFNL:
-
Critical food and nutrition literacy
- FCL:
-
Food choice literacy
- FLL:
-
Food label literacy
- SEM:
-
Structural equation modeling
- SES:
-
Socioeconomic status
References
Sobal J, Bisogni CA. Constructing food choice decisions. Ann Behav Med. 2009;38:s37–46.
Colatruglio S, Slater J. Food literacy: bridging the gap between food, nutrition and well being. In: Deer F, Falkenberg T, McMillan B, Sims L, editors. Sustainable well-being: concepts, issues, and educational practices. Winnipeg: ESWB Press; 2014. p. 37–55.
Laska MN, Larson NI, Neumark-Sztainer D, Story M. Does involvement in food preparation track from adolescence to young adulthood and is it associated with better dietary quality? Findings from a 10-year longitudinal study. Public Health Nutr. 2012;15:1150–8.
Zoellner J, You W, Connell C, Smith-Ray RL, Allen K, Tucker KL, et al. Health literacy is associated with healthy eating index scores and sugar-sweetened beverage intake: findings from the rural Lower Mississippi Delta. J Am Diet Assoc. 2011;111:1012–20.
Vidgen HA, Gallegos D. Defining food literacy and its components. Appetite. 2014;76:50–9.
Vaitkeviciute R, Ball LE, Harris N. The relationship between food literacy and dietary intake in adolescents: a systematic review. Public Health Nutr. 2015;18:649–58.
Brooks N, Begley A. Adolescent food literacy programmes: a review of the literature. Nutr Diet. 2014;71:158–71.
Kim SY, Sim S, Park B, Kong IG, Kim JH, Choi HG. Dietary habits are associated with school performance in adolescents. Medicine (Baltimore). 2016;95:e3096.
Cullen T, Hatch J, Martin W, Higgins JW, Sheppard R. Food literacy: definition and framework for action. Can J Diet Pract Res. 2015;76:140–5.
Velardo S. The nuances of health literacy, nutrition literacy, and food literacy. J Nutr Educ Behav. 2015;47(385–389):e381.
Doustmohammadian A, Omidvar N, Keshavarz-Mohammadi N, Abdollahi M, Amini M, Eini-Zinab H. Developing and validating a scale to measure Food and Nutrition Literacy (FNLIT) in elementary school children in Iran. PLoS One. 2017;12:e0179196.
Nutbeam D. The evolving concept of health literacy. Soc Sci Med. 2008;67:2072–8.
Mikkila V, Rasanen L, Raitakari OT, Pietinen P, Viikari J. Longitudinal changes in diet from childhood into adulthood with respect to risk of cardiovascular diseases: the cardiovascular risk in young finns study. Eur J Clin Nutr. 2004;58:1038–45.
Colatruglio S, Slater J. Challenges to acquiring and utilizing food literacy: perceptions of young Canadian adults. Can Food Stud. 2016;3:96–118.
Pirouznia M. The correlation between nutrition knowledge and eating behavior in an American school: the role of ethnicity. Nutr Health. 2000;14:89–107.
Marsh HW, Morin AJ, Parker PD, Kaur G. Exploratory structural equation modeling: an integration of the best features of exploratory and confirmatory factor analysis. Annu Rev Clin Psychol. 2014;10:85–110.
Castro MA, Baltar VT, Marchioni DM, Fisberg RM. Examining associations between dietary patterns and metabolic CVD risk factors: a novel use of structural equation modelling. Br J Nutr. 2016;115:1586–97.
Mueller RO, Hancock GR. Structural equation modeling. In the reviewer’s guide to quantitative methods in the social sciences. Charlotte: Routledge, Information Age Publishing; 2018. p. 445–56.
Doustmohammadian A, Keshavarz Mohammadi N, Omidvar N, Amini M, Abdollahi M, Eini-Zinab H, et al. Food and nutrition literacy (FNLIT) and its predictors in primary schoolchildren in Iran. Health Promot Int. 2019;34:1002–13.
Tabacchi G, Battaglia G, Alesi M, Paoli A, Palma A, Bellafiore M. Food literacy predictors and associations with physical and emergent literacy in pre-schoolers: results from the training-to-health project. Public Health Nutr. 2020;23:356–65.
Khorramrouz F, Doustmohammadian A, Eslami O, Khadem-Rezaiyan M, Pourmohammadi P, Amini M, et al. Relationship between household food insecurity and food and nutrition literacy among children of 9–12 years of age: a cross-sectional study in a city of Iran. BMC Res Notes. 2020;13:1–6.
West EG, Lindberg R, Ball K, McNaughton SA. The role of a food literacy intervention in promoting food security and food literacy—OzHarvest’s NEST Program. Nutrients. 2020;12:2197.
Begley A, Paynter E, Butcher LM, Dhaliwal SS. Examining the association between food literacy and food insecurity. Nutrients. 2019;11:445.
Larson NI, Story M, Eisenberg ME, Neumark-Sztainer D. Food preparation and purchasing roles among adolescents: associations with sociodemographic characteristics and diet quality. J Am Diet Assoc. 2006;106:211–8.
Soleymani MR. Investigating the relationship between information literacy and academic performance among students. J Educ Health Promot. 2014;3:95.
Chung LMY. Food literacy of adolescents as a predictor of their healthy eating and dietary quality. J Child Adolesc Behav. 2017;5:1–2.
Liao L-L, Lai I-J, Lee C-K. Nutrition literacy: a mediator of healthy-eating behavior based on the social ecological framework. In: source: 19th International Congress on Nutrition & Health; 2018. p. 6–6.
Chang Y, Kim J, Chatterjee S. The association between consumer competency and supplemental nutrition assistance program participation on food insecurity. J Nutr Educ Behav. 2017;49:657–666.e651.
Krause C, Sommerhalder K, Beer-Borst S, Abel T. Just a subtle difference? Findings from a systematic review on definitions of nutrition literacy and food literacy. Health Promot Int. 2016;33:378–89.
Palumbo R. Sustainability of well-being through literacy. The effects of food literacy on sustainability of well-being. Agricult Agricult Sci Proc. 2016;8:99–106.
Godrich SL, Davies CR, Darby J, Devine A. What are the determinants of food security among regional and remote Western Australian children? Aust N Z J Public Health. 2017;41:172–7.
Ronto R, Ball L, Pendergast D, Harris N. Environmental factors of food literacy in Australian high schools: views of home economics teachers. Int J Consum Stud. 2017;41:19–27.
Meyer N, Reguant-Closa A. “Eat as if you could save the planet and win!” Sustainability integration into nutrition for exercise and sport. Nutrients. 2017;9:412.
Barbour LR, Ho MY, Davidson ZE, Palermo CE. Challenges and opportunities for measuring the impact of a nutrition programme amongst young people at risk of food insecurity: a pilot study. Nutr Bull. 2016;41:122–9.
Esfandiari S, Omidvar N, Eini-Zinab H, Doustmohammadian A, Amirhamidi Z. Associations among food insecurity, academic performance, and weight status in primary schoolchildren in Tehran, Iran: a cross-sectional study. J Nutr Educ Behav. 2018;50(109–117):e101.
Dewi NU, Nurulfuadi N, Aiman U, Hartini DA, Pradana F, Bohari B. Food Insecurity and anthropometry in adolescents: a literature review. Open Access Macedonian J Med Sci. 2020;8:234–40.
Magulod GC Jr. Anthropometric status and eating behavior as predictors of University Students’ Academic Achievement. Asia Pac J Multidiscip Res. 2019;7:32–42.
Burrows T, Goldman S, Pursey K, Lim R. Is there an association between dietary intake and academic achievement: a systematic review. J Hum Nutr Diet. 2017;30:117–40.
Bellotti B. Food literacy: reconnecting the city with the country, vol. 22; 2010. p. 29–34. Availabe from: http://search.informit.com.au/documentSummary;dn=609839497923648;res=IELHSS.
Block LG, Grier SA, Childers TL, Davis B, Ebert JE, Kumanyika S, et al. From nutrients to nurturance: a conceptual introduction to food well-being. J Public Policy Mark. 2011;30:5–13.
Desjardins E. “Making something out of nothing”: food literacy among youth, young pregnant women and young parents who are at risk for poor health: Ontario Public Health Association; 2013. Available from: http://www.osnpph.on.ca/resources/Food%20Literacy%20Study.LDCPOntario.Final.Dec2013.pdf.
Howard A. What's to Eat?: improving food literacy in Canada. In Conference Board of Canada. Available from: http://www.conferenceboard.ca/temp/d95c5003-64f9-43b3-bb90-0844b849460a/14-091_whatstoeat_cfic_rptpdf2013. Accessed 21 Aug 2021.
Schnoegl S, Zehetgruber R, Danninger S, Setzwein M, Wenk R, Freudenberg M, et al. Savoury Dishes for Adult Education and Counselling. Guidelines and Toolbox. In: BEST Institut fu¨r berufsbezogene Weiterbildung und Personaltraining (ed); 2006.
Truman E, Elliott C. Barriers to food literacy: a conceptual model to explore factors inhibiting proficiency. J Nutr Educ Behav. 2019;51:107–11.
Topley A. At the table: a case for food literacy coordination. Victoria: Greater Victoria Food Literacy Working Group; 2013. Available from https://mail.google.com/mail/u/0/?ui=2&ik=14f4dc246b&view=att&th=13fab6fa0b29ac06&attid=02&disp=safe&zw.
Fordyce-Voorham S. Identification of essential food skills for skill-based healthful eating programs in secondary schools. J Nutr Educ Behav. 2011;43:116–22.
Bickel G, Nord M, Price C, Hamilton W, Cook J. Guide to measuring household food security. Guide to Measuring Household Food Security in the United States: Revised 2000 No 6 March 2000 USDA. Alexandria: Food and Nutrition Services; 2000.
Rafiei M, Nord M, Sadeghizadeh A, Entezari MH. Assessing the internal validity of a household survey-based food security measure adapted for use in Iran. Nutr J. 2009;8:1.
Geboers B, de Winter AF, Luten KA, Jansen CJ, Reijneveld SA. The association of health literacy with physical activity and nutritional behavior in older adults, and its social cognitive mediators. J Health Commun. 2014;19:61–76.
Bostock S, Steptoe A. Association between low functional health literacy and mortality in older adults: longitudinal cohort study. BMJ. 2012;344:e1602.
Zoellner J, Connell C, Bounds W, Crook L, Yadrick K. Nutrition literacy status and preferred nutrition communication channels among adults in the Lower Mississippi Delta. Prev Chronic Dis. 2009;6:A128.
Organization WH. WHO AnthroPlus software, software for assessing growth and development of the world’s children. Geneva: WHO; 2007.
Schreiber JB, Nora A, Stage FK, Barlow EA, King J. Reporting structural equation modeling and confirmatory factor analysis results: a review. J Educ Res. 2006;99:323–38.
Hooper D, Coughlan J, Mullen M. Structural equation modelling: guidelines for determining model fit. Electron J Bus Res Methods. 2008;6:53–60.
Arbuckle JL. Amos (version 7.0) [computer program]. Chicago: SPSS; 2006.
Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80.
Martin LT, Chen P. 13 Child health and school readiness: the significance of health literacy. Health and Education in Early Childhood. In: Reynolds JA, Rolnick JA, Temple JA, editors. Predictors, Interventions, and Policies. Cambridge: University Press; 2014. https://doi.org/10.1017/CBO9781139814805.018.
Fernández SJPM. Dietary habits and nutritional status of school aged children in Spain. Nutr Hosp. 2006;21:374–8.
Bröder J, Okan O, Bauer U, Bruland D, Schlupp S, Bollweg TM, et al. Health literacy in childhood and youth: a systematic review of definitions and models. BMC Public Health. 2017;17:361.
Pekka P, Pirjo P, Ulla U. Influencing public nutrition for non-communicable disease prevention: from community intervention to national programme-experiences from Finland. Public Health Nutr. 2002;5:245–52.
Sirin SR. Socioeconomic status and academic achievement: a meta-analytic review of research. Rev Educ Res. 2005;75:417–53.
Liu J, Peng P, Luo L. The relation between family socioeconomic status and academic achievement in China: a meta-analysis. Educ Psychol Rev. 2020;32:49–76.
Jamaluddine Z, Sahyoun NR, Choufani J, Sassine AJ, Ghattas H. Child-reported food insecurity is negatively associated with household food security, socioeconomic status, diet diversity, and school performance among children attending UN Relief and Works Agency for Palestine Refugees schools in Lebanon. J Nutr. 2019;149:2228–35.
Faught EL, Williams PL, Willows ND, Asbridge M, Veugelers PJ. The association between food insecurity and academic achievement in Canadian school-aged children. Public Health Nutr. 2017;20:2778–85.
Shankar P, Chung R, Frank DA. Association of food insecurity with children's behavioral, emotional, and academic outcomes: a systematic review. J Dev Behav Pediatr. 2017;38:135–50.
Melchior M, Chastang J-F, Falissard B, Galéra C, Tremblay RE, Côté SM, et al. Food insecurity and children’s mental health: a prospective birth cohort study. PLoS One. 2012;7:e52615.
Parmenter K, Waller J, Wardle J. Demographic variation in nutrition knowledge in England. Health Educ Res. 2000;15:163–74.
Paakkari O, Torppa M, Villberg J, Kannas L, Paakkari L. Subjective health literacy among school-aged children. Health Educ. 2018;118:182–95.
Sanders LM, Shaw JS, Guez G, Baur C, Rudd R. Health literacy and child health promotion: implications for research, clinical care, and public policy. Pediatrics. 2009;124:S306–14.
Ranucci C, Pippi R, Buratta L, Aiello C, Gianfredi V, Piana N, et al. Effects of an intensive lifestyle intervention to treat overweight/obese children and adolescents. Biomed Res Int. 2017;2017:1–11.
Lee HA, Lee WK, Kong K-A, Chang N, Ha E-H, Hong YS, et al. The effect of eating behavior on being overweight or obese during preadolescence. J Prev Med Public Health. 2011;44:226.
Nowak AJ, Kolouch G, Schneyer L, Roberts KH. Building food literacy and positive relationships with healthy food in children through school gardens. Child Obes. 2012;8:392–5.
Adam M, Young-Wolff KC, Konar E, Winkleby M. Massive open online nutrition and cooking course for improved eating behaviors and meal composition. Int J Behav Nutr Phys Act. 2015;12:143.
Garcia AL, Reardon R, McDonald M, Vargas-Garcia EJ. Community interventions to improve cooking skills and their effects on confidence and eating behaviour. Curr Nutr Rep. 2016;5:315–22.
Pirouznia M. The association between nutrition knowledge and eating behavior in male and female adolescents in the US. Int J Food Sci Nutr. 2001;52:127–32.
McGowan L, Caraher M, Raats M, Lavelle F, Hollywood L, McDowell D, et al. Domestic cooking and food skills: a review. Crit Rev Food Sci Nutr. 2017;57:2412–31.
da Rocha Leal FM, de Oliveira BMPM, Pereira SSR. Relationship between cooking habits and skills and Mediterranean diet in a sample of Portuguese adolescents. Perspect Public Health. 2011;131:283–7.
Utter J, Denny S, Lucassen M, Dyson B. Adolescent cooking abilities and behaviors: associations with nutrition and emotional well-being. J Nutr Educ Behav. 2016;48(35–41):e31.
Robson SM, Stough CO, Stark LJ. The impact of a pilot cooking intervention for parent-child dyads on the consumption of foods prepared away from home. Appetite. 2016;99:177–84.
Hersch D, Perdue L, Ambroz T, Boucher JL. The impact of cooking classes on food-related preferences, attitudes, and behaviors of school-aged children: a systematic review of the evidence, 2003-2014. Prev Chronic Dis. 2014;11:E193.
Doustmohammadian A, Omidvar N, Shakibazadeh E. School-based interventions for promoting food and nutrition literacy (FNLIT) in elementary school children: a systematic review protocol. Syst Rev. 2020;9:1–7.
Berezowitz CK, Bontrager Yoder AB, Schoeller DA. School gardens enhance academic performance and dietary outcomes in children. J Sch Health. 2015;85:508–18.
Fu M-L, Cheng L, Tu S-H, Pan W-H. Association between unhealthful eating patterns and unfavorable overall school performance in children. J Am Diet Assoc. 2007;107:1935–43.
Adelantado-Renau M, Beltrán Valls MR, Toledo Bonifás M, Bou Sospedra C, Pastor MC, Moliner-Urdiales D. The risk of eating disorders and academic performance in adolescents: DADOS study. Nutr Hosp. 2018;35:1201–7.
Acknowledgments
The authors hereby express their gratitude to the Shahid Beheshti University of Medical Sciences, National Nutrition and Food Technology Research Institute (NNFTRI), Dr. Fatemeh Mohammadi-Nasrabadi, and all coordinators and interviewers, and all the students who participated in this study. This research was conducted with the approval and funding of the NNFTRI.
Funding
This research was conducted by a grant from the research council of NNFTRI.
Author information
Authors and Affiliations
Contributions
AD was responsible for collecting, analyzing, and interpreting the data, drafting and editing the article. NO, NKM, HE-Z carried out the study design and analysis. AD, NO, NKM, MA1, MA2, and HE-Z participated in conceiving and designing the research, revising the article, and collecting data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
National Nutrition and Food Technology Research Institute (NNFTRI) ethical committee (No.1394.20/16-10-2015) funded and approved the study. Written informed consent was obtained from students and their parents.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Fig. S1.
Food and nutrition literacy status in 10–12 years old students in Tehran.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Doustmohammadian, A., Omidvar, N., Keshavarz-Mohammadi, N. et al. The association and mediation role of Food and Nutrition Literacy (FNLIT) with eating behaviors, academic achievement and overweight in 10–12 years old students: a structural equation modeling. Nutr J 21, 45 (2022). https://doi.org/10.1186/s12937-022-00796-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-022-00796-8